Embed Size (px)
DESCRIPTION
Radiological pathology of cerebrovascular disorders http://yassermetwally.com http://yassermetwally.net
Citation preview

Issues in Radiological pathologyCerebrovascular disorders
Neuroimaging and neuropathology share common perspectives in medicine. In no field is thismore evident than in the diagnosis and study of nervous system pathology: radiology andpathology are anatomically oriented specialties that depend primarily on structural changes todiagnose disease. Both specialties are broadening their perspectives of morphology todemonstrate metabolism, as with functional imaging in radiology and withimmunocytochemical markers in anatomical pathology. Pathologists thus regard theirradiologic counterparts as colleagues with similar morphologic approaches to diagnosis, despitethe different tools used. In no discipline is this companionship more strongly felt than in therespective subspecialties that focus on disorders of the nervous system.
2014
Professor Yasser Metwallywww.yassermetwally.com
1/1/2014
Issues in Radiological pathologyCerebrovascular disorders
Neuroimaging and neuropathology share common perspectives in medicine. In no field is thismore evident than in the diagnosis and study of nervous system pathology: radiology andpathology are anatomically oriented specialties that depend primarily on structural changes todiagnose disease. Both specialties are broadening their perspectives of morphology todemonstrate metabolism, as with functional imaging in radiology and withimmunocytochemical markers in anatomical pathology. Pathologists thus regard theirradiologic counterparts as colleagues with similar morphologic approaches to diagnosis, despitethe different tools used. In no discipline is this companionship more strongly felt than in therespective subspecialties that focus on disorders of the nervous system.
2014
Professor Yasser Metwallywww.yassermetwally.com
1/1/2014
Issues in Radiological pathologyCerebrovascular disorders
Neuroimaging and neuropathology share common perspectives in medicine. In no field is thismore evident than in the diagnosis and study of nervous system pathology: radiology andpathology are anatomically oriented specialties that depend primarily on structural changes todiagnose disease. Both specialties are broadening their perspectives of morphology todemonstrate metabolism, as with functional imaging in radiology and withimmunocytochemical markers in anatomical pathology. Pathologists thus regard theirradiologic counterparts as colleagues with similar morphologic approaches to diagnosis, despitethe different tools used. In no discipline is this companionship more strongly felt than in therespective subspecialties that focus on disorders of the nervous system.
2014
Professor Yasser Metwallywww.yassermetwally.com
1/1/2014

Neuroimaging is nothing but how "neuropathology and neuroanatomy" are approached clinically by neurologists andneurosurgeons through radiological films. Neuroimaging from the neuropathological and neuroanatomical perspectives ishow gross pathology and anatomy are demonstrated radiologically. Without having a good Knowledge of neuropathologyand neuroanatomy it is not possible at all to understand neuroimaging.
Neuroimaging and neuropathology share common perspectives in medicine. In no field is this more evident than in thediagnosis and study of nervous system pathology: radiology and pathology are anatomically oriented specialties thatdepend primarily on structural changes to diagnose disease. Both specialties are broadening their perspectives ofmorphology to demonstrate metabolism, as with functional imaging in radiology and with immunocytochemical markersin anatomical pathology. Pathologists thus regard their radiologic counterparts as colleagues with similar morphologicapproaches to diagnosis, despite the different tools used. In no discipline is this companionship more strongly felt than inthe respective subspecialties that focus on disorders of the nervous system.
Neuropathologists understand, acknowledge, and admire the numerous contributions by neuroimaging in defining manyneurological disorders. Neuroimaging enable us to diagnose gross pathology during life. Neuropathologists usually mustwait until autopsy to demonstrate tissue changes, but surgical specimens are becoming increasingly more frequent, forexample, with the advent of epilepsy surgery.
Neuroradiologists and neuropathologists have a mutual need for collaboration. Radiologists need tissue confirmation tofully understand the significance of images seen, and pathologists' findings need to be relevant to diagnoses that often restinitially with the neurologist/neuroradiologist, and provide insight into pathogenesis through unique tissue examinations.
In my opinion the best neuroradiologist is the neurologist or the neurosurgeons who must be capable of independentlyinterpreting a neuroimaging study. Understanding neuropathology and neuroanatomy, and how they are demonstratedradiologically, are essential for interpreting a neuroimaging study. This EBook is directed primarily to neurologists andneurosurgeons. In this PDF publication, neuroimaging of cerebrovascular disorders is approached from theneuropathological and neuroanatomical perspectives. This publication addresses the question of how neuropathology andneuroanatomy are related to neuroimaging and why they are essential for our basic understanding of a neuroimagingstudy.
This publication covers cerebrovascular disorders from the radiological pathology point of view. The publication is free ofcharge and can be freely distributed. I certainly hope that you will find this publication as useful as I truly wish.
Professor Yasser Metwallywww.yassermetwally.com
My web site | My face book page | My video channel | The online newspaper
© yassermetwally.com corporation, all rights reserved

INDEX
Radiological pathology of embolic cerebral infarction
Radiological pathology of hemorrhagic infarction
Radiological pathology of watershed infarction
Radiological pathology of cortical laminar necrosis
Radiological pathology of microvascular cerebral hemorrhage
Radiological pathology of cerebral microbleeds
Radiological pathology of spontaneous cerebral hemorrhage
Radiological pathology of amyloid cerebral angiopathy
Radiological pathology of ischemic microvascular brain diseases
Radiological pathology of transient ischemic attacks
Radiological pathology of cerebral aneurysms
Radiological pathology of multi-infarct dementia
Radiological pathology of cerebral veno-sinus thrombosis
My web site | My face book page | My video channel | The online newspaper
© yassermetwally.com corporation, all rights reserved

INTRODUCTION CT FINDINGS IN ACUTE STROKE VASCULAR FINDINGS IN ACUTE
INFARCTION PARENCHYMAL CHANGES OF ACUTE
INFARCTION RADIOLOGICAL PATHOLOGY OF OLD
INFARCTION THROMBOLYSIS: WHO AND WHEN TO
TREAT
RADIOLOGICAL PATHOLOGY OF CEREBRAL INFARCTION
Stroke is the number three cause of mortality in the adult population and affects more than400,000 people in the United States annually. 8,23 Ischemic infarcts account forapproximately 85% of all strokes. Previously the medical management of infarctsprimarily involved diagnosis, stabilization during the acute period, and subsequentrehabilitation. As a result of the development of new therapy options, includingthrombolytic agents and brain-protective drugs, stroke is increasingly becoming a treatablecondition. These treatment choices have created a significant impetus for the early clinicaland radiographic detection of acute infarcts.
Although magnetic resonance (MR) imaging has been shown to be more sensitive thancomputed tomography (CT) in detecting acute strokes within the first 24 hours, CTremains the emergent imaging test of choice to evaluate acute ischemia. It is fast,noninvasive, and readily available in almost all hospitals. Despite its limitations, CTcontinues to be used for all major stroke therapy trials. Until other methods of stroke
Professor Yasser Metwallywww.yassermetwally.com
INDEX
1

imaging, such as xenon CT and MR diffusion/perfusion, become widely and rapidlyavailable in most institutions, CT remains the primary screening tool for acute ischemia.
CLINICAL IMPORTANCE OF EARLY STROKE DETECTION BY CT
Two major drug trials testing the safety and efficacy of early thrombolytic therapy havebeen completed in the past 4 years. Although both studies demonstrated improved clinicaloutcomes after the administration of intravenous thrombolytic drugs, the results weredependent on the appropriate screening of potential patients. The National Institute ofNeurological Disorders (NINDS) and Stroke rt-PA Stroke Study Group treated 624 acutestroke patients with either intravenous recombinant human tissue plasminogen activator(tPA) or placebo within 3 hours of the onset of Symptoms. Despite an overall increasedincidence of symptomatic intracerebral hemorrhage in the therapeutic group, this studydemonstrated an improved clinical outcome with thrombolytic therapy without asignificant difference in mortality. Patients treated with tPA were 30% more likely to haveminimal or no disability at 3 months compared with patients given a placebo.
Further analysis of the NINDS data demonstrated that intracranial hemorrhage was amore common complication in patients with edema or infarct on the initial scan, occurringin 31% of these patients compared with 6% of cases without early CT findings. 24 Despitethis complication, this subset of patients was still more likely to have an improved clinicaloutcome at 3 months. The study therefore concluded that patients with edema or masseffect on the baseline CT were candidates for tPA if it was administered within 3 hours ofthe onset of symptoms.
A second study was conducted by the European Cooperative Acute Stroke Study (ECASS).12 This group treated 620 stroke patients with either intravenous thrombolytic agent orplacebo within 6 hours after the onset of symptoms. Patients with evidence of majorischemic changes, defined as hypoattenuation lesions involving greater than 33% of themiddle cerebral artery (MCA) territory already visible at the time of the first scan, were tobe excluded from the protocol. Fifty-two patients with CT findings of extended infarctswere incorrectly admitted into the study because of misinterpretation of the initial film.These patients had no beneficial effect from intravenous tPA and demonstrated a mildincreased rate of fatal cerebral hemorrhage compared with the remaining population. The215 patients with small hypoattenuation lesions experienced an increased chance of goodoutcome if treated with intravenous thrombolytic therapy. ECASS originally concludedthat although intravenous thrombolytic therapy was effective in improving neurologicoutcome in a subset of patients with moderate to severe neurologic deficit and no evidenceof extended infarct on CT scan, its use was not recommended because of difficulty inidentifying this subgroup and the associated unacceptable risk of increased hemorrhagiccomplications and death. 12
A subsequent reanalysis of the ECASS data, which correctly reclassified the patients withextended ischemic changes, demonstrated that (1) response to tPA is different for patientswith no, small, or large areas of edema visible on initial CT 45 and (2) patients with largeischemic zones already apparent on the initial CT scan most likely will not benefit from
Professor Yasser Metwallywww.yassermetwally.com
2

thrombolytic therapy. 42 Treatment with tPA significantly increased the cure rate ofpatients with no or small cytotoxic edema by 8% and 18% but decreased the cure rate to6% for patients with large cytotoxic edema. If patients with extended infarcts alreadypresent on the initial scans are excluded from the treatment population, the probability ofclinical improvement with thrombolytic therapy increases.
The results of these two studies underscore the importance of careful clinical andradiologic screening before the administration of thrombolytic drugs. Although tPA has thepotential to improve clinical outcomes of patients with acute strokes, the drug must begiven to the appropriate population within a relatively small time window. If treatment isdelayed or CT scans are not accurately interpreted, the potential benefits of thrombolytictherapy can be negated.
CT FINDINGS IN ACUTE STROKE
When reviewing the CT scan of potential stroke patients, the radiologist shouldsystematically answer several questions that determine the patient's medical management.Can the cause of the neurologic problem be identified on the scan? Are the findingsconsistent with an acute ischemic infarct, or is there another abnormality? Manyneurologic disorders can mimic an acute infarct, including tumors, subdural hematomas,hemorrhages from underlying masses or vascular malformations, and venous occlusivedisease. These diagnoses can often be excluded on noncontrast CT scans; however,additional imaging, including contrast-enhanced CT or MR examinations, may be neededto confirm the diagnosis.
When the diagnosis of ischemic infarct is suspected, careful review of the film for evidenceof major arterial occlusion, early parenchymal edema, or hemorrhage is indicated. Thesefindings help determine if thrombolytic therapy is indicated and may influence how it isadministered, either intravenously or intraarterially. Identification of hemorrhage iscrucial because its presence precludes thrombolytic therapy.
VASCULAR FINDINGS IN ACUTE INFARCTION
Asymmetric hyperdensity within a major cerebral artery represents one of the earliest CTsigns of stroke and is caused by occlusion of the vessel from either an embolus or athrombus. 10,28,33 The density of blood on CT is linearly related to the hemoglobinconcentration. Flowing blood has a density of approximately 40 Hounsfield units (HU) witha normal range of 35 to 60 HU . When a thrombus or embolus occurs, serum is extrudedfrom the clot producing an increase in the hemoglobin concentration and a subsequentincrease in density. 22 Intraluminal thrombus measures approximately 80 HU with a rangeof 77 to 89 HU. Atheromatous vessels typically have higher densities because of thepresence of wall calcification and usually measure between 114 and 321 HU.
Professor Yasser Metwallywww.yassermetwally.com
3

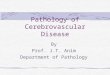
Figure 1. Hyperdense middlecerebral artery sign. A,Noncontrast axial CT scandemonstrates a linear focus ofhyperdensity in the region of theleft middle cerebral arteryrepresenting an embolus (arrow).B, Left common carotidangiogram performed twentyhours after the ictusdemonstrates complete occlusionof the middle cerebral artery atits origin (arrow). Minimalcortical collaterals are noted onthis late arterial phaseangiogram.
The hyperdense artery sign has been described primarily in the MCA and basilar artery.Because of their extended courses through the subarachnoid space, these arteries are easilyvisualized and can be directly compared with other arterial and venous structures. A fewcases of calcified emboli to the anterior cerebral artery have been reported; however,noncalcified occlusion of the anterior cerebral distribution is rarely detected.46 Hyperdensecerebral arteries usually resolve within 1 week secondary to lysis of the clot andrecanalization of the vessel.
Professor Yasser Metwallywww.yassermetwally.com
4

Figure 2. A 62-year-old man who presented with suddenonset of left hemiparesis and confusion. A, Noncontrast axialCT scan performed 90 minutes after the onset of symptomsdemonstrates a linear hyperdensity in the region of the rightmiddle cerebral artery (arrow) consistent with a hyperdensemiddle cerebral artery sign. Compare with the normaldensity of the left middle cerebral artery. B, A more superiorimage of the initial scan demonstrates loss of the insularribbon (arrows) consistent with early ischemic change in theright MCA distribution. Bilateral remote occipital infarctsare also noted. The patient was started on IV thrombolytictherapy; however, one hour after the infusion began, thepatient developed hypotension and seizure activity. A repeatCT scan was performed to evaluate for possible hemorrhage.C, Noncontrast CT scan performed three hours after ictusdemonstrates obscuration of the right lenticular nucleirepresenting progression of ischemic change. D, CT scanperformed 24 hours later demonstrates a large infarctinvolving the majority of the right middle cerebral arterydistribution producing mild mass effect.
Professor Yasser Metwallywww.yassermetwally.com
5

Figure 3. A thrombosedmiddle cerebral artery(arrow) that commonlygives the characteristichyperdense MCAradiological sign
The hyperdense MCA sign (HMCAS) has been well described in the literature as one of theearliest signs of MCA infarct. It is associated with occlusion of the proximal MCA or itsbranches and has been identified in 35% to 50% of patients presenting with clinical signsof acute MCA stroke. 2,36,43
Proximal MCA occlusion is one of the most serious cerebrovascular occlusive conditions.Mortality associated with MCA occlusion can range from 5% to 45%, and survivorstypically have severe neurologic deficits.17,32,43 If collateral circulation is inadequate, thesestrokes can produce malignant brain edema, uncal herniation, and subsequentcompression of the midbrain. Rapid detection and early, aggressive treatment of proximalMCA occlusion is indicated to reduce both mortality and morbidity.
Studies have demonstrated that the HMCAS predicts a poorer clinical outcome comparedwith patients without the sign. 19,31 Occlusion of the proximal Ml segment of the MCAcorrelates with an infarct of 100 mL or greater in the majority of cases.36Tomsick etal35noted that the HMCAS is associated with a poor response to intravenous thrombolytictherapy. Clinical follow-up performed 3 months after intravenous tPA demonstrated thatpatients with a positive HMCAS had larger infarcts and were significantly less likely to becompletely neurologically improved compared with the patients without an HMCAS. Theseresults indicate that patients with an HMCAS, if detected before the formation of extensiveparenchymal ischemic changes, may benefit from more aggressive initial treatment, such asintra-arterial thrombolysis.
Several conditions may mimic a hyperdense thrombosed vessel, including a highhematocrit or vessel wall calcification. To prevent false-positive results, the radiologistshould closely adhere to a narrow definition of HMCAS. The HMCAS is defined as anMCA that is denser than its counterpart and denser than any visualized vessel of similar
Professor Yasser Metwallywww.yassermetwally.com
6

size that is not attributable to vessel calcifications.30 Using this definition, the HMCAS is anaccurate and moderately sensitive tool in detecting early MCA occlusion. In a blindedanalysis performed by six neuroradiologists, Tomsick et al, 37 demonstrated a sensitivity of78%, specificity of 93%, and accuracy of 91% for the HMCAS.
PARENCHYMAL CHANGES OF ACUTE INFARCTION
Pathophysiology
The CT detection of acute infarcts depends on the development of edema within the brainparenchyma, which produces subtle density changes and mass effect. To understand betterthe CT findings of acute ischemia, a brief review of the histologic changes that occur duringa stroke are presented.
Table 1. Pathological stages of cerebral infarctio
Time Gross pathology Microscopical pathologyFrom 8-18Hr
The damaged zone become pale, andthe demarcation between the whiteand gray matter is indistinct.Edematous swelling is apparent andaccompanied by cortical congestion.At this stage the infarcted area issoft in consistency.
Ischemic neuronal death, withcapillary endothelial swellingaccompanied by exudation ofedematous fluid and extravasation ofRBCs even in anemic infarction
2- 10 days The edema and the swelling persistbut to a decreasing degree and theinfarcted zone becomes friable andits boundary becomes betterdefined.
Stage of phagosytic acivity andparenchymatous liquefaction:
Exudation of neutrophil leukocytesbegins for a brief time and causesinflammatory reaction and is replacedon the second day by macrophagesladen with Sudanophilic breakdownproducts originating fromdisintegration of myelin sheaths.Macrophage activity becomes mostmarked from the 5th to the 30th dayi.e. during the phase ofparenchymatous liquefaction
After 10 days liquefaction begins and after 3weeks cavitations becomes moreevident. From then on the necrotictissues is replaced by yellowishtissue which causes depression of thecerebral cortex.
After severalmonths
A cystic cavity is organized, thecavity has ragged outlines and isintersected by vascular connectivetissues strands and is covered on itsouter surface by a thin meningealmembrane .
Stage of cicatrization:The residualcystic cavity becomes surrounded by glialproliferation which is first protoplasmicand then fibrillary (astrogliosis) withfrequent vascular connective tissuesstrand that run across the cavity
Professor Yasser Metwallywww.yassermetwally.com
7

Normal cerebral blood flow ranges from 50 to 60 mL/100 g tissue/min. During an ischemicinfarct, blood supply to a portion of the brain is significantly reduced. As cerebral bloodflow decreases, injury occurs in the brain progressing from electrical dysfunction toreversible cellular damage and eventually to cell death. At approximately 20 mL/100 g,electrical activity in the brain ceases, and water homeostasis begins to be disrupted. 13,16 Atcritical flow rates of 10 to 15 mL/100 g, there is disruption of ion homeostasis within thecells producing rapid increases of extracellular potassium and intracellular sodium. 5,15
This disruption causes water to shift into the intracellular compartment producingastrocytic swelling (cytotoxic edema).
The development of cytotoxic edema aggravatesischemia by causing progressive compression of themicrocirculation, which further decreases blood flow.29As the ischemic changes worsen, capillary wallsbecome permeable allowing leakage of intracellularproteins and subsequent accumulation ofextracellular water (vasogenic edema).25 Worseningedema produces additional mass effect causing a
decrease in cerebral perfusion pressure and collateral flow. Cytotoxic edema may bedetectable within 1 hour of the onset of stroke; however, vasogenic edema usually does notdevelop until 6 hours or more after ictus.
Figure 4. Acute infarctions with mass effect due to edema
Severe ischemia can cause a 7 to 8HU change at I hour that should bevisible on CT. With marginal cerebralblood flows between 15 and 20mL/100 g, ischemic edema takeslonger to develop and may not bedetected on early CT scans.
Professor Yasser Metwallywww.yassermetwally.com
8

Table 2. Comparison between the cytotoxic and vasogenic edema of recent infarction
Parameter Cytotoxic (intracellular) Vasogenic (extracellular)Time Within 1 hour of the onset of stroke Does not develop until 6 hours or
more after ictus.Pathophysiology At critical flow rates of 10 to 15
mL/100 g, there is disruption of ionhomeostasis within the cellsproducing rapid increases ofextracellular potassium andintracellular sodium. This disruptioncauses water to shift into theintracellular compartment producingastrocytic swelling (cytotoxic edema).
The development of cytotoxicedema aggravates ischemia bycausing progressive compressionof the microcirculation, whichfurther decreases blood flow. Asthe ischemic changes worsen,capillary walls become permeableallowing leakage of intracellularproteins and subsequentaccumulation of extracellularwater (vasogenic edema).
Composition Increased intracellular water andsodium
Plasma filtrate including plasmaproteins
Location ofedema
Gray and white matter Chiefly white matter
Pathology Cellular swelling, usually ofastrocytes in the grey matter.
Grossly , the gyri are flattened andthe sulci narrowed; the whitematter is moist and swollen.Microscopically, there is micro-vacuolization of the white matter,poor staining, and "halo's"around nuclei.
Capillarypermeability tolarge molecules
Normal Increased
Neuroimaging Normal (1) obscuration of the lentiformnucleus, (2) loss of the insularribbon, (3) diffuse low densitywith loss of the gray-whiteinterface, and (4) sulcaleffacement, (5) mass effect
Professor Yasser Metwallywww.yassermetwally.com
9

Figure 5. A, In vasogenicedema the gyri areflattened and the sulcinarrowed; the whitematter is moist andswollen. B, left sided acuteembolic brain infarction,showing evidence of brainedema with mass effect,flattened gyri and sulcaleffacement.
Ischemic changes that occur above 15 mL/ 100 g can be reversible. At flow rates below 10to 15 mL/100 g, tissue damage is usually irrevocable after 1 hour of hypoperfusion.16Otherfactors also play a role in the reversibility of ischemic changes. During low levels ofperfusion, small amounts of glucose may be available to brain tissue for glycolysis, butoxidation cannot occur. The subsequent development of lactic acidosis adversely affects theviability of brain tissue. 27
Sensitivity of CT in Evaluating Acute Ischemia: How Early Can Stroke BeDetected?
How quickly an acute infarct can be visualized is governed primarily by the severity ofhypoperfusion; however, the duration, size, and location of ischemia also play importantroles.21When cerebral blood flow drops below the critical value of 10 to 15 mL/100 g,ischemic changes are usually irreversible, and edema develops fast, permitting earlydetections. 15
As edema progresses, water content within the parenchyma increases. This increase causesa subsequent decrease in the brain's specific gravity, which is linearly proportional to CTattenuations. 26 In other words, as edema increases, brain density proportionatelydecreases. A 1 % change in water content changes the CT attenuation by 2.6 HU. Typicallya change of 4 HU or greater is needed to detect the change visually. In cases of severeischemia caused by proximal MCA occlusion, cytotoxic edema can produce a 3% increasein water within 1 hour of the onset of Symptoms. 3,11
This can increase to 6% at 2 to 4 hours. 29 Therefore, severe ischemia can cause a 7 to 8 HUchange at I hour that should be visible on CT. With marginal cerebral blood flows between
Professor Yasser Metwallywww.yassermetwally.com
10

15 and 20 mL/100 g, ischemic edema takes longer to develop and may not be detected onearly CT scans.
In the future, more advanced imaging techniques, such as MR perfusion and xenon CT,may play an important role in determining the cerebral blood flow of ischemic areas tohelp determine tissue viability. Until then, noncontrast CT can provide importantinformation. If hypoperfusion is less severe and collaterals to an ischemic area areadequate, edema may not develop, and early CT scans are negative. 24 Conversely thepresence of more extensive edema on an early CT scan indicates severe hypoperfusion andmay predict a less favorable outcome after thrombolytic therapy.
The sensitivity of early CT scans in detecting acute strokes also depends on the duration,location, and size of the infarct. As the time of ischemia increases, CT abnormalitiesbecome more obvious; however, the absolute presence or absence of edema primarily relieson the severity of hypoperfusion and adequacy of collateral circulation. Larger infarcts arevisible earlier than smaller infarcts because of the increased volume of tissue involved (i.e.,MCA infarcts are detected sooner than small cortical or lacunar infarcts). 45
Several researchers have studied the sensitivity and accuracy of detecting infarcts on CT.Bryan et al 6 performed MR imaging and CT scans on 31 stroke patients within 24 hours ofthe onset of their symptoms. The locations of the infarcts included the posterior fossa aswell as supratentorial cortical, subcortical, and combined lesions. Eighty-two percent ofearly MR imaging scans showed an abnormality compared with 58% of CT scans. Onfollow- up examinations performed 7 to 10 days later, approximately 90% of both MRimaging and CT scans were abnormal. Mohr et al 20 demonstrated that although CTshowed deep and brain stem infarcts less often than MR imaging, it was equally sensitive indetecting convexity lesions.
When analysis is restricted to the assessment of MCA infarcts, the overall sensitivity of CTsignificantly increases. Moulin et al 21 reviewed 100 patients with MCA stroke. Ninety-fourpercent of all CT scans performed within 14 hours after the onset of symptoms wereabnormal; 88% of CT scans obtained within 6 hours of ictus were abnormal. These resultscompare favorably with data of von Kummer et al. A review of 44 patients demonstratedthat CT performed within 6 hours of the onset of symptoms has an accuracy of 95% and amean sensitivity of 82% of detecting MCA infarcts. CT scans performed within the first 2hours of symptoms, however, were much less sensitive in detecting early ischemia. Truwitet al 40 and Tomura et al 38described subtle findings of MCA stroke that can increase thesensitivity of CT to greater than 90% in detecting major MCA occlusions.
The presence of parenchymal changes on early CT scans also correlates with the degree ofintracranial occlusive disease. Horowitz et al 14 studied 50 patients with ischemic strokesthat produced at least hemiparesis. CT scans were performed within 4 hours of ictus andwere correlated with angiography or carotid ultrasound. Acute CT abnormalities,including hypodensities and mass effect, were seen in 56% of patients. When there wasmajor vascular occlusion, however, either occlusion of the MCA trunk or two or moreMCA branches, the CT scan was positive in 86% of cases
Professor Yasser Metwallywww.yassermetwally.com
11

CT Findings
Several articles describing early CT findings of acute infarcts have been published inrecent years. These findings have primarily focused on MCA ischemia and havesignificantly improved the overall sensitivity of CT in detecting early MCA infarcts. Themajor CT findings of acute MCA stroke include (1) obscuration of the lentiform nucleus,(2) loss of the insular ribbon, (3) diffuse low density with loss of the gray-white interface,(4) sulcal effacement, (5) gray matter enhancement and (6) hemorrhagic infarction
o Obscuration of the Lentiform Nucleus.
In 1988, Tomura et al 38 described obscuration of the lenticular nucleus as an early sign ofMCA infarct. This finding is caused by cellular edema arising within the basal ganglia andclosely correlates with a proximal MCA occlusion. Twenty-five patients who had clinicalevidence of MCA infarcts underwent CT scanning within 6 hours of the onset of symptoms.The scans were then retrospectively reviewed for obscuration of the lenticular nuclei aswell as decreased density within the brain parenchyma and sulcal effacement. Twentythree of the patients (92%) demonstrated an obscured outline or partial disappearance ofthe lentiform nucleus. This sign was visualized earlier than other CT findings and in a fewcases was present within 1 hour after the onset of the stroke. Parenchymal hypodensitiesand sulcal effacement occurred later and were present on significantly fewer initial scans.
The lenticular nuclei receive their blood supply from the lenticulostriate arteries whicharise from the MI trunk of the MCA. Collateral circulation to this area is poor comparedwith the cortex. Occlusion of the proximal MCA disrupts the primary blood supply to thesestructures. 7 As a result of the insufficient collaterals as well as the relatively high metabolicrate of the lenticular nuclei, 5 proximal MCA occlusion can quickly cause critically lowcerebral blood flow, which produces early ischemic changes on CT.
Firlick et al 9 performed CT, xenon CT, and angiography on 20 patients with acute MCAinfarcts. Early CT changes in the basal ganglia were associated with significantly lowercerebral blood flows in the MCA territory compared with patients with normal CT scans.An early basal ganglia hypodensity correlated with a mean cerebral blood flow in theaffected MCA territory of less than 10 mL/100 g. Patients with more distally locatedocclusions, beyond the origins of the lenticulostriate arteries, preserve blood supply to thebasal ganglia and do not develop this early sign.
Bozzao et al 4 evaluated 36 patients with acute MCA infarcts with CT and angiography andcorrelated changes on early CT scans with the angiographic findings. CT scans wereperformed within 4 hours, and angiograms were obtained within 6 hours from the onset ofsymptoms. Bozzao et al, 4 noted that all patients with early CT findings of MCA infarctsdemonstrated an arterial occlusion on angiography. Involvement of the lenticular nucleicorresponded closely with a proximal MCA occlusion.
Professor Yasser Metwallywww.yassermetwally.com
12

o Loss of the Insular Ribbon. (LIR)
Another early sign of acute MCA infarction is loss of the insular ribbon (LIR) which isdescribed as loss of definition of the gray-white interface in the lateral margins of theinsula. This area is supplied by the insular segment of the MCA and its claustral branchesand is the region most distal from anterior and posterior cerebral collateral circulation. Asa result, collateral flow to the insular region is decreased compared with other portions ofthe cerebral cortex.
Truwit et al 40 performed both retrospective and prospective evaluations of CT scans inpatients with clinical evidence of acute MCA distribution infarcts to evaluate the sensitivityand accuracy of the LIR sign. In a retrospective analysis of 11 cases, LIR was seen in allpatients (100%). In a prospective study, the LIR sign was identified in 12 of 16 patients(75%). Obscuration of the lenticular nucleus occurred less frequently and was identified in73% and 63% of patients. They concluded that LIR is more frequently observed in acuteMCA infarcts than other early CT findings.
In two patients, the LIR was localized to the posterior segment of the insula and wasassociated with a more limited infarct . This situation may be due to more distal occlusionof posterior MCA branches within the operculum.
The presence of obscuration of the lenticular nucleus or LIR without other signs ofextensive infarct does not preclude the use of thrombolytic agents. These patients mayreceive significant benefit from intravenous or intraarterial thrombolysis; because of thepresence of early CT changes, however, they may be more likely to have areas ofirreversible damage compared with patients with negative CT scans.
o Diffuse Parenchymal Hypodensity and Sulcal effacement.
As ischemic changes progress, both cytotoxic and vasogenic edema increase producingareas of hypoattenuation throughout the affected circulation. In larger infarcts, mass effectalso increases producing effacement of sulci and compression of ventricles.
Figure 6. A 52-year-old woman whopresented with sudden onset of leftarm weakness. A and B, CT scanperformed three hours after the onsetof symptoms demonstrates focal lossof the insular ribbon posteriorly(arrows). A more superior imageperformed through the lateralventricles demonstrates an area oflow attenuation in the right posteriorfrontal cortex with loss of the gray-white interface (arrows) consistentwith ischemic change in the rightMCA distribution.
Professor Yasser Metwallywww.yassermetwally.com
13

Detection of anterior and posterior cerebral artery infarcts as well as posterior fossa lesionsrelies predominantly on the presence of parenchymal hypodensity and sulcal effacement.As a result of the lack of other subtle CT findings, such as obscuration of the lenticularnucleus and LIR, these infarcts may not be detected as early as large MCA strokes.
In cases of MCA infarcts, extensive parenchymal hypodensity on early CT scans isassociated with a high mortality rate as well as a poor clinical outcome in survivors. Whengreater than 50% of the vascular territory was involved, the mortality rate increased up to85% because of malignant brain edema. 43 Early craniectomy decreases the mortality ratefor patients with severe edema ; however,clinical outcome remains poor.
Figure 7. A 67-year-old man who presented with a 5-hour history of left leg weakness. Aand B, CT scan shows subtle low attenuation and loss of sulcation in the right parasagittalfrontal lobe extending to the convexity (arrowheads) consistent with an anterior cerebralartery distribution infarct. C, MR diffusion scan demonstrates abnormal high signal in theright frontal parasagittal region confirming the diagnosis of an ACA infarct.
The presence of extensive ischemic change typically excludes the use of thrombolytictherapy. 42 The likelihood of clinical improvement is low, whereas the rate of complication,including hemorrhage, is significantly increased. 18,43,47In the future, faster mechanicalmethods of removing clot within the MCA may offer benefit to these patients; however, inmost cases, irreversible damage has been done.
Professor Yasser Metwallywww.yassermetwally.com
14

