Embed Size (px)
Citation preview

DR. AMIR BAHADUR
Re-absorption and Secretion by Nephron

Important to remember
Different types of cells and different structures at different parts of nephron causes different changes to the filtrate
Difference of osmolality in various parts of nephron causes changes to filtrate
Different hormones/chemicals exert their actions

Few basic facts
120mL/min-----GFR1mL/ min--------Urine formed119mL/min------Re-absorbed
172L/day---- filtered1.5L/day------urine formedApprox 170L---- re-absorbed

Filtrate
Water GlucoseAmino acidsBicarbonates SodiumChloridePhosphates

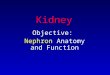
PCT structure

PCT--- series of events
On baso-lateral membrane are 3Na/ 2K ATPase. 3 Na out to interstitium, 2K inside to PCT cell
K- leaky channels---- K outside to insterstitium
Above two events, set the start by Negative electro-chemical state inside the PCT cell

Sodium in PCT
Concentration gradient for sodiumElectric gradient for sodiumSodium transporters (co-transporters)Facilitated transport Other arm of co-transporter can attach
glucose, chloride or amino acid.Sodium is transported from lumen to
PCT cells via facilitated diffusion65% sodium is re-absorbed in PCT

Glucose & Amino Acids in PCT
Co-transporters in the luminal brush border with one arm for sodium and other for glucose and amino acid.
Glucose and amino acids are transported via secondary active transport from lumen to the PCT cells.
100% of glucose and amino acids are re-absorbed in PCT.

Chloride in PCT
Chloride is re-absorbed by same way as glucose and amino acids.
Only difference is that preference is given to glucose and amino acid and later chlorine is take up.
Chloride re-absorption from lumen to PCT is secondary active transport.
65% of chloride is re-absorbed in PCT


Bicarbonate
Not really re-absorbedRather replaced hydrogen ions are transported from inside of
PCT to lumen of PCT via Na/H counter-transport
H combines with HCO3 in lumen to form carbonic acid which dis-associates to CO2 and H2O.
CO2 diffuse into PCT and combines with H2O to form H and HCO3 ions.
HCO3 are transported to interstitium.


Water
Trans-cellular by the solutesPara-cellular through tight junctionsAlso solutes go along with water through
tight junctions65% water is re-absorbed in PCT

Plasma proteins
Usually no plasma proteins are filtered.
If filtered, PCT brush border has affinity to get them attached
PINO-CYTOSIS and re-absorbed to PCT cell

Secretion in to PCT lumen
Oxalates Urates Bile salts Catecholamines ToxinsDrugs Secreted through special channels in the
baso-lateral surface. Transported across concentration gradient from capp to interstitium to PCT cell to Lumen.

Bit more in PCT
Minimal urea re-absorption across concentration gradient.
PTH---- phosphate trashing hormone--- inhibits phosphate re-absorption.
Angiotensin II acts on PCT and increases sodium re-absorption.
PCT cells also activates 25-hydroxy cholecalciferol to 1,25 di-hydroxy cholecalciferol

Leaving PCT
Same proportion of solutes and water are re-absorbed in PCT hence; the osmolality of filtrate entering and leaving PCT is SAME.
Though osmolality of the filtrate remains the same, quantity of water and solutes decreases.

Descending Loop of Henle
Cells are freely permeable to waterCells are minimally active metabolicallyNo brush border and not much of
ATPasesDescending limb is freely permeable to
water and interstitium is hyper-osmolar so water re-absorbed.
20% of water here.

Descending Loop of Henle
Water going out, solutes retained and further solutes coming in---- all across conentration gradient.
Filtrate is concentrated so much that filtrate osmolality equals that of interstitium.

Ascending Loop of Henle
Ascending Loop of Henle is totally impermeable to water up to half of distal convoluted tubule.
Hyper-osmotic filtrate reach thick part of ascending Loop of Henle

Thick part of ALOH
On the baso-lateral membrane of this part, 3Na/2K ATPases and they create negative gradient inside the cell.
The luminal membrane has Na-K-2Cl co-transporter which pumps 1 sodium, 1 pottasium and 2 chlorides in to the cells from lumen.
This sodium is pumped out in to the interstitium by the ATPases.
Chloride moves to interstitium via chloride channels.

Thick part of ALOH
K is getting in to the cell via Na/K ATPases and also by Na-K-2Cl co-transport.
Cell is TOO RICH in potassium. Potassium leaks to lumen via leaky channels
and make the lumen electro-positive. This electro-positivity of lumen created by
potassium excess repels the calcium and magnesium ions of the filtrate.
This repulsive force cause re-absorption of Ca and Mg through tight junctions.

Thick part of ALOH
Processes of re-absorbing solutes with out water causes…….
a)Increase of osmolality in interstitiumb)Decrease of osmolality in the tubules.
So this part is also called DILUTING SEGMENT

Thick part of ALOH
25% sodium is re-absorbed25% chloride is re-absorbedHow much water?

Loop diuretics
Frusemide Blocks Na-K-2Cl co-transport.More sodium going next partMore Ca and Mg going next partLess K going next part

Early Distal Convoluted Tubules
First half of EDCT have same roles as that of ALOH
Diluting segmentAt start of EDCT is present-------?
Mechanism of solutes re-absorption is bit different.

EDCT
3Na/2K ATPases at baso-lateral membrane
Na/Cl co-transport channels at luminal membrane instead of Na-K-2Cl co-transporters
EDCT cell is negative inside, Na poor cell5% Na is re-absorbed in DCT

Thiazide diuretic
Thiazide diuretics can block this Na/Cl co-transporter and causes diuresis
Weak diuretic Calcium conserving diuretic

EDCT---- calcium re-absorption
Para-thyroid hormonal acts on EDCT for re-absorption of calcium.
PTH increases the activity of calcium pump and Ca/Na exchanger at baso-lateral membrane and make cell calcium poor hence; increase calcium re-absorption via calcium channels.

Late DCT & Cortical Collecting tubules
Discussed together due to same properties
Principal cells and inter-calated cells

Inter-calated Cells
Inter-calated cells are special cells meant for hydrogen secretion.
H ions are produced in the inter-calated cells by decomposition of carbonic acid and H ion is transported to lumen by H-ATPases on luminal membrane.
HCO3 produced is supplied to circulation hence; called bicarbonate factory

Principal Cells
Baso-lateral membrane has 3Na/2K ATPases, making cells Na poor.
Luminal membrane has Na and K channels.
Na moves to the principal cells across electrical gradient.
Potassium moves out from cell to lumen through K channels across electrical gradient.

Principal Cells
Aldosterone acts on principal cellsIncreases the ATPases activity on baso-
lateral membrane, making cells more poor in Na and more rich in K
Also K channels are increased on luminal membrane
Na channels are also increased and Na re-absorption is increased.
Increased Na re-absorption, drag extra water as well.

K- sparing Diuretics
Spironolactone Blocks the action of aldosterone Less K is secreted to the lumen.
Amiloride/ triamterineBlock Na channelsLess K is secreted to the lumen

Principal Cells
Anti-diuretic Hormone (ADH)In absence of ADH, no water pores on
luminal membrane, water not absorbed.In presence of ADH, water pores on
luminal side apparent and water re-absorption increases.

Medullary Collecting Tubles
Some of the cells act as principal cells and some act as inter-calated cells.
Final tunning of urine osmolality. Special receptors for urea. Urea is transported to inerstitium via
concentration gradient which is taken in to the loop of Henle again and put in to the cycle again.