Embed Size (px)
Citation preview
REDUCING THE RISK OF
MEDICATION-ALCOHOL
INTERACTIONS IN OLDER ADULTS
Patricia W. Slattum, PharmD, PhD, CGP
Virginia Commonwealth University
Objectives
Identify medications that may interact with
alcohol and potential outcomes
in older adults.
Describe risk factors for adverse
events from alcohol and medication
interactions among older adults.
Discuss treatment issues in pain,
falls, depression and insomnia
when alcohol and medication
interactions play a role.
Using case studies, develop
strategies to manage alcohol and medication interactions in older adults.
Case
Study
BW
BW
no longer drives, but has three sons living nearby who help with errands such
as grocery shopping and doctor appointments.
93 year old white male
lives with his wife independently in a small
apartment.
married for 71 years
is blind and has significant functional limitations.
requires BW’s assistance with activities of daily
living.
Case BW
BW suffers from
CHF
atrial fibrillation
osteoarthritis
recently diagnosed with depression
His current medications include:
Furosemide 40 mg BID
Potassium 20 mEq BID
Digoxin 0.125 mg QD
Warfarin 4 mg QD
Sertraline 50 mg QD
Acetaminophen 500 mg QID prn
Case BW
His warfarin therapy has been difficult to manage.
His INR has fluctuated above and below the target range.
Told his doctor that he wanted to stop taking all of these medications and
was tired of the monitoring and dosing changes.
His functional status has begun to decline and his family hired a
companion service to assist him 3 mornings each week.
Over the past several months:
After working at the home for 2 weeks, the companion reported to the son that there were empty alcohol bottles in the trash.
BW has a long history of episodes of alcohol misuse, but had been abstinent for almost 15 years after falling down the stairs and breaking his arm while intoxicated.
The son had purchased a bottle of alcohol for his father recently because some friends were planning to visit.
Case BW
Case BW
1 week
After the third fall he was
transported to the ER and
was admitted for
heart failure exacerbation.
Case BW
The sons called a family meeting to discuss living
arrangements for BW
They discover that each of them has been purchasing
alcohol for their father over the past few months.
Neighbors and grandchildren have also purchased alcohol
for him. After some investigating it appears that he may have
been drinking as much as 9 ozof bourbon daily.
• Our bodies experience physical changes as we age.
• These changes can impact:
How well medications get into and out of the body.
How the body responds to medications.
The Aging Body and Medications
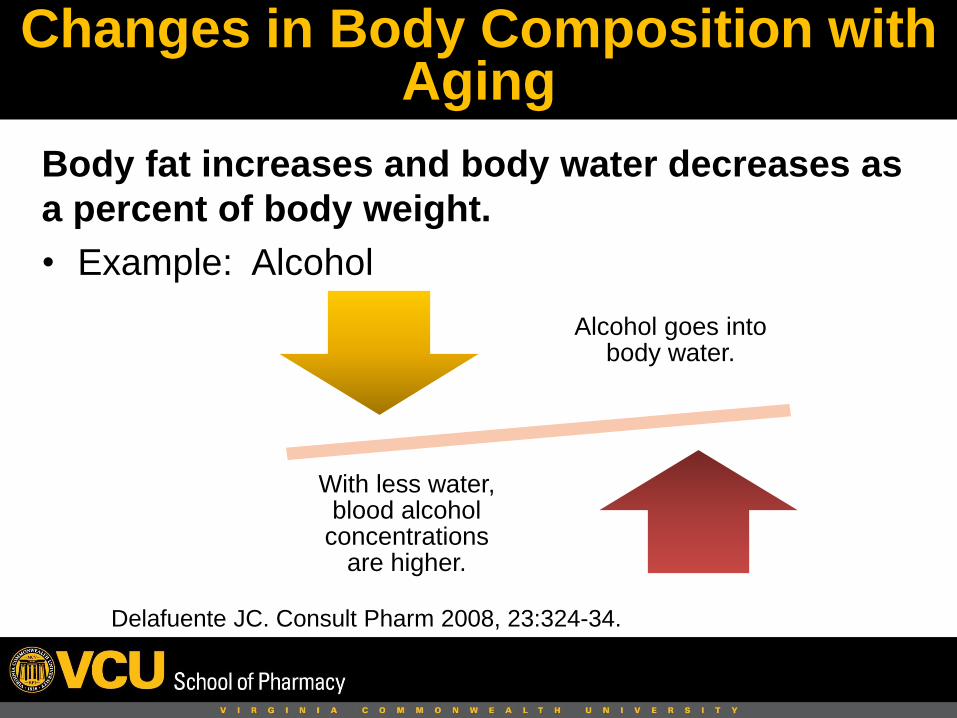
Body fat increases and body water decreases as
a percent of body weight.