TABLE 3. EARLY CT SCAN FEATURES OF HYPERACUTE ISCHEMIC STROKE
RADIOLOGICALFEATURE
DESCRIPTION
Hyperdensethrombosed vessel,
When a thrombus or embolus occurs, serum is extruded from theclot producing an increase in the hemoglobin concentration and asubsequent increase in density. The hyperdense MCA sign(HMCAS) has been well described in the literature as one of theearliest signs of MCA infarct. It is associated with occlusion of theproximal MCA or its branches and has been identified in 35% to50% of patients presenting with clinical signs of acute MCA stroke.It is defined as an MCA that is denser than its counterpart anddenser than any visualized vessel of similar size that is notattributable to vessel calcifications .
Diffuse ParenchymalHypodensity andSulcal effacement.
A 1 % change in water content changes the CT attenuation by 2.6HU. Typically a change of 4 HU or greater is needed to detect thechange visually. In cases of severe ischemia caused by proximalMCA occlusion, cytotoxic edema can produce a 3% increase inwater within 1 hour of the onset Of Symptoms. This can increase to6% at 2 to 4 hours. Therefore, severe ischemia can cause a 7 to 8HU change at I hour that should be visible on CT. If hypoperfusionis less severe and collaterals to an ischemic area are adequate,edema may not develop, and early CT scans are negative.Conversely the presence of more extensive edema on an early CTscan indicates severe hypoperfusion and may predict a lessfavorable outcome after thrombolytic therapy.
Loss of the InsularRibbon. (LIR)
Loss of definition of the gray-white interface in the lateral marginsof the insula .
Obscuration of theLentiform Nucleus.
Obscuration of the lenticular nucleus is an early sign of MCAinfarct . This finding is caused by cellular edema arising within thebasal ganglia and closely correlates with a proximal MCAocclusion.
o Gray matter enhancement (GME)
One early pattern seen with MRI is areas of increased signal intensity (long T2) involvingcortical and deep gray matter structures. This may be demonstrating the selectivevulnerability of these structures to ischemia and hypoxia. A CT correlate of this MRIfinding may be the inconsistently visualized regions of gray matter enhancement (GME).To date, nearly all cases of GME visualized by CT have shown a corresponding area ofincreased signal (long T2) by MRI. This long T2 abnormality, corresponding to the region,of GME may persist for years although a frank area of infarction may not be demonstrableby CT.
Professor Yasser Metwallywww.yassermetwally.com
15

o Hemorrhagic infarction
This type of infarction is regarded as distinct from anemic infarction althoughmicroscopical haemorrhage is frequent in the later. It has frankly hemorrhagic featureswhich consist of petechial zones that are frequently confluent and are situated in the cortex.These hemorrhagic areas may involve the entire infarction but tend most often to involvethe boundary zones supplied by meningeal arterial anastomosis or, in case of middlecerebral infarct, in the basal ganglia. Hemorrhagic infarction is secondary corticalreirregation which takes place in the capillary blood vessels that have been damaged by theinitial hypoxia. Reirregation takes place when lysis (natural or by therapeuticthrombolysis) or secondary mobilization of the thrombus takes place.
Figure 8. Haemorrhagic infarctions. They have frankly hemorrhagic features which consistof petechial zones that are frequently confluent and are situated in the cortex.
Professor Yasser Metwallywww.yassermetwally.com
16

Figure 9. A, Plain CT scan showing middle cerebral artery hemorrhagic infarction, noticepetechial zones situated in the basal ganglia, B, MRI T2 image showing a left sidedhemorrhagic infarction, notice cortical hypointense petechial zones composed mainly of
deoxyhemoglobin
o Fogging effect
Fogging is the temporary loss of visibility of an infarct on CT which occurs in the subacutephase at about 2 weeks after stroke. It occurs in up to 40% of medium to large infarcts onCT. Cerebral infarcts therefore may be overlooked or grossly underestimated if the scan isperformed during the second and third week after stroke. 51,52,53
Increase of x-ray attenuation on day 10 is known as the fogging effect and appears to be afavorable prognostic factor. Fogging is generally considered to be due to macrophageinvasion and proliferation of capillaries within the infarct area, but probably alsorepresents partial restoration of some viable tissue. 51,52,53
Professor Yasser Metwallywww.yassermetwally.com
17

Figure 10. A, Initial CT scan examination showed multiple small hypodense lesions in theright parieto-temporo-occipital lobes, left occipital and left frontal lobe representing acuteinfarcts. B, Repeated CT examination 10 days later in the same patient as (A) showed thatthe lesions are no longer apparent (fogging effect)
o Gyral Enhancement
Superficial enhancement of the brain parenchyma is usually caused by vascular orinflammatory processes and is only rarely neoplastic. Vascular causes of serpentine (gyral)enhancement include vasodilatation after reperfusion of ischemic brain, the vasodilatationphase of migraine headache, posterior reversible encephalopathy syndrome (PRES), andvasodilatation with seizures. Serpentine enhancement from breakdown of the blood-brainbarrier is most often seen in acutely reperfused cerebral infarction, subacute cerebralinfarction, PRES, meningitis, and encephalitis. The primary distinction between vascularand inflammatory causes of the serpentine pattern of enhancement relies on correlationwith clinical history and the region of enhancement. An abrupt onset of symptoms suggestsa vascular cause, whereas a more indolent history and nonspecific headache or lethargysuggests inflammation or infection. Gyral lesions affecting a single artery territory areoften vascular, whereas inflammatory lesions may affect multiple territories. The mostcommon vascular processes affect the middle cerebral artery territory (up to 60% of cases).However, PRES lesions usually localize in the posterior cerebral artery territory.
Professor Yasser Metwallywww.yassermetwally.com
18

Figure 11. Cortical gyral enhancement. (a) Diagram illustrates gyral enhancement that islocalized to the superficial gray matter of the cerebral cortex. There is no enhancement ofthe arachnoid, and none in the subarachnoid space or sulci. (b) Coronal gadolinium-enhanced T1-weighted MR image in a case of herpes encephalitis shows multifocal,intraaxial, curvilinear, cortical gyri-form enhancement that involves both temporal lobes.The enhancement is most prominent on the right but is also seen in the left insular region(arrows) as well as in the medial frontal lobes and cingulate gyrus (arrowhead)..
Vascular gyral enhancement results from various mechanisms with variable time courses.The earliest enhancement can be caused by reversible blood-brain barrier changes whenischemia lasts for only several hours before reperfusion occurs. Early reperfusion may alsoproduce vasodilatation, with increased blood volume and shortened mean transit time.These features were first observed at conventional angiography; they were described asdynamic changes and were called "luxury perfusion" because of the increased blood flow.The increased blood flow is caused by autoregulation mechanisms, which are "tricked" bythe increased tissue PCO2 that accumulates before reperfusion occurs. Ischemia orinfarction may demonstrate gyral enhancement on both CT and MR images within minutes(with early reperfusion). In the healing phases of cerebral infarction, from several days (5–7 days) to several weeks after the event, there will be vascular proliferation or hypertrophy.Contrast enhancement usually fades away between 4 weeks and 4 months after the stroke,and enhancement is usually replaced by brain volume loss. The vascular changes facilitatethe breakdown and removal of the dead brain tissue and lead to the encephalomalacia andatrophy characteristic of old "healed" infarction. The imaging appearance of postictalstates may mimic the findings of cerebral infarction in several features, including gyralswelling, increased signal intensity on T2-weighted images and decreased signal intensityon T1-weighted images, sulcal effacement, and gyral enhancement. Reperfusion, whether
Professor Yasser Metwallywww.yassermetwally.com
19

acute (eg, after thrombolysis) or subacute to chronic ("healing" infarction), is required todeliver contrast material to produce enhancement.
Figure 12. Cortical gyral enhancement in embolic cerebral infarction in a 65-year-oldwoman. (a) On an axial nonenhanced CT scan, the sulci in the right hemisphere arenormally prominent; on the left, the parietal sulci are effaced within a wedge-shaped regionof abnormal hypoattenuation. The gyral surface is actually slightly hyperattenuating due toreperfusion injury with secondary petechial hemorrhage in the infarcted cortex. (b) Axialcontrast-enhanced CT scan shows cortical gyral enhancement. The same endothelialdamage that allows red cells to extravasate also permits contrast material to escape thevascular lumen and enter the brain parenchyma.
Professor Yasser Metwallywww.yassermetwally.com
20

Figure 13. Cortical gyral enhancement in subacute thrombotic cerebral infarction. (a)Axial contrast-enhanced CT scan shows enhancement that is limited to the opercularsurfaces, insula, and caudate nucleus head (all of which are gray matter). (b) Photograph ofan axially sectioned gross specimen shows green staining, which is caused by bilirubinbound to serum albumin, and which outlines areas of the brain where the blood-brain-barrier is no longer intact. Note how the green stain is almost exclusively in the gray matterof the cortex (arrowheads), basal ganglia (*), caudate nucleus, and claustrum. In theseareas, the healing process would have removed the infarcted tissue, resulting inencephalomalacia and atrophy, if the patient had not died (the jaundiced patient died 2weeks after left internal carotid thrombosis caused infarction of the anterior and middlecerebral artery territories).
RADIOLOGICAL PATHOLOGY OF OLD INFARCTION
During the first week, there is a transient inflammatory reaction, especially around bloodvessels and in the meninges, due to release of arachidonic and other fatty acids. As the coreof the infarcted area disintegrates, endothelial cells from the periphery proliferate andcapillaries grow into the dead tissue. Neovascularization (which accounts for contrastenhancement) peaks at 2 weeks.
Mononuclear cells from the blood stream enter the infarct through damaged vessels. Theyingest the products of degradation of neurons and myelin and are transformed into lipid-laden macrophages. Macrophage reaction appears early and peaks at 3-4 weeks. Astrocytesfrom the surrounding undamaged brain proliferate and form a glial scar around the
Professor Yasser Metwallywww.yassermetwally.com
21

infarct (astrogliosis). This is completed in approximately 2 months. After that, the infarctremains unchanged. With maturation of new capillaries and glial scar formation, the bloodbrain barrier is once again sealed. Neurons do not regenerate. So, some brain tissue is lostforever.
With progression of time the infarction gets more hypodense and the mass effect graduallydecreases with time due to gradual reduction of brain edema because the blood brainbarrier is once again sealed. Negative mass effect is the end result. It is tempting to considerthat these CT changes in old infarcions represent edema. The question then arises: Is thisvasogenic edema or cytotoxic edema? Because the blood-brain barrier is sealed in oldinfarctions, vasogenic edema is unlikely. The cells are not dead or dying, so that cytotoxicedema is also unlikely.
Figure 14. A, subacute infarction, B, old infarction with extensive gliosis and cavitations
Figure 15. (A) Old infarction with extensive gliosis, microcavitations, the infarction ishypodense with negative mass effect (B)
Professor Yasser Metwallywww.yassermetwally.com
22

Perhaps the edema results from the increased number of astrocytic cells that spread apartthe normal myelinated axons of the white matter. The presence of significant amount ofnormal appearing astrocytes (hyperplasia), with marked cytoplasmic hypertrophy and lownuclear to cytoplasm ratio result in total increase in the water content of the brain. Thesecells may merely have different physical and chemical properties than the normal tightlypacked bundles of axons that traverse through the brain. Astrogliosis is commonlyassociated with widened fluid filled extracellular spaces (microcavitations andmacrocavitations) which definitely increase tissues water content resulting in thecharacteristic CT scan/MRI picture. 48,49,50
Figure 16. With progression of time (from A to C) the infarction gets more hypodense,more well defined and the mass effect gradually decreases with time due to gradualreduction of brain edema because the blood brain barrier is once again sealed. The initialhypodensity in acute infarction is due to edema (A) while the the ultimate hypodensity inold infarction (C) is due to astrogliosis with widened fluid filled extracellular spaces(microcavitations and macrocavitations). During the evolution of the infarction the edemaand the swelling decreases and the infarction boundary becomes better defined, and theinfarcted area becomes more hypodense.
Perhaps the edema results from the increased number of astrocytic cells that spread apartthe normal myelinated axons of the white matter. The presence of significant amount ofnormal appearing astrocytes (hyperplasia), with marked cytoplasmic hypertrophy and lownuclear to cytoplasm ratio result in total increase in the water content of the brain. Thesecells may merely have different physical and chemical properties than the normal tightlypacked bundles of axons that traverse through the brain. Astrogliosis is commonlyassociated with widened fluid filled extracellular spaces (microcavitations andmacrocavitations) which definitely increase tissues water content resulting in thecharacteristic CT scan/MRI picture. 48,49,50
Figure 16. With progression of time (from A to C) the infarction gets more hypodense,more well defined and the mass effect gradually decreases with time due to gradualreduction of brain edema because the blood brain barrier is once again sealed. The initialhypodensity in acute infarction is due to edema (A) while the the ultimate hypodensity inold infarction (C) is due to astrogliosis with widened fluid filled extracellular spaces(microcavitations and macrocavitations). During the evolution of the infarction the edemaand the swelling decreases and the infarction boundary becomes better defined, and theinfarcted area becomes more hypodense.
Perhaps the edema results from the increased number of astrocytic cells that spread apartthe normal myelinated axons of the white matter. The presence of significant amount ofnormal appearing astrocytes (hyperplasia), with marked cytoplasmic hypertrophy and lownuclear to cytoplasm ratio result in total increase in the water content of the brain. Thesecells may merely have different physical and chemical properties than the normal tightlypacked bundles of axons that traverse through the brain. Astrogliosis is commonlyassociated with widened fluid filled extracellular spaces (microcavitations andmacrocavitations) which definitely increase tissues water content resulting in thecharacteristic CT scan/MRI picture. 48,49,50
Figure 16. With progression of time (from A to C) the infarction gets more hypodense,more well defined and the mass effect gradually decreases with time due to gradualreduction of brain edema because the blood brain barrier is once again sealed. The initialhypodensity in acute infarction is due to edema (A) while the the ultimate hypodensity inold infarction (C) is due to astrogliosis with widened fluid filled extracellular spaces(microcavitations and macrocavitations). During the evolution of the infarction the edemaand the swelling decreases and the infarction boundary becomes better defined, and theinfarcted area becomes more hypodense.
Professor Yasser Metwallywww.yassermetwally.com
23

Figure 17. Astrocytes have extensive vascular foots, Astrogliosis (astrocytic hyperplasia)commonly results in the formation of a mesh with enlargement of extracellular spaces andextensive fluid-filled microcavitations. This, coupled with marked cytoplasmic hypertrophyof astrocytes-that results in low nuclear to cytoplasm ratio- are responsible for the CT scanpicture of old infarction.
Figure 18. Reactive astrocytosis. Notice the mesh between the astrocytes
Professor Yasser Metwallywww.yassermetwally.com
24

Table 4. Comparison between CT hypodensity of recent and old infarctions
Recent infarction Old infarction
Etiology of CT hypodensityVasogenic edema (cytotoxicedema does not contribute toCT hypodensity)
Astrogliosis with widenedfluid filled extracellularspaces (microcavitations andmacrocavitations)
THROMBOLYSIS: WHO AND WHEN TO TREAT
Both the radiologist and the clinician play important roles in determining who is acandidate for thrombolytic therapy and how it is administered. The clinician mustcarefully assess the patient for the extent of ischemic symptoms; time of onset; andpresence of other complicating factors that may preclude thrombolysis, such as recentmajor surgery or other contraindications for anticoagulation. The radiologist then mustcarefully review the imaging studies for the presence of hemorrhage or extensive ischemicchange that would prevent treatment.
Figure 19. A 62-year-old woman who presented with a 4-hour history of right hemiparesisand aphasia. A and B, Noncontrast CT scan demonstrates a large area of low attenuationin the left middle cerebral artery distribution with obscuration of the lentiform nuclei, lossof the gray-white interface, and effacement of sulci. Due to the presence of a well-definedinfarct this patient was not considered a candidate for thrombolytic therapy. C, CT scanperformed 4 days later demonstrates a large left MCA infarct with mass effect andmoderate midline shift to the right. A craniectomy has been performed to relieveintracranial pressure.
Patients may be considered for three different treatment options: intravenous, intra-arterial, or combined intravenous and intra-arterial thrombolysis. The type ofthrombolytic therapy is determined by the duration and severity of symptoms. If a patient
Professor Yasser Metwallywww.yassermetwally.com
25

presents within 3 hours of ictus and has no contraindications to thrombolysis, he or she is acandidate for intravenous tPA therapy. Intravenous therapy is not considered if theduration of ischemia is longer than 3 hours or the time of onset is unknown.
As mentioned earlier in this article, patients with major vessel occlusion, such as internalcarotid, proximal MCA, or basilar artery thrombosis, have a poorer response tointravenous therapy compared with those with smaller branch occlusions and should beconsidered for intra-arterial therapy, if available. Clinical and radiographic features of thisgroup include a dense vessel sign, either MCA or basilar; clinical evidence of ischemia inthese vascular distributions; and a National Institutes of Health Stroke Scale Score greateror equal to 10.
Intra-arterial thrombolysis can also be administered after longer duration of ischemia thanintravenous therapy. MCA occlusions can be treated up to 6 hours after onset of symptoms.After 6 hours, the risk of hemorrhage is believed to outweigh the potential benefits. Basilarartery occlusions typically have dire clinical outcomes and therefore may be treated up to24 or 48 hours after ictus.
CONCLUSION
Despite the development of advanced imaging techniques, such as xenon CT, MRdiffusion/perfusion, and MR angiography, CT scanning continues to play a major role inthe assessment of acute strokes. Although CT is less sensitive than MR imaging in detectingacute ischemia, it is useful in screening patients for potential thrombolytic therapy. Whenreviewing CT scans of potential thrombolysis patients, several key points should beconsidered. The presence of hemorrhage is a contraindication for thrombolytic agents.Stroke patients with negative CT scans or small areas of edema are candidates fortreatment; however, the presence of early MCA ischemic changes indicates more severehypoperfusion, which may predict a poorer clinical outcome. Evidence of extensive MCAinfarct on the initial CT scan usually precludes treatment with thrombolysis because of theincreased risk of hemorrhage and decreased clinical benefit. The presence of a hyperdenseMCA sign is associated with a poorer outcome after intravenous therapy; therefore, moreaggressive therapy, such as intra-arterial thrombolysis, should be considered if technicallyfeasible.
Professor Yasser Metwallywww.yassermetwally.com
26

TABLE 5. CT SCAN FEATURES ASSOCIATED WITH A POORER OUTCOMEAFTER THROMBOLYTIC FEATURES
Radiologicalfeature Description
Brain edema,diffuse lowdensity on theinitial CT scan
The absolute presence or absence of edema primarily relies on theseverity of hypoperfusion and adequacy of collateral circulation. Thepresence of more extensive edema on an early CT scan indicates severehypoperfusion and may predict a less favorable outcome afterthrombolytic therapy. The rate of complication, including hemorrhage, issignificantly increased in this subgroup of patients .
HyperdenseMCA sign
It is associated with occlusion of the proximal MCA or its branches and itis present in 30% to 50% of patients presenting with clinical signs ofacute MCA stroke .
Sites ofocclusion
Internal carotid, proximal MCA, or basilar artery thrombosis, have apoorer response to intravenous therapy compared with those with smallerbranch occlusions and should be considered for intra-arterial therapy, ifavailable.
Figure 20. Topography of the cerebral main vascular territories
Professor Yasser Metwallywww.yassermetwally.com
27

Figure 21. Topography of the cerebral main vascular territories
References
1. Astrup J, Siejo BK, Symon L: Threshold in cerebral ischemia: The ischemic penumbra.Stroke 12:723-725, 1981
2. Bastianello S, Pierallini A, Colonnese C, et al: Hyperdense middle cerebral artery CTsign: Comparison with angiography in the acute phase of ischemic supratentorialinfarction. Neuroradiology 33:207-211, 1991
3. Bell BA, Symon L, Branston NM: CBF and time thresholds for the formation of ischemicedema, and effect of reperfusion in baboons. J Neurosurg 62:31-41,1985
Professor Yasser Metwallywww.yassermetwally.com
28

4. Bozzao, L, Bastianello S, Fantozzi LM, et al: Correlation of angiographic and sequentialCT findings in patients with evolving cerebral infarctions. AJNR Am j Neuroradiol10:1215-1222,1989
5. Brant-Zawadski M, Pereira B, Weinstein P, et al: MR imaging of acute experimentalischemia in cats. AJNR Am j Neuroradiol 7:7-11, 1986
6. Bryan RN, Levy LM, Whitlow WD, et al: Diagnosis of acute cerebral infarction:Comparison of CT and MR imaging. AJNR Am j Neuroradiol 12:611-620,1991
7. Caplan V, Babikian V, Helgason C, et al: Occlusive disease of the middle cerebral artery.Neurology 35:975- 982,1985
8. Division of Chronic Disease Control and Community Intervention: Cardiovasculardisease surveillance: Stroke, 1980-1989. Atlanta, Centers for Disease Control andPrevention, 1994
9. Firlick AD, Kaufmann AM, Weschler LR, et al: Quantitative cerebral blood flowdeterminations in acute ischemic stroke: Relationship to computed tomography andangiography. Stroke 28:2208-2213, 1997
10. Gacs, G, Fox Aj, Barnett Hj, et al: CT visualization of intracranial arterialthromboembolism. Stroke 4:756- 762,1983
11. Garcia JH: Experimental ischemic stroke: A review. Stroke 15:5-14, 1984
12. Hacke W, Kaste M, Fieshi C, et al: Intravenous thrombolysis with recombinant tissueplasminogen activator for acute hemispheric stroke: The European cooperative acutestroke study (ECASS). JAMA 274:1017- 1025,1995
13. Heiss WD, Hayakawa T, Walta AG: Cortical neuronal function during ischemia:Effects of occlusion of one middle cerebral artery on single unit activity in cats. ArchNeurol 33:813-820, 1976
14. Horowitz Sli, Zito JL, Donnaromma R, et al: Computed tomographic-angiographicfindings within the first five hours of cerebral infarction. Stroke 22:1245- 1253,1991
15. Hossman KA, Schuier Fj: Experimental brain infarcts in cats: I. Pathophysiologicalobservations. Stroke 11:583-592, 1980
16. Iannotti F, Hoff J: Ischemic brain edema with and without reperfusion: Anexperimental study in gerbils. Stroke 14:562-567, 1983
17. Kaste M, Waltimo 0: Prognosis of patients with middle cerebral artery occlusion.Stroke 7:482-484, 1976
Professor Yasser Metwallywww.yassermetwally.com
29

18. Levy DE, Brott TG, Haley EC, et al: Factors related to intracranial hematomaformation in patients receiving tissue-type plasminogen activator for acute ischemic stroke.Stroke 25:291-297, 1994
19. Leys D, Pruvo JP, Godefroy D, et al: Prevalence and significance of hyperdense middlecerebral artery in acute stroke. Stroke 23:317-324, 1992
20. Mohr JP, Biller J, Hilal SK, et al: MR vs CT imaging in acute stroke. Stroke 23:142-149, 1992
21. Moulin T, Cattin F, Crepin-Leblond T, et al: Early CT signs in acute middle cerebralartery infarction: Prdictive value for subsequent infarct locations and outcome. Neurology47:366-375, 1996
22. New PF, Aronow S: Attenuation measurements of whole blood and fractions incomputed tomography. Radiology 121:635-640,1976
23. NINDS Stroke Study Group: Tissue plasminogen activator for acute ischemic stroke. NEngl J Med 333:1581-1587,1995
24. NINDS Stroke Study Group: Intracerebral hemorrhage after intravenous tPA therapyfor ischemic stroke. Stroke 28:2109-2188, 1997
25. O'Brien MD: Ischemic cerebral edema: A review. Stroke 10:623-628, 1979
26. Phelps ME, Gado MH, Hoffman EJ: Correlation of effective atomic number andelectron density with attenuation coefficients measured with polychromatic X-rays.Radiology 11 7:585-588, 1975
27. Plum F: What causes infarction in ischemic brain? The Robert Wartenburg Lecture.Neurology 33:222-233,. 1983
28. Pressman BD, Touae EJ, Thompson JR: An early CT sign of ischemic infarction:Increased density in a cerebral artery. AJNR Am j Neuroradiol 8:645-668,1987
29. Raichle ME: The pathophysiology of brain ischemia. Ann Neurol 13:2-10,1983
30. Rauch RA, Bazan C, Larsson EM, et al: Hyperdense middle cerebral arteries identifiedon CT as a false sign of vascular occlusion. AJNR Am j Neuroradiol 14:669- 673,1993
31. Ricci S, Caputo N, Aija G, et al: Prognostic value of the dense middle cerebral artery inpatients with acute ischemic stroke. Ital J Neurol Sci 12:45-47, 1991
32. Saito 1, Segawa H, Shiokawa Y, et al: Middle cerebral artery occlusion: Correlation ofcomputed tomography with clinical outcome. Stroke 18:863-868, 1987
Professor Yasser Metwallywww.yassermetwally.com
30

33. Schuierer G, Huk W: The unilateral hyperdense middle cerebral artery: An early CTsign of embolism or thrombus. Neuroradiology 30:120-122, 1988
34. Schuknecht B, Ratzka M, Hofmann: The dense artery sign-major cerebral arterythromboembohsm demonstrated by computed tomography. Neuroradiology 32:98-103,1990
35. Tomsick TA, Brott T, Barsan W, et al: Prognostic value of the hyperdense middlecerebral artery sign and stroke scale score before ultraearly thrombolytic therapy. AJNRAm j Neuroradiol 17:79-85, 1996
36. Tomsick TA, Brott T, Barsan W, et al: Thrombus localization with emergency cerebralCT. AJNR Am j Neuroradiol 13:257-263, 1992
37. Tomsick TA, Brott TG, Chambers AA, et al: Hyperdense middle cerebral artery signon CT: Efficacy in detecting middle cerebral artery thrombosis. AJNR Am j Neuroradiol11:473-477,1990
38. Tomura N, Uemura K, Inugan-d A, et al: Early CT finding in cerebral infarction:Obscuration of the lentiform nucleus. Radiology 168:463-467,1988
39. Torack RM, Alcala H, Gado M, et al: Correlative assay of computerized cranialtomography (CCT), water content and specific gravity in normal and pathologicalpostmortem brain. J Neuropathol Exp Neurol 35:385-392,1976
40. Truwit CL, Barkovich Aj, Gean-Marton A, et al: Loss of the insular ribbon: Anotherearly CT sign of acute middle cerebral artery infarction. Radiology 176:801- 806,1990
41. Unger E, Littlefield J, Gado M: Water content and water structures in CT and MRsignal changes: Possible influence in detection of early stroke. AJNR Am j Neuroradiol9:687-691, 1988
42. von Kummer R, Allen KL, Holle R, et al: Acute stroke: Usefulness of early CT findingsbefore thrombolytic therapy. Radiology 205:327-333, 1997
43. von Kununer R, Meyding-Lamade U, Forsting M, et al: Sensitivity and prognosticvalue of early CT in occlusion of the middle cerebral artery trunk. AJNR Am JNeuroradiol 15:9-15, 1994
44. von Kummer R, Nolte PN, Schnittger H, et al: Detectability of cerebral hemisphereischaemic infarcts by CT within 6 h of stroke. Neuroradiology 38:31-33, 1996
45. von Kummer R, Weber J: Brain and vascular imaging in acute ischemic stroke: Thepotential of computed tomography. Neurology 4(suppl):S52-55,1997
Professor Yasser Metwallywww.yassermetwally.com
31

46. Yock DH: CT demonstration of cerebral emboh. j Comput Assist Tomogr 5:190-196,1981
47. Yokogami K, Nakdno S, Ohta H, et al: Prediction of hemorrhagic complications afterthrombolytic therapy for middle rerebral artery occlusion: Value of pre- and post-therapeutic computed tomographic findings and angiographic occlusive site. Neurosurgery49:1102- 1107,1996
48. Bames D, McDonald WI, Landon DN, et al: The characterization of experimentalgliosis by quantitative nuclear magnetic resonance imaging. Brain 111:83-94, 1988
49. Newcombe J, Hawkins CP, Henderson CL, et al: Histopathology of multiple sclerosislesions detected by magnetic resonance imaging in unfixed postmortem central nervoussystem tissue. Brain 114:1013- 1023, 1991
50. Stewart WA, Hall LD, Berry K, et al: Correlation between NMR scan and brain slices:Data in multiple sclerosis. Lancet 2:412, 1984
51. Skriver EB, Olsen TS. Transient disappearance of cerebral infarcts on CT scan, the so-called fogging effect.Neuroradiology 1981;22:61-65.
52. Becker H, Desch H, Hacker H, Pencz A. CT fogging effect with ischemic cerebralinfarcts. Neuroradiology 1979;18:185-192.
53. Ackerman RH, Lev MH, Alpert NM, et al. Infarct fogging on CT: prevalence, features,and PET/MRI correlates. In: Proceedings of the 28th Annual Meeting of the AmericanSociety of Neuroradiology; 1990; Los Angeles, CA.
Created by Professor Yasser Metwally
http://yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
32

INDEX |
INTRODUCTION
NEUROIMAGING OFHEMORRHAGIC INFARCTION
o Arterial hemorrhagicinfarction
o Hemorrhagic Venousinfarction
INTRODUCTION
A hemorrhagic infarction can be defined as an ischemic infarct in which an area ofbleeding exists within ischemic cerebral tissue. This definition includes small hemorrhagesconfined to minor ischemic areas in gray matter as well as much larger areas involvingcortical and deep lesions. Hemorrhagic infarction has been recognized as a complication ofembolic stroke. In pathological studies, cerebral embolism was associated withhemorrhagic infarction in 50% to 70% of cases (13). In an angiographic study reported byYamaguchi et al (4), the incidence of hemorrhagic infarction in patients with cardiogenicembolism was 37.5%, which was significantly higher than the 1.5% in patients with non-embolic stroke. A prospective survey by Hornig et al (5) based on clinical and radiologicalstudies has indicated that hemorrhagic infarction occurs in 43% of ischemic stroke
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
33

patients. Regarding the arterial distribution of hemorrhagic infarction, 90% of the patientshad involvement of the anterior circulation (6). However, there was little information onthe involvement of the posterior circulation. In 1996, Chaves et al (7) investigatedcerebellar hemorrhagic infarction, and concluded that the causes, imaging findings andconsequences of hemorrhagic infarction in posterior circulation were similar to those inanterior circulation. Anecdotal evidence implicated large embolic cerebral infarcts (5, 8, 9),uncontrolled hypertension ( 10), advanced age and institution of anticoagulants (10-12) orthrombolytic agents (13, 14) as special risk factors for hemorrhagic infarction. Infarct sizeseemed to be the most important factor for secondary hemorrhage. The reason forpreferential hemorrhagic transformation of a large infarct with a mass effect might includemore extensive edema, compression of small vessels in the area surrounding the lesion andstasis of blood flow. After the decrease of edema, reperfusion of these vessels occurs andbecause these capillaries often have a disrupted endothelium, a diapedesis of blood willoccur (15, 16). Cerebellar hemorrhagic infarction was common when the full cerebellararterial territories were involved, probably reflecting the larger size of infarcts, which isknown to be a risk factor associated with hemorrhagic infarction in the anterior circulation(7). As compared to cerebellar hemorrhagic infarction, massive pontine hemorrhagicinfarction was relatively uncommon. The reason why the incidence of pontine hemorrhagicinfarction is low has not been clarified. (50)
The pathogenesis of hemorrhagic infarction has been investigated in experimental andclinical studies. There are three theories concerning the mechanism of hemorrhagicinfarction. The most common pattern in supratentorial and cerebellar hemorrhagicinfarction is complete interruption of arterial blood supply, followed by reperfusion. In1951, Fisher and Adams ( 1 ) reported a high incidence of hemorrhagic infarction in theirautopsy study of cerebral embolism. They postulated that hemorrhagic transformationoccurs when an embolus fragments and migrates distally, thereby opening the previouslyoccluded vessel and exposing the necrotic brain to the full force of arterial blood pressure.The downstream migration of the embolus after its initial impact leads to extravasation ofblood via reflow into damaged vessels of the proximally infarcted zone. Reconstitution ofblood flow results in hemorrhagic transformation of the embolic infarction (2, 17). Thismigration embolism could occur in the vertebrobasilar circulation system as well as thecarotid and cerebellar systems. As suggested by Kimura et al (18) in this volume, theextensive embolic occlusion of the entire length of the basilar artery and migration of theembolus are assumed to develop into massive pontine hemorrhagic infarction.
The second mechanism is extravasation from leptomeningeal collateral vessels. Somepatients with cardiogenic embolic stroke developed hemorrhagic infarction withoutopening of occluded vessels. In such cases, restoration of blood flow occurs throughleptomeningeal collaterals. Ogata et al ( 19) indicated that hemorrhage into an infarct withpersisting occlusion of the proximal artery may occur when the involved blood vessels areexposed to the force of arterial blood pressure from the leptomeningeal collaterals. A lesscommon pattern is incomplete and insufficient perfusion caused by stenotic vessels,followed by gradual necrosis of cerebral tissue. (50)
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
34

