Embed Size (px)
Citation preview

Reconstruction of the AuricleDr. Erami M.D.ENT Resident
Department Of ENTShahid Sadoghi Hospital
Yazd Iran

• A 39-year-old male individualwas involved in a fight andhuman bite

• Time of trauma: 3pm• Time of refer : 6pm• PMH :neg• NPO time: 30min(8:30)

• Amputated segment

• Wound cleaning :• Cleansing is best performed with:
10-mL syringe with an 18-gauge angiocatheter attached.• isotonic sodium chloride solution• dilute povidone-iodine (Betadine)• dilute hydrogen peroxide
• Wound closure:Wound closure is a source of controversy.Head and neck wounds, being in a cosmetically sensitive area, may be closed if they are less than 12 hours old and are not obviously infected

Antibiotic:
The current recommendations from the Infectious Diseases Society of America (IDSA) in patients with an infected human bite wound:
• amoxicillin/clavulanate or ampicillin/sulbactam
• an acceptable alternative in the penicillin-allergic patient
• Trimethoprim-sulfamethoxazole or a quinolone such as levofloxacin or moxifloxacin
+ in addition to +• clindamycin

•Cummings 2015:
• to close simple and complex lacerations that involve cartilage
• Perichondrial and skin sutures are usually sufficient• Occasionally, anchoring sutures through cartilage must be placed
sparingly to bring wound edges together while maintaining the original shape and prominence.
• In older patients, the cartilage is more brittle, and it is difficult to place sutures solely in the cartilage that do not pull through.

•Cummings 2015:
• Small segments of denuded cartilage • as long as perichondrium is still present can be reliably covered with split
or full-thickness skin grafts
• defects that cannot be closed without distorting the ear, especially those that involve the helical rim, can be dealt with in a staged manner
• A robust vascular supply frequently allows partially avulsed auricular segments to survive

•Cummings 2015:
• Some authors advocate deepithelialization of the avulsed segment followed by burial in a postauricular subcutaneous pocket
• whereas others believe that the final result of a reconstructed auricle is more reliable with an autograft than with banked cartilage, which often resorbs to some degree and is ultimately distorted.

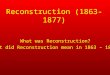
A,. Devitalized skin has been removed to reveal a well-preserved cartilaginous framework suitable for reconstruction.
B, Avulsed cartilage anatomically aligned with intact inferior framework and banked in a postauricularscalp pocket.
Dog-bite injury resulted in composite defect of superior auricle

•Cummings 2015:• A variation of the “pocket principle” described byBaudet involve deepithelialization ofonly the posterior aspect of the avulsed segment followed by fenestration of the exposed cartilage at1-cm intervals.• The anterior skin edge of the avulsed segment maythen be sutured to a modest postauricular scalp flap
elevated over the mastoid to provide a vascular supply. • The flap should be divided several weeks later and askin graft should be applied posteriorly on the auricle.

•Cummings 2015:• Advocates of this technique cite preservation of the original cartilaginous
framework and overlying skin with reliable results.
• A temporoparietal fascia flap followed by splitthickness skin grafting also serves to salvage an amputated auricle in an acute setting.
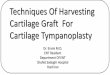
• In experienced hands, microvascular replantation of an avulsed segment generally yields the best final outcome, even in cases of venous insufficiency or inability to perform a venous anastomosis.
• Leech therapy and anticoagulation protocols are acceptable adjuncts in these cases and often have favorable results.

Appearance of the composite graft on second postoperative day. Venous congestion was relieved by leech therapy.

• Topographic anatomy of auricle :


• Arterial blood supplyto auricle :
• superficial temporal a.• Postauricular a.



• Auricular Reconstruction Based on Anatomic Location:
• Defects of Conchal Bowl and Root of Helix
• Defects of Superior Third of Auricle
• Defects of Middle Third of Auricle
• Defects of Inferior Third of Auricle

• Defects of Middle Third of Auricle :
• Small defects (<1.5 cm) may be closed by converting the defect into a wedge-shaped excision, although this approach will have a direct impact on the vertical height of the ear.
• Full-thickness helical defects less than 2.5 cm are amenable to helical chondrocutaneous advancement flaps.
• Defects that are larger than 2.5 cm in width and confined to the helical rim may be repaired with an interpolated cutaneous tube flap.
• Large defects of the central third of the auricle involving the helix and antihelix require cartilage grafting to achieve the necessary structural support.

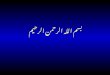
• Two-stage postauricular advancement flap for repair of defect of central third of auricle.
• A, Traumatic auricular defect

• B, Design of postauricularadvancement flap.

• C, Stages of reconstruction

• D, First stage completed

• E, Second stage.
• Release of flap from posterior attachment and incorporation ofsupporting septal cartilage graft.Graft, shown outside of flap, wasinserted beneath flap to provideframework for constructed helix

• F, Postoperative result at• 6 months.