• Example: Alcohol
Delafuente JC. Consult Pharm 2008, 23:324-34.
Changes in Body Composition with Aging
Alcohol goes into body water.
With less water, blood alcohol
concentrations are higher.
Most drugs leave the body through the liver and kidney.
Delafuente JC. Consult Pharm 2008, 23:324-34.
Changes in the Kidney and Liver with Aging
• Liver and kidney function decline with aging.
• Drugs take longer to get out of the body.
• Older adults may need lower doses or a longer time
between doses.
Bowie M, Slattum P. J Geriatr
Pharmacother 2007;5: 263-303
Changes in Drug Response with Aging
Older adults may
• Have decreased functional ability before taking the medication.
• Be more sensitive to medications.
• Be less able to compensate for the effects of medications.
This may result in unwanted effects of
medications.
Altered mental status/confusion
Fatigue
Falling
Constipation
Urinary Incontinence
Depression
Dizziness
Tangiisuran B, et al. Age and Ageing 2009;38:358-359. Weingart SN, et al. Arch Intern Med 2005;
165:234-240. Schmader KE, et al. Am J Med 2004;116:394-401.
Adverse events often mistaken for normal aging!
Atypical Presentation of Adverse Drug Events in Older Adults
• Prevalence increases as number of prescribed
drugs increases• 5 to 7 drugs = 4 fold greater risk
• 8 to 10 drugs = 8 fold greater risk
• Cannot prevent all drug interactions!
Mallet L, et al. Lancet 2007;370:185-91.
http://www.fda.gov/downloads/ForConsumers/ConsumerUpdates/ucm096391.pdf
Drug Interactions
• Patient groups at increased risk:– Older adults taking multiple medications
– Those seeing more than one doctor
– Those being infrequently or inadequately monitored
– Those with impaired liver or kidney function
• Dietary supplements, herbal products and over-the –counter medications and alcohol must also be considered.
• Pharmacists look for drug interactions when filling prescriptions.
Mallet L, et al. Lancet 2007;370:185-91.
Drug-Drug Interactions
Harmful interactions: Mixing alcohol with Medicines Brochure
https://pubs.niaaa.nih.gov/publications/Medicine/medicine.htm
Drug-Alcohol Interactions
Mixing certain medications with alcohol can cause
adverse events
Mixing alcohol with sedatives, pain
medications or other drugs acting on the brain can result in
increased sedation, unsteadiness or falls.
Mixing alcohol with aspirin, ibuprofen, naproxen or similar drugs can increase
risk of gastrointestinal
bleeding.
Mixing alcohol with blood pressure
lowering medications can cause blood
pressure to go too low.
OTHER
http://www.rochester.edu/uhs/healthtopics/Alcohol/interactions.html
https://webapps.ou.edu/alcohol/docs/13EtohandMedicationInteractions40-54.pdf
Alcohol and AcetaminophenA
ce
tam
ino
ph
en
found in many combination pain products.
recommendations for maximum dose/day recently decreased to 3,000 mg/day.
when taken during or right after drinking increases the risk of liver damage.
chronic drinking may increase the production of toxic metabolites of acetaminophen.
Pain
Depression
Insomnia
Other
Treatment Issues
• Many medications recommended to manage
pain in older adults interact with alcohol:
– Acetaminophen
– Nonsteroidal Anti-inflammatory Drugs
– Opiate analgesics
• Some patients may be using alcohol to
self-treat pain.