Thrombolytic therapy of acute ischemic stroke patients is currently one of the mostcontroversial topics in clinical medicine. The use of thrombolytic agents can increase thelikehood of hemorrhagic infarction (13, 14). The decision regarding whether to usethrombolytic agents should be based on thorough evaluation of the individual patients by aphysician with a speciality in treating stroke patients. Patients with large infarcts andsevere neurological deficits have a higher risk of hemorrhagic transformation afterthrombolysis. However, it remains debatable how to prevent and manage hemorrhagicinfarction caused by acute therapeutic agents in ischemic stroke patients. More clinicalresearch is needed.
NEUROIMAGING OF HEMORRHAGIC INFARCTION
Arterial hemorrhagic infarction
Ischemic infarction can be divided into "bland or non-hemorrhagic" infarction andinfarction associated with secondary bleeding — referred to as hemorrhagic conversion ortransformation (HT) — in ischemically infarcted areas. Bland infarction is characterizedby bland widespread leukocyte infiltration and macrophage invasion, with only scatteredred cells being found. Hemorrhagic conversion may take the form of hemorrhagicinfarction (HI) or, less commonly, parenchymatous hemorrhage associated with a cerebralembolic infarction (PH). The occurrence of Hemorrhagic conversion is "predominantly anatural tissue consequence of embolism". (50)
Bland or non-hemorrhagic
Bland infarction is characterized by bland widespread leukocyteinfiltration and macrophage invasion, with only scattered red cellsbeing found. The occurrence of Hemorrhagic conversion ofinfarction is "predominantly a natural tissue consequence ofembolism"
Hemorrhagicconversion of infarction
Hemorrhagic infarction (HI)
Parenchymatous hemorrhage associated with a cerebral embolicinfarction (PH)
An autopsy, hemorrhagic infarction may vary from patchy petechial bleeding to moreconfluent hemorrhages, representing multifocal extravasation of blood from capillaries orvenules. Hemorrhagic infarction and Parenchymatous hemorrhage associated with acerebral embolic infarction (PH) have different incidences, pathogenesis, and clinicaloutcome, but distinguishing HI and PH on CT may be difficult. Although HI and PH haveoften been grouped together, there are certain features on CT that help characterize thesetwo types of hemorrhagic transformation. On CT, HI appears as a discontinuousheterogeneous mixture of high and low densities occurring within the vascular territory ofthe infarct. In contrast, PH appears as a discrete, homogeneous collection of blood thatoften exerts mass effect and may extend beyond the original infarct boundaries or even intothe ventricles. (50)
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
35

hemorrhagic infarction(HI)
HI appears as a discontinuous heterogeneous mixture of high andlow densities occurring within the vascular territory of the infarct
Parenchymatoushemorrhage associatedwith a cerebral embolicinfarction (PH)
Parenchymatous hemorrhage associated with a cerebral embolicinfarction (PH) appears as a discrete, homogeneous collection ofblood that often exerts mass effect and may extend beyond theoriginal infarct boundaries or even into the ventricles
Hemorrhagic infarction occurs regularly in the natural evolution of acute embolic stroke.Hemorrhagic transformation of an infarction can occur spontaneously in up to 30% ofpatients by serial CT brain scan. (19) Transformation of a bland embolic infarct tohemorrhagic infarction is rare in the first 6 hours. Most hemorrhagic infarctions areasymptomatic, and it is not uncommon to detect hemorrhagic infarction on CT in patientswho are stable or improving. The pathogenesis of hemorrhagic conversion ortransformation in ischemically infarcted areas appears to relate to reperfusion of bleedingfrom recanalized but ischemically injured vessels by the natural, dynamic dissolution ofthrombi i.e., an embolus that represents all or part of a thrombus has a spontaneoustendency to lyse and disperse. Reperfusion into the ischemically injured vessels cantherefore result in varying degrees of blood extravasation through the damaged blood-brain barrier. (50)
Hemorrhagic infarction has been often explained as a result of reperfusion of the vascularbed of the infarct, such as would occur after fragmentation and distal migration of anembolus or after early reopening of a large vessel occlusion in the setting of a largeinfarction; the full pressure of arterial blood into hypoxic capillaries results in a diapedesisor red cells through their hypoxic walls. The concept of restored lumen patency isconsistent with greater frequency of hemorrhagic infarction in patients with cardioembolicinfarcts.
The occurrence of parenchymatous hemorrhage (PH) in areas of ischemic infarction is lesscommon that that of HI. PH appears to be associated with anticoagulation therapy,Antiplatelet therapy and thrombolytic therapy, with a low incidence of spontaneous PH inareas of ischemic infarction (on the order of 2% to 9%) in patients not receivinganticoagulation therapy. In contrast to HI, clinical deterioration is often associated withPH. It has been proposed that the pathogenesis of PH may involve "ischemic necrosisresulting in the rupture of small penetrating vessels analogous to hypertensive hemorrhage,leading to massive bleeding rather that the multifocal diapedesis of blood through capillarywalls, as seen in HI". (50)
The observation that some hemorrhagic infarctions develop distal to the site of a persistingocclusion suggests that reperfusion is not always a necessary condition. Investigators fromJapan (20) examined the brains of 14 patients who died from herniation of the brain aftercardioembolic stroke with persistent occlusion of the internal carotid-middle arterial axis .The finding of hemorrhagic infarct in 7 of the patients contradicts the concept thatreopening a previously occluded vessel is the only pathophysiologic mechanism for thedevelopment of hemorrhagic infarct. Analysis of blood pressure after stroke has revealedone or more surges of arterial hypertension or rapid rise of blood pressure in patients with
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
36

hemorrhagic stroke without a reopening of the occluded artery; it has been speculated thatthese blood pressure rises might explain hemorrhagic infarction in many cases. (50)
A relationship between hyperglycemia and hemorrhagic transformation has also beensuggested by he observation that occluding the middle cerebral artery of markedlyhyperglycemia cats was associated with 5-fold more frequent and 25-fold more extensivehemorrhage into infarcts than in normoglycemic animals (21). Compared with permanentocclusion, temporary restoration of blood flow after 4 hours caused the most extensivehemorrhage into infarcts. It was concluded that hyperglycemia and restoration of bloodflow to ischemic territories were strong risk factors for hemorrhagic infarct conversion.The evidence suggests that the marked tissue energy depletion accompanied by acidosisdamages brain vessels, causing leakage of edema fluid and red blood cells (21). Diffuse HIassociated with marked hyperglycemia has been reported in two patients (22).
In summary, HI occurs regularly in the natural evolution of acute embolic stroke and isusually asymptomatic. Parenchymatous hemorrhage associated with a cerebral embolicinfarctions (PHs) occur less frequently, but are often symptomatic due to extension andmass effect beyond the original infarct territory. Interest in these issues has been furthergenerated by trials of thrombolytic therapy for acute ischemic stroke.
Hemorrhagic infarction is regarded as distinct from anemic infarction althoughmicroscopical haemorrhage is frequent in the later. It has frankly hemorrhagic featureswhich consist of petechial zones that are frequently confluent and are situated in the cortex.These hemorrhagic areas may involve the entire infarction but tend most often to involvethe boundary zones supplied by meningeal arterial anastomosis or, in case of middlecerebral infarct, in the basal ganglia. Hemorrhagic infarction is secondary corticalreirregation which takes place in the capillary blood vessels that have been damaged by theinitial hypoxia. Reirregation takes place when lysis (natural or by therapeuticthrombolysis) or secondary mobilization of the thrombus take place.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
37

Figure 1. Haemorrhagic infarctions. They have frankly hemorrhagic features which consistof petechial zones that are frequently confluent and are situated in the cortex.
Figure 2. Noncontrast CT brain scan within 1 hour of acute onset of aphasia andright-sided weakness (A), which demonstrates an old right posterior cerebral arteryterritory infarct, and 24 hours later, after thrombolytic therapy (B), demonstratingdramatic hemorrhage transformation of the cerebral infarct.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
38

Figure 3. Parenchymatous hemorrhage associated with a cerebral embolic infarctions(PHs) occur less frequently, but are often symptomatic due to extension and mass effectbeyond the original infarct territory.
o Anticoagulants and hemorrhagic infarctions (50)
The occurrence of ICH in patients receiving oral anticoagulants is generally a seriousevent. On one hand, the risk of ICH is increased by eight to 11 fold by the chronic use ofwarfarin anticoagulation. On the other hand, this mechanism of ICH often leads to largerhaematomas than those in patients not receiving anticoagulants, a feature that correlateswith substantially higher mortality rates.
Table 2. The clinical features of ICH in patients receiving oral anticoagulants include:
Anticoagulant
Anticoagulant
Anticoagulant
Anticoagulant
A low frequency of associated bleeding elsewhere in the body. Lack of consistent association between ICH and preceding head
trauma or cerebral infarction. Larger haematoma volumes in anticoagulated patients than in non-
anticoagulated patients, as a result of more prolonged bleedingperiods.
A bad prognosis in anticoagulant-related ICHS, with mortality ratesexceeding 50-60%
Box 1. Other features related to the occurrence of anticoagulant-related ICH are lessconsistently observed, and include: (50)
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
39

1. Duration of anticoagulation prior to onset of ICH: in some reports. mosthaemorrhages (70%) occurred within the first year of treatment, whereas in othersonly about one-third of the cases occurred within that period of time.
2. Relationship between intensity of anticoagulation and risk of ICH: in some studies.ICH was more likely with excessive prolongation of the prothrombin time, but inothers there was no clear relationship.
3. Role of hypertension in causing ICH in patients on oral anticoagulants: a strongassociation with hypertension is present.
4. Location of ICH: a relatively high frequency of cerebellar haemorrhages inanticoagulated patients has been reported in some series, but not in others.
Thrombolytic agents and hemorrhagic infarctions
Thrombolytic agents, in particular streptokinase and recombinant tissue- typeplasminogen activator (rt-PA), are widely used in the treatment of patients with acutemyocardial infarction (MI). Although the frequency of ICH is low (0.4-1.3% of treatedpatients). especially with the intravenous use of the fibrin-specific agent rt-PA, itsoccurrence is always serious and often fatal. (50)
Table 3. The clinical and CT aspects of ICH related to the use of rt-PA in MI include thefollowing
Thrombolysis
Thrombolysis
Thrombolysis
Onset soon after treatment, close to 40% of them during the rt-PAinfusion and another 25% occurring within 24 hours of onset ofinfusion in one series .
Predominantly lobar location, with rare examples of bleeding into theposterior fossa and putamen
Multiple simultaneous haemorrhages in about one-third of the cases. Mortality rate of 44-66%.
The mechanism of bleeding in the setting of rt-PA use is not clear. A potential role of theconcomitant use of intravenous heparin in the production of ICH has been suggested. TheGlobal Use of Strategies to Open Occluded Coronary Arteries as the majority of patientswith this complication have excessively prolonged activated partial thromboplastin time(APTT) ( 100 seconds) at the time of onset of the ICH. Local vascular factors with bleedingpotential, such as CAA, have been recently reported as the suspect substrate of ICH in thesetting of thrombolysis for acute MI. Other features, such as age 65 years, history ofhypertension, and previous aspirin use have been suggested as risk factors, but have notbeen clearly documented.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
40

More details about hemorrhagic transformation of arterial infarctionswith thrombolytic therapy (50)
The most feared complication in acute ischemic stroke is hemorrhagic transformation (HT)as it has devastating clinical consequences and is associated with an over ten-fold increasein mortality (23). Although in clinical practice this complication may be less frequent thanfailure of treatment to recanalized occluded cerebral artery or early reocclusion, ICHseems to represent an important obstacle to the generalization of thrombolytic therapy(24). Intracerebral hemorrhage mostly occurs in the core of the infracted area, thussuggesting that ischemic events can have an important role (25).
In experimental models of focal cerebral ischemia, the basal lamina of the vessels and theextracellular matrix show an alteration and the adhesion between the microvessel cells andthe extracellular matrix is dearranged so there can be an extravasation of blood elements.There is an increase in capillary permeability that comes along with an inrush of plasmacomponents inside the brain tissue, an inflammatory reaction with thrombin activation,and an increasing of many mediators such as platelet-activating factor, tumor necrosisfactor ? and bradykinin, which contribute to increase endothelial permeability. In addition,oxidative damage may increase hemorrhagic risk (26).
Metalloproteinases (50)
Matrix metalloproteinases (MMP) are involved in the hemorrhagic transformation, andtheir activation is partly responsible for the BBB disruption. MMPs represent a family ofproteolytic enzymes combined with zinc, which acts normally on the remodeling of theextracellular matrix. Inappropriate activation can induce proteolysis of the matrix of theneurovascular unity (endothelium, astrocyte, and neuron). MMPs are liberated by theendothelium and the polynucleates at the inflammatory stage of ischemia and utilize typeIV collagen and laminin as substrates. (27). In some animal models of focal cerebralischemia, activation of MMP-9 is associated with increased permeability of the BBB thatleads to edema formation and hemorrhagic transformation (27).
MMP-2 and MMP-9 released during the ischemic event can damage the vessel components,particularly type IV collagen, fibronectin, and laminin, thus altering the basal lamina ofthe cerebral vessels. In humans, elevation of MMP-9 is linked to the severity of ischemicstroke (28) , and the pretherapeutic MMP-9 rate is an independent predictor of the risk ofhemorrhagic transformation related to thrombolysis (29).
Risk factors for HT after thrombolytic therapy (50)
Exact knowledge of mechanisms related to ICH after thrombolysis and the role ofbiomarkers could be useful in selecting patients that can benefit from such treatment.Other elements must be taken in account for the genesis of rt-PA-related ICH: age,hypertension, diabetes mellitus or cerebral amyloid angiopathy, extent of early ischemicsigns shown on brain CT scan or the volume of cerebral ischemic lesions on diffusionweighted MRI, and the presence of leukoaraiosis (30).
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
41

The first trials on rt-PA have provided evidence that higher doses of lytic agents lead tohigher rates of sICH, so the dose was limited to 0.9 mg/kg up to 90 mg in total (31).
Age has been consistently found to be a risk factor for sICH after thrombolysis for acuteischemic stroke (8). Recent data from several open-label studies on use of rt-PA haveshown that the risk of sICH in the elderly is comparable to that of younger patients.Certain trial showed that the benefit-risk ratio of intravenous rt-PA can be favorable incarefully selected elderly stroke patients treated within three hours. The sICH rate was4.4% in the group of patients aged 80 years or older included in this study (32). The StrokeSurvey Group rt-PA analysis also concluded that it was not justified to systematicallycontraindicate thrombolysis for patients older than 80 years (33).
Many authors have shown the importance of the baseline stroke severity in hemorrhagicrisk after thrombolysis (9). The Multicentre tPA Acute Stroke Survey study showed thatthe NIHSS score was an independent marker of ICH, with an odds ratio of 1.38 for a one-point increase in the NIHSS score (33).
Some authers on their report did not find a significant association of severity ofneurological deficit at baseline with increased risk of sICH (10). Moreover, the ECASS Itrial showed that severity of neurological deficit at admission represented a risk factor forhemorrhagic trans-formation and not for parenchymal hematoma (31). Another factorwhich may contribute to the development of rt-PA-related sICH is hypertension during thefirst 24 hours after ischemic stroke (34).
Experimental and human studies indicate that hyperglycemia predicts higher strokemortality independently from stroke severity, stroke type, or age. These data suggest thathyperglycemia may directly contribute to poor outcomes by exacerbating acute braininjury (29). In the PROACT II study, there was an increased risk of sICH in patients withpretherapeutic glycemia higher than 200 mg/dl (35).
The mechanism of hyperglycemia-related ICH is not clear. There are numerous animalexperimental proofs that hyperglycemia provokes microvascular lesions as well as BBBdamage, leading to hemorrhagic transformation of the cerebral infarction (36). HoweverSome authers did not find that a history of diabetes mellitus was a risk factor for sICH,despite the fact that many patients with diabetes mellitus had elevated serum glucose atstroke onset (25). The significance of early ischemic changes on baseline brain CT scan aspredictors of hemorrhagic transformation scan remains controversial (26). With the adventof advanced MRI such as diffusion- (DWI) and perfusion-weighted imaging (PWI), It hasbeen demonstrated in recent studies that in anterior circulation strokes, an acute DWIlesion volume >70 cm3 has a high specificity for poor outcomes with or without therapy(37).
A retrospective multicenter study evaluated whether leukoaraiosis is a risk factor for sICHin patients treated with alteplase for anterior circulation stroke. All patients had receivedmagnetic resonance imaging evaluation before thrombolysis and for statistical analysis.Leukoaraiosis in the deep white matter was dichotomized into absent or mild versus
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
42

moderate or severe. The rate of sICH was significantly higher in patients with moderate tosevere leukoaraiosis than in patients without relevant leukoaraiosis (37).
The risk of ICH after thrombolysis in ischemic stroke patients carrying old asymptomaticmicrobleeds (which can considered as a marker of microangiopathy, and of amyloidangiopathy) remains a controversial subject (38). In a published pooled analysis of 570patients, the presence of microbleeds was not predictive of sICH after thrombolysis exceptgrade 3 microbleeds (39).
Some authors have suggested that the differences between symptomatic and asymptomaticICHs are due to the intensity of bleeding rather than physiopathologic differences. Forothers, hemorrhagic infarctions and parenchymal hematomas after t-PA have a differentclinical, etiologic, and biological significance (40). Benign hemorrhagic transformation canbe associated with the natural history of ischemic stroke while parenchymal hematomas,especially the PH-type 2 (homogeneous hematomas with mass effect occupying 30% ofischemic lesion volume) could be linked to the t-PA itself and particularly to its impact onhomeostasis (as demonstrated by elevation of fibrin degradation products after treatment)(41).
Any extension of the thrombolytic treatment window also implies an increased risk of HT.Data shows that the occurrence of HT in patients treated within three hours of symptomonset was 4.8%, while for those treated between three and six hours after onset theoccurrence rose to 6.4% (42).
Although tPA can cause fatal or symptomatic brain hemorrhage, patients treated with tPAstrictly following protocol have a higher likelihood of functional neurologic recovery. Thus,only physicians experienced in stroke management should use tPA to treat patients withacute stroke; inexperienced physicians are more likely to violate protocols, resulting inmore brain hemorrhages and deaths (43,44,45).
Venous infarction
In sinovenous thrombosis, the mechanism for venous infarction is obstruction of venousdrainage with increasing venous pressure in the affected region of the brain. The venouscongestion results in significant extravasation of fluid into the brain, producing focalcerebral edema and hemorrhage. The edema may be transient, if venous flow is re-established, or be associated with permanent tissue infarction if the increased venous bloodpressure eventually exceeds the arterial blood pressure. In the latter situation, there isinsufficient delivery of arterial blood and regional ischemic infarction (50). Recently, MRimaging studies utilizing diffusion-weighted imaging (DWI) have demonstrated cytotoxicedema early in acute CSVT, preceding the onset of vasogenic edema. These findingssupport the presence of primary neuronal injury early in venous infarction (50).
Once the initial thrombus has formed, the resultant obstruction and venous stasis canpromote propagation of the initial thrombus. Anticoagulant therapy is aimed at preventingextension of the initial thrombus and allowing the fibrinolytic system to achieve dissolution
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
43

of the existing thrombus. Unlike an arterial ischemic stroke, relief of venous obstruction,even if very delayed, may relieve the circulatory congestion in CSVT with clinical benefit.
Figure 4. Deep venous thrombosis: male newbornborn at term developed hypernatremia,dehydration, and seizures at day 8 of life; axialnoncontrast CT shows bilateral thalamichemorrhagic infarction secondary to deep venousthrombosis. Note increased density in the internalcerebral veins and the vein of Galen (arrow).
Thrombotic occlusion of the superior sagittal sinus or the dominant lateral sinus interfereswith the absorption of cerebrospinal fluid (CSF) through impaired function of the“arachnoid granulations” that line the superior sagittal sinus. The latter mechanismfurther increases the extent of cerebral swelling and results in a communicatinghydrocephalus (50).
In addition to the intracerebral and intravascular events in CSVT, pressure on the opticnerves secondary to raised intracranial pressure initially causes papilloedema, which ifunrelieved over time can progress to permanent visual loss.
o Imaging of venous infarction
Venous infarction may be evident on CT as a diffuse low-attenuating lesion. Mass effect iscommon, and, in one study, 40% of symptomatic patients showed CT evidence ofhemorrhage (50). Bilateral, parasagittal, hypoattenuating lesions on CT is a commonfeature of venous thrombosis in the superior sagittal sinus. These lesions do not conform toan arterial distribution but do involve the cortex. Early changes are often subtle, withedema and swelling of the frontal/parietal gyri. In addition, isolated involvement of thetemporal lobe is common and found in cerebral sinus thrombosis of the transverse sinus.Bilateral thalamic hypoattenuating lesions on CT may be evident in deep venousthrombosis and on non-contrast-enhanced CT, thrombus may be seen in the straight sinus.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
44

Figure 5. Deep venous thrombosis in a 27-year-old woman with antiphospholipid antibodysyndrome who presented with headache, nausea, and vomiting that progressed to aphasiaand a decreased level of consciousness. Axial noncontrast CT (A) and T2-weighted MRI (B)show bilateral thalamic ischemia or infarction (open arrow). On CT, a small hemorrhage isseen in the right lateral ventricle (solid arrow). (C) T1-weighted sagittal MRI demonstratessubacute thrombus in the vein of Galen and straight sinus.
Figure 6. Bilateral parasagittal hemorrhages secondary to superior sagittal sinusthrombosis (A) Axial noncontrast CT shows a high attenuation in the superior sagittalsinus (solid arrow) and bilateral parasagittal hemorrhages (open arrows). (B) Fluid-attenuated inversion-recovery sequence in another patient shows mixed-signal-intensitylesions in both frontal lobes with a fluid-fluid level (arrow) in a hematoma cavity on theleft.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
45

MRI is sensitive to the parenchymal changes seen in cerebral sinus thrombosis. Corticaland subcortical high-signal-intensity lesions on fluid-attenuated inversion-recoverysequence and T2-weighted imaging may highly suggest cerebral sinus thrombosis when thelesions do not correspond to an arterial territory (50). Restriction of diffusion on diffusion-weighted imaging (DWI) with a corresponding decrease in the apparent diffusioncoefficient (ADC) value is often irreversible in arterial infarction and correlates with apermanent neurologic deficit (4). Diffusion techniques have been used in cerebral sinusthrombosis to differentiate reversible ischemic tissue from irreversible ischemia (4).Preliminary results have shown some potential in predicting the prognosis of the cerebralsinus thrombosis (50). Recent investigations of cerebral sinus thrombosis have revealedthat mixed signal intensity on DWI may represent both cytotoxic and vasogenic edema (50).A reduced ADC value in CVT may not correlate with neuronal death and a permanentneurologic deficit (50). Therefore, a decrease of ADC in cerebral sinus thrombosis may nothave the same prognostic value as it does in arterial stroke (50), and venous ischemia maybe reversible despite decreased ADC values. This correlates with the important clinicalimprovement that may occur after an initial major cerebral sinus thrombosis-relatedneurologic deficit.
Figure 7. Diffusion imaging. T2-weighted (A) and fluid-attenuated inversion-recoverysequence (B) MRIs show scattered high-signal-intensity lesions (arrows). (C) Diffusion-weighted imaging demonstrates a mixed-signal-intensity area (arrow) suggesting bothcytotoxic and vasogenic edema. (D) ADC map reveals that the lesions are predominantlyhyperintense (arrows).
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
46

o Pathophysiology of cerebral sinus thrombosis and its parenchymal changes
The pathophysiology of brain parenchymal involvement in venous occlusion differs fromthat in arterial occlusion. Parenchymal changes may be secondary to cytotoxic edema,vasogenic edema, or intracranial hemorrhage. The primary underlying mechanism is likelyto be increased venous pressure. If collateral pathways of venous drainage are insufficient,especially in the presence of cortical venous involvement, subsequent parenchymal changesmay occur. If venous pressure continues to increase, with a consequent diminishment inarterial perfusion pressure, cell death may ensue. If adequate collateral pathways developor recanalization occurs before cell death or intracranial hemorrhage, the parenchymalchanges may resolve partly or completely. Vasogenic and cytotoxic edema patterns maycoexist.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
47

Table 4. Effect of increased intracranial venous pressure due to sinovenous thrombosis.(50)
Comment
Venous thrombosis produce effects on the vein that include increase in diameter and length of thethin walled vein, kinking, folding, stenosis, and sometimes occlusion. This has been described as ahemodynamic effect caused by pressure and flow of arterial blood in a vein.
In the presence of venous thrombosis, a subpial or cortical vein dilates, lengthens, and may kinkat the junction with the sinus. It may also balloon to the point of rupture or thromboses The deepvenous collector in the galenic malformations (the embryonic precursor to the vein of Galen)typically shows a dilatation and focal stenosis at the outlet to the straight sinus or a falcine sinus.Occasionally, this structure spontaneously thromboses.
Under normal conditions, there is negative venous pressure in the dural sinuses relative to theheart. There are no valves and pulsatile flow in the sinuses. Blood is effectively sucked throughthe shunt rather than pushed. An increased resistance to flow occurs when the venous pressurerises. This may occur transiently during a Valsalva maneuver or chronically in severe right heartfailure or when there is a stenosis in the venous sinuses due to sinus thrombosis. When there isincreased venous pressure, there is a corresponding decrease in water resorption by thearachnoid granulations, which is reflected in an increased amount of water in the ventricles andsubarachnoid spaces. The third and lateral ventricles become prominent, and the cerebral sulcienlarge. If the fontanelles are open, the head enlarges (macrocrania). Normally, the posteriorfossa drainage relies on the petrosal sinuses draining anteriorly to the cavernous sinus andcaudally to the jugular bulb. In the absence of anterior drainage and restricted caudal drainage,there is an increase in cerebellar water, which results in a small fourth ventricle and tonsillarherniation.
With persistent increase of the venous pressure due to venous thrombosis, there will be reductionof the venous return, stasis of blood, or even reversal of flow of blood (cerebral venous reflux)depending on the degree of venous pressure rise. Stasis of blood in the venous sinuses predisposesto further thrombosis. Cerebral venous reflux predisposes to dilatation of superficial, deepvenous system, transcerebral vein, white matter congestive encephalopathy with edema, petechialhaemorrhages and mass effect. Increase of intravenous pressure often results in venous wallremodelling with increase in diameter and length of the thin walled vein, kinking, folding,stenosis, and sometimes occlusion of thrombosis.
Venous infarction or ischemic cerebral changes can occur due to increased venous pressure -secondary to venous thrombosis, the mechanism for venous infarction is obstruction of venousdrainage with increasing venous pressure in the affected region of the brain. The venouscongestion results in significant extravasation of fluid into the brain, producing focal cerebraledema and hemorrhage. The edema may be transient, if venous flow is re-established, or beassociated with permanent tissue infarction if the increased venous blood pressure eventuallyexceeds the arterial blood pressure. In the latter situation, there is insufficient delivery of arterialblood and regional ischemic infarction. MR imaging studies utilizing diffusion-weighted imaging(DWI) have demonstrated cytotoxic edema early in acute venous thrombosis, preceding the onsetof vasogenic edema. These findings support the presence of primary neuronal injury early invenous infarction.
Under normal conditions, there is negative venous pressure in the dural sinuses relative tothe heart. There are no valves and pulsatile flow in the sinuses. Blood is effectively suckedthrough the shunt rather than pushed. An increased resistance to flow occurs when the
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
48

venous pressure rises. This may occur transiently during a Valsalva maneuver orchronically in severe right heart failure or when there is a stenosis in the venous sinusesdue to sinus thrombosis. Venous hypertension probably passes into three stages dependingupon the degree of venous hypertension and the chronicity of the condition.
Table 5. Stages of cerebral venous hypertension (50)
Stage I
Absence of anyparenchymalchanges
When there is increased venous pressure, there is a corresponding decrease inwater resorption by the arachnoid granulations, which is reflected in anincreased amount of water in the ventricles and subarachnoid spaces. The thirdand lateral ventricles become prominent, and the cerebral sulci enlarge. If thefontanelles are open, the head enlarges (macrocrania). Normally, the posteriorfossa drainage relies on the petrosal sinuses draining anteriorly to the cavernoussinus and caudally to the jugular bulb. In the absence of anterior drainage andrestricted caudal drainage, there is an increase in cerebellar water, which resultsin a small fourth ventricle and tonsillar herniation. At this stage the thrombosedsinus will show the characteristic MRI signal changes but without anyparenchymal changes.
Stage II
Early cerebralcongestiveencephalopathywith reversibleparenchymalchanges
With persistent increase of the venous pressure due to venous thrombosis, therewill be reduction of the venous return, stasis of blood, or even reversal of flow ofblood (cerebral venous reflux) depending on the degree of venous pressure rise.Stasis of blood in the venous sinuses predisposes to further thrombosis. Cerebralvenous reflux predisposes to dilatation of superficial, deep venous system,transcerebral vein, white matter congestive encephalopathy with edema,petechial haemorrhages and mass effect. Increase of intravenous pressure oftenresults in venous wall remodelling with increase in diameter and length of thethin walled vein, kinking, folding, stenosis, and sometimes occlusion ofthrombosis. Parenchymal changes in this stage are due to reversible edemaedema and petechial hemorrhage once venous flow is restored
Stage III
Late cerebralcongestiveencephalopathywith irreversibleparenchymalchanges
Venous infarction or ischemic cerebral changes can occur due to increasedvenous pressure -secondary to venous thrombosis, the mechanism for venousinfarction is obstruction of venous drainage with increasing venous pressure inthe affected region of the brain. The venous congestion results in significantextravasation of fluid into the brain, producing focal cerebral edema andhemorrhage. The edema may be transient, if venous flow is re-established, or beassociated with permanent tissue infarction if the increased venous bloodpressure eventually exceeds the arterial blood pressure. In the latter situation,there is insufficient delivery of arterial blood and regional ischemic infarction.MR imaging studies utilizing diffusion-weighted imaging (DWI) havedemonstrated cytotoxic edema early in acute venous thrombosis, preceding theonset of vasogenic edema. These findings support the presence of primaryneuronal injury early in venous infarction.
Acute dural sinus thrombosis leads to distinct stages of parenchymal changes, the severityof which depends on the degree of venous congestion, which, in turn, is closely related tointradural sinus pressure. As intradural sinus pressure increases, progression from mildparenchymal change to severe cerebral edema and/or hematoma may occur if thrombolysisis delayed.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
49

In the analysis of 29 patients with dural sinus thrombosis (by MRI, and dural sinuspressure measurement using a Tracker 18 end-hole catheter proximal to the thrombus andconnected to a pressure transducer at ear level with the waveform displayed on either anAlpha 9 pressure monitor) , Fong, at al, (49) could identify five stages of brain parenchymalchanges secondary of sinus thrombosis, each stage relates to the dural intrasinus pressure.
Table 6. Parenchymal changes, and intrasinus pressure in dural sinus thrombosis (49)
Acute dural sinus and cerebral venous thrombosis may lead to various stages ofparenchymal changes of venous infarction, with the degree of severity depending on thedegree of venous congestion and elevated dural sinus pressure. The prognosis of venousthrombosis depends to a significant extent on the use of thrombolytics. Severe neurologicsymptoms, including coma, may be reversible if treatment with thrombolytics is startedbefore massive cerebral edema or hemorrhage has developed. Stage I may be treated withanticoagulants alone; however, if the patient deteriorates clinically, prompt thrombolysis isprobably needed. All other stages should be treated with thrombolysis. A progression frommild brain swelling to severe cerebral edema and/or hemorrhage from increasing duralsinus pressure may occur if treatment with thrombolysis is delayed. (50)
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
50