• The first stage involves :
• creating a cutaneous advancement flap based posteriorly on the scalp. • The width of the flap is equal to the height of the defect, and the flap is
elevated from the skin of the medial aspect of the remaining auricle and from the postauricular sulcus skin immediately adjacent to the defect.

• The first stage involves :
• The flap is advanced over the lateral aspect of the defect.
• The medial aspect of the auricular cartilage is exposed :• as a result of dissecting the skin away from it in the process of creating
the flap.
• The exposed cartilage is attached to and nourished by the denuded postauricular soft tissue.

• The first stage involves :
• During the first stage, septal or conchal cartilage is implanted beneath the advancement flap to replace missing portions of the auricular cartilage.
• The cartilage graft is sutured directly to the borders of the auricular cartilage defect.
• The advancement flap provides soft tissue coverage for the cartilage graft and replaces the missing skin of the lateral ear.

• The second surgical stage:
• performed 3 weeks later• involves :• detachment of the advancement flap from the scalp.• The flap is then folded on itself as a hinge flap to cover the medial aspect of
the cartilage graft. • For this to occur, the medial aspect of the cartilage graft and the auricular
cartilage attached to the postauricular denuded soft tissue during the first surgical stage are released from their attachments to the postauricular soft tissue.


• The second surgical stage:
• Flap inset must provide adequate skin coverage of the cartilage graft and prevent exposure of any auricular cartilage medially.
• A full-thickness skin graft is used to close the postauricular donor area if it cannot be closed primarily.
In cases of extensive cartilage loss in the central third of the ear: • a more complex framework using the sixth to eighth ribs is carved and
tailored to the missing segment of auricular cartilage.• The framework is then covered by a postauricular skin advancement flap

• Reconstruction of central and inferior auricular defect with costal cartilage framework.
• A, Defect resulting from motor• vehicle accident.

• B, Drawings showing stagesof reconstruction.

• C, Costal cartilage graft tailored toreplace missing cartilaginous segment.

• D, Framework implanted beneathpostauricular skin.

• E, Postoperative result 4 months afterframework elevation with overlying Skinand full-thickness skin grafting of medialsurface of constructed area.

• Another approach to reconstruction:
• Another approach to reconstruction of the middle third of the helixwhen the skin of the medial aspect of the concha and the postauricular
sulcus are intact is :• to use a postauricular interpolated advancement flap in two surgical stages.

• Unlike most interpolated flaps that are transferred by pivotal movement, this flap is transferred by advancement over the intervening skin of the postauricular sulcus.
• In contrast to the previous discussion, in which the skin of the medial ear is incorporated into the advancement flap, in this case the skin of the medial aspect of the ear and of the postauricular sulcus is left undisturbed.
• The advancement flap is incised posterior to the postauricular sulcus.• It is advanced over the skin of the postauricular sulcus and sutured to the
margins of the lateral auricular skin defect. • This creates a skin-lined channel representing the postauricular sulcus
beneath the pedicle of the flap

• A, Loss of central third of helix

• B, First stage
• Interpolated flapfrom postauricular skin attached tolateral margin of auricular defect.Skin of postauricular sulcus leftundisturbed.

• C, Hinge flap based on auricleis designed for reconstruction of helix.

• The second stage is performed :• 2 to 3 months after the first stage.• The pedicle of the interpolated flap is divided :• from its posterior attachment to the scalp.• The flap is folded over like a hinge to restore the absent helix and is sutured
to the border of the skin defect of the medial aspect of the concha.• A cartilage graft may be positioned under the flap during the second stage if
structural support is necessary.• The donor defect resulting from flap inset is closed primarily or with a local
scalp flap. • Detaching the pedicle of the flap restores the postauricular sulcus to its
original condition.

• D, Second stage
• Pedicle of interpolated flapdivided and hinge flap foldedmedially and sutured to exposedskin margin of postauricular sulcus.

• E, Donor defect from inset ofinterpolated flap closed primarily.

• F, G, Four months after inset of flap

• The advantages:• The advantage of using the interpolated postauricular advancement flap
compared with the technique of incorporating the postauricular skin into an advancement flap is :
• that the medial aspect of the concha is not denuded and does not require subsequent release from attachments to the mastoid periosteum.
• A skin graft is not required to cover the medial aspect of the reconstructed ear and any cartilage graft that may have been used for the framework of the ear. In addition, skin grafts are not required to restore the postauricularsulcus because the skin of the postauricular sulcus is left in situ by the interpolated flap technique

• A, Defect of inferior third of helix and antihelix

• B, Interpolated flap from postauricular skindesigned for reconstruction of ear.• Skin of postauricular sulcusleft undisturbed.

• C, First stage completed.• Interpolated flap sutured to lateralmargin of auricular defect.• Rubber band drain placed inpostauricular sulcus beneathpedicle of flap.

• D, One week after transfer of flap.

• E, Two months after transfer of interpolated flap.• Probe has been inserted beneathpedicle of flap in postauricular sulcus.• Hinge flap based on auricle isdesigned for reconstruction of ear.