Pain
CASE
STUDY
LR
LR
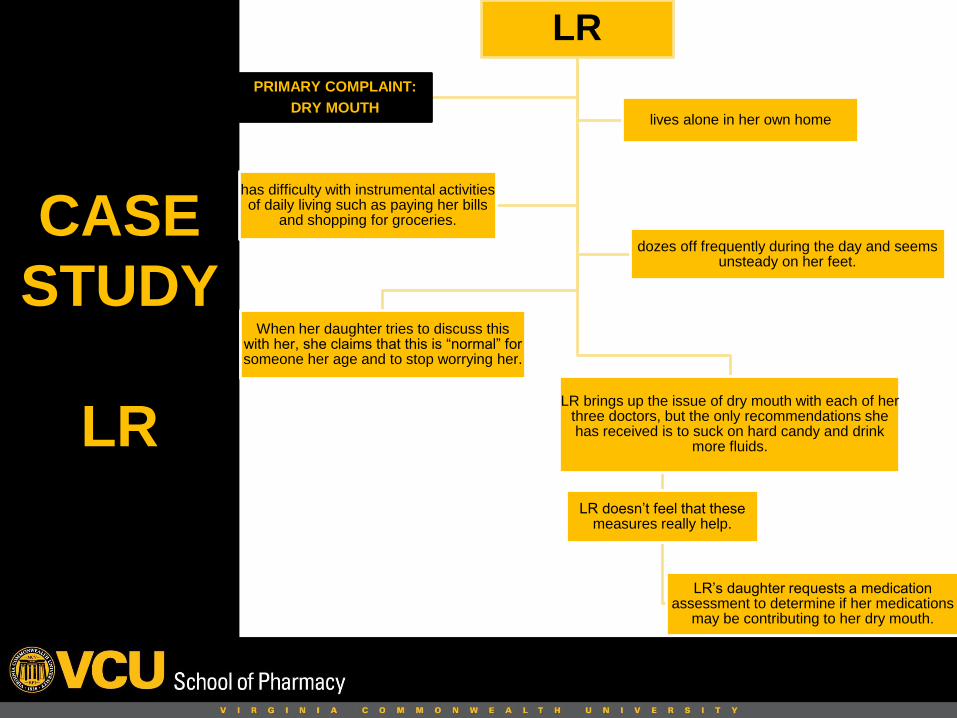
When her daughter tries to discuss this with her, she claims that this is “normal” for someone her age and to stop worrying her.
LR brings up the issue of dry mouth with each of her three doctors, but the only recommendations she has received is to suck on hard candy and drink
more fluids.
LR doesn’t feel that these measures really help.
LR’s daughter requests a medication assessment to determine if her medications
may be contributing to her dry mouth.
PRIMARY COMPLAINT:
DRY MOUTHlives alone in her own home
has difficulty with instrumental activities of daily living such as paying her bills
and shopping for groceries.
dozes off frequently during the day and seems unsteady on her feet.
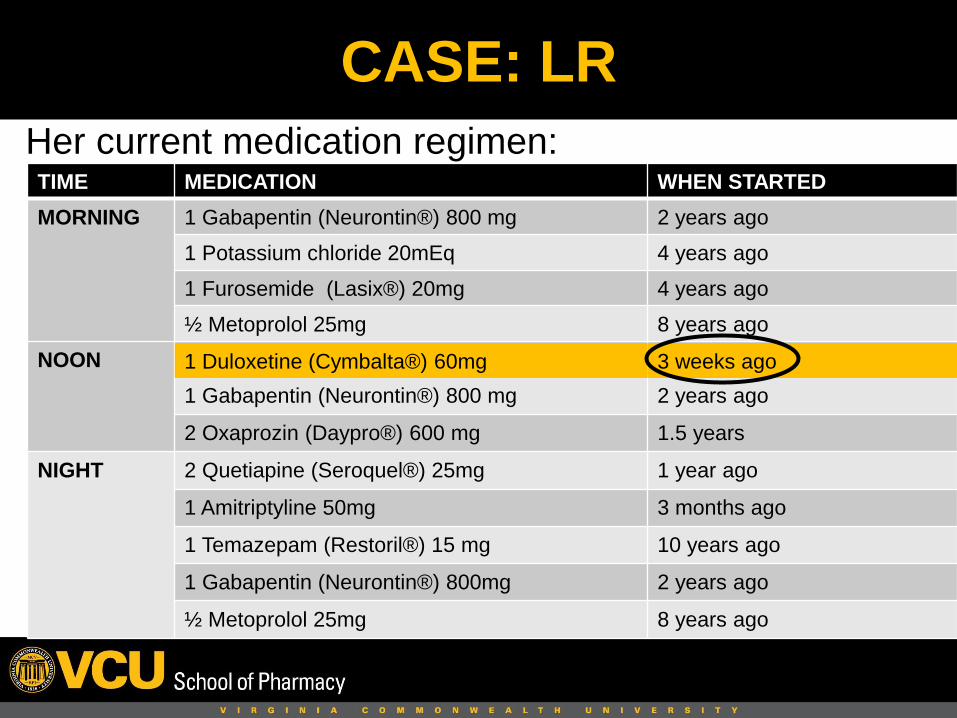
Her current medication regimen:
CASE: LR
TIME MEDICATION WHEN STARTED
MORNING 1 Gabapentin (Neurontin®) 800 mg 2 years ago
1 Potassium chloride 20mEq 4 years ago
1 Furosemide (Lasix®) 20mg 4 years ago
½ Metoprolol 25mg 8 years ago
NOON 1 Duloxetine (Cymbalta®) 60mg 3 weeks ago
1 Gabapentin (Neurontin®) 800 mg 2 years ago
2 Oxaprozin (Daypro®) 600 mg 1.5 years
NIGHT 2 Quetiapine (Seroquel®) 25mg 1 year ago
1 Amitriptyline 50mg 3 months ago
1 Temazepam (Restoril®) 15 mg 10 years ago
1 Gabapentin (Neurontin®) 800mg 2 years ago
½ Metoprolol 25mg 8 years ago
1 Duloxetine (Cymbalta®) 60mg 3 weeks ago
• During an interview, LR admitted to
changing the administration times of some
of her medications and to consuming
“some” alcohol most days of the week.