Table 7. Biochemical stages of sinus thromboses (50)
STAGE MRI PICTURE
The acutedeoxyhemoglobinstage of bloodproducts
(days I through5)
In the acute stage of thrombus formation (0–5 days), the signal ispredominantly isointense on T1-weighted images and hypointense onT2-weighted images because of deoxyhemoglobin in red blood cellstrapped in the thrombus. A venous thrombus in the acute stage mayhave a signal intensity that mimics a normal flow state, and such afinding may lead to diagnostic error. The signal may be veryhypointense on T2-weighted images and may be mistakenly thought toindicate a flow void. According to some estimates, in 10%–30% of casesof sinus thrombosis, the thrombus at initial presentation or imagingexamination is in the acute stage of formation. Contrast-enhanced MRvenography or CT venography is usually necessary to achieve adefinitive diagnosis at this stage.
The subacuteextracellularmethemoglobinstage of bloodproducts (fromday 5 throughday 15)
In the subacute stage of thrombus development (6–15 days), the signal ispredominantly hyperintense on both T1-weighted images and T2-weighted images because of methemoglobin in the thrombus. Subacute-stage thrombus has been found in 55% of patients at clinicalpresentation with cerebral venous thrombosis. This stage of formation isthe easiest stage at which to detect a thrombus on MR images, as thesignal intensity of the sinus is most different from that in normal flowstates. The finding of increased signal intensity on both T1-weightedimages and T2-weighted images is almost always abnormal.
Chronic duralsinus thrombosis
The thrombus becomes hypointense and heterogeneous because ofpartial resolution and recanalization and might enhance aftergadolinium administration. Enhancement within the occluded duralsinus is due to organization of the thrombus.
Chronic thrombosis with incomplete recanalization of the sinus maypresent a diagnostic challenge at MR imaging. As many as 15% ofpatients in whom sinus thrombosis is diagnosed at MR imaging mayhave a chronic (>15-day-old) thrombus. Compared with the MR signalin normal brain parenchyma, the signal in a chronic thrombus istypically isointense or hyperintense on T2-weighted images andisointense on T1-weighted images; however, significant variability inthrombus signal intensity exists. The signal intensity may be similar tothat of very slowly moving oxygenated blood.
Sinus enhancement in sinus thrombosis is presumably secondary to an organized thrombuswith intrinsic vascularization as well as to slow flow in dural and intrathrombus collateralchannels.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
51

Parenchymal changes secondary to congestive encephalopathy are shown by MRI assubcortical white matter precontrast T1 hypointensity, with patchy, irregular and linearenhancement and T2 hyperintensity mixed with linear and patchy hypointensity and signalvoid structures. Changes are due to edema, petechial hemorrhages and dilated veins.Parenchymal changes commonly show positive mass effect and are usually focal ratherthan diffuse. Bilateral parenchymal changes are not uncommon. Although parenchymalchanges may occur in areas of the brain that are directly drained by the occluded venoussinus, in some patients the parenchymal changes may not closely correlate with the locationof venous occlusion.
Parenchymal swelling without abnormalities in attenuation or signal intensity on imagesmay occur in as many as 42% of patients with cerebral venous thrombosis. Sulcaleffacement, diminished cistern visibility, and a reduction in ventricular size may occur.Patients with brain swelling and without parenchymal signal intensity changes tend to haveintrasinus pressures in the intermediate range (20–25 mm Hg); however, intrasinuspressures also may be markedly elevated. Such patients typically have more prominentclinical symptoms than would be expected on the basis of imaging findings. (50)
In view of the variable nature of the parenchymal abnormalities that may occur in cerebralvenous thrombosis, the use of the term venous infarct in reference to these lesions should bediscouraged because that term implies irreversibility. In contrast with arterial ischemicstates, many parenchymal abnormalities secondary to venous occlusion are reversible. It ismuch better to refer to these parenchymal changes secondary to cerebral sinus thrombosisas cerebral venous encephalopathy. Persistence of parenchymal MRI signal changes over along time might warrant the usage of the terminology venous infarction. (50)
o Parenchymal hemorrhage in cerebral sinus thrombosis
Parenchymal hemorrhage can be seen in one-third of cases of cerebral venous thrombosis.Flame-shaped irregular zones of lobar hemorrhage in the parasagittal frontal and parietallobes are typical findings in patients with superior sagittal sinus thrombosis and shouldprompt additional imaging evaluations (eg, with MR venography or CT venography).Hemorrhage in the temporal or occipital lobes is more typical of transverse sinus occlusion.Hemorrhage in cerebral venous thrombosis is typically cortical with subcortical extension.Smaller zones of isolated subcortical hemorrhage also may be seen and may beaccompanied by minimal edema. MR imaging with GRE sequences is sensitive in thedepiction of these zones of parenchymal hemorrhage. (50)
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
52

Figure 8. Bilateral hemorrhagic venousinfarction (A) due to superior sagittalthromboses (B)
The mechanism of hemorrhage in cerebral venous thrombosis is multifactorial.Hemorrhage may be precipitated by continued arterial perfusion in areas of cell death, ascan be seen at reperfusion in arterial ischemia. Elevation of venous pressure beyond thelimit of the venous wall also is likely operative. Hemorrhage was noted in patients withintrasinus pressures higher than 42 mm Hg but not in those with lower pressures.
Contrast Enhancement
Parenchymal enhancement in 1%–29% of cases of cerebral venous thrombosis has beenreported. The enhancement is typically gyral in location and may extend into the whitematter. Parenchymal enhancement, which indicates disruption of the blood-brain barrier,may be seen in areas of cytotoxic or vasogenic edema and in the presence of eitherirreversible or reversible brain abnormalities. Increased tentorial enhancement (likelyrelated to dural venous collaterals), adjacent leptomeningeal enhancement, and prominentcortical venous enhancement (secondary to venous congestion) also may be visible after theadministration of contrast material. (50)
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
53

Figure 9. Axial MR image series with a color overlay represents the majorsuperficial cortical venous drainage territories. Most of the superiorcerebrum (green) is drained primarily into the superior sagittal sinus,which also receives drainage from the parasagittal cortical regions at lowerlevels. The sylvian veins drain blood from the peri-insular region (yellow)into the basal dural sinuses. The transverse sinuses receive blood from thetemporal, parietal, and occipital lobes (blue). The Labbé vein, if dominant,may drain much of this territory. Parenchymal abnormalities such ashemorrhage or edema in this territory may be indicative of thrombosis ofthe transverse sinus or Labbé vein.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
54

Figure 10. Axial MR image with color overlay shows the drainage territory of the deepcerebral veins (internal cerebral vein, vein of Galen) (pink), in which parenchymalabnormalities due to deep venous occlusion typically are found. The deep white matter(medullary) venous drainage territory (blue) also is shown.
References
1. Fisher CM, Adams RD. Observations on brain embolism with special reference tothe mechanism of hemorrhagic infarction. J Neuropathol Exp Neurol 10: 92-94,1951.
2. Jorgensen L, Torvik A. Ischaemic cerebrovascular diseases in an autopsy series:Part 2. Prevalence, location, pathogenesis, and clinical course of cerebral infarcts. JNeurol Sci 9: 285-320, 1969.
3. Lodder J, Krijne-Kubat B, Broekman J. Cerebral hemorrhagic infarction atautopsy: Cardiac embolic cause and the relationship to the cause of death. Stroke17: 626-629, 1986.
4. Yamaguchi T, Minematsu K, Choki J, Ikeda M. Clinical and neuroradiologicalanalysis of thrombotic and embolic cerebral infarction. Jpn Circ J 48: 50-58, 1984.
5. Hornig CR, DorndorfW, Agnoli AL. Hemorrhagic cerebral infarction -Aprospective study. Stroke 17: 179-185, 1986.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
55

6. Moulin T, Crepin-Leblond T, Chopard JL, Bogousslavsky J. Hemorrhagic infarcts.Eur Neurol 34: 64-77, 1993.
7. Chaves CJ, Pessin MS, Caplan LR, et al. Cerebellar hemorrhagic infarction.Neurology 46: 346-349, 1996.
8. Toni D, Fiorelli M, Bastianello S, et al. Hemorrhagic transformation of braininfarct: Predictability in the first 5 hours from stroke onset and influence on clinicaloutcome. Neurology 46: 341-345, 1996.
9. Lodder J. CT-detected hemorrhagic infarction: relation with the size of the infarct,and the presence of midline shift. Acta Neurol Scand 70: 329-335, 1984.
10. Cerebral Embolism Study Group. Immediate anticoagulation of embolic stroke:brain hemorrhage and management options. Stroke 15: 779-789, 1984.
11. Cerebral Embolism Study Group. Cardioembolic stroke, early anticoagulation, andbrain hemorrhage. Arch Intern Med 147: 636-640, 1987. 12) Yatsu FM, Hart RG,Mohr JP, Grotta JC. Anticoagulation of embolic strokes of cardiac origin: Anupdate. Neurology 38: 314-316, 1988.
12. Adams HP Jr, Brott TG, Furlan AJ, et al. Guideline for thrombolytic therapy foracute stroke: A supplement to the guidelines for the management of patients withacute ischemic stroke. A statement for healthcare professionals from a specialwriting group of the stroke council, American HeartAssociation. Stroke 27: 1711-1718, 1996.
13. Hacke W, Brott T, Caplan L, et al. Thrombolysis in acute ischemic stroke:controlled trials and clinical experience. Neurology 53 (Suppl 4): S3S14, 1999.
14. Faris AA, Hardin CA, Poser CM. Pathogenesis of hemorrhagic infarction of thebrain. I. Experimental investigations of role of hypertension and of collateralcirculation. Arch Neurol 9: 468-472, 1963.
15. Garcia JH, Lowry SL, Briggs L, et al. Brain Capillaries Expand and Rupture inAreas ofIschemia and Reperfusion. in: Reivich M, Hurtig HI (Eds.)Cerebrovascular Diseases. Raven Press, NewYork, 1983: 169-179.
16. Okada Y, Yamaguchi T, Minematsu K, et al. Hemorrhagic transformation incerebral embolism. Stroke 20: 598-603, 1989.
17. Kimura K, Ogata J, Minematsu K, Yasaka M, Yamaguchi T. Massive pontinehemorrhagic infarction associated with embolic basilar artery occlusion. Intern Med40: 658-661, 2001.
18. Ogata J, Yutani C, Imakita M, et al. Hemorrhagic infarct of the brain without areopening of the occluded arteries in cardioembolic stroke. Stroke 20: 876-883,1989.
19. Weisberg LA. Nonseptic cardiogenic cerebral embolic stroke: clinical-CTcorrelations. Neurology. 1985;35(6):896–899.
20. Ogata J, Fujishima M, Tamaki K, Nakatomi Y, Ishitsuka T, Omae T (1981)Vascular changes underlying cerebral lesions in stroke-prone spontaneouslyhypertensive rats. A serial section study. Acta Neuropathol (Berl) 54:183–188
21. Wagner KR, Kleinholz M, de Courten-Myers GM, Myers RE.: (1992)Hyperglycemic versus normoglycemic stroke: topography of brain metabolites,intracellular pH, and infarct size. J Cereb Blood Flow Metab. 1992 Mar;12(2):213-22. [Abstract]
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
56

22. Broderick JP, Hagen T, Brott T, Tomsick T: Hyperglycemia and hemorrhagictransformation of cerebral infarcts. Stroke. 1995 Mar;26(3):484-7.
23. Berger C, Fiorelli M, Steiner T, et al. Hemorrhagic Transformation of IschemicBrain Tissue: Asymptomatic or Symptomatic? Stroke. 2001; 32: 1330-1335.
24. Giuseppe Micieli, Simona Marcheselli, Piera Angela Tosi. Safety and efficacy ofalteplase in the treatment of acute ischemic stroke. Vascular Health and RiskManagement 2009;5: 397-409.
25. Savitz SI, Lew R, Bluhmki E, et al. Shift analysis versus dichotomization of themodified Rankin scale outcome scores in the NINDS and ECASS II trials. Stroke.2007; 38: 3205-3212.
26. Caplan LR. Stroke thrombolysis: slow progress. Circulation. 2006;114:187-190.27. Sumii T, Lo EH. Involvement of matrix metalloproteinase in thrombolysis-
associated hemorrhagic transformation after embolic focal ischemia in rats. Stroke.2002;33:831-836.
28. Giuseppe Micieli, Simona Marcheselli, Piera Angela Tosi. Safety and efficacy ofalteplase in the treatment of acute ischemic stroke. Vascular Health and RiskManagement 2009;5: 397-409.
29. Montaner J, Molina CA, Monasterio J, et al. Matrix metalloproteinase-9pretreatment level predicts intracranial hemorrhagic complications afterthrombolysis in human stroke. Circulation. 2003;107:598-603.
30. Derex L, Hermier M, Adeleine P, et al. Clinical and imaging predictors ofintracerebral hemorrhage in stroke patients treated with intravenous tissueplasminogen activator. J Neurol Neurosurg Psychiatry.2005;76:70-75.
31. Cocho D, Borrell M, Marti-Fabregas J, et al. Pretreatment hemostatic markers ofsymptomatic intracerebral hemorrhage in patients treated with tissue plasminogenactivator. Stroke. 2006;37:996-999.
32. Berrouschot J, R0ther J, Glahn J, et al. Outcome and severe hemorrhagiccomplications of intravenous thrombolysis with tissue plasminogen activator in veryold stroke patients. Stroke. 2005;36:2421-2425.
33. Heuschmann PU, Kolominsky-Rabas PL, Roether J, et al. Predictors of in-hospitalmortality in patients with acute ischemic stroke treated with thrombolytic therapy.JAMA. 2004;292:1831-1838
34. Ribo M, Montaner J, Molina CA, et al. Admission fibrinolytic profile is associatedwith symptomatic hemorrhagic transformation in stroke patients treated with tissueplasminogen activator. Stroke. 2004;35:2123-2127.
35. Capes SE, Hunt D, Malmberg K, et al. Stress hyperglycemia and prognosis of strokein nondiabetic and diabetic patients: a systematic overview. Stroke. 2001;32:2426-2432.
36. Lindsbert P. Brain tissue salvage in acute stroke. Neurocrit Care. 2004;1:301-308.37. Kase CS, Furlan AJ, Wechsler LR, et al. Cerebral hemorrhage after intra-arterial
thrombolysis for ischemic stroke: the PROACT II trial.Neurology. 2001;57:1603-1610.
38. Barak ERJ, Kamalian S, Rezai Gharai L, et al. Does hyperacute diffusion andperfusion weighted imaging predict outcome in acute ischemic stroke. InternationalStroke Conference. 2008; 39: 607.
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
57

39. Barber PA, Demchuk AM, Zhang J, et al. Validity and reliability of a quantitativecomputed tomography score in predicting outcome of hyperacute stroke beforethrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme EarlyCT Score. Lancet. 2000;355:1670-1674.
40. Neumann-Haefelin T, Hoelig S, Berkefeld J, et al. Leukoaraiosis is a risk factor forsymptomatic intracerebral hemorrhage after thrombolysis for acute stroke. Stroke.2006;37:2463-2466.
41. Kakuda W, Thijs VN, Lansberg MG, et al. Clinical importance of microbleeds inpatients receiving IV thrombolysis. Neurology. 2005;65:1175-1178.
42. Fiehler J, Albers GW, Boulanger JM, et al. Bleeding risk analysis in stroke imagingbefore thromboLysis (BRASIL): pooled analysis of T2*-weighted magneticresonance imaging data from 570 patients. Stroke. 2007;38:2738-2744.
43. Thomalla G, Sobesky J, Kohrmann M, et al. Two tales: hemorrhagictransformation but not parenchymal hemorrhage after thrombolysis is related toseverity and duration of ischemia. MRI study of acute stroke patients treated withintravenous tissue plasminogen activator within 6 hours. Stroke. 2007;38:313-318.
44. Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with Alteplase 3 to 4.5 hoursafter Acute Ischemic Stroke. N Engl J Med. 2008; 359: 1317-1329.
45. Metwally Y. Onlines newspapers. Cerebrovascular disorders (stroke) 2010.Available from: http://yassermetwally.com/
46. Metwally Y. Onlines newspapers. Medical management of stroke 2010. Availablefrom: http://yassermetwally.com/
47. Metwally Y. Onlines newspapers. Thrombolytic therapy in stroke management2010. Available from: http://yassermetwally.com/
48. Von Kummer R. Early major ischemic changes on computed tomography shouldpreclude use of tissue plasminogen activator. Stroke.2003; 34: 820-821.
49. Fong Y. Tsai, Ay-Ming Wang, Violet B. Matovich, Mark Lavin, Bruce Berberian,Tereasa M, at al: MR Staging of Acute Dural Sinus Thrombosis: Correlation withVenous Pressure Measurements and Implications for Treatment and Prognosis. AmJ Neuroradiol 16:1021–1029, May 1995
50. Metwally, MYM: Textbook of neuroimaging, A CD-ROM publication, (Metwally,MYM editor) WEB-CD agency for electronic publication, version 11.2a. April 2010
www.yassermetwally.com
Professor Yasser Metwallywww.yassermetwally.com
58

INTRODUCTION
EXTERNAL WATERSHED(BORDER ZONE)INFARCTION
INTERNAL WATERSHED(BORDER ZONE)INFARCTS
CORTICAL LAMINARNECROSIS
INTRODUCTION
Border zone or watershed infarcts are ischemic lesions that occur in characteristiclocations at the junction between two main arterial territories. These lesions constituteapproximately 10% of all brain infarcts and are well described in the literature. Theirpathophysiology has not yet been fully elucidated, but a commonly accepted hypothesisholds that decreased perfusion in the distal regions of the vascular territories leaves themvulnerable to infarction. Two types of border zone infarcts are recognized: external(cortical) and internal (subcortical). To select the most appropriate methods for managingthese infarcts, it is important to understand the underlying causal mechanisms. Internalborder zone infarcts are caused mainly by hemodynamic compromise, whereas externalborder zone infarcts are believed to result from embolism but not always with associatedhypoperfusion. Various imaging modalities have been used to determine the presence andextent of hemodynamic compromise or misery perfusion in association with border zoneinfarcts, and some findings (eg, multiple small internal infarcts) have proved to beindependent predictors of subsequent ischemic stroke. A combination of several advanced
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
59

techniques (eg, diffusion and perfusion magnetic resonance imaging and computedtomography, positron emission tomography, transcranial Doppler ultrasonography) can beuseful for identifying the pathophysiologic process, making an early clinical diagnosis,guiding management, and predicting the outcome.
Watersheds or border zones are areas that lie at the junction of two different drainageareas. The vascular supply of the cerebral parenchyma can be envisioned in a similarmanner, with defined boundaries between different arterial systems. Cerebral infarcts inborder zones were first discussed in 1883 (1) and were defined as ischemic lesions in anarea between two neighboring vascular territories (2). These territories can be furtherclassified in two broad categories as (a) external (cortical) or (b) internal (subcortical)border zones. Border zone infarcts constitute approximately 10% of all cerebral infarcts(3). Various theories have been proposed to explain their pathogenesis. It is believed thatrepeated episodes of severe systemic hypotension are the most frequent cause (3).Susceptibility of border zones to ischemia was proved in an autopsy study of patients withborder zone infarcts (4). Various neuropathologic studies have shown neuronal necrosisfrom hypotension in these regions and have advanced our understanding of thepreferential distribution of border zone infarcts (5,6).
The appearances of border zone infarcts depicted by standard imaging modalities are welldescribed. Advanced imaging techniques can help identify areas of misery perfusionassociated with these infarcts. Misery perfusion represents a chronic failure of cerebralautoregulation associated with decreased cerebral perfusion pressures in the presence ofextracranial and intracranial atheromatous disease. The important information derivedfrom imaging can be useful for patient management and disease prognosis.
The article begins with a discussion of the anatomic locations, classification, andpathophysiology of border zone infarcts. The existing literature about the causalmechanisms of associated hemodynamic compromise is reviewed, and the imagingappearances of the lesions are described in detail.
Classification of Border Zone Infarcts
Border zone infarcts are grouped into two main categories based on their location in eitherexternal (cortical) or internal (subcortical) regions at axial computed tomography (CT).Various terms for these lesions have been used in the literature, with the most commonsummarized in the Table 1.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
60

Table 1. Border Zone Infarcts
The external or cortical border zones are located at the junctions of the anterior, middle,and posterior cerebral artery territories. Infarcts in the anterior external border zones andparamedian white matter are found at the junction of the territories supplied by theanterior and middle cerebral arteries, and those in the parieto-occipital areas (posteriorexternal border zones) are found at the junction of the territories supplied by the middleand posterior cerebral arteries.
The internal or subcortical border zones are located at the junctions of the anterior,middle, and posterior cerebral artery territories with the Heubner, lenticulostriate, andanterior choroidal artery territories. Internal border zone infarcts thus may be designatedas infarcts of the lenticulostriate–middle cerebral artery, lenticulostriate–anterior cerebralartery, Heubner–anterior cerebral artery, anterior choroidal–middle cerebral artery, andanterior choroidal–posterior cerebral artery territories (7). Infarcts of the lenticulostriate–middle cerebral artery border zone, which is supplied by the end branches of deepperforating lenticulostriate arteries and medullary penetrators from the pial–middlecerebral artery, are the most commonly seen at imaging.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
61

Color plate 1. Watershed infarcts occur at the border zones between major cerebralarterial territories as a result of hypoperfusion. There are two patterns of border zoneinfarcts: 1.Cortical border zone infarctions Infarctions of the cortex and adjacentsubcortical white matter located at the border zone of ACA/MCA and MCA/PCA2.Internal border zone infarctions Infarctions of the deep white matter of the centrumsemiovale and corona radiata at the border zone between lenticulostriate perforators andthe deep penetrating cortical branches of the MCA or at the border zone of deep whitematter branches of the MCA and the ACA.
Pathophysiology of Border Zone Infarcts
Border zone infarcts involve the junction of the distal fields of two nonanastomosingarterial systems (8). The conventional theory implicates hemodynamic compromiseproduced by repeated episodes of hypotension in the presence of a severe arterial stenosisor occlusion. The lower perfusion pressure found within the border zone areas in thissetting confers an increased susceptibility to ischemia, which can lead to infarction. Thiscausal role of severe arterial hypotension has been well described and confirmed by theresults of experimental studies in animals (9,10). The typical clinical manifestations ofsyncope, hypotension, and episodic fluctuating or progressive weakness of the hands arealso supportive of this theory of hemodynamic failure (11,12). Radiologic studies alsosupport the hypothesis that border zone infarcts distal to internal carotid artery disease aremore likely to occur in the presence of a noncompetent circle of Willis.
In sharp contrast with this widely prevalent interpretation, several pathologicinvestigations have emphasized an association between border zone infarction andmicroemboli, and embolic material has been found within areas of border zone infarctionin autopsy series (13). Preferential propagation of emboli in the border zone regions alsohas been found in experimental studies (14).
Border zone infarction may be better explained by invoking a combination of two ofteninterrelated processes: hypoperfusion and embolization (15). Hypoperfusion, or decreased
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
62

blood flow, is likely to impede the clearance (washout) of emboli. Because perfusion is mostlikely to be impaired in border zone regions, clearance of emboli will be most impaired inthese regions of least blood flow. Severe occlusive disease of the internal carotid arterycauses both embolization and decreased perfusion. Similarly, cardiac disease is oftenassociated with microembolization from the heart and aorta with periods of diminishedsystemic and brain perfusion. This theory, although it seems reasonable, remains unprovedand has been challenged on many accounts.
Color plate 2. This coronal section of the cerebral hemispheres demonstrates the result of asevere global hypoxic-ischemic insult. It is from a person who was resuscitated afterexperiencing a large pulmonary embolus with severe hypoxia and hypotension. She livedseveral months following the event, first in coma, then in a vegetative state. This sectionshows marked thinning of the majority of the cortical ribbon (compare to normal) andatrophy of the deep gray structures. The lateral ventricles are secondarily enlarged; thispassive enlargement of the ventricles as a result of loss of brain tissue is known ashydrocephalus ex vacuo.
EXTERNAL WATERSHED (BORDER ZONE) INFARCTION
Anterior external border zone infarctso Imaging Appearance
The external, cortical border zones are located between the anterior, middle, and posteriorcerebral arteries and are usually wedge-shaped or ovoid. However, their location may varywith differences in the arterial supply. It is sometimes difficult to determine whether aperson has sustained a border zone infarct on the basis of the location of the infarct in
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
63

relation to the vessels on a CT or MR image (16,17). Because of this extensive anatomicvariation, minimum and maximum distribution territories of each vessel have beendefined. It is not uncommon to describe a cortical infarct as a “territorial” infarct if it liescompletely within the expected or possible maximum area of a vascular territory or as a“potential” infarct if it is outside these maxima (18). Furthermore, the location of corticalborder zones may vary because of the development of leptomeningeal collaterals (8). Theanatomy of cortical border zones can be complex, with marked variability due to individualdifferences in the territories supplied by the major arteries of the brain.
Color plate 3. The bilaterally symmetric dark discolored areas seen superiorly and justlateral to the midline represent recent infarction in the watershed zone between anteriorand middle cerebral arterial circulations. Such watershed infarctions can occur withrelative or absolute hypoperfusion of the brain.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
64

Figure 1. Coronal fluid-attenuated inversion recovery MR images show the distribution ofexternal (cortical) border zone infarcts at the junctions of the anterior cerebral artery andmiddle cerebral artery territories (A) and the middle cerebral artery and posteriorcerebral artery territories (B). (C) Diffusion-weighted MR images show a cortical borderzone infarct at the junction of the anterior cerebral artery and middle cerebral arteryterritories. Angiography of the right-sided common carotid and internal carotid arteries inthe same patient showed normal vessels with no occlusion or stenosis.
o Causal Mechanisms
The mechanism of external border zone infarction has been widely debated. Many studieshave documented hemodynamic abnormalities in the anterior watershed or frontal corticalborder zone. However, in many studies, no evidence of such hemodynamic impairment wasfound (19). In other studies, substantially fewer severe stenoses or occlusions of majorvessels than border zone infarcts were found (20). The cerebral or carotid vessels mayappear entirely normal or show mild or moderate narrowing without hemodynamiccompromise. Isolated cortical border zone infarcts may be embolic in nature and are lessfrequently associated with hemodynamic compromise. Microemboli from the heart oratherosclerotic plaques in major arteries may preferentially propagate to cortical borderzones, which have lower perfusion than other areas of the vasculature, and, thus, a limitedability to wash out these emboli. Many patients with cortical border zone infarcts haveconcomitant smaller cortical infarcts. These findings support the hypothesis that anembolic mechanism plays a crucial role in the pathogenesis of external border zoneinfarcts.
Figure 1. Coronal fluid-attenuated inversion recovery MR images show the distribution ofexternal (cortical) border zone infarcts at the junctions of the anterior cerebral artery andmiddle cerebral artery territories (A) and the middle cerebral artery and posteriorcerebral artery territories (B). (C) Diffusion-weighted MR images show a cortical borderzone infarct at the junction of the anterior cerebral artery and middle cerebral arteryterritories. Angiography of the right-sided common carotid and internal carotid arteries inthe same patient showed normal vessels with no occlusion or stenosis.
o Causal Mechanisms
The mechanism of external border zone infarction has been widely debated. Many studieshave documented hemodynamic abnormalities in the anterior watershed or frontal corticalborder zone. However, in many studies, no evidence of such hemodynamic impairment wasfound (19). In other studies, substantially fewer severe stenoses or occlusions of majorvessels than border zone infarcts were found (20). The cerebral or carotid vessels mayappear entirely normal or show mild or moderate narrowing without hemodynamiccompromise. Isolated cortical border zone infarcts may be embolic in nature and are lessfrequently associated with hemodynamic compromise. Microemboli from the heart oratherosclerotic plaques in major arteries may preferentially propagate to cortical borderzones, which have lower perfusion than other areas of the vasculature, and, thus, a limitedability to wash out these emboli. Many patients with cortical border zone infarcts haveconcomitant smaller cortical infarcts. These findings support the hypothesis that anembolic mechanism plays a crucial role in the pathogenesis of external border zoneinfarcts.
Figure 1. Coronal fluid-attenuated inversion recovery MR images show the distribution ofexternal (cortical) border zone infarcts at the junctions of the anterior cerebral artery andmiddle cerebral artery territories (A) and the middle cerebral artery and posteriorcerebral artery territories (B). (C) Diffusion-weighted MR images show a cortical borderzone infarct at the junction of the anterior cerebral artery and middle cerebral arteryterritories. Angiography of the right-sided common carotid and internal carotid arteries inthe same patient showed normal vessels with no occlusion or stenosis.
o Causal Mechanisms
The mechanism of external border zone infarction has been widely debated. Many studieshave documented hemodynamic abnormalities in the anterior watershed or frontal corticalborder zone. However, in many studies, no evidence of such hemodynamic impairment wasfound (19). In other studies, substantially fewer severe stenoses or occlusions of majorvessels than border zone infarcts were found (20). The cerebral or carotid vessels mayappear entirely normal or show mild or moderate narrowing without hemodynamiccompromise. Isolated cortical border zone infarcts may be embolic in nature and are lessfrequently associated with hemodynamic compromise. Microemboli from the heart oratherosclerotic plaques in major arteries may preferentially propagate to cortical borderzones, which have lower perfusion than other areas of the vasculature, and, thus, a limitedability to wash out these emboli. Many patients with cortical border zone infarcts haveconcomitant smaller cortical infarcts. These findings support the hypothesis that anembolic mechanism plays a crucial role in the pathogenesis of external border zoneinfarcts.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
65

o Clinical Course
Patients with external border zone infarcts have a more benign clinical course and a betterprognosis than those with internal border zone infarcts, although the severity of clinicalsigns and symptoms and the score on the National Institutes of Health Stroke Scale at thetime of admission might not differ substantially between the two patient groups. Theexternal border zone is closer to the cortical surface, where penetrating arteries originate,and thus it has a better chance of developing a collateral supply through leptomeningeal ordural anastomoses. However, when external border zone infarcts occur in association withinternal border zone infarcts, there is a higher probability of hemodynamic impairment,and the prognosis may not be good (21).
Figure 2. Bilateral border infarcts.. A 60 yo male brought unconscious to casualty withpossible cardiac event. On admission MRI Diffusion show bilateral fronto parietal andparieto occipital cortical restricted diffusion. Similar restricted diffusion in caudate nuclei.Area of involvement corresponds to cortical as well as internal border zone infarcts.
Posterior External (Cortical) Border Zone Infarcts
Anterior external border zone infarcts are more common than posterior ones because ofthe high prevalence of internal carotid artery disease. Vertebrobasilar system disease withsuperimposed fetal circulation (ie, a fetal-type posterior cerebral artery) may lead toposterior external border zone infarcts. Unilateral posterior external border zone infarctshave been related to cerebral emboli either of cardiac origin or from the common carotidartery, whereas bilateral infarcts are more likely to be caused by underlying hemodynamicimpairment (vascular stenosis) (27).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
66

Figure 3. Axial diffusion-weighted MR image andapparent diffusioncoefficient map showbilateral posteriorcortical border zoneinfarcts.
INTERNAL WATERSHED (BORDER ZONE) INFARCTS
Imaging Appearance
Internal border zone infarcts appear in multiples, in a rosarylike pattern. In one report,this pattern was described as a series of three or more lesions, each with a diameter of 3mm or more, arranged in a linear fashion parallel to the lateral ventricle in the centrumsemiovale or corona radiata (19). Internal border zone infarcts are classified on the basis oftheir radiologic appearance as either confluent or partial (8). Partial infarcts are usuallylarge, cigar shaped, and arranged in a pattern resembling the beads of a rosary, paralleland adjacent to the lateral ventricle. The duration of hemodynamic compromise has beenpostulated as the cause of the varied radiologic appearances, with a brief episode ofcompromise leading to a partial infarct, and a longer period of compromise, to confluentinfarcts (22). Confluent internal border zone infarcts may be manifested by a stepwiseonset of contralateral hemiplegia. They also may be associated with a poorer recovery thanis typical for partial infarcts.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
67