• Traumatic avulsion of inferior two-thirds of auricleWith loss of skin of postauricular sulcus and medial ear:
• first surgical stage:• When the skin of the medial ear and postauricular sulcus is absent
from traumatic loss or from excision, the remaining auricle is sutured to the postauricular skin as the first surgical stage.
• When the ear has completely healed, a second stage is performed

• second surgical stage:
• a hinge flap based on the auricle is designed so that the flap can be constructed from the postauricular skin.
• Cartilage grafts are included during the second stage to provide a framework for the constructed ear.
• The donor site of the hinge flap is covered with a full-thickness skin graft harvested from the groin or supraclavicular fossa or closed with a scalp advancement flap

• A, Skin margin of antihelix wasSutured to postauricular skin margin.

• B, Hinge flap based on auricleis designed for reconstruction of ear.

• C, Hinge flap dissected.Auricular cartilage graft harvestedfrom contralateral ear insertedbeneath flap for framework.Full-thickness skin graft in place tocover donor defect of hinge flap.

• D, Hinge flap folded mediallyover cartilage graft and suturedto skin graft used to reconstructpostauricular sulcus.

• E, Postoperative result at 1 year.• No revision surgery performed


• Advantage of local flaps to skin grafts:• good color and texture match of the reconstructed auricle
Even if direct suturing is possible, care is needed to prevent distortion.(mobility of auricular skin is poor because its thin subcutaneous tissue)
• The auricle can be divided into three parts in consideration of reconstruction methods:
1. Concha2. Helix3. Ear lobe

• Strategy for partial auricular reconstruction:
• Concha : retroauricular flap
• Helix• Cartilage defect(-) :• Cartilage defect(+)• Defect less than 1.5cm :• Defect from 1.5cm to 3cm :• Defect about 1/3 of the helix :• Defect over 1/3 of the helix :
• Ear lobe : retroauricular chondrocutaneous flap

• A defect from 1.5 cm to 3.0 cm:
• A composite graft from the contralateral auricle is useful
• for using a composite graft the maximum size of a defect is 3 cm(because a defect of the donor site of more than 1.5 cm can not be directly sutured).
• in order to obtain sufficient blood supply:• The skin of the composite graft should be sutured to the skin of recipient
site (blood supply can usually be observed one day after the operation).
• Congestion may occur, but it usually improves after about 5 days.

• A defect about one-third of the helix:
• There are some reports of reconstruction using only a local flap without cartilaginous reconstruction, but post-operative deformity due to scar contracture may occur.
• Park reported a one-stage reconstruction method using• free cartilage graft• local flap• skin graft
but this method is slightly complicated.
• Reconstruction methods using a conchal chondrocutaneous flap are useful.• Cartilaginous reconstruction is necessary for such reconstruction.

• A defect of the upper one-third of the helix:
• Donelan reported a useful conchal chondrocutaneous flap:designed on the concha and elevated with conchal cartilage. Then the flap isrotated to the upper part of the helix.
(blood supply from the helical crus as a pedicle)
• The skin defect of the donor site of Donelan’s flap is covered with a skin graft.
• Yotsuyanagi covered a conchal skin defect with a retroauricular flap.
• The posterior surface of the reconstructed upper helix is covered with a retroauricular local flap.

• A defect of the middle one-third of the helix :• Several reconstruction methods using chondrocutaneous flaps have bee reported.• Millard reported a two-stage reconstruction method :
• using a conchal chondrocutaneous flap and local flaps.• Yotsuyanagi and Selçuk reported a one-stage reconstruction method.
• Yostuyanagi elevates the conchal chodrocutaneous flap as a subcutaneous flap and transfers it to the middle part of the helix. The conchal skin defect is covered with a retroauricular flap. The retroauricular skin defect is directly sutured if possible or covered with a local flap or skin graft.
• Selçuk reported a retroauricular chondrocutaneous transposition flap. The cartilage of the flap is revolved about 90 degrees in order to fit to the helical cartilaginous defect and covered with a skin flap.
• We usually use Yotsuyanagi’s method for a defect of the middle one-third of the helix because more cartilage can be transferred than that by Selcuk’s method, which is important for structural strength.




• A defect of more than one-third of the helix:
• It is difficult to reconstruct with local flaps only.
• In such cases, a costal cartilage graft is necessary to maintain the size and form of the auricle.
• The grafted costal cartilage should be covered with a vascularized flap as a temporoparietal fascial flap, and its surface is covered with a skin graft.
• It is important to make a cartilage frame that has a high helix and deep scapha to make a fine threedimensional structure.

• Strategy for partial auricular reconstruction:
• Concha : retroauricular flap
• Helix• Cartilage defect(-) : local flaps• Cartilage defect(+)• Defect less than 1.5cm : direct suture• Defect from 1.5cm to 3cm : composite graft• Defect about 1/3 of the helix : conchal chondrocutaneous flap + local flaps• Defect over 1/3 of the helix : costal cartilage graft + TPF + skin graft
• Ear lobe : retroauricular chondrocutaneous flap
(TPF : temporoparietal fascial flap )