• She also takes 1000 mg of acetaminophen
in the morning and before going to bed in
the evening each day.
CASE: LR
What are the signs that LR may be
experiencing medication-related problems?
1. New complaint of dry mouth
2. Difficulty with instrumental activities of daily living
3. Dozing off during the day
4. Unsteady on her feet
5. Living alone
What strategies may be used to help LR?
CASE: LR

• Alcohol interacts with all classes of
antidepressants.
• Major depression and alcohol use disorder:
either doubles the chance of having the other.
• There appears to be a causal link between
alcohol use disorder and major depression.
• Best treatment approaches for the older adult
are still unknown.
Boden and Fergussen. Addiction 2011;106:906-914.
Depression
Mohanty M, Slattum PW. Age in Action 2011; Summer
CASE
STUDY
SP
SP
After moving to a senior living center, she started drinking more heavily leading to several falls and a
fractured arm.
82 year old female
Diagnosed with depression and treated with antidepressants in the
past
Has Chronic Obstructive Pulmonary Disorder
(COPD)
Was a smoker for the last 40 years and a
moderate alcohol drinker
Her prescriptions consisted of 11 medications:
• advair (combination of fluticasone & salmeterol), tiotropium, albuterol, montelukast, and Mucinex(guaifenesin and pseudoephedrine) for COPD
• paroxetine for depression
• simvastatin for cholesterol
• supplements (iron and calcium)
• also taking digoxin for congestive heart failure and primodine for tremor. However, during the interview she did not mention a history of tremor or heart failure.
Mohanty M, Slattum PW. Age in Action 2011; Summer
CASE: SP
• What were the signs that SP might be experiencing a medication-related problem?
1. Falls
2. Fracture
3. Living in a senior living center
4. Smoking
5. Depression
• What recommendations do you have for SP?
CASE: SP
• Alcohol interacts significantly with sedatives used to treat insomnia.
• Alcohol worsens sleep disorders.
• Options:
– Treat underlying health conditions
– Evaluate medications as a contributor
– Sleep hygiene: daytime exercise, limit caffeine, exposure to natural light during day, limit napping during the day, etc.