Figure 4. FLAIR and MRI T2 images showing examples of Internal border zone infarcts
Internal border zone infarcts must be differentiated from superficial perforator(medullary) infarcts, which may have a similar appearance on MR images. Superficialperforator infarcts, which are caused by the occlusion of medullary arteries from pialplexuses, are smaller, superficially located, and widely scattered, whereas internal borderzone infarcts tend to localize in paraventricular regions (23). Superficial perforator infarctsare associated with less severe vascular stenoses and a better prognosis than internalborder zone infarcts. Because of the difficulty of differentiating between the two types ofinfarcts on radiologic images, they have sometimes been collectively described assubcortical white matter infarcts, but that term is diagnostically nonspecific.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
68

Figure 5. Internal watershed infarction
o Causal Mechanisms
In contrast to external border zone infarcts, internal border zone infarcts are causedmainly by arterial stenosis or occlusion, or hemodynamic compromise. The greatervulnerability of internal border zones to hemodynamic compromise has been explained onthe basis of anatomic characteristics of the cerebral arterioles within these zones. Theinternal border zones are supplied by medullary penetrating vessels of the middle andanterior cerebral arteries and by deep perforating lenticulostriate branches. The medullarypenetrating arteries are the most distal branches of the internal carotid artery and have thelowest perfusion pressure. The deep perforating lenticulostriate arteries have littlecollateral supply, and there are no anastomoses between the deep perforators and the whitematter medullary arterioles. Therefore, the centrum semiovale and corona radiata aremore susceptible than other regions to ischemic insults in the setting of hemodynamiccompromise.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
69

Figure 6. Internalwatershed infarction
o Clinical Course
Internal border zone infarcts are associated with a poor prognosis and clinicaldeterioration (21,22). Patients may undergo prolonged hospitalization, and they have anincreased likelihood of remaining in a disabled state during clinical follow-up. The resultsof diffusion-weighted imaging studies suggest that patients with internal border zoneinfarcts have an increased risk for stroke during the first few days after infarction (24).Perfusion studies in patients with such infarcts have shown a far greater area of miseryperfusion than is reflected on diffusion-weighted images. Involvement of the adjacentcortex also has been found on perfusion images (25). Thus, the typically small internalborder zone infarcts represent the “tip of the iceberg” of decreased perfusion reserve andmay be predictive of impending stroke. This hypothesis was tested further withquantitative carbon 11–flumazenil positron emission tomography (PET), which showed adecrease in benzodiazepine receptors, a finding suggestive of neuronal damage beyond theregion of infarction seen on MR images (26).
Conclusions
Internal (subcortical) border zone infarcts, which typically appear in a linear rosarylikepattern in the centrum semiovale, are caused mainly by hemodynamic compromise.External (cortical) border zone infarcts are believed to be caused by embolism, sometimeswith associated hypoperfusion. External border zone infarcts usually follow a benignclinical course, whereas internal border zone infarcts are associated with higher morbidityand a higher risk for future stroke. Different therapeutic approaches may be required toprevent early clinical deterioration in patients with different types of border zone infarcts.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
70

CORTICAL LAMINAR NECROSIS
Cortical laminar necrosis occurs as a consequence of oxygen or glucose depletion in thewatershed intracortical area in the third cortical layer, as in anoxia, hypoglycaemia, statusepilepticus, ischaemic stroke CNS vasculitis, neuro-lupus and drugs (46). Corticalpseudolaminar necrosis, also known as cortical laminar necrosis and simply laminarnecrosis, is the (uncontrolled) death of cells in the (cerebral) cortex of the brain in a band-like pattern, (46) with a relative preservation of cells immediately adjacent to the meninges.Pathologically Cortical laminar necrosis represents cytotoxic oedema affecting a particularlayer of cerebral cortex (third grey matter layer) at the acute stage and isneuropathologically characterized by delayed selective neuronal necrosis at the acute stagefollowed by reactive change of glia and deposition of fat-laden macrophages. In particularthe characteristic high intensity on precontrast Tl-weighted images in Cortical laminarnecrosis, which generally begins to appear about 2 weeks after the ictus, becomesprominent at 1-2 months and began to fade at 3-11 months, is due to the deposition of fat-laden macrophages or methemoglobin representing intracortical microhemorrhages.
Chronic brain infarcts are typically seen as low-intensity lesions on T1-weighted and high-intensity lesions on T2- weighted images due to prolonged T1 and T2 values (46). In someinfarcts, high-intensity lesions are observed on precontrast T1-weighted images.Haemorrhagic infarcts show characteristic changes of the signal intensity, similar to thoseof haemorrhage, due to deoxyhaemoglobin, methohaemoglobin, and haemosiderin (52,53).Petechial haemorrhage may occur in cortical infarcts (cortical laminar necrosis) but cannotexplain the high-intensity laminar lesions in all patients on precontrast TI images (46,47).In general high intensity on precontrast Tl-weighted images (T1 shortening) can be due tomethaemoglobin, mucin, high protein concentration, lipid or cholesterol, calcification andcortical laminar necrosis (51). In ischaemic stroke, high intensity laminar lesions can becortical laminar necrosis, haemorrhagic infarcts (microhaemorrhage), or a combination ofthe two.
The grey matter has six layers. The third is the most vulnerable to depletion of oxygen andglucose (watershed intracortical zone). When a relatively mild ischaemic or hypoglycaemicinsult occurs, the vulnerable layers are selectively injured (selective neuronal vulnerability)(64).
Because the third grey matter layer is the most vulnerable to anoxia and hypoglycemia,Cortical laminar necrosis is a specific type of cortical infarction, usually seen in the settingof anoxic encephalopathy. Other etiologies like hypoglycemia, status epilepticus andimmunosuppressive chemotherapy have been implicated. (55,56) The appearance of theMR images in the setting of diffuse cortical laminar necrosis can be deceptive. Properlywindowed diffusion weighted imaging can be very helpful in detecting cortical laminarnecrosis, especially in the setting of anoxic-hypoxic encephalopathy in the early subacutephase. (57) Cortical laminar necrosis in the setting of anoxic encephalopathy has auniversally poor prognosis, with most patients either progressing to brain death orremaining in a persistent vegetative state. (56).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
71

Boyko et al. (51) described cortical laminar necrosis in brain infarcts as linear high onprecontrast TI imags signal based on the cortical surface and becoming less intense overtime (months). In hypoxic brain damage, Precontrast Tl-weighted images revealed alaminar hyperintensity lesion in the cortex in the late subacute stage (21-28 days) whichtended to fade after 2 months but persisted up to 11 months (46). In laminar corticalnecrosis, cortical high intensity on precontrast Tl-weighted images generally begins toappear about 2 weeks after the ictus, became prominent at 1-2 months and began to fade at3 months, although it could persist up to 11 months. FLAIR images are more sensitive thanTl weighted images to the cortical laminar lesions. Early cortical changes on day 1 showedhigh intensity on T2- weighted images and low intensity on Tl-weighted images, which laterbecame high intensity on precontrast T1 images. This early change is due to prolonged Tland T2 values caused by acute ischaemic change (tissue oedema).
The cortical laminar necrosis, seen as a laminar high signal lesion on precontrast T1-weighted images, was first described by Sawada et al. (55) in a patient with anoxicencephalopathy. The cortical lesion is usually in the watershed region (watershedintracortical zone) in this condition (46). Cortical laminar necrosis is also reported inischaemic stroke (46,47,48,49). Although Nabatame et al. {50} thought the high intensity onprecontrast T1-weighted images was due to methohaemoglobin in haemorrhagic tissue,pathological studies revealed no haemorrhage (46,50,51). Takahashi et al. (54) reported apatient with a cortical laminar lesion showing low intensity on T2-weighted images in thechronic stage, which they thought due to haemosiderin.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
72

Color plate 4. Cortical laminar necrosis.
Color plate 5. Cortical laminar necrosis. Earlyin the disease, gross findings will becharacterized by edema and swelling. Note theswollen glistening appearance of the cerebralcortex. Note the vague line between cortex andsubcortical white matter (arrows).Histologically this line would correspond to anearly (laminar) band of cortical necrosis.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
73

Figure 7. A 60-year-old woman with an anti phospholipid antibody syndrome. All images 1month after ictus. a A Tl weighted image shows a high-intensity right occipital laminarlesion, with low intensity in white matter. b There is intense contrast enhancement of thegrey matter, none of the white matter. c A T2-weighted image demonstrates an isointenselaminar lesion, while the white matter shows very high intensity. d A proton-density imagedemonstrates the high-intensity laminar cortical lesion.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
74

Figure 8. A 73-year-old man with speech disturbance. a At 1.5 months after the ictus, aprecontrast T1-weighted image demonstrates a high-intensity left parietal laminar lesion(arrow). B, At 6 months, there is no high intensity and no contrast enhancement (C), but aFLAIR image (D) still shows a high-intensity laminar lesion.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
75

Figure 9. Precontrast T1 image showing cortical laminar necrosis demonstrated as alaminar linear cortical hyperintensity.
References
1. Pozzi S . Sur un cas de cirrhose atrophique granuleuse disseminee des circonvolutionscerebrales. Encephale 1883;3:155–177.
2. Schneider M . Durchblutung und sauerstoffversorgung des gehirns. Verh Dtsch TesKreislaufforsch 1953;19:3–12.
3. Torvik A . The pathogenesis of watershed infarcts in the brain. Stroke 1984;15(2):221–223.
4. Romanul FC, Abramowicz A . Changes in brain and pial vessels in arterial border zones.Arch Neurol 1964;11:40–65.
5. Adams JH, Brierley JB, Connor RCR, Treip CS . The effects of systemic hypotensionupon the human brain: clinical and neuropathological observations in 11 cases. Brain1966;89(2):235–268.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
76

6. Brierley JB, Prior PF, Calverley J, Jackson SJ, Brown AW . The pathogenesis ofischaemic neuronal damage along the cerebral arterial boundary zones in Papio anubis.Brain 1980;103(4):929–965.
7. Del Sette M, Eliasziw M, Streifler JY, Hachinski VC, Fox AJ, Barnett HJ . Internalborderzone infarction: a marker for severe stenosis in patients with symptomatic internalcarotid artery disease. For the North American Symptomatic Carotid Endarterectomy(NASCET) Group. Stroke 2000;31(3): 631–636.
8. Momjian-Mayor I, Baron JC . The pathophysiology of watershed infarction in internalcarotid artery disease: review of cerebral perfusion studies. Stroke 2005;36(3):567–577.
9. Howard R, Trend P, Russell RW . Clinical features of ischemia in cerebral arterialborder zones after periods of reduced cerebral blood flow. Arch Neurol 1987;44(9):934–940.
10. Brierley JB, Excell BJ . The effects of profound systemic hypotension upon the brain ofM. rhesus: physiological and pathological observations. Brain 1966;89(2):269–298.
11. Bogousslavsky J, Regli F . Unilateral watershed cerebral infarcts. Neurology1986;36(3):373–377.
12. Bladin CF, Chambers BR . Clinical features, pathogenesis, and computed tomographiccharacteristics of internal watershed infarction. Stroke 1993;24(12):1925–1932.
13. Masuda J, Yutani C, Ogata J, Kuriyama Y, Yamaguchi T . Atheromatous embolism inthe brain: a clinicopathologic analysis of 15 autopsy cases. Neurology 1994;44(7):1231–1237.
14. Pollanen MS, Deck JHN . The mechanism of embolic watershed infarction:experimental studies. Can J Neurol Sci 1990;17(4):395–398.
15. Caplan LR, Hennerici M . Impaired clearance of emboli (washout) is an important linkbetween hypoperfusion, embolism, and ischemic stroke. Arch Neurol 1998;55(11):1475–1482.
16. van der Zwan A, Hillen B . Review of the variability of the territories of the majorcerebral arteries. Stroke 1991;22(8):1078–1084.
17. van der Zwan A, Hillen B, Tulleken CA, Dujovny M . A quantitative investigation ofthe variability of the major cerebral arterial territories. Stroke 1993; 24(12):1951–1959.
18. Provenzale JM, Jahan R, Naidich TP, Fox AJ . Assessment of the patient withhyperacute stroke: imaging and therapy. Radiology 2003;229(2):347–359.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
77

19. Derdeyn CP, Khosla A, Videen TO, et al . Severe hemodynamic impairment and borderzone region infarction. Radiology 2001;220(1):195–201.
20. Yong SW, Bang OY, Lee PH, Li WY . Internal and cortical border-zone infarction:clinical and diffusion-weighted imaging features. Stroke 2006;37(3): 841–846.
21. Moriwaki H, Matsumoto M, Hashikawa K, et al. Hemodynamic aspect of cerebralwatershed infarction: assessment of perfusion reserve using iodine-123-iodoamphetamineSPECT. J Nucl Med 1997; 38(10):1556–1562.
22. Krapf H, Widder B, Skalej M . Small rosarylike infarctions in the centrum ovalesuggest hemodynamic failure. AJNR Am J Neuroradiol 1998;19(8): 1479–1484.
23. Lee PH, Bang OY, Oh SH, Joo IS, Huh K . Subcortical white matter infarcts:comparison of superficial perforating artery and internal border-zone infarcts usingdiffusion-weighted magnetic resonance imaging. Stroke 2003;34(11):2630–2635.
24. Bang OY, Lee PH, Heo KG, Joo US, Yoon SR, Kim SY . Specific DWI lesion patternspredict prognosis after acute ischaemic stroke within the MCA territory. J NeurolNeurosurg Psychiatry 2005;76(9): 1222–1228.
25. Arakawa S, Minematsu K, Hirano T, et al . Topographic distribution of miseryperfusion in relation to internal and superficial borderzones. AJNR Am J Neuroradiol2003;24(3):427–435.
26. Yamauchi H, Kudoh T, Kishibe Y, Iwasaki J, Kagawa S . Selective neuronal damageand borderzone infarction in carotid artery occlusive disease: a 11C-flumazenil PET study.J Nucl Med 2005;46(12): 1973–1979.
27. Belden JR, Caplan LR, Pessin MS, Kwan E . Mechanisms and clinical features ofposterior border-zone infarcts. Neurology 1999;53(6):1312–1318.
28. Bartynski WS, Grabb BC, Zeigler Z, Lin L, Andrews DF . Watershed imaging featuresand clinical vascular injury in cyclosporin A neurotoxicity. J Comput Assist Tomogr1997;21(6):872–880.
29. Sarazin M, Caumes E, Cohen A, Amarenco P . Multiple microembolic borderzonebrain infarctions and endomyocardial fibrosis in idiopathic hypereosinophilic syndromeand in Schistosoma mansoni infestation. J Neurol Neurosurg Psychiatry 2004;75(2): 305–307.
30. McMillan HJ, Johnston DL, Doja A . Watershed infarction due to acutehypereosinophilia. Neurology 2008;70(1):80–82.
31. Tatu L, Moulin T, Bogousslavsky J, Duvernoy H . Arterial territories of human brain:brainstem and cerebellum. Neurology 1996;47(5):1125–1135.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
78

32. Duvernoy HM . The human brainstem and cerebellum: surface, structure,vascularization and three dimensional sectional anatomy with MRI. New York, NY:Springer-Verlag, 1995.
33. Amarenco P, Kase CS, Rosengart A, Pessin MS, Bousser MG, Caplan LR . Very small(border zone) cerebellar infarcts: distribution, causes, mechanisms and clinical features.Brain 1993;116(Pt 1): 161–186.
34. Kruit MC, Launer LJ, Ferrari MD, van Buchem MA . Infarcts in the posteriorcirculation territory in migraine: the population-based MRI CAMERA study. Brain2005;128(Pt 9):2068–2077.
35. Derdeyn CP, Videen TO, Yundt KD, et al . Variability of cerebral blood volume andoxygen extraction: stages of cerebral haemodynamic impairment revisited. Brain2002;125(Pt 3):595–607.
36. Vagal AS, Leach JL, Fernandez-Ulloa M, Zuccarello M . The acetazolamide challenge:techniques and applications in the evaluation of chronic cerebral ischemia. AJNR Am JNeuroradiol 2009;30(5): 876–884.
37. Powers WJ, Press GA, Grubb RL Jr.., Gado M, Raichle ME . The effect ofhemodynamically significant carotid artery disease on the hemodynamic status of thecerebral circulation. Ann Intern Med 1987;106(1):27–34.
38. Powers WJ . Cerebral hemodynamics in ischemic cerebrovascular disease. Ann Neurol1991;29(3): 231–240.
39. Chaves CJ, Silver B, Schlaug G, Dashe J, Caplan LR, Warach S . Diffusion- andperfusion-weighted MRI patterns in borderzone infarcts. Stroke 2000; 31(5):1090–1096.
40. Ozgur HT, Kent Walsh T, Masaryk A, et al . Correlation of cerebrovascular reserve asmeasured by acetazolamide-challenged SPECT with angiographic flow patterns and intra-or extracranial arterial stenosis. AJNR Am J Neuroradiol 2001;22(5): 928–936.
41. Grubb RL Jr.., Derdeyn CP, Fritsch SM, et al . Importance of hemodynamic factors inthe prognosis of symptomatic carotid occlusion. JAMA 1998;280(12):1055–1060.
42. Yamauchi H, Fukuyama H, Nagahama Y, et al . Significance of increased oxygenextraction fraction in five-year prognosis of major cerebral arterial occlusive diseases. JNucl Med 1999;40(12):1992–1998.
43. Markus H . Transcranial Doppler detection of circulating cerebral emboli: a review.Stroke 1993;24(8): 1246–1250.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
79

44. Babikian VL, Hyde C, Pochay V, Winter MR . Clinical correlates of high-intensitytransient signals detected on transcranial Doppler sonography in patients withcerebrovascular disease. Stroke 1994;25(8):1570–1573.
45. Hendrikse J, Petersen ET, van Laar PJ, Golay X . Cerebral border zones between distalend branches of intracranial arteries: MR imaging. Radiology 2008;246(2):572–580.
46. Graham DI (1992) Hypoxia and vascular disorders. In: Adams JH, Corsellis JAN,Duchen LW (eds) Greenfield's neuropathology. 5 th edn. Arnold, London, pp 153-268
47. Bryan RN, Willcott MR, Schneiders NJ, Ford 11,Derman HS (1983) Nuclear magneticresonance evaluation of stroke. A preliminary report. Radiology 149: 189-192
48. Sipponen JT (1984) Visualization of brain infarction with nuclear magnetic resonanceimaging. Neuroradiology 26: 387-391
49. Brant-Zawadzki M, Weinstein P, Bartkowski H, Moseley M (1987) MR imaging andspectroscopy in clinical and experimental cerebral ischemia: a review. AJNR 8: 39-48
50. Nabatame H, Fujimoto N, Nakamura K et al. (1990) High intensity areas onnoncontrast T'l-weighted MR images in cerebral infarction. J Comput Assist Tomogr 14:521-526
51. Boyko DB, Burger PC, Shelburne JD, Ingram P (1992) Non-heme mechanisms for T1shortening: pathologic, CT, and MR elucidation. AJNR 13: 1439-1445
52. Hecht-Leavitt C, Gomori JM, Gross man RI et al. (1986) High-field MRI ofhemorrhagic cortical infarction. AJNR 7: 581-585
53. Hesselink JR, Healy ME, Dunn WM, Rothrock JF, McCreight PHB, Brahme F (1986)Magnetic resonance imaging of hemorrhagic cerebral infarction. Acta Radiol [Suppl] 369:46-48
54. Takahashi S, Higano S, Ishii K et al. (1993) Hypoxic brain damage: cortical laminarnecrosis and delayed changes in white matter at sequential MR imaging. Radiology 189:449-456
55. Sawada H, Udaka F, Seriu N, Shindou K, Kameyama M, Tsujimura M (1990) MRIdemonstration of cortical laminar necrosis and delayed white matter in jury in anoxicencephalopathy. Neuro radiology 32: 319-321
56. Donaire A, Carreno M, Gomez B, Fossas P, Bargallo N, Agudo R, et al. Corticallaminar necrosis related to prolonged focal status epilepticus. J Neurol NeurosurgPsychiatr 2006;77:104-6.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
80

57. Yoneda Y, Yamamoto S. Cerebral cortical laminar necrosis on diffusion-weighted MRIin hypoglycaemic encephalopathy. Diab Med 2005;22:1098-100.
58. McKinney AM, Teksam M, Felice R, Casey SO, Cranford R, Truwit CL, et al.Diffusion-weighted imaging in the setting of diffuse cortical laminar necrosis and hypoxic-ischemic encephalopathy. AJNR Am J Neuroradiol 2004;25:1659-65.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
81

INTRODUCTION
INTRODUCTION
Cortical laminar necrosis occurs as a consequence of oxygen or glucose depletion in thewatershed intracortical area in the third cortical layer, as in anoxia, hypoglycaemia, statusepilepticus, ischaemic stroke CNS vasculitis, neuro-lupus and drugs [1]. Corticalpseudolaminar necrosis, also known as cortical laminar necrosis and simply laminarnecrosis, is the (uncontrolled) death of cells in the (cerebral) cortex of the brain in a band-like pattern,[1] with a relative preservation of cells immediately adjacent to the meninges.Pathologically Cortical laminar necrosis represents cytotoxic oedema affecting a particularlayer of cerebral cortex (third grey matter layer) at the acute stage and isneuropathologically characterized by delayed selective neuronal necrosis at the acute stagefollowed by reactive change of glia and deposition of fat-laden macrophages. In particularthe characteristic high intensity on precontrast Tl-weighted images in Cortical laminar
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
82

necrosis, which generally begins to appear about 2 weeks after the ictus, becomesprominent at 1-2 months and began to fade at 3-11 months, is due to the deposition of fat-laden macrophages or methemoglobin representing intracortical microhemorrhages.
Chronic brain infarcts are typically seen as low-intensity lesions on T1-weighted and high-intensity lesions on T2- weighted images due to prolonged T1 and T2 values [3, 4]. In someinfarcts, high-intensity lesions are observed on precontrast T1-weighted images.Haemorrhagic infarcts show characteristic changes of the signal intensity, similar to thoseof haemorrhage, due to deoxyhaemoglobin, methohaemoglobin, and haemosiderin [7, 8].Petechial haemorrhage may occur in cortical infarcts (cortical laminar necrosis) but cannotexplain the high-intensity laminar lesions in all patients on precontrast TI images [9]. Ingeneral high intensity on precontrast Tl-weighted images (T1 shortening) can be due tomethaemoglobin, mucin, high protein concentration, lipid or cholesterol, calcification andcortical laminar necrosis [6]. In ischaemic stroke, high intensity laminar lesions can becortical laminar necrosis, haemorrhagic infarcts (microhaemorrhage), or a combination ofthe two.
The grey matter has six layers. The third is the most vulnerable to depletion of oxygen andglucose (watershed intracortical zone). When a relatively mild ischaemic or hypoglycaemicinsult occurs, the vulnerable layers are selectively injured (selective neuronal vulnerability)[1].
Because the third grey matter layer is the most vulnerable to anoxia and hypoglycemia,Cortical laminar necrosis is a specific type of cortical infarction, usually seen in the settingof anoxic encephalopathy. Other etiologies like hypoglycemia, status epilepticus andimmunosuppressive chemotherapy have been implicated.[11,12] The appearance of the MRimages in the setting of diffuse cortical laminar necrosis can be deceptive. Properlywindowed diffusion weighted imaging can be very helpful in detecting cortical laminarnecrosis, especially in the setting of anoxic-hypoxic encephalopathy in the early subacutephase.[13] Cortical laminar necrosis in the setting of anoxic encephalopathy has auniversally poor prognosis, with most patients either progressing to brain death orremaining in a persistent vegetative state.[12].
Boyko et al. [6] described cortical laminar necrosis in brain infarcts as linear high onprecontrast TI imags signal based on the cortical surface and becoming less intense overtime (months). In hypoxic brain damage, Precontrast Tl-weighted images revealed alaminar hyperintensity lesion in the cortex in the late subacute stage (21-28 days) whichtended to fade after 2 months but persisted up to 11 months [9]. In laminar corticalnecrosis, cortical high intensity on precontrast Tl-weighted images generally begins toappear about 2 weeks after the ictus, became prominent at 1-2 months and began to fade at3 months, although it could persist up to 11 months. FLAIR images are more sensitive thanTl weighted images to the cortical laminar lesions. Early cortical changes on day 1 showedhigh intensity on T2- weighted images and low intensity on Tl-weighted images, which laterbecame high intensity on precontrast T1 images. This early change is due to prolonged Tland T2 values caused by acute ischaemic change (tissue oedema).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
83

The cortical laminar necrosis, seen as a laminar high signal lesion on precontrast T1-weighted images, was first described by Sawada et al. [10] in a patient with anoxicencephalopathy. The cortical lesion is usually in the watershed region (watershedintracortical zone) in this condition [9]. Cortical laminar necrosis is also reported inischaemic stroke [5,6]. Although Nabatame et al. [5] thought the high intensity onprecontrast T1-weighted images was due to methohaemoglobin in haemorrhagic tissue,pathological studies revealed no haemorrhage [6, 11]. Takahashi et al. [9] reported apatient with a cortical laminar lesion showing low intensity on T2-weighted images in thechronic stage, which they thought due to haemosiderin.
Figure 1. Cortical laminar necrosis.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
84

Figure 2. Cortical laminar necrosis. Early inthe disease, gross findings will be characterizedby edema and swelling. Note the swollenglistening appearance of the cerebral cortex.Note the vague line between cortex andsubcortical white matter (arrows).Histologically this line would correspond to anearly (laminar) band of cortical necrosis.
Figure 3. A 60-year-old woman with an anti phospholipid antibody syndrome. All images 1month after ictus. a A Tl weighted image shows a high-intensity right occipital laminarlesion, with low intensity in white matter. b There is intense contrast enhancement of thegrey matter, none of the white matter. c A T2-weighted image demonstrates an isointenselaminar lesion, while the white matter shows very high intensity. d A proton-density imagedemonstrates the high-intensity laminar cortical lesion.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
85

Figure 4. A 73-year-old man with speech disturbance. a At 1.5 months afterthe ictus, a precontrast T1-weighted image demonstrates a high-intensity leftparietal laminar lesion (arrow). B, At 6 months, there is no high intensity andno contrast enhancement (C), but a FLAIR image (D) still shows a high-intensity laminar lesion.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
86

Figure 5. Precontrast T1 image showing cortical laminar necrosisdemonstrated as a laminar linear cortical hyperintensity.
In cortical laminar necrosis, CT does not demonstrate haemorrhage orcalcification, and MRI also fails to demonstrate haemorrhage. Although themechanism of Tl shortening (precontrast T1 hyperintensity) in the corticallaminar necrosis remains unclear, high cortical intensity on precontrast Tl-weighted image (generally begins to appear about 2 weeks after the ictus,becomes prominent at 1-2 months and began to fade at 3 months) is believed tooccur by neuronal damage and reactive tissue change, (reactive change of gliaand deposition of fat-laden macrophages) [9, 10] . On FLAIR images, corticallaminar necrosis is demonstrated as linear cortical hyperintensity due toincreased mobile protons in the reactive tissue. A less likely explanation is thatmicrohaemorrhage in the cortical laminar lesion can occur in some patients,which may contribute to Tl shortening.
On CT cortical laminar necrosis shows contrast enhancement due todisruption of the blood-brain barrier, where loss of neurons and vascularproliferation occur [11]. On MRI contrast enhancement occurs in the corticallesion with disruption of the blood-brain barrier. Parenchymal enhancementin brain infarcts is common and is generally maximal between 3 days and 3weeks; it disappears by 3 months [13-15]. The greater sensitivity of MRI tochanges in the blood-brain barrier results in prolonged detection of blood-
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
87

brain barrier disruption in the cortical lesion, at up to 8 months in our series.
Figure 6. MR (diffusion weighted imaging) showing gyriform increased signalsuggestive of cortical laminar necrosis
Epilepsy, metabolic disorders and Neuro-lupus
Transient radiological changes, such as hyperintense cortical lesions in T2,FLAIR, and diffusion weighted images, have been reported in patients withfocal Neuro-lupus.2,3,4. Radiologically, Cortical laminar necrosis ischaracterised by high intensity cortical lesions on T1 weighted and FLAIRimages following a gyral distribution, associated with volume loss over theunderlying cortex. Cortical laminar necrosis has been described associatedwith hypoxia, metabolic disturbances, drugs, infections, and Neuro-lupus.Cortical laminar necrosis associated with Neuro-lupus is mostly due to severehypoglycaemia or hypoxia or significant decreases in blood pressure duringthe episodes of focal Neuro-lupus. The hypothesis that the necrosis observed inthese patients is primarily a consequence of repeated seizures is furthersupported by the fact that Cortical laminar necrosis is seen in the same areasas those displaying acute cortical oedema and hyperperfusion during the acutephase of Neuro-lupus. Furthermore, these hyperintense lesions did not involveseparate vascular territories and occurred at a distance from the structurallesions. The location of Cortical laminar necrosis is also concordant with thelocation of continuous epileptic activity shown by surface EEG during Neuro-lupus.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
88

Hypoglycemia
First described in a patient with anoxic encephalopathy, it was found later thatlaminar cortical necrosis represented cytotoxic oedema affecting a particularlayer of cerebral cortex neuropathologically characterised by delayed selectiveneuronal necrosis and is a consequence of hypoxic-ischaemic encephalopathy,hypoglycaemic encephalopathy, status epilepticus and ischaemic stroke.Mechanisms of laminar cortical necrosis are not well elucidated.
Figure 7. Cortical laminar necrosis in a patient with hypoglycemia. (A)Diffusion- weighted MRI shows linear hyperintensities in a gyral pattern inright parietal and insular cortices (white arrow). (B) MRI Apparent diffusioncoefficient image showing hypo intensities in these areas suggestive ofrestriction of diffusion.(C) Susceptibility weighted image shows hyperintensities within the right parietal and insular cortices without bloomingartifacts.
Figure 8. Cortical laminar necrosis in a patient with hypoglycemia (A) MRIcoronal T2-weighted image of brain showing hyperintense signals from medialtemporal lobe (thick white arrow) of right side sparing cerebellar hemispheres.(B) MRI FLAIR images showing hyperintensities in the hippocampal regionand parahippocampal gyrus right more than the left. (C) MRI brain coronal
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
89

section T2-weighted images showing hyperintensities bilaterally in thehippocampal region.
References
1. Graham DI (1992) Hypoxia and vascular disorders. In: Adams JH, CorsellisJAN, Duchen LW (eds) Greenfield's neuropathology. 5 th edn. Arnold,London, pp 153-268
2. Bryan RN, Willcott MR, Schneiders NJ, Ford 11,Derman HS (1983) Nuclearmagnetic resonance evaluation of stroke. A preliminary report. Radiology 149:189-192
3. Sipponen JT (1984) Visualization of brain infarction with nuclear magneticresonance imaging. Neuroradiology 26: 387-391
4. Brant-Zawadzki M, Weinstein P, Bartkowski H, Moseley M (1987) MRimaging and spectroscopy in clinical and experimental cerebral ischemia: areview. AJNR 8: 39-48
5. Nabatame H, Fujimoto N, Nakamura K et al. (1990) High intensity areas onnoncontrast T'l-weighted MR images in cerebral infarction. J Comput AssistTomogr 14: 521-526
6. Boyko DB, Burger PC, Shelburne JD, Ingram P (1992) Non-hememechanisms for T1 shortening: pathologic, CT, and MR elucidation. AJNR13: 1439-1445
7. Hecht-Leavitt C, Gomori JM, Gross man RI et al. (1986) High-field MRI ofhemorrhagic cortical infarction. AJNR 7: 581-585
8. Hesselink JR, Healy ME, Dunn WM, Rothrock JF, McCreight PHB,Brahme F (1986) Magnetic resonance imaging of hemorrhagic cerebralinfarction. Acta Radiol [Suppl] 369: 46-48
9. Takahashi S, Higano S, Ishii K et al. (1993) Hypoxic brain damage: corticallaminar necrosis and delayed changes in white matter at sequential MRimaging. Radiology 189: 449-456
10. Sawada H, Udaka F, Seriu N, Shindou K, Kameyama M, Tsujimura M(1990) MRI demonstration of cortical laminar necrosis and delayed whitematter in jury in anoxic encephalopathy. Neuro radiology 32: 319-321
11. Donaire A, Carreno M, Gomez B, Fossas P, Bargallo N, Agudo R, et al.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
90

Cortical laminar necrosis related to prolonged focal status epilepticus. JNeurol Neurosurg Psychiatr 2006;77:104-6.
12. Yoneda Y, Yamamoto S. Cerebral cortical laminar necrosis on diffusion-weighted MRI in hypoglycaemic encephalopathy. Diab Med 2005;22:1098-100.
13. McKinney AM, Teksam M, Felice R, Casey SO, Cranford R, Truwit CL, etal. Diffusion-weighted imaging in the setting of diffuse cortical laminarnecrosis and hypoxic-ischemic encephalopathy. AJNR Am J Neuroradiol2004;25:1659-65.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
91

INDEX http://yassermetwally.com
INTRODUCTION& PATHOGENESIS PATHOGENESIS OF HYPERTENSIVE
CEREBRAL HEMORRHAGE PATHOLOGY CT SCAN IMAGING OF CEREBRAL
HEMORRHAGE MR IMAGING OF CEREBRAL
HEMORRHAGE CEREBRAL EDEMA ASSOCIATED WITH
NONTRAUMATIC CEREBRALHEMORRHAGE
REFERENCES
RADIOLOGICAL PATHOLOGY OF MICROVASCULAR CEREBRALHAEMORRHAGE:
Haemorrhagic microvascular brain disease constitutes the other facet of the bad coin (themicrovascular brain disease) the first facet of which is the ischemic microvascular braindisease. Both the haemorrhagic and the ischaemic microvascular brain disease sharecommon haemorheological, metabolic endocrinal abnormalities (The metabolic syndrome)and cardiac changes(LVH).
In microvascular brain disease, the small penetrating arterioles of the subependymal andthe pial microvascular systems tend to become stenosed and undergo lipohyalinosis or theymay dilate to form microaneurysms. From the pathological point of view both
92

Lipohyalinosis and microaneurysms, almost invariably, coexist in the same individual, thusmaking the patient Liable to develop either the ischaemic or the haemorrhagicmicrovascular brain.
Figure 1.Microaneurysms of the smallpenetratingarterioles
Microaneurysmal formation occurs predominantly in the territory of the subependymalmicrovascular system,thus making the incidence of the haemorrhagic microvascular eventsmuch more frequent in the periventricular gray matter (thalamus, basal ganglia and theinternal capsule) or the immediate periventricular white matter. The coexistence oflipohyalinosis and microaneurysms in the periventricular regions will explain thepropensity of the diseased microvascular system either to thrombose (resulting in lacunarinfarctions) or to rupture and leak resulting in periventricular haematoma formation.Lacunar infarctions and hypertensive cerebral haemorrhages are two facets of one and thesame bad coin (the microvascular brain disease).
93

Figure 2. Microaneurysms are predominately distributed in the immediate periventricular region
Microaneurysmal formation should weaken the arteriolar wall so that rupture and leakagecan occur even in normotensive states. When microaneurysmal rupture occurs, thebleeding will result in haematoma formation. The bleeding will then be arrested byocclusive thrombosis of the bleeding microaneurysms. Following microaneurysmal ruptureand bleeding, the size of the resulting haematoma will be determined by the bleeding time.The bleeding time is a function of the whole blood viscosity in general and the plateletaggregability in particular.
Should microaneurysmal bleeding occurs during periods of higher blood viscosity, thebleeding time will be shorter and subsequently the size of the resulting haematoma will besmaller. In fact during high blood viscosity the bleeding is not infrequently arrested beforeforming haemorrhages adequate to give rise to immediate clinical sequelae. Patients withhigher blood viscosity and thrombotic tendency, although less likely to develop serioushaemorrhagic microvascular events, they are particularly liable to develop seriousischaemic microvascular events.
During periods of lower blood viscosity and thrombotic tendency of the blood,microaneurysmal bleeding might result in huge haematoma formation that may split alongthe planes of the white matter forming a substantial space occupying clot, or may ruptureinto the ventricular system resulting in massive ventricular haemorrhage. In generalinverse correlation is present between the haematoma size and the current blood viscosityat the time of microaneurysmal bleeding.
94

Patients with microvascular brain disease might have recurrent events which could bepurely haemorrhagic or purely ischaemic, however, it is not uncommon for some patientsto fluctuate between the haemorrhagic and the ischaemic events, developing haemorrhagicevents at certain times and ischaemic events at other times. In general ischaemicmicrovascular events are much more common and much more frequent than thehaemorrhagic events.
PATHOGENESIS OF HYPERTENSIVE CEREBRAL HEMORRHAGE
Hypertension causes fibrinoid necrosis of these penetrating arterioles. The massiveintracerebral hemorrhage which is a complication of hypertension, arises from rupture of anecrotic arteriole or from rupture of a minute "miliary" aneurysm formed at the site ofnecrosis. These aneurysms were first described by CHARCOT and BOUCHARD. Thefrequency of fibrinoid necrosis and miliary aneurysm formation in vessels within basalganglia and thalamus accounts for the frequency of intracerebral hemorrhage in thoselocations. Fibrinoid is identified by its structureless or sometimes granular red appearanceon H&E stain and by the fact that , unlike hyalinized smooth muscle which is alsoeosinophilic, the fibrinoid areas stain with stains for fibrin such as PTAH or Putz stain orwith certain trichrome stains. The fibrinoid change in these vessels was calledlipohyalinosis by Miller-Fisher in a very influential series of articles. However that term isconfusing because hyalinized arteries are arteries whose media has undergone a pathologicchange which is not fibrinoid necrosis and which by itself does not lead to rupture. Indeedhyalinized arterioles are common in hypertension. The term lipohyalinosis stresses thepresence of fat in the degenerate arteriolar wall but again this change is not the hallmark ofthe arterioles that are in danger of rupturing or forming miliary aneurysms. The fibrinoidchange is the critical change in these diseased arteriolar segments looks and stains just likethe fibrinoid seen in renal and other arterioles in malignant hypertension. The importantpoint to remember is that, for unknown reasons, the brain arterioles can undergo fibrinoidnecrosis even in so-called benign hypertension--that is in patents with only modest bloodpressure elevation. For that reason it is important to treat even benign hypertension. Theseries figures below illustrates the pathologic processes that can lead to rupture.
95

Figure 3. A, The figure shows the wall of an arteriole stained with H&E. The amorphouspink [eosinophilic] material in the wall could be either fibrinoid or amyloid. To prove thatit is firbrinpoid the section or its close neighbor should be stained with any one of severaltechniques that stain fibrin [e.g. Putz stain-blue; or the PTAH stain-blue; or a trichromestain such as the azo carmine stain; the azo carmine is particularly good because itdistinguishes fibrinoid from garden variety hyalinization by staining fibrin/fibrinoid redwhile staining collagen or hyalinized collagen blue.]. B, This section was stained withazocarmine. An arteriole in the subarachnoid space has an amorphous red materialoccupying a good portion of its wall. This is fibrinoid. Fibrinoid is frequently segmental indistribution so that the entire circumference may not be involved and other areas along thelength of the vessel may also be spared. C, This figure was also stained with azocarmine.The arteriole wall is replaced by red fibrinoid and displays aneurysmal dilation.
96

Figure 4. A,B Sometimes a miliary aneurysm thrombosis rather than ruptures. It thenappears as a fibrous ball which may be separated from the parent vessel due to the plane atwhich the section has been cut. If the section is close to the parent arteriole there will beelastic tissue at the margin of the ball. This elastic tissue stains black with the VVG stain in(B)
Figure 5. The pathologist gotlucky when this section wastaken. Here a miliary aneurysmthat has neen converted to afibrous ball or globe, shown inthis longitudinal section, stillconnected to the parentarteriole by a thin neck.
PATHOLOGY
Cerebral Haematomas occur much more frequently at the putameno-capsular and thethalamic regions and may rupture into the ventricular system. Less common sites includethe cortical and the immediate subcortical white matter, especially in the parietal region,the pons and the cerebellum.
The resulting haematoma is dark red in colour due to the existence of deoxyhaemoglobininside the intact RBCS. During the subacute stage (3 days - one month) the dark red colour
97

of the haematoma is replaced by a brownish discoloration, which starts at the periphery ofthe haematoma and then extends to its center. This brownish discoloration occurs due tothe replacement of deoxyhaemoglobin by the oxidized methemoglobin.
Acute hematoma usually spreads between white matter tracts resulting in island of viablebrain tissues within the hematoma itself. Bleeding usually stops shortly after the initialictus, however in a substantial minority of patients the hematoma continues to expandusually within the first hour after the presentation. Expansion after one hour is unusual.Once hematoma forms, vasogenic edema forms around the clot as osmotically active serumproteins are released from the hematoma. Edema peaks at about 48 hours and usuallybegins to resolve after 5 days. Whether the brain tissues surrounding the acute hematomais ischemic -due to vascular compression- or not is controversial. Functional suppression(diaschisis) of brain activity rather than ischemia is more probable.
Risk of Hematoma Enlargement
In nearly one quarter of initially alert patients presenting with spontaneous intracerebralhemorrhage, secondary deterioration in level of consciousness occurs within the first 24hours after onset. Hematoma expansion and edema formation are believed to be the majorfactors involved In several large prospective and retrospective studies, investigators haveevaluated the rate of hematoma enlargement after initial presentation and report ratesranging from 14 to 38% within the first 24 hours of admission.[27,28]
In their review of 627 patients with spontaneous intracerebral hemorrhage Fujii, et al..[27]reported that CT scanning within 24 hours of admission demonstrated enlargement of thehematoma in 14% of patients. Five factors were found to be associated with enlargement:admission shortly after onset of symptoms, heavy alcohol consumption, irregularly shapedhematoma, reduced level of consciousness, and low level of fibrinogen.
98

Figure 6. Cerebral (A) and pontine (B) acute haemorrhage, C, acute cerebellar hemorrhage
Gradually the haematoma is surrounded by reactive gliosis and macrophages laden withhaemosiderin granules (Ferric hydroxide). The clot is gradually absorbed starting with itsperiphery and is replaced by a yellow fluid, this is called an apoplectic cyst. Reactive gliosisprogressively increases and ultimately transforms the haematoma into a slit-like scar.
Figure 7. A, acute putameno-capsular & intraventricular hemorrhage, B, apoplectic cyst
Figure 8. A, Subacute caudate hemorrhage, B, apoplectic cyst, C, Hypertensivehemorrhage into basal ganglia region (specifically: internal capsule).
Pathologically the brains of patients with cerebral haemorrhages very frequently showevidence of past microvascular ischaemic events such as lacunar infarctions,leukoaraiosis,etc.
INCIDENCE OF COMMON ANATOMICAL SITES IN HYPERTENSIVEINTRACEREBRAL HAEMORRHAGE
99

Figure 9. Incidence (in % ) of the common anatomical sites in hypertensive intracerebralhaemorrhage
STRUCTURAL NEUROIMAGING OF MICROVASCULAR CEREBRALHAEMORRHAGE
CT imaging of haematoma.
A cerebral haematoma, in the acute stage, has higher attenuation values on precontrastscan (hyperdense). The higher attenuation values of fresh blood is due to the existence ofpacked haemoglobin in the haematoma. In particular the globin component of thehaemoglobin is responsible for the increased CT density on precontrast scan. Withprogressive absorption of haemoglobin, (this usually starts from the periphery of thehaematoma) the attenuation value of the haematoma gradually decreases until the highdensity haematoma is replaced by a low density space occupying cyst.
Figure 10. A, Acute haematoma, B, an apoplectic cyst and C, an old haematoma (slit-likescar)
100

The evolution of the haematoma from a high density clot to a low density cyst usually takesa period that ranges between one month to three months. The walls of this cyst mightenhance and the haematoma at this stage might be mixed with abscess or glioma. History isof paramount significance at this stage. Very old haematoma appears by CT scan as a slit-like hypodense area with negative mass effect.
In general Haematomas are space-occupying with positive mass effect and are commonlysurrounded by a hypodense oedema area. The most common sites are the putameno-capsular and the thalamic sites and either of them might rupture intraventricularly. Lesscommon sites includes the parietal lobe, pons and cerebellum.
The diagnosis of acute ICH is virtually 100% reliable with non-contrast CT due to thecharacteristic mass of blood of high attenuation value, due to the presence of the globincomponent of the haemoglobin molecule. Under exceptional circumstances, patients withprofound anaemia, with a haematocrit of 20% or less have presented with an acutehaematoma which was isointense to brain on account of the low haemoglobin contents ofthe fresh haematoma. Fresh blood has an attenuation value of 55-85 Hounsfield units, thehigh attenuation (50-70 Hounsfield units) is from high protein concentration within intactred blood cells and not iron content 1.
As the fresh clot starts to retract after 24-48 hours from onset, there is serum extrusionaround its periphery, resulting in a ring of hypointensity that surrounds the haematoma .In the subacute stage, the haematoma maintains its mass effect but becomes progressivelyless dense, from the periphery toward the center, until reaching isointensity with theadjacent brain parenchyma. The infusion of intravenous contrast at this stage candemonstrate an area of ring enhancement at the periphery of the haematoma. In thechronic stage, the mass effect of the haematoma is no longer present, post-contrastenhancement has disappeared after about 6 weeks from onset , and the residual is ahypointense cavity, at times in the form of a slit that can be indistinguishable from an areaof old cavitated infarction.
o More detailed description of the CT scan appearance of brain hemorrhage
The CT appearance of hemorrhage is determined by the degree of attenuation of the x-raybeam, which is proportional to the density of hemoglobin protein (relative to plasmaconcentration) within the hematoma.
Immediately following vessel rupture, the hematoma consists of a collection of red bloodcells, white blood cells, platelet clumps, and protein-rich serum that has a heterogeneousappearance on CT with attenuation in the range of 30–60 Hounsfield units (HU),depending on the degree of plasma extrusion [20]. In this hyperacute phase, hemorrhagemay be difficult to distinguish from normal cortex because of similar attenuation. Overminutes to hours, a fibrin clot forms with an increase in attenuation to 60–80 HU (Fig. 11)[20]. Clot retraction and extrusion of serum can further increase attenuation to as high as80–100 HU in the center of the hematoma. The degree of attenuation may be reduced inpatients with severe anemia [21], impaired clot formation due to coagulopathy, or volume
101

averaging with adjacent tissue. Vasogenic edema evolves around the hematoma withinhours and may continue to increase for up to 2 weeks after hemorrhage onset [22].
Figure 11. CT appearance of hemorrhage.Serial CT scans of right thalamic hematoma.(A) Acute ICH in the right thalamus withmean attenuation 65 HU. (B) CT performed 8days later than (A); the periphery of thehematoma is now isodense to the brain whilethe center of the hematoma has meanattenuation 45 HU. (C) CT performed 13 dayslater than (A) shows continued evolution ofthe hematoma with decreasing attenuation.(D) CT performed 5 months later than (A)shows a small area of encephalomalacia in thelocation of the previous hemorrhage.
Over the following days, cells and protein are broken down and scavenged bymacrophages, leading to slowly decreasing attenuation, with the greatest decrease at theperiphery of the hematoma and more gradual evolution toward the center (Fig. 11) [23].Within 4 to 9 days, the hematoma attenuation decreases to that of normal cortex, andwithin 2 to 3 weeks to that of normal white matter [20].
The CT recognition of subacute intracerebral hematoma can be challenging because theattenuation is similar to that of normal brain tissue, although mass effect may still bepresent. MR imaging can confirm subacute hematoma. As time goes on, attenuationcontinues to decrease to levels below that of the normal brain. Eventually, the hematomaresolves into a fluid-filled or slit-like cavity that may be difficult to visualize on CT (Fig.11). Contrast enhancement is not present in the initial days following ICH but may developat the periphery in weeks to months [24], sometimes leading to diagnostic confusion withbrain tumor or abscess.
A blood-fluid level may be seen in medium to large ICH within the first hours after onset;the dependent portion displays higher attenuation (Fig. 12) due to sedimentation of cellularelements [25]. This finding may be more common in ICH caused by anticoagulation [26],but it is not specific and has also been described in ICH due to hypertension, trauma,tumor, or arterial-venous malformation. The association with shorter time interval fromICH onset, and in some cases with anticoagulation, has led to speculation that incompleteclotting is required for blood-fluid level formation.
102

Figure 12. CT with blood-fluid level. A 77-year-old woman wasadmitted with coma of 4 hours' duration. CT scan showsmassive left hemispheric hematoma with blood-fluid level. Nohistory of anticoagulation or coagulopathy.
Box 1. As the hemorrhage evolves, different characteristic appearances can be identified onCT, depending on the age of the bleed. CT findings over time are as follows:
After 7-10 days, the high density of blood begins to decrease, starting from theperiphery of the lesion.
From 1-6 weeks, peripheral enhancement can be seen, mimicking the appearanceof an abscess, possibly related to hypervascularity at the periphery of a resolvinghematoma or disruption of the blood-brain barrier.
By 2-4 months, decreased density indicates cavity formation. A residual cavity isthe final stage, which is reached after complete absorption of necrotic andhemorrhagic tissue.
MRI Imaging of cerebral haematoma
Imaging of haematoma by MRI is time dependent as follow:
o The hyperacute stage (0 - 12 hour)
The acute hematoma less than 12 hours old is composed mostly of intracellularoxyhemoglobin with the edematous brain undergoing necrosis. 1 On T2-weighted MRimages, hyperacute hematoma will exhibit inhomogeneous signal due to hypointensedeoxyhemoglobin and hyperintense, edematous cortical tissue. MR is less sensitive than CTin the hyperacute stage because diamagnetic intra- cellular oxyhemoglobin lacks unpairedelectrons and thus clot signal is close to normal brain parenchyma- normal to slightly lowersignal on TI-weighted images and slightly higher signal on T2-weighted images 2,3. Repeatimaging is indicated to monitor the size of the hemorrhage and the development of delayedhemorrhage and vasogenic edema.
o The acute stage (12 Hr - 3 days)
103

Due to the presence of the magnetically susceptible deoxyhaemoglobin. The T2 relaxationtime will be markedly shortened, so that fresh blood appears hypointense (black) on the T2weighted MRI images. This hypointensity is commonly surrounded by a widerhyperintense area that represents oedema. On the T1 weighted images fresh blood appearsisointense or slightly hyperintense.
Acute hematoma one to three days old are composed mostly of paramagnetic intracellulardeoxyhemoglobin. The deoxyhemoglobin is formed by the dissociation of oxygen fromhemoglobin, a process that begins within several hours. Because the deoxyhemoglobinwithin intact, clotted hypoxic red blood cells does not cause T1 shortening, the hematomawill have normal to slightly lower signal on TI-weighted MR images. The concentration ofred blood cells with clot and the concentration of fibrin cause T2 shortening, with areas ofvery low signal on T2-weighted spin echo and T2 * -weighted gradient echo images 3.
Figure 13. A 62-year-old female withhypertension presented with acute-onset ataxia and confusion.Noncontrast CT exam of the head [leftimage] showed a large, right cerebellarhemorrhage, which was evacuated torelieve the mass effect on the brainstemand fourth ventricle. The cerebellarhemorrhage is seen hypointense on theT2 image due to Deoxyhemoglobin[right image].
Figure 14. The concentration of red blood cells withclot and the concentration of fibrin cause T2shortening, with areas of very low signal on T2-weighted spin echo and T2 * -weighted gradient echoimages
o The subacute stage (3 days - one month)
The picture of hematoma is determined by the oxidation of deoxyhemoglobin tomethemoglobin and its shift from the intracellular to the extracellular compartment. Thepicture of haematoma, during this period is governed by the progressive reduction in theconcentration of deoxyhaemoglobin and the progressive increase in the concentration ofthe oxidized methemoglobin. These changes take place from the periphery of thehaematoma to its center. Intracellular oxidized methemoglobin induces shorting of T2
104

relaxation time while extracellular oxidized methemoglobin induces prolongation of T2relaxation time
Progressive reduction in the concentration of deoxyhaemoglobin and shift of oxidizedmethemoglobin from the intracellular to the extracellular compartment, due to lyse ofRBCs, results in progressive disappearance of the T2 hypointensity observed in the acutestage. Absence of the deoxyhaemoglobin and appearance extracellular oxidizedmethemoglobin will result in progressive prolongation of the T2 relaxation time that startsfrom the periphery of the haematoma to its center, this results in progressive increase ofthe T2 signal intensity (it becomes brighter); At first the periphery of the haematomabecomes brighter on the T2 weighted images, and this brightness progressively extends tothe center.
Within a few days, the subacute hematoma start to undergo liquefaction with developmentof vasogenic edema. As the edema increases over the first week, it may be great enough tocause herniation. The edema has fluid or water characteristics: iso- to hypointense on TI-weighted images, and hyperintense on T2-weighted images. With oxidation ofdeoxyhemoglobin to strongly paramagnetic intracellular methemoglobin, proton-electrondipole-dipole interactions between hydrogen atoms and the paramagnetic centers ofmethemoglobin will cause marked TI shortening and very high signal intensity on TI-weighted images 4 within the periphery of the hematoma. The intracellular methemoglobinwill cause T2 shortening and very low signal on T2-weighted images.
After erythrocyte membrane breakdown and extracellular migration of methemoglobin,there is neovascularization with removal of blood components and debris by macrophages.The new blood vessels at the periphery of the lesion lack the tight endothelial junctions ofan intact blood brain barrier, and so there is intense enhancement of the margins on bothcontrast CT and MR 1. The fragile granulation tissue vessels predispose the patient toadditional episodes of acute hemorrhage. CT will show a decrease in the density of thehemorrhage and decrease in the mass effect, the latter due to a decrease in edema. MR willexhibit the persistent high signal of extracellular methemoglobin on TI - and T2-weightedimages 4 for up to a year. The peripheral rim of hemosiderin and ferritin has slightly lowsignal on Tl- and marked low signal on T2-weighted images [201 from the susceptibilityeffect of hemosiderin within macrophage lysosomes.
105

Figure 15. MRI T2 image (A) and proton density image (B) showing a subacutehaematoma, notice the peripheral hypointense hemosiderin ring
Because the extracellular oxidized methemoglobin has a paramagnetic quality it results inshortening of the T1 relaxation time, so that the haematoma in the subacute stage appearshyperintense (bright) on the T1 weighted MRI images. This again starts from the peripheryof the haematoma and progresses to its center, because as mentioned beforemethemoglobin starts to appear at the periphery of the haematoma, this results initially inring hyperintensity on the T1 images.
Figure 16. Early subacute hemorrhagic contusion in a 78-year- old male. Sagittal TI-weighted image demonstrates high signal intensity at the periphery of the hematoma,consistent with extracellular methemoglobin.
The haemosiderin pigmentation that surrounds thehaematoma in the subacute and chronic stages isresponsible for the rim of hypointensity that surrounds thehaematoma on the T2 weighted and proton density images.
Figure 17. The hypointense hemosiderin ring of subacutehaematoma
o Chronic stage (one month to 3 months)
Due to complete absorption of the deoxyhaemoglobin and diffuse and homogeneousincrease of the oxidized methemoglobin within the haematoma; it appears diffuselyhyperintense (bright) on both the T1 and T2 weighted images.
106

Clot resorption begins from the periphery inward, and depending on the size of thehematoma, may vary from one to six weeks in duration. Necrotic tissue is sloughed andcystic cavities are formed over the next 6 to 12 months. Focal atrophy is characterized by adecrease in the size of cortical gyri, with compensatory enlargement of cerebrospinal fluidspaces and dilatation of the adjacent ventricle. Cystic cavities are surrounded by gliosis andhemosiderin scarring.
The hematomabiochemicalstages
Table 1. The MRI biochemical stages of cerebral hematomas
Biochemical substance MRI changesOxyhemoglobin Oxyhemoglobin lacks unpaired electrons and thus clot signal
is close to normal brain parenchyma- normal to slightlylower signal on TI-weighted images and slightly higher signalon T2-weighted images
Paramagnetic intracellulardeoxyhemoglobin.
Because the deoxyhemoglobin within intact, clotted hypoxicred blood cells does not cause T1 shortening, the hematomawill have normal to slightly lower signal on TI-weighted MRimages. The concentration of red blood cells with clot and theconcentration of fibrin cause T2 shortening, with areas ofvery low signal on T2-weighted spin echo and T2 * -weightedgradient echo images
Paramagnetic intracellularmethemoglobin.
Proton-electron dipole-dipole interactions between hydrogenatoms and the paramagnetic centers of methemoglobin willcause marked TI shortening and very high signal intensity onTI-weighted images within the periphery of the hematoma.
107

The intracellular methemoglobin will cause T2 shorteningand very low signal on T2-weighted images.
Extracellular migration ofmethemoglobin.
MR will exhibit the persistent high signal of extracellularmethemoglobin on TI - and T2-weighted images for up to ayear. The peripheral rim of hemosiderin and ferritin hasslightly low signal on Tl- and marked low signal on T2-weighted images [20] from the susceptibility effect ofhemosiderin within macrophage lysosomes.
Clot resorption begins fromthe periphery inward, anddepending on the size of thehematoma, may vary fromone to six weeks in duration.Necrotic tissue is sloughedand cystic cavities areformed over the next 6 to 12months.
Focal atrophy is characterized by a decrease in the size ofcortical gyri, with compensatory enlargement ofcerebrospinal fluid spaces and dilatation of the adjacentventricle. Cystic cavities are surrounded by gliosis andhemosiderin scarring.
SUMMARY
Table 2. The biochemical stages of cerebral hematomas
Hyperacute stage[0-12 Hr]
Immediately after an intracerebral bleed, the liquefied mass in thebrain substance contains oxyhemoglobin but no paramagneticsubstances. Therefore, it looks like any other proteinaceous fluidcollection.
Acute stage [4Hr -3days]
Reduction in oxygen tension in the hematoma results in the formationof intracellular deoxyhemolobin and methemoglobin in intact redcells. These substances have a paramagnetic effect that produces T2shortening. A thin rim of increased signal surrounding the hematomaon T2-weighted images represents edema.
Subacute stage[3days-3 weeks]
As red blood cells lyse, redistribution of methemoglobin into theextracellular space changes the effect of this paramagnetic substanceto one of predominantly T1 shortening. The longer T2 results from(1)a combination of red blood cell lysis (T2 shortening disappears), (2)osmotic effects that draw fluid into the hematoma, and (3) therepetition times (TR) that are in general use for T2-weightedsequences, which are not sufficiently long to eliminate T1 contrasteffects in the image.
Chronic stage[3weeks-3 months]
Phagocytic cells invade the hematoma (starting at the outer rim andworking inward), metabolizing the hemoglobin breakdown productsand storing the iron as superparamagnetic hemosiderin and ferritin.
108

Table 3. Effect of blood products on the MRI signal
Hyperacute stage [0-12 Hr] Oxyhemoglobin
T1 T2lacks unpaired electrons and thus clot signalis close to normal brain parenchyma- normalto slightly lower signal on TI-weightedimages and slightly higher signal on T2-weighted images
Acute stage [4Hr -3days]
Deoxyhemoglobinwithin intact, clottedhypoxic red blood
No effect
T2 shortening, withareas of very lowsignal on T2-weightedspin echo and T2 * -weighted gradientecho images
Early subacute stage[3days-3 weeks]
Stronglyparamagneticintracellularmethemoglobin,
TI shortening andvery high signalintensity on TI-weighted imageswithin the peripheryof the hematoma
The intracellularmethemoglobin willcause T2 shorteningand very low signalon T2-weightedimages
Late subacute stage[3days-3 weeks]
extracellularmigration ofethemoglobin
MR will exhibit the persistent high signal ofextracellular methemoglobin on TI - and T2-weighted images for up to a year
Chronic stage[3weeks-3 months]
Focal atrophy is characterized by a decrease in the size of corticalgyri, with compensatory enlargement of cerebrospinal fluid spacesand dilatation of the adjacent ventricle. Cystic cavities aresurrounded by gliosis and hemosiderin scarring.
Table 4. Effect of blood products on the MRI signal
Phase Time Hemoglobin T1 T2
Hyperacute <24 hours Oxyhemoglobin(intracellular)
Iso or hypo Hyper
Acute 1-3 days Deoxyhemoglobin(intracellular)
Iso or hypo Hypo
Early subacute >3 days Methemoglobin(intracellular)
Hyper Hypo
Late subacute >7 days Methemoglobin(extracellular)
Hyper Hyper
109

Chronic >14 days Hemosiderin(extracellular)
Iso or hypo Hypo
CEREBRAL EDEMA ASSOCIATED WITH NONTRAUMATIC CEREBRALHEMORRHAGE
Traditionally, ICH was believed to cause permanent brain injury directly by mass effect.However, the importance of hematoma-induced inflammatory response and edema ascontributors to secondary neuronal damage has since been recognized. 28,29,30
At least three stages of edema development occur after ICH (Table 5). In the first stage, thehemorrhage dissects along the white matter tissue planes, infiltrating areas of intact brain.Within several hours, edema forms after clot retraction by consequent extrusion ofosmotically active plasma proteins into the underlying white matter 28,29. The second stageoccurs during the first 2 days and is characterized by a robust inflammatory response. Inthis stage, ongoing thrombin production activates by the coagulation cascade, complementsystem, and microglia. This attracts polymorphonuclear leukocytes andmonocyte/macrophage cells, leading to up-regulation of numerous immunomediators thatdisrupt the blood-brain barrier and worsen the edema. 28,29,30 A delayed third stage occurssubsequently, when red blood cell lysis leads to hemoglobin-induced neuronal toxicity.28,29,30 Perihematomal edema volume increases by approximately 75% during the first 24hours after spontaneous ICH and has been implicated in the delayed mass effect thatoccurs in the second and third weeks after ICH. 28,29,30
Thrombin is an essential component of the coagulation cascade, which is activated in ICH.In low concentrations thrombin is necessary to achieve hemostasis. However, in highconcentrations, thrombin induces apoptosis and early cytotoxic edema by a direct effect.Furthermore, it can activate the complement cascade and matrix metalloproteinases(MMP) which increase the permeability of the blood brain barrier. 28,29,30
Delayed brain edema has been attributed, at least in part, to iron and hemoglobindegradation. Hemoglobin is metabolized into iron, carbon monoxide, and biliverdin byheme oxygenase. Studies in animal models show that heme oxygenase inhibition attenuatesperihematomal edema and reduces neuronal loss. 28,29,30 Furthermore, intracerebralinfusion of iron causes brain edema and aggravates thrombin-induced brain edema. Inaddition, iron induces lipid peroxidation generating reactive oxygen species (ROS), anddeferoxamine, an iron chelator, has been shown to reduce edema after experimental ICH.28,29,30
110