Insomnia
Mohanty M, Slattum PW. Age in Action 2011; Summer
CASE
STUDY
OP
OP
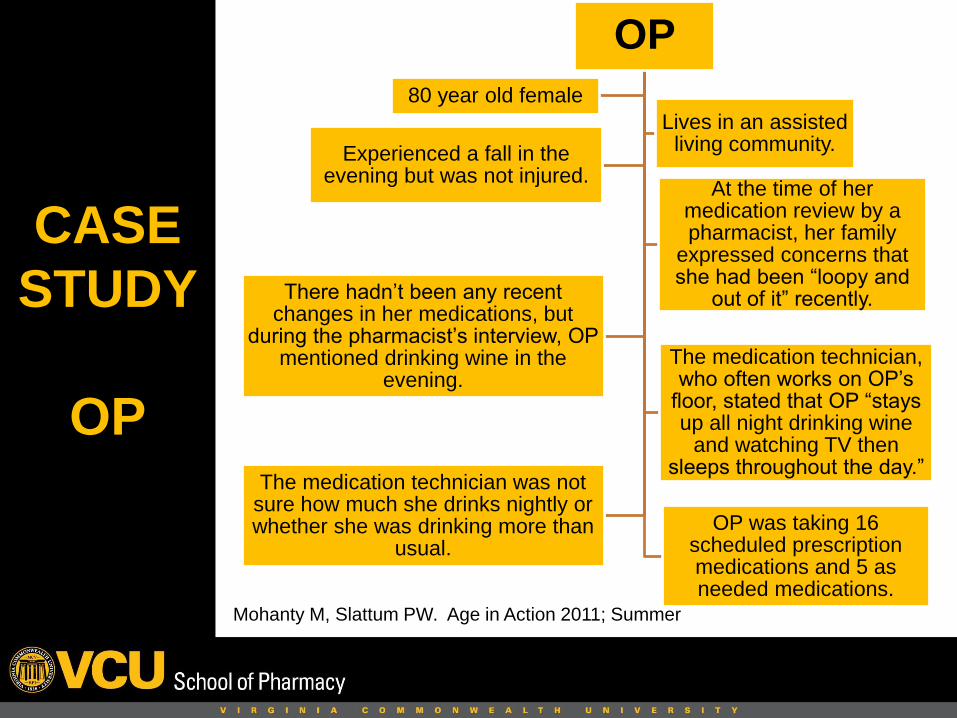
80 year old female
Lives in an assisted living community.
At the time of her medication review by a pharmacist, her family
expressed concerns that she had been “loopy and
out of it” recently.
Experienced a fall in the evening but was not injured.
There hadn’t been any recent changes in her medications, but
during the pharmacist’s interview, OP mentioned drinking wine in the
evening. The medication technician, who often works on OP’s
floor, stated that OP “stays up all night drinking wine
and watching TV then sleeps throughout the day.”
The medication technician was not sure how much she drinks nightly or whether she was drinking more than
usual.
OP was taking 16 scheduled prescription medications and 5 as needed medications.
Her scheduled prescriptions included:
– lisinopril, nadolol, and amlodipine for hypertension
– furosemide for edema
– levothyroxine for thyroid replacement
– albuterol for asthma
– pantoprazole for gastroesophageal reflux disease (GERD)
– solifenacin for urinary incontinence
– citalopram, bupropion, and quetiapine for depression
– trazodone for insomnia and depression
– tramadol for pain
– supplements of potassium and Vitamin D
Mohanty M, Slattum PW. Age in Action 2011; Summer
CASE: OP
What are the signs that OP may be experiencing a medication-related problem?
1. Falls
2. Living in an assisted living facility
3. Being "loopy and out of it"
4. Excessive daytime sleepiness
5. Watching TV all night
What recommendations do you have?
CASE: OP
Improving the Quality of Medication Use in
Elderly Patients: A Not-So-Simple Prescription
“Putting the pieces of the puzzle together to
create a solution remains a formidable, but not
insurmountable task….All the pieces of the
puzzle lie before us; it remains for us to find a
way to fit them together”
Jerry H. Gurwitz, M.D.
Gurwitz JH, Arch Intern Med 2002; 162:1670-3
During his hospitalization, BW abstained from alcohol and his medications were adjusted.
After returning home
• His CHF symptoms and mood improved.
• His gait, balance and functional status improved.
• His family support and companion services were expanded to assist with medication adherence and to monitor for alcohol use.
REVISITING CASE: BW
The National Institute on Alcohol Abuse and Alcoholism (NIAAA)
Drinking Guidelines for Older Adults (over 65 y/o) recommends:
Responsible Drinking
Consider concurrent
medicationsNo more than 7 drinks per week
(one drink per day)
Maximum of 2 drinks on
special occasions
Somewhat lower
limits for women
• Stay engaged
• Exercise the body
• Eat well
• Read warning labels
• Don’t mix alcohol and medications before
seeking advice
Wellness Promotion for the Adult
Take-away Message for Family Caregivers
If you are an adult child, friend or
caregiver of an older adult who
is in need of assistance:
Face the problem
Be direct with the individual
Be supportive without enabling
Offer encouragement and praise
Encourage them to seek help from community resources
Take-away Message for Professionals
If you are a professional in
the field:
Discuss alcohol use with clients/patients
Refer to pharmacist or prescriber for advice on mixing alcohol with specific medications
Learn and use Screening, Brief Intervention, and Referral to Treatment (SBIRT)
Know your community resources