Table 5. Stages of edema after ICH
First stage (hours) Second stage (within first 2 days) Third stage (after first 2days)
Clot retraction andextrusion ofosmotically activeproteins
Activation of thecoagulation cascade andthrombin synthesis
Complement activation Perihematomal
inflammation and leukocyteinfiltration
Hemoglobin inducedneuronal toxicity
References
1. New PF, Aronow S. Attenuation measurements of whole blood and blood fractions incomputed tomography. Radiology 1976;121:635-40.
2. Atlas SW, Thulbom KR. MR detection of hyperacute parenchymal hemorrhage of thebrain. Am J Neuroradiol 1998;19:1471-507.
3. Gomori JM, Grossman RI, Goldberg HI, et al. Intracranial hematomas: imaging byhigh-field MR. Radiology 1985;157:87-93.
4. Wilberger JE, Rothfus WE, Tabas J, et al. Acute tissue tear hemorrhages of the brain:computed tomography and clinicopathological correlations. Neurosurgery 1990;27:208-13.
5. Barnett HJM, Yatsu FM, Mohr JP, Stein BM, eds.: Stroke: Pathophysiology, Diagnosis,and Management. 3rd ed. Churchill Livingstone; 1998.
6. Bradley WG Jr: MR appearance of hemorrhage in the brain. Radiology 1993 Oct;189(1): 15-26.
7. Broderick JP, Brott T, Tomsick T: Intracerebral hemorrhage more than twice ascommon as subarachnoid hemorrhage. J Neurosurg 1993 Feb; 78(2): 188-91.
8. roderick JP, Brott TG, Duldner JE: Volume of intracerebral hemorrhage. A powerfuland easy-to-use predictor of 30-day mortality. Stroke 1993 Jul; 24(7): 987-93.
9. Challa VR, Moody DM, Bell MA: The Charcot-Bouchard aneurysm controversy: impactof a new histologic technique. J Neuropathol Exp Neurol 1992 May; 51(3): 264-71.
10. Chan S, Kartha K, Yoon SS: Multifocal hypointense cerebral lesions on gradient-echoMR are associated with chronic hypertension. AJNR Am J Neuroradiol 1996 Nov-Dec;17(10): 1821-7.
111

11. Fazekas F, Kleinert R, Roob G: Histopathologic analysis of foci of signal loss ongradient-echo T2*- weighted MR images in patients with spontaneous intracerebralhemorrhage: evidence of microangiopathy-related microbleeds. AJNR Am J Neuroradiol1999 Apr; 20(4): 637-42.
12. Gokaslan ZL, Narayan RK: Intracranial Hemorrhage in the Hypertensive Patient.Neuroimaging Clinics of North America 1992; 2: 171-86.
13. Gomori JM, Grossman RI: Mechanisms responsible for the MR appearance andevolution of intracranial hemorrhage. Radiographics 1988 May; 8(3): 427-40.
14. Nelson JS, Parisi JE, Schochet SS Jr: Principles and Practise of Neuropathology.Mosby - Year Book, Inc. St. Louis, MO; 1993.
15. Robertson CS, Contant CF, Gokaslan ZL: Cerebral blood flow, arteriovenous oxygendifference, and outcome in head injured patients. J Neurol Neurosurg Psychiatry 1992 Jul;55(7): 594-603.
16. Ruscalleda J, Peiro A: Prognostic factors in intraparenchymatous hematoma withventricular hemorrhage. Neuroradiology 1986; 28(1): 34-7.
17. Spangler KM, Challa VR, Moody DM: Arteriolar tortuosity of the white matter inaging and hypertension. A microradiographic study. J Neuropathol Exp Neurol 1994 Jan;53(1): 22-6.
18. Taveras JM, Pile-Spellman J: Neuroradiology. 3rd ed. Williams & Wilkins; 1996.
19. Welch KMA, Caplan LR, Reis DJ, Weir B, Siesjo BK, eds.: Primer on CerebrovascularDiseases. Morgan Kaufmann; 1997.
20. Bergstrom M, Ericson K, Levander B, et al.. Variation with time of the attenuationvalues of intracranial hematomas. J Comput Assist Tomogr. 1977;1(1):57–63.
21. Kasdon DL, Scott RM, Adelman LS, et al.. Cerebellar hemorrhage with decreasedabsorption values on computed tomography: a case report. Neuroradiology.1977;13(5):265–266.
22. Inaji M, Tomita H, Tone O, et al.. Chronological changes of perihematomal edema ofhuman intracerebral hematoma. Acta Neurochir Suppl. 2003;86:445–448.
23.Messina AV. Computed tomography: contrast enhancement in resolving intracerebralhemorrhage. AJR Am J Roentgenol. 1976;127(6):1050–1052.
24. Ichikawa K, Yanagihara C. Sedimentation level in acute intracerebral hematoma in apatient receiving anticoagulation therapy: an autopsy study. Neuroradiology.1998;40(6):380–382.
112

25. Pfleger MJ, Hardee EP, Contant CF, et al.. Sensitivity and specificity of fluid-bloodlevels for coagulopathy in acute intracerebral hematomas. AJNR Am J Neuroradiol.1994;15(2):217–223.
26. Dolinskas CA, Bilaniuk LT, Zimmerman RA, et al.. Computed tomography ofintracerebral hematomas. I. Transmission CT observations on hematoma resolution. AJRAm J Roentgenol. 1977;129(4):681–688.
27. Fujii Y, Takeuchi S, Sasaki O, et al: Multivariate analysis of predictors of hematomaenlargement in spontaneous intracerebral hemorrhage. Stroke 29:1160–1166, 1998
27. Kazui S, Naritomi H, Yamamoto H, et al: Enlargement of spontaneous intracerebralhemorrhage. Incidence and time course. Stroke 27:1783–1787, 1996
28. Xi G, Keep R, Hoff J. Mechanisms of brain injury after intracerebral haemorrhage.Lancet Neurol. 2006;5:53–63.
29. Gebel JM, Jauch EC, Brott TG, et al. Natural history of perihematomal edema inpatients with hyperacute spontaneous intracerebral hemorrhage. Stroke. 2002;33:2631–2635.
30. Zazulia AR, Diringer MN, Derdeyn CP, et al. Progression of mass effect afterintracerebral hemorrhage. Stroke. 1999;30:1167–1173.
Created by Professor Yasser Metwally
http://yassermetwally.com
113

INDEX
INTRODUCTION
INTRODUCTION
In the last decade or so, cerebral microbleeds (CMBs) – tiny perivascular hemorrhagesseen as small, well-demarcated, hypointense, rounded lesions on MRI sequences that aresensitive to magnetic susceptibility – have generated increasing interest among neurologistsand clinical stroke researchers. As MRI techniques become more sophisticated, Cerebralmicrobleeds are increasingly detected in various patient populations (including all types ofstroke, Alzheimer’s disease and vascular cognitive impairment) and healthy community-dwelling older people. Their presence raises many clinical dilemmas and intriguingpathophysiological questions. Cerebral microbleeds are emerging as an important newmanifestation and diagnostic marker of cerebral small-vessel disease.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
114

Box 1. Cerebral microbleeds are a potential predictor of
1- Future intracerebral hemorrhagic risk.
2- A possible contributor to cognitive impairment anddementia.
3- A potential key link between vascular anddegenerative pathologies.
Cerebral microbleeds are defined radiologically as small, rounded, homogeneous,hypointense lesions on T2*-weighed gradient-recalled echo (T2*-GRE) and related MRIsequences that are sensitive to magnetic susceptibility.[2] Scharf et al. were the first toreport on small, intracerebral black dots of signal loss on T2-weighted spin-echo MRI inpatients with hypertensive cerebrovascular disease and intracerebral hemorrhage (ICH)associated with ischemic white matter disease and lacunar infarcts.[3] They called theselesions ‘hemorrhagic lacunes’, and their further characterization using T2*-GRE MRIsequences led to the current radiologic definition of ‘microbleeds’, a term coined byOffenbacher and colleagues in 1996.[4] A key feature of Cerebral microbleeds is that theyare not seen well on conventional computed tomography or MRI scans. Availablehistopathological studies suggest that Cerebral microbleeds radiological lesions are due totiny bleeds adjacent to abnormal small vessels, being mainly affected by hypertensiveangiopathy (arteriolosclerosis – usually lipohyaline degeneration related to hypertension)or cerebral amyloid angiopathy (CAA).[5]
Cerebral amyloid angiopathy
Cerebral amyloid angiopathy (CAA), also known as congophilic angiopathy, affectsexclusively the cerebral vasculature, without involvement of other areas of the body. Theamyloid substance is deposited in the media and adventitia of small and medium diameterarteries, as well as in veins, of the cortical surface and leptomeninges. The histologicaldiagnosis is made by showing areas of the vessel wall that stain with Congo red and show acharacteristic apple green birefringence under polarized light.
Cerebral amyloid angiopathy characteristically affects the elderly, with a linear increase infrequency with age. In routine autopsy studies, the frequency of Cerebral amyloidangiopathy has been 5-13% in those patients aged 60-69, 20-40% in patients aged 70-79,35-45% in patients aged 80-89, and 45-58% in individuals older than 90 years of age. Themain clinical manifestation of Cerebral amyloid angiopathy is Intracerebral hemorrhage,but an association with Alzheimer's disease and with a leukoencephalopathy are now wellrecognized as well.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
115

Figure 1. Lobar hemorrhage due to amyloid angiopathy, B Microscopic section of the braincortex, section has been stained with Congo Red for amyloid viewed with polarized light.The section shows relatively preserved cortical neurons and the blood vessels showsbirefringence with polarized light. In some areas the walls of the blood vessels are yellow-green (arrow). Diagnosis: Amyloid angiopathy, also known as congophilic angiopathy.
Table 1. The Intracerebral hemorrhages that occur in the setting of Cerebral amyloidangiopathy have several characteristic features. These include:
CCA
CCA
CCA
CCA
CCA
CCA
CCA
A lobar location, due to the cortical and leptomeningealdistribution of the angiopathy.
A frequently irregular, variegated appearance on acomputed tomography (CT) scan, which results fromextension of the superficially-located haemorrhage into theadjacent subarachnoid space.
A tendency to be recurrent, on occasion with multipleepisodes of lobar Intracerebral hemorrhage over periods ofmonths or years, a feature that is exceptionally rare inIntracerebral hemorrhage due to hypertension.
The occasional presence of multiple simultaneoushaemorrhages, is also a distinct rarity in Intracerebralhemorrhage of hypertensive mechanism.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
116

Figure 2. Precontrast CT scan showing irregular variegated putameno-capsularhaemorrhage [left two images] and a lobar subcortical haemorrhage [right]
The Intracerebral hemorrhage in patients with Cerebral amyloid angiopathy canoccasionally be related to preceding head trauma or a neurosurgical procedure, raising thepossibility that mechanically-induced vascular rupture may be at times involved in itspathogenesis. Similarly, the use of anticoagulant and fibrinolytic agents is beingincreasingly suspected as a potential risk factor in instances of Intracerebral hemorrhagein the elderly, presumed to harbour Cerebral amyloid angiopathy as a local vascular lesionpredisposing to Intracerebral hemorrhage.
The actual mechanism of bleeding in Cerebral amyloid angiopathy has not been elucidated.A factor that may be related to bleeding is the association of this angiopathy with othervascular changes, notably fibrinoid necrosis. Such vascular lesion has been found with highfrequency (71%) in instances of Cerebral amyloid angiopathy associated withIntracerebral hemorrhage, while it is not present in patients with Cerebral amyloidangiopathy but without Intracerebral hemorrhage. These data suggest that despite the highprevalence of Cerebral amyloid angiopathy in the elderly, the relatively low frequency ofIntracerebral hemorrhage may be explained by the need to have the associated changes offibrinoid necrosis in the affected vessels, in order to result in rupture and Intracerebralhemorrhage.
Figure 3. Precontrast CT scan showing lobar subcorticalhaemorrhage
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
117

CA with Intracerebral hemorrhage is a sporadic condition, but two rare familial formshave been described only in specific geographical locations in Iceland and in Holland. Thelatter form of familial Cerebral amyloid angiopathy with Intracerebral hemorrhage hasbeen characterized as a biochemical abnormality in the precursor protein of amyloid,which is also present in Alzheimer's disease and Down's syndrome.
Figure 4. Precontrast CT scan showingsimultaneous cerebral and cerebellarhaemorrhage in a single patient
Other associations of Cerebral amyloid angiopathy include Alzheimer's disease and aleukoencephalopathy. The histological features of Alzheimer's disease are present inapproximately 40% of patients with Cerebral amyloid angiopathy-related Intracerebralhemorrhage, and 30-40% of patients with Cerebral amyloid angiopathy have clinicalfeatures of dementia. The leukoencephalopathy of Cerebral amyloid angiopathy affects thewhite matter of the cerebral hemispheres, with preservation of the 'U' fibres, corpuscallosum, internal capsule, optic radiation, and white matter of the temporal lobes. Theimaging diagnosis of this leukoencephalopathy is greatly facilitated by the use of magneticresonance imaging (MRI), which shows hyperintensity of the white matter in T2-weightedsequences.
Box 2. Cerebral microbleeds are increasingly recognized in patients with the followingneurological disorders
1- Cerebrovascular disease (including first-ever and recurrent ischemic or hemorrhagicstroke),[6,7]
2- Alzheimer’s disease,[8,9]
3- Vascular cognitive impairment[10]
4- Normal elderly populations. [11]
Cerebral microbleeds are emerging as a manifestation and diagnostic marker of cerebralsmall-vessel disease (along with lacunar infarcts, leukoaraiosis, ) .[13–17] They are apotential predictor of Intracerebral hemorrhage risk, a possible contributor to cognitive
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
118

impairment and dementia and may provide a new imaging tool to understand the linksbetween vascular and degenerative pathologies.[2]
Cerebral microbleeds are small brain hemorrhages that are presumed to result fromleakage of blood cells from damaged small vessel walls. They were first detected on MRimaging only in the mid-1990s, as MR imaging sequences sensitive to blood-breakdownproducts became available (eg, T2-weighted gradient-echo technique), which are essentialfor microbleed detection. Histologically, these small black dots on MR imaging representhemosiderin-laden macrophages that are clustered around small vessel. The choice of fieldstrength, sequence parameters (particularly echo time), and postprocessing (eg,susceptibility-weighted imaging technique) have all been found to have a major influenceon the detection rate of cerebral microbleeds. With these advances in imaging, theprevalence of microbleeds has been estimated to be more than 20% in persons aged 60years and older, increasing to nearly 40% in those older than 80 years. Microbleeds arealso commonly asscoiated with microvascular brain disease. Microbleed location isgenerally divided into deep (ie, basal ganglia, thalamus) and infratentorial versus lobarbrain regions.
Figure 5. Cerebral Microbleeds. (A) An axial T2-weighted MRI. (B) A T2*-weightedgradient-recalled echo (T2*-GRE) MRI. Note the microbleeds – small, dark dot-like lesions(arrow) visible only on the T2*-weighted gradient-recalled echo (T2*-GRE) MRI.
In the aging population, microbleeds in lobar locations share apolipoprotein E (APOE) e4genotype as a common risk factor with Cerebral amyloid angiopathy (CAA) andAlzheimer's disease (AD), suggestive of a potential link between vascular and amyloidneuropathology. This link has further been corroborated by the finding that topography oflobar microbleeds in community-dwelling elderly individuals follows the same posteriordistribution as is known from amyloid disease in Cerebral amyloid angiopathy (CAA) andAlzheimer's disease (AD). Furthermore, some reports show that presence of microbleeds,
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
119

and particularly those in lobar locations, relates to worse cognitive function, both inhealthy elderly individuals and in patients diagnosed with Alzheimer's disease (AD). Incontrast, deep or infratentorial microbleeds in aging individuals are primarily linked toclassic cardiovascular risk factors and are more likely caused by hypertensivevasculopathy. Longitudinal studies indicate that incident microbleeds commonly occurover time: annually, 3% of presumed healthy elderly individuals develop new microbleeds,increasing to more than 7% of those who already have microbleeds at baseline. Incomparison, these rates are doubled in patients attending a memory clinic.
Table 2. Location of cerebral microbleeds and clinical significance
Location Clinical significance
lobar locations In the aging population, microbleeds in lobar locations shareapolipoprotein E (APOE) e4 genotype as a common risk factorwith Cerebral amyloid angiopathy (CAA) and Alzheimer's disease(AD), suggestive of a potential link between vascular and amyloidneuropathology.
Deep or infratentorialmicrobleeds
Deep or infratentorial microbleeds in aging individuals areprimarily linked to classic cardiovascular risk factors and aremore likely caused by hypertensive vasculopathy and small vesseldisease.
The increasing evidence that microbleeds reflect both vascular disease as well as amyloidangiopathy has led to the belief that these may well represent the missing link between thevascular and amyloid hypotheses in the pathogenesis of Alzheimer's disease (AD).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
120

Figure 6. A postmortem section of thebrain showing a cortical microbleed(arrow) in a patient with Alzheimer’sdisease and CAA
Figure 7. Microbleed imaging. T1-weighted (left), T2-weighted (middle), and T2-weighted(right) images. Cerebral microbleeds, depicted by arrows, are visualized only on the T2-weighted image and not on the T1-weighted or T2-weighted images. The T2-weightedimage is susceptible to paramagnetic properties of hemosiderin, causing the microbleeds toappear as black dots of signal loss.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
121

Figure 8 Microbleed location. T2-weighted MR images showing microbleeds (arrows) inlobar (left), deep (middle), and infratentorial (right) locations.
Table 3. Pathology of ischemic microvascular brain disease
Central and corticalatrophy
This is secondary to chronic global reduction of brain perfusion.
Leukoaraiosis (diffuseperiventricular whitematter disease)
Leukoaraiosis is an ischaemic demyelination of the immediateperiventricular white matter with axonal loss, astrogliosis and interstitialedema. It is secondary to chronic global reduction of brain perfusion.
Lacunar infarctions lacunar infarctions are secondary to the micro vascular thrombo-occlusive episodes. They are most numerous in the periventricular graymatter (thalamus and basal ganglia) and the immediate periventricularwhite matter. Spasm of the fine penetrating arterioles (secondary toincreased VSMCs sensitivity) -can also result in Lacunar infarctions.
Granular atrophy Granular atrophy is defined pathologically as infarctions localized to thecerebral cortex and not extending to the subcortical white matter.
Basal ganglioniccalcifications
These are calcification of the the arteriolar wall of the microcirculationwithin the basal ganglia.
Dilated Virchow-RobinSpaces
Dilation of Virchow-Robin Spaces provides a potential alternativebiomarker of microvascular disease (small vessel disease).
Cerebral Microbleeds The increasing evidence that microbleeds reflect both microvascularbrain disease as well as amyloid angiopathy has led to the belief thatthese may well represent the missing link between the vascular andamyloid hypotheses in the pathogenesis of Alzheimer’s disease (AD).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
122

Physical Principles of Microbleed MRI Detection
The available data suggest that Cerebral microbleeds are composed of small collections ofblood-breakdown products (in particular hemosiderin) contained within perivascularmacrophages. Hemosiderin is an extremely paramagnetic material; this property, knownas magnetic susceptibility, describes the degree to which a tissue (or any material) respondsmagnetically when placed in an exogenous magnetic field.[20] Consequently, whenhemosiderin deposits are brought into the magnetic field of an MRI scanner, microscopiclocal magnetic fields develop, which create significant macroscopical inhomogeneities in themagnetic field surrounding Cerebral microbleeds , leading to fast decay of the local MRIsignal, a phenomenon called the ‘susceptibility effect’.[12] Similar distortions of themagnetic field are also caused by the close proximity of tissues with different magneticsusceptibilities (e.g., at the interface of soft tissues, bone and air).
Figure 9. Lobar microbleeds on 3-dimensional T2*-weighted gradient-recalled echo MRI in an 80 years old manwith dementia and cerebral amyloidangiopathy.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
123

Figure 10. Example ofincident microbleeds on 3-dimensional T2*-weightedgradient-recalled echo MRIin an 80 years old man. Themicrobleeds are lobar inlocation
Figure 11. Radiologic-pathologic correlation of cerebral microbleeds on MR imaging (3 T).Postmortem brain MR imaging shows on T2-weighted imaging a hypointense focus on thegray-white matter interface (white arrow). MR image in the middle of the isolated tissueblock containing this hypointense focus. Pathologic analysis of this tissue block(hematoxylin and eosin stain) shows macrophages containing hemosiderin (black arrows),confirming that the hypointense lesion on MR imaging is compatible with a microbleed.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
124

Figure 12. Example of incidentmicrobleeds on 3-dimensional T2*-weighted gradient-recalled echo MRIin an 80 years old man. Themicrobleeds are mainly lobar inlocation. The patient is presentedclinical with the clinical picture ofAlzheimer dementia.
MRI Criteria for Microbleed Identification & Differential Diagnosis
Cerebral microbleeds are defined as small, rounded or ovoid, blooming, homogeneoussignal voids on T2*-GRE and related MRI sequences that are sensitive to susceptibilityeffects. A precise size definition does not appear to substantially influence the detection ofCerebral microbleeds : although the upper size limit is usually taken to be between 5 and10 mm, a recent analysis revealed that the volume of microbleeds and macrobleeds (at leastin a cohort of patients with Cerebral amyloid angiopathy) is not a continuum, but shows abimodal distribution.[32] Blood vessels in the subarachnoid space, calcifications of thebasal ganglia or cavernous malformations can all give rise to small, dot-like, low-signalareas on T2*-GRE MRI. Careful inspection of contiguous slices using different imagingmodalities (CT, T2 MRI, FLAIR or DWI) and lesion geometry and location facilitates theidentification of Cerebral microbleeds .
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
125

Figure 13. Deep microbleeds in a patientwith lacunar stroke
Histopathological Correlates of Cerebral microbleeds
Neuroimaging–pathological correlation studies, as well as other histopathological analysesof Cerebral microbleeds ,[38,44–47] show that Cerebral microbleeds are commonlyassociated with two different small-vessel pathologies: hypertensive vasculopathy(Lipohyelinosis) and Cerebral amyloid angiopathy. Moreover, these two microangiopathicdisorders seem to influence Cerebral microbleeds topography. Typically, hypertensivevasculopathy results in Cerebral microbleeds in the basal ganglia, thalamus, brainstem andcerebellum, while Cerebral amyloid angiopathy is characterized by a lobar, cortical–subcortical distribution.[2]
Risk Factors & Associations
Apart from being associated with specific underlying vasculopathies, Cerebral microbleedsare strongly associated with a number of clinical syndromes including ischemic andhemorrhagic stroke, Alzheimer’s disease and vascular cognitive impairment.[12]
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
126

Figure 14. Patterns of Cerebral Microbleed Distribution. (A) Axial T2*-weighted gradient-recalled echo of an elderly individual without a history of hypertension, showingmicrobleeds in strictly lobar.
o Pathophysiology of Cerebral microbleeds
Cerebral microbleeds are unique among the MRI manifestations of cerebral small-vesseldisease, in that they seem to provide direct evidence of microvascular leakiness, causingblood-breakdown products to extravasate through the vessel wall. By contrast,Leukoaraiosis -in small vessel disease) lack pathological specificity and may result from awide range of both vascular and inflammatory conditions. In the setting of small-vesseldisease, the vascular endothelium of small arterioles and capillaries seems to becomepermeable to elements such as red blood cells, inflammatory cells and plasma proteins,[66]which are normally excluded by the BBB.[67] Thus, it seems highly plausible thatendothelial/BBB derangement could play a key role in Cerebral microbleeds formation,[68]although direct evidence for this hypothesis is limited so far.
Clinical Implications of Cerebral microbleeds
It is now becoming evident that Cerebral microbleeds can contribute to neurologicdysfunction, long-term disability and cognitive impairment. A population-based study ofelderly people (n = 435) with or at high risk of cardiovascular disease investigated theprognostic value of Cerebral microbleeds regarding overall, cardiovascular-related andstroke-related mortality.[87] Compared with subjects without any Cerebral microbleeds ,subjects with more than one Cerebral microbleed had a sixfold risk of stroke-related death(hazard ratio: 5.97; 95% CI: 1.60–22.26; p = 0.01).[87] However, the most striking findingswere that deep Cerebral microbleeds were found to be significantly and independently
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
127

associated with cardiovascular mortality (hazard ratio: 2.67; 95% CI: 1.23–5.81; p = 0.01),whereas strictly lobar Cerebral microbleeds were significantly associated with stroke-related mortality (hazard ratio: 7.20; 95% CI: 1.44–36.10; p = 0.02).[87] Also in a previousstudy, the presence of Cerebral microbleeds (especially multiple Cerebral microbleeds )was the strongest predictor of mortality (among other MRI markers of vascular damage,such as WMCs) in a memory clinic population of 1138 patients.[88]
As well as affecting mortality and stroke risk, the accumulation of multiple Cerebralmicrobleeds could have a cumulative effect on brain functions subserved by distributednetworks, such as gait or cognition. It is important to note that there are many potentialconfounders in the study of how Cerebral microbleeds could affect brain function andcause clinical impairment. Their close relationship and overlap with other imagingcorrelates of cerebral small vessel disease such as lacunes and white matter damage, as wellas all types of clinical stroke syndromes, makes it challenging to dissect their independenteffects.
Cerebral microbleeds & Neurological Functiono Gait.
In a cross-sectional study, De Laat et al. reported the first indications that Cerebralmicrobleeds (especially in the temporal and frontal lobe, basal ganglia and thalamus) maybe associated with gait disturbances, independently of other coexisting markers of cerebralsmall-vessel disease.[89] In addition, in a prospective cohort of elderly patients (n = 94)presenting with spontaneous lobar Intracerebral hemorrhage, Greenberg and colleaguesshowed that a high number of Cerebral microbleeds at baseline was associated with a high3-year cumulative risk of cognitive impairment, functional dependence or death (beingmore than 50% in individuals with more than six Cerebral microbleeds ).[90] Cerebralmicrobleeds have also been associated with clinical disability in cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy.[91]
o Cognition.
There has been increasing attention given to Cerebral microbleeds in relation to cognition.Werring and colleagues systematically examined the cognitive impact of Cerebralmicrobleeds [92] in a neurovascular clinic population. Consecutive patients with Cerebralmicrobleeds (n = 25) were compared with a control group without Cerebral microbleeds (n= 30) that was closely matched for age, leukoaraiosis severity, prevalence and location ofcortical infarctions and ischemic stroke subtype (i.e., factors likely to influencecognition).[92] A striking difference in the prevalence of executive dysfunction was foundbetween the two groups: 60% of patients with Cerebral microbleeds were impaired infrontal executive function (i.e., initiation, planning and higher-order problem-solvingbehaviors among others), compared with only 30% of nonmicrobleed patients (p =0.03).[92]
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
128

Cerebral microbleeds as Prognostic Markers of Recurrent Stroke
Whether Cerebral microbleeds are a marker of increased future stroke risk (particularlyintracerebral hemorrhage) is one of the most clinically relevant questions at present, yetfew longitudinal data of good quality are available. A previous systematic reviewdemonstrated that Cerebral microbleeds were more prevalent among patients withrecurrent stroke rather than patients with a first-ever stroke.[6] Although this generalconclusion was derived from a small number of patients (n = 1021), it suggests thatCerebral microbleeds may be a useful imaging marker of ongoing cerebrovasculardamage,[6] which can add additional information about stroke recurrence (to that obtainedusing standard MRI sequences).
Overall, the association of Cerebral microbleeds with spontaneous intracerebralhemorrhage raises a clinical dilemma concerning the safety of antithrombotic treatments.Since Cerebral microbleeds provide direct evidence of blood leakage from pathologicallyfragile small vessels, their presence may be a risk factor for antithrombotic-associatedintracerebral hemorrhage, raising the important question of whether Cerebral microbleedsmay shift the risk–benefit balance away from antithrombotic use in some patients.
Cerebral microbleeds & Treatment: Balancing the Riskso Cerebral microbleeds & Antithrombotic Treatment.
Antiplatelet and anticoagulant treatments are widely used in patients at high risk ofcardiovascular or cerebrovascular disease (e.g., ischemic stroke, ischemic heart disease oratrial fibrillation). In our aging population, the lifetime risk for developing atrialfibrillation is one in four people over the age of 40 years.[125] If left untreated, atrialfibrillation increases the risk of ischemic stroke fivefold, with the highest risk seen inelderly patients who have had a previous stroke or transient ischemic attack. In this setting,anticoagulation reduces ischemic stroke risk by approximately 65%. However, this benefithas to be balanced against an increased risk of intracerebral hemorrhage, which is themost feared complication of anticoagulation, causing death or severe disability in up to75% of patients.[126] A recent observational inception cohort study of patients treatedwith anticoagulation (of whom a quarter had a previous history of stroke) reported a 2.5%(95% CI: 1.1–4.7%) risk of Intracerebral hemorrhage in 1 year.[127] Over the last decade,increasing use of warfarin to prevent cardioembolic stroke due to atrial fibrillation has ledto a fivefold increase in the incidence of anticoagulant-related intracerebral hemorrhage,which now accounts for approximately 15% of all intracerebral hemorrhage.[128] Thistrend is set to continue and will be a huge future healthcare, social and economic challenge.With the potential availability of new oral anticoagulants such as dabigatran,[129] it islikely that even more acute cardioembolic stroke patients will be using oral anticoagulationfor secondary stroke prevention. It is a paradox that many of these elderly patients at thehighest risk of cardioembolic stroke are also at the highest risk of Intracerebralhemorrhage. In many patients, this makes it extremely difficult to balance the antiocclusiveand prohemorrhagic effects of antithrombotic drugs; improving this risk–benefitassessment for individual patients remains a major goal of research in cerebrovascularmedicine.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
129

Because anticoagulation-related intracerebral hemorrhage is associated with increased ageand previous stroke, and it often occurs with anticoagulation intensity within thetherapeutic range,[130] it is likely that the mechanism underlying this high risk is relatedto individual patient factors (e.g., an age-related disorder of small brain vessels, such asCerebral amyloid angiopathy or hypertensive small-vessel disease). In keeping with thishypothesis, some studies suggest that WMCs (a marker of small-vessel disease) increase therisk of anticoagulant-related Intracerebral hemorrhage.[131,132] Because they providedirect evidence of blood leakage from pathologically fragile small vessels, Cerebralmicrobleeds might be a stronger independent predictor of anticoagulation-associatedIntracerebral hemorrhage. The available studies on Cerebral microbleeds andanticoagulation-associated Intracerebral hemorrhage risk have many limitations, withmost being cross-sectional studies in Asian cohorts, so their findings cannot clearly showcausative relationships and may not be generalizable to other populations.[120,133–146]Nonetheless, existing data support the hypothesis that the presence of Cerebral microbleedsincreases the risk of Intracerebral hemorrhage as a complication of antithromboticmedication.[135,142,145] A prospective study reported Cerebral microbleeds in 87% ofpatients with Intracerebral hemorrhage following warfarin treatment for atrialfibrillation,[142] while a recent case–control study also reported more Cerebralmicrobleeds in warfarin-associated Intracerebral hemorrhage than in matched warfarinusers without Intracerebral hemorrhage.[141]
Cerebral microbleeds in the Setting of Other Treatmentso Thrombolysis
Another relevant question is whether there is an increased risk of intracerebralhemorrhage after thrombolysis of patients with ischemic stroke when Cerebralmicrobleeds are present. Some studies that explored the association between Cerebralmicrobleeds and the risk of hemorrhagic transformation following intravenous tissueplasminogen activator in patients who have had ischemic stroke have indicated possiblelinks,[143,152] while more recent studies have questioned these findings.[153,154] TheBRASIL study (the largest prospective, multicenter study to date), which included 570ischemic stroke patients, found that symptomatic Intracerebral hemorrhage occurred in5.8% of patients with Cerebral microbleeds versus 2.7% of patients without Cerebralmicrobleeds (p = 0.170).[153] However, all of the studies were underpowered to providereliable data of such an effect[6,155] and leave unanswered the questions of the role ofstrictly lobar microbleeds (reflecting underlying Cerebral amyloid angiopathy pathology)and multiple Cerebral microbleeds on the shaping of the risk.[49]
o Statins
Some neurologists have raised concerns over the use of statins in patients with Cerebralmicrobleeds . In the Rotterdam study, low serum cholesterol levels were found to bestrongly associated with the presence of strictly lobar microbleeds.[56] However, thisassociation was not replicated in the recent update of the study.[85] Lee and colleagues alsofound a relationship between low cholesterol concentrations and higher microbleed burdenin the 172 patients they studied.[156] In a more recent retrospective analysis of 349 patients
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
130

with acute ischemic stroke or transient ischemic attack, previous statin therapy was notassociated with either the prevalence or the degree of Cerebral microbleeds .[157] The roleof statins and low serum cholesterol in patients with microbleeds needs further exploration,particularly in light of the results of a randomized controlled trial of atorvastatin inpatients with stroke, which showed a small increase in the incidence of Intracerebralhemorrhage among patients receiving high doses of the drug.[158] The increased risk ofIntracerebral hemorrhage may be due to pleiotropic effects of statins other than the lipid-lowering effects.[159]
References
1.Werring D. Cerebral Microbleeds: Pathophysiology to Clinical Practice. CambridgeUniversity Press, Cambridge, UK (2011).
2.Greenberg SM, Vernooij MW, Cordonnier C et al. Cerebral microbleeds: a guide todetection and interpretation. Lancet Neurol. 8, 165—174(2009).
3.Scharf J, Brauherr E, Forsting M, Sartor K. Significance of haemorrhagic lacunes onMRI in patients with hypertensive cerebrovascular disease and intracerebral haemorrhage.Neuroradiology 36, 504—508 (1994).
4.Offenbacher H, Fazekas F, Schmidt R,Koch M, Fazekas G, Kapeller P. MR of cerebralabnormalities concomitant with primary intracerebral hematomas. AJNR Am. J.Neuroradiol. 17, 573—578 (1996).
5.Fazekas F, Kleinert R, Roob G et al.Histopathologic analysis of foci of signal loss ongradient-echo T2*-weighted MR images in patients with spontaneous intracerebralhemorrhage: evidence of microangiopathy-related microbleeds. AJNR Am. J. Neuroradiol.20, 637—642 (1999).
6.Cordonnier C, Al-Shahi Salman R, Wardlaw J. Spontaneous brain microbleeds:systematic review, subgroup analyses and standards for study design and reporting. Brain130, 1988—2003 (2007).
7.Werring DJ, Coward LJ, Losseff NA, Jager HR, Brown MM. Cerebral microbleeds arecommon in ischemic stroke but rare in TIA. Neurology 65, 1914—1918 (2005).
8.Pettersen JA, Sathiyamoorthy G, Gao FQ et al. Microbleed topography, leukoaraiosis,and cognition in probable Alzheimer disease from the sunnybrook dementia study. Arch.Neurol. 65, 790—795 (2008).
9.Cordonnier C, van der Flier WM. Brain microbleeds and Alzheimer's disease: innocentobservation or key player? Brain 134, 335—344 (2011).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
131

10.Cordonnier C, van der Flier WM, Sluimer JD, Leys D, Barkhof F, Scheltens P.Prevalence and severity of microbleeds in a memory clinic setting. Neurology 66, 1356 —1360 (2006).
11.Poels MM, Vernooij MW, Ikram MA et al. Prevalence and risk factors of cerebralmicrobleeds: an update of the Rotterdam scan study. Stroke 41, S103—S106 (2010).
12.Werring DJ. Cerebral microbleeds: clinical and pathophysiological significance. J.Neuroimaging 17, 193—203 (2007).
13.Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristicsto therapeutic challenges. Lancet Neurol. 9, 689—701 (2010).
14.Thompson CS, Hakim AM. Living beyond our physiological means: small vessel diseaseof the brain is an expression of a systemic failure in arteriolar function: a unifyinghypothesis. Stroke 40, E322—E330 (2009).
15.Vinters HV. Cerebral amyloid angiopathy. A critical review. Stroke 18, 311—324(1987).
16.Attems J, Jellinger K, Thal DR, Van Nostrand W. Review: Sporadic cerebral amyloidangiopathy. Neuropathol. Appl. Neurobiol. 37, 75—93 (2011).
17.Imaizumi T, Miyata K, Inamura S, Kohama I, Sang Nyon K, Nomura T. The differencein location between traumatic cerebral microbleeds and microangiopathic microbleedsassociated with stroke. J. Neuroimaging DOI: 10.1111/j.1552-6569.2011.00593.x (2011)(Epub ahead of print).
18.Scheid R, Preul C, Gruber O, Wiggins C, von Cramon DY. Diffuse axonal injuryassociated with chronic traumatic brain injury: evidence from T2*-weighted gradient-echoimaging at 3 T. AJNR Am. J. Neuroradiol. 24, 1049—1056 (2003).
19.Gouw AA, Seewann A, van der Flier WM et al. Heterogeneity of small vessel disease: asystematic review of MRI and histopathology correlations. J. Neurol. Neurosurg.Psychiatry (2010).
20.Roberts TP, Mikulis D. Neuro MR: principles. J. Magn. Reson. Imaging 26, 823—837(2007).
21.Mikulis DJ, Roberts TP. Neuro MR: protocols. J. Magn. Reson. Imaging 26, 838—847(2007).
22.Chavhan GB, Babyn PS, Thomas B, Shroff MM, Haacke EM. Principles, techniques,and applications of T2*-based MR imaging and its special applications. Radiographics 29,1433—1449 (2009).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
132

23.Tanaka A, Ueno Y, Nakayama Y, Takano K, Takebayashi S. Small chronichemorrhages and ischemic lesions in association with spontaneous intracerebralhematomas. Stroke 30, 1637—1642 (1999).
24.Gregoire SM, Werring DJ, Chaudhary UJ et al. Choice of echo time on GRE T2*-weighted MRI influences the classification of brain microbleeds. Clin. Radiol. 65, 391—394(2010).
25.Conijn MM, Geerlings MI, Luijten PR et al. Visualization of cerebral microbleeds withdual-echo T2*-weighted magnetic resonance imaging at 7.0 T. J. Magn. Reson. Imaging 32,52—59 (2010).
26.Ayaz M, Boikov AS, Haacke EM, Kido DK, Kirsch WM. Imaging cerebral microbleedsusing susceptibility weighted imaging: one step toward detecting vascular dementia. J.Magn. Reson. Imaging 31, 142—148 (2010).
27.Nandigam RN, Viswanathan A, Delgado P et al. MR imaging detection of cerebralmicrobleeds: effect of susceptibility-weighted imaging, section thickness, and field strength.AJNR Am. J. Neuroradiol. 30, 338—343 (2009).
28.Vernooij MW, Ikram MA, Wielopolski PA, Krestin GP, Breteler MM, van der Lugt A.Cerebral microbleeds: accelerated 3D T2*-weighted GRE MR imaging versus conventional2D T2*-weighted GRE MR imaging for detection. Radiology 248, 272—277 (2008).
29.Tatsumi S, Ayaki T, Shinohara M, Yamamoto T. Type of gradient recalled-echosequence results in size and number change of cerebral microbleeds. AJNR Am. J.Neuroradiol. 29, E13 (2008).
30.Stehling C, Wersching H, Kloska SP et al. Detection of asymptomatic cerebralmicrobleeds: a comparative study at 1.5 and 3.0 T. Acad. Radiol. 15, 895—900 (2008).
31.Jeerakathil T, Wolf PA, Beiser A et al. Cerebral microbleeds: prevalence andassociations with cardiovascular risk factors in the Framingham study. Stroke 35, 1831—1835 (2004).
32.Greenberg SM, Nandigam RN, Delgado P et al. Microbleeds versus macrobleeds:evidence for distinct entities. Stroke 40, 2382—2386 (2009).
33.Gregoire SM, Chaudhary UJ, Brown MM et al. The Microbleed Anatomical RatingScale (M ARS): reliability of a tool to map brain microbleeds. Neurology 73, 1759—1766(2009).
34.Cordonnier C, Potter GM, Jackson CA et al. improving interrater agreement aboutbrain microbleeds: development of the Brain Observer Microbleed Scale (BOMBS). Stroke40, 94—99 (2009).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
133

35.Haacke EM, Xu Y, Cheng YC, Reichenbach JR. Susceptibility weighted imaging (SWI).Magn. Reson. Med. 52, 612—618 (2004).
36.Mittal S, Wu Z, Neelavalli J, Haacke EM. Susceptibility-weighted imaging: technicalaspects and clinical applications, part 2. AJNR Am. J. Neuroradiol. 30, 232—252 (2009).
37.Charidimou A, Werring DJ. Letter by Charidimou and Werring regarding article,'Cerebral microbleeds in the elderly'. Stroke 42(4), E368 (2011).
38.Fisher M, French S, Ji P, Kim RC. Cerebral microbleeds in the elderly. A pathologicalanalysis. Stroke 41(12), 2782—2785 (2010).
39.Wu Z, Mittal S, Kish K, Yu Y, Hu J, Haacke EM. Identification of calcification withMRI using susceptibility-weighted imaging: a case study. J. Magn. Reson. Imaging 29,177—182 (2009).
40.Goos JD, van der Flier WM, Knol DL et al. Clinical relevance of improved microbleeddetection by susceptibility-weighted magnetic resonance imaging. Stroke 42(7), 1894—1900(2011).
41.Conijn MM, Geerlings MI, Biessels GJ et al. Cerebral microbleeds on MR imaging:comparison between 1.5 and 7T. AJNR Am. J. Neuroradiol. 32(6), 1043—1049 (2011).
42.Schrag M, McAuley G, Pomakian J et al. Correlation of hypointensities in susceptibility-weighted images to tissue histology in dementia patients with cerebral amyloid angiopathy:a postmortem MRI study. Acta Neuropathol. 119(3), 291—302 (2011).
43.Tatsumi S, Shinohara M, Yamamoto T. Direct comparison of histology of microbleedswith postmortem MR images: a case report. Cerebrovasc. Dis. 26, 142—146 (2008).
44.De Reuck J, Deramecourt V, Cordonnier C, Leys D, Maurage CA, Pasquier F. Theimpact of cerebral amyloid angiopathy on the occurrence of cerebrovascular lesions indemented patients with Alzheimer features: a neuropathological study. Eur. J. Neurol.18(6), 913—918 (2011).
45.De Reuck J, Deramecourt V, Cordonnier C, Leys D, Pasquier F, Maurage CA.Prevalence of small cerebral bleeds in patients with a neurodegenerative dementia: aneuropathological study. J. Neurol. Sci. 300(1—2), 63—66 (2010).
46.Machida K, Tojo K, Naito KS, Gono T, Nakata Y, Ikeda S. Cortical petechialhemorrhage, subarachnoid hemorrhage and corticosteroid-responsiveleukoencephalopathy in a patient with cerebral amyloid angiopathy. Amyloid 15, 60—64(2008).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
134

47.Kikuta K, Takagi Y, Nozaki K, Okada T, Hashimoto N. Histological analysis ofmicrobleed after surgical resection in a patient with moyamoya disease. Neurol. Med. Chir.(Tokyo) 47, 564—567 (2007).
48.Cordonnier C. Brain microbleeds: more evidence, but still a clinical dilemma. Curr.Opin. Neurol. 24(1), 69—74 (2011).
49.Cordonnier C. Brain microbleeds. Pract. Neurol. 10, 94—100 (2010).
50.Koennecke HC. Cerebral microbleeds on MRI: prevalence, associations, and potentialclinical implications. Neurology 66, 165—171 (2006).
51.Fiehler J. Cerebral microbleeds: old leaks and new haemorrhages. Int. J. Stroke 1,122—130 (2006).
52.Horita Y, Imaizumi T, Niwa J et al. Analysis of dot-like hemosiderin spots using braindock system. No. Shinkei Geka. 31, 263—267 (2003).
53.Tsushima Y, Tanizaki Y, Aoki J, Endo K. MR detection of microhemorrhages inneurologically healthy adults. Neuroradiology 44, 31—36 (2002).
54.Roob G, Schmidt R, Kapeller P, Lechner A, Hartung HP, Fazekas F. MRI evidence ofpast cerebral microbleeds in a healthy elderly population. Neurology 52, 991—994 (1999).
55.Sveinbjornsdottir S, Sigurdsson S, Aspelund T et al. Cerebral microbleeds in thepopulation based AGES—Reykjavik study: prevalence and location. J. Neurol. Neurosurg.Psychiatry 79, 1002—1006 (2008).
56.Vernooij MW, van der Lugt A, Ikram MA et al. Prevalence and risk factors of cerebralmicrobleeds: the Rotterdam scan study. Neurology 70, 1208—1214 (2008).
57.Mesker DJ, Poels MM, Ikram MA et al. Lobar distribution of cerebral microbleeds: therotterdam scan study. Arch. Neurol. 68, 656—659 (2011).
58.Rosand J, Muzikansky A, Kumar A et al. Spatial clustering of hemorrhages in probablecerebral amyloid angiopathy. Ann. Neurol. 58, 459—462 (2005).
59.Knudsen KA, Rosand J, Karluk D, Greenberg SM. Clinical diagnosis of cerebralamyloid angiopathy: validation of the Boston criteria. Neurology 56, 537—539 (2001).
60.O'Donnell HC, Rosand J, Knudsen KA et al. Apolipoprotein E genotype and the risk ofrecurrent lobar intracerebral hemorrhage. N. Engl. J. Med. 342, 240—245 (2000).
61.Lee SH, Park JM, Kwon SJ et al. Left ventricular hypertrophy is associated withcerebral microbleeds in hypertensive patients. Neurology 63, 16—21 (2004).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
135

62.Staals J, van Oostenbrugge RJ, Knottnerus IL, Rouhl RP, Henskens LH, Lodder J.Brain microbleeds relate to higher ambulatory blood pressure levels in first-ever lacunarstroke patients. Stroke 40, 3264—3268 (2009).
63.Henskens LH, van Oostenbrugge RJ, Kroon AA, de Leeuw PW, Lodder J. Brainmicrobleeds are associated with ambulatory blood pressure levels in a hypertensivepopulation. Hypertension 51, 62—68 (2008).
64.Qiu C, Cotch MF, Sigurdsson S et al. Retinal and cerebral microvascular signs anddiabetes: the age, gene/environment susceptibility—Reykjavik study. Diabetes 57, 1645—1650 (2008).
65.Wardlaw JM, Lewis SC, Keir SL, Dennis MS, Shenkin S. Cerebral microbleeds areassociated with lacunar stroke defined clinically and radiologically, independently of whitematter lesions. Stroke 37, 2633—2636 (2006).
66.Cullen KM, Kocsi Z, Stone J. Pericapillary haem-rich deposits: evidence formicrohaemorrhages in aging human cerebral cortex. J. Cereb. Blood Flow Metab. 25, 1656—1667 (2005).
67.Neuwelt EA, Bauer B, Fahlke C et al. Engaging neuroscience to advance translationalresearch in brain barrier biology. Nat. Rev. Neurosci. 12, 169—182 (2011).
68.Wardlaw JM. Blood—brain barrier and cerebral small vessel disease. J. Neurol. Sci.299, 66—71 (2010).
69.Vasilevko V, Passos GF, Quiring D et al. Aging and cerebrovascular dysfunction:contribution of hypertension, cerebral amyloid angiopathy, and immunotherapy. Ann. NYAcad. Sci. 1207, 58—70 (2010).
70.Iadecola C, Park L, Capone C. Threats to the mind: aging, amyloid, and hypertension.Stroke 40, S40—S44 (2009).
71.Zlokovic BV. The blood—brain barrier in health and chronic neurodegenerativedisorders. Neuron 57, 178—201 (2008).
72.Koh SH, Park CY, Kim MK et al. Microbleeds and free active MMP-9 are independentrisk factors for neurological deterioration in acute lacunar stroke. Eur. J. Neurol. 18, 158—164 (2011).
73.Kidwell CS, Greenberg SM. Red meets white: do microbleeds link hemorrhagic andischemic cerebrovascular disease? Neurology 73, 1614—1615 (2009).
74.Kimberly WT, Gilson A, Rost NS et al. Silent ischemic infarcts are associated withhemorrhage burden in cerebral amyloid angiopathy. Neurology 72, 1230—1235 (2009).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
136

75.Menon RS, Kidwell CS. Neuroimaging demonstration of evolving small vessel ischemicinjury in cerebral amyloid angiopathy. Stroke 40, E675—E677 (2009).
76.Gregoire SM, Charidimou A, Gadapa N et al. Acute ischaemic brain lesions inintracerebral haemorrhage: multi-centre cross-sectional MRI study. Brain (2011) (Inpress).
77.Jeon SB, Kwon SU, Cho AH, Yun SC, Kim JS, Kang DW. Rapid appearance of newcerebral microbleeds after acute ischemic stroke. Neurology 73, 1638—1644 (2009).
78.Cianchetti FA, Nishimura N, Schaffer CB. Cortical microhaemorrhages reducestimulus-evoked calcium responses in nearby neurons. J. Cereb. Blood Flow Metab. 29,S217—S218 (2009).
79.Baumann CR, Schuknecht B, Lo Russo G et al. Seizure outcome after resection ofcavernous malformations is better when surrounding hemosiderin-stained brain also isremoved. Epilepsia 47, 563—566 (2006).
80.Hammen T, Romstock J, Dorfler A, Kerling F, Buchfelder M, Stefan H. Prediction ofpostoperative outcome with special respect to removal of hemosiderin fringe: a study inpatients with cavernous haemangiomas associated with symptomatic epilepsy. Seizure 16,248—253 (2007).
81.Greenberg SM, Vonsattel JP, Stakes JW, Gruber M, Finklestein SP. The clinicalspectrum of cerebral amyloid angiopathy: presentations without lobar hemorrhage.Neurology 43, 2073—2079 (1993).
82.Roch JA, Nighoghossian N, Hermier M et al. Transient neurologic symptoms related tocerebral amyloid angiopathy: usefulness of T2*-weighted imaging. Cerebrovasc. Dis. 20,412—414 (2005).
83.Watanabe A, Kobashi T. Lateral gaze disturbance due to cerebral microbleed in themedial lemniscus in the mid-pontine region: a case report. Neuroradiology 47, 908—911(2005).
84.Gregoire SM, Brown MM, Kallis C, Jager HR, Yousry TA, Werring DJ. MRI detectionof new microbleeds in patients with ischemic stroke: five-year cohort follow-up study.Stroke 41, 184—186 (2010).
85.Poels MM, Ikram MA, van der Lugt A et al. Incidence of cerebral microbleeds in thegeneral population: the Rotterdam scan study. Stroke 42(3), 656—661 (2011).
86.Goos JD, Henneman WJ, Sluimer JD et al. Incidence of cerebral microbleeds: alongitudinal study in a memory clinic population. Neurology 74, 1954—1960 (2010).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
137

87.Altmann-Schneider I, Trompet S, de Craen AJ et al. Cerebral microbleeds arepredictive of mortality in the elderly. Stroke 42, 638—644 (2011).
88.Henneman WJ, Sluimer JD, Cordonnier C et al. MRI biomarkers of vascular damageand atrophy predicting mortality in a memory clinic population. Stroke 40, 492—498(2009).
89.de Laat KF, van den Berg HA, van Norden AG, Gons RA, Olde Rikkert MG, deLeeuwFE. Microbleeds are independently related to gait disturbances in elderly individuals withcerebral small vessel disease. Stroke 42, 494—497 (2011).
90.Greenberg SM, Eng JA, Ning M, Smith EE, Rosand J. Hemorrhage burden predictsrecurrent intracerebral hemorrhage after lobar hemorrhage. Stroke 35, 1415—1420(2004).
91.Viswanathan A, Guichard JP, Gschwendtner A et al. Blood pressure and haemoglobinA1c are associated with microhaemorrhage in CADASIL: a two-centre cohort study. Brain129, 2375—2383 (2006).
92.Werring DJ, Frazer DW, Coward LJ et al. Cognitive dysfunction in patients withcerebral microbleeds on T2*-weighted gradient-echo MRI. Brain 127, 2265—2275 (2004).
93.Werring DJ, Gregoire SM, Cipolotti L. Cerebral microbleeds and vascular cognitiveimpairment. J. Neurol. Sci. 299(1—2), 131—135 (2010).
94.Seo SW, Hwa Lee B, Kim EJ et al. Clinical significance of microbleeds in subcorticalvascular dementia. Stroke 38, 1949—1951 (2007) .
95.Goos JD, Kester MI, Barkhof F et al. Patients with Alzheimer disease with multiplemicrobleeds: relation with cerebrospinal fluid biomarkers and cognition. Stroke 40, 3455—3460 (2009).
96.Yakushiji Y, Nishiyama M, Yakushiji S et al. Brain microbleeds and global cognitivefunction in adults without neurological disorder. Stroke 39, 3323—3328 (2008) .
97.Cummings JL. Frontal-subcortical circuits and human behavior. Arch. Neurol. 50,873—880 (1993).
98.Qiu C, Cotch MF, Sigurdsson S et al. Cerebral microbleeds, retinopathy, and dementia:the AGES—Reykjavik Study. Neurology 75, 2221—2228 (2010).
99.Pfeifer LA, White LR, Ross GW, Petrovitch H, Launer LJ. Cerebral amyloidangiopathy and cognitive function: the H AAS autopsy study. Neurology 58, 1629—1634(2002).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
138

100.Pathological correlates of late-onset dementia in a multicentre, community-basedpopulation in England and Wales. Neuropathology Group of the Medical Research CouncilCognitive Function and Ageing Study (MRC CFAS). Lancet 357, 169—175 (2001).
101.Keage HA, Carare RO, Friedland RP et al. Population studies of sporadic cerebralamyloid angiopathy and dementia: a systematic review. BMC Neurol. 9, 3 (2009) .
102.Greenberg SM, Gurol ME, Rosand J, Smith EE. Amyloid angiopathy-related vascularcognitive impairment. Stroke 35, 2616—2619 (2004).
103.Chabriat H, Joutel A, Dichgans M, Tournier-Lasserve E, Bousser MG. Cadasil. LancetNeurol. 8, 643—653 (2009).
104.Liem MK, Lesnik Oberstein SA, Haan J et al. MRI correlates of cognitive decline inCADASIL: a 7-year follow-up study. Neurology 72, 143—148 (2009).
105.Ryan NS, Bastos-Leite AJ, Rohrer JD et al. Cerebral microbleeds in familialAlzheimer's disease. Brain DOI: 10.1093/brain/awr126 (2011) (Epub ahead of print).
106.Moorhouse P, Rockwood K. Vascular cognitive impairment: current concepts andclinical developments. Lancet Neurol. 7, 246—255 (2008).
107.Pendlebury ST, Rothwell PM. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: a systematic review and meta-analysis. Lancet Neurol. 8,1006—1018 (2009).
108.Hennerici MG. What are the mechanisms for post-stroke dementia? Lancet Neurol. 8,973—975 (2009).
109.Gregoire S, Smith K, Sokolowsky N et al. Brain microbleeds as a risk factor forcognitive decline in stroke clinic patients: 6-year follow-up study. ABN joint annualmeeting 2009 with the Spanish Society of Neurology: J. Neurol. Neurosur. PsychiatryDOI:10.1136/jnnp.2009.191726 (2009).
110.Birns J, Morris R, Jarosz J, Markus HS, Kalra L. Hy per tension-related cognitivedecline: is the time right for intervention studies? Minerva Cardioangiol. 57, 813—830(2009).
111.Hachinski V, Iadecola C, Petersen RC et al. National Institute of NeurologicalDisorders and Stroke—Canadian Stroke Network vascular cognitive impairmentharmonization standards. Stroke 37, 2220—2241 (2006).
112.Hachinski V. Shifts in thinking about dementia. JAMA 300, 2172—2173 (2008).
113.Fotuhi M, Hachinski V, Whitehouse PJ. Changing perspectives regarding late-lifedementia. Nat. Rev. Neurol. 5, 649—658 (2009).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
139

114.Iadecola C. The overlap between neurodegenerative and vascular factors in thepathogenesis of dementia. Acta Neuropathol. 120, 287—296 (2010).
115.Smith EE, Greenberg SM. p-amyloid, blood vessels, and brain function. Stroke 40,2601—2606 (2009).
116.Skoog I, Lernfelt B, Landahl S et al. 15-year longitudinal study of blood pressure anddementia. Lancet 347, 1141—1145 (1996).
117.Fan YH, Mok VC, Lam WW, Hui AC, Wong KS. Cerebral microbleeds and whitematter changes in patients hospitalized with lacunar infarcts. J. Neurol. 251, 537—541(2004).
118.Imaizumi T, Horita Y, Hashimoto Y, Niwa J. Dotlike hemosiderin spots on T2*-weighted magnetic resonance imaging as a predictor of stroke recurrence: a prospectivestudy. J. Neurosurg. 101, 915—920 (2004).
119.Naka H, Nomura E, Takahashi T et al. Combinations of the presence or absence ofcerebral microbleeds and advanced white matter hyperintensity as predictors ofsubsequent stroke types. AJNR Am. J. Neuroradiol. 27, 830—835 (2006).
120.Soo YO, Yang SR, Lam WW et al. Risk vs benefit of anti-thrombotic therapy inischaemic stroke patients with cerebral microbleeds. J. Neurol. 255, 1679—1686 (2008).
121.Boulanger JM, Coutts SB, Eliasziw M et al. Cerebral microhemorrhages predict newdisabling or fatal strokes in patients with acute ischemic stroke or transient ischemicattack. Stroke 37, 911—914 (2006).
122.Thijs V, Lemmens R, Schoofs C et al. Microbleeds and the risk of recurrent stroke.Stroke 41, 2005—2009 (2010).
123.Jeon SB, Kang DW, Cho AH et al. Initial microbleeds at MR imaging can predictrecurrent intracerebral hemorrhage. J. Neurol. 254, 508—512 (2007).
124.Bokura H, Saika R, Yamaguchi T et al. Microbleeds are associated with subsequenthemorrhagic and ischemic stroke in healthy elderly individuals. Stroke 42(7), 1867—1871(2011).
125.Lloyd-Jones DM, Wang TJ, Leip EP et al. Lifetime risk for development of atrialfibrillation: the Framingham Heart Study. Circulation 110, 1042—1046 (2004).
126.Fang MC, Go AS, Chang Y et al. Death and disability from warfarin-associatedintracranial and extracranial hemorrhages. Am. J. Med. 120, 700—705 (2007).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
140

127.Hylek EM, Evans-Molina C, Shea C, Henault LE, Regan S. Major hemorrhage andtolerability of warfarin in the first year of therapy among elderly patients with atrialfibrillation. Circulation 115, 2689—2696 (2007).
128.Flaherty ML, Kissela B, Woo D et al. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology 68, 116—121 (2007).
129.Diener HC, Connolly SJ, Ezekowitz MD et al. Dabigatran compared with warfarin inpatients with atrial fibrillation and previous transient ischaemic attack or stroke: asubgroup analysis of the RE-LY trial. Lancet Neurol. 9, 1157—1163 (2010).
130.Rosand J, Hylek EM, O'Donnell HC, Greenberg SM. Warfarin-associated hemorrhageand cerebral amyloid angiopathy: a genetic and pathologic study. Neurology 55, 947—951(2000).
131.Gorter JW. Major bleeding during anticoagulation after cerebral ischemia: patternsand risk factors. Stroke Prevention In Reversible Ischemia Trial (SPIRIT). EuropeanAtrial Fibrillation Trial (EAFT) study groups. Neurology 53, 1319—1327 (1999).
132.Smith EE, Rosand J, Knudsen KA, Hylek EM, Greenberg SM. Leukoaraiosis isassociated with warfarin-related hemorrhage following ischemic stroke. Neurology 59,193—197 (2002).
133.Alemany M, Stenborg A, Terent A, Sonninen P, Raininko R. Coexistence ofmicrohemorrhages and acute spontaneous brain hemorrhage: correlation with signs ofmicroangiopathy and clinical data. Radiology 238, 240—247 (2006).
134.Copenhaver BR, Hsia AW, Merino JG et al. Racial differences in microbleedprevalence in primary intracerebral hemorrhage. Neurology 71, 1176—1182 (2008).
135.Fan YH, Zhang L, Lam WW, Mok VC, Wong KS. Cerebral microbleeds as a riskfactor for subsequent intracerebral hemorrhages among patients with acute ischemicstroke. Stroke 34, 2459—2462 (2003).
136.Imaizumi T, Honma T, Horita Y et al. Dotlike hemosiderin spots are associated withpast hemorrhagic strokes in patients with lacunar infarcts. J. Neuroimaging 15, 157—163(2005).
137.Jeong SW, Jung KH, Chu K, Bae HJ, Lee SH, Roh JK. Clinical and radiologicdifferences between primary intracerebral hemorrhage with and without microbleeds ongradient-echo magnetic resonance images. Arch. Neurol. 61, 905—909 (2004).
138.Lee GH, Kwon SU, Kang DW. Warfarin-induced intracerebral hemorrhage associatedwith microbleeds. J. Clin. Neurol. 4, 131—133 (2008).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
141

139.Lee SH, Bae HJ, Kwon SJ et al. Cerebral microbleeds are regionally associated withintracerebral hemorrhage. Neurology 62, 72—76 (2004).
140.Lee SH, Kim BJ, Roh JK. Silent microbleeds are associated with volume of primaryintracerebral hemorrhage. Neurology 66, 430—432 (2006).
141.Lee SH, Ryu WS, Roh JK. Cerebral microbleeds are a risk factor for warfarin-relatedintracerebral hemorrhage. Neurology 72, 171—176 (2009).
142.Naka H, Nomura E, Wakabayashi S et al. Frequency of asymptomatic microbleeds onT2*-weighted MR images of patients with recurrent stroke: association with combinationof stroke subtypes and leukoaraiosis. AJNR Am. J. Neuroradiol. 25, 714—719 (2004).
143.Nighoghossian N, Hermier M, Adeleine P et al. Old microbleeds are a potential riskfactor for cerebral bleeding after ischemic stroke: a gradient-echo T2*-weighted brainMRI study. Stroke 33, 735—742 (2002).
144.Nishikawa T, Ueba T, Kajiwara M, Miyamatsu N, Yamashita K. Cerebral microbleedsin patients with intracerebral hemorrhage are associated with previous cerebrovasculardiseases and white matter hyperintensity, but not with regular use of antiplatelet agents.Neurol. Med. Chir. (Tokyo) 49, 333—338; discussion 338—339 (2009).
145.Orken DN, Kenangil G, Uysal E, Forta H. Cerebral microbleeds in ischemic strokepatients on warfarin treatment. Stroke 40, 3638—3640 (2009).
146.Schonewille WJ, Singer MB, Atlas SW, Tuhrim S. The prevalence of microhemorrhageon gradient-echo magnetic resonance imaging in acute lacunar infarction. J. StrokeCerebrovasc. Dis. 14, 141—144 (2005).
147.Lovelock CE, Cordonnier C, Naka H et al. Antithrombotic drug use, cerebralmicrobleeds, and intracerebral hemorrhage: a systematic review of published andunpublished studies. Stroke 41, 1222—1228 (2010).
148.Haacke EM, DelProposto ZS, Chaturvedi S et al. Imaging cerebral amyloid angiopathywith susceptibility-weighted imaging. AJNR Am. J. Neuroradiol. 28, 316—317 (2007).
149.Gregoire SM, Jager HR, Yousry TA, Kallis C, Brown MM, Werring DJ. Brainmicrobleeds as a potential risk factor for antiplatelet-related intracerebral haemorrhage:hospital-based, case-control study. J. Neurol. Neurosurg. Psychiatry 81, 679—684 (2010).
150.Wong KS, Chan YL, Liu JY, Gao S, Lam WW. Asymptomatic microbleeds as a riskfactor for aspirin-associated intracerebral hemorrhages. Neurology 60, 511—513 (2003).
151.Leys D, Cordonnier C. Brain microbleeds as a potential risk factor for antiplatelet-related intracerebral haemorrhage. J. Neurol. Neurosurg. Psychiatry 81, 589—590 (2010).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
142

152.Kidwell CS, Saver JL, Villablanca JP et al. Magnetic resonance imaging detection ofmicrobleeds before thrombolysis: an emerging application. Stroke 33, 95—98 (2002).
153.Fiehler J, Albers GW, Boulanger JM et al. Bleeding Risk Analysis in Stroke ImagingBefore Thrombolysis (BRASIL): pooled analysis of T2*-weighted magnetic resonanceimaging data from 570 patients. Stroke 38, 2738—2744 (2007).
154.Lee SH, Kang BS, Kim N, Roh JK. Does microbleed predict haemorrhagictransformation after acute atherothrombotic or cardioembolic stroke? J. Neurol.Neurosurg. Psychiatry 79, 913—916 (2008).
155.Vernooij MW, van der Lugt A, Breteler MM. Risk of thrombolysis-relatedhemorrhage associated with microbleed presence. Stroke 39, E115; author reply E116(2008).
156.Lee SH, Bae HJ, Yoon BW, Kim H, Kim DE, Roh JK. Low concentration of serumtotal cholesterol is associated with multifocal signal loss lesions on gradient-echo magneticresonance imaging: analysis of risk factors for multifocal signal loss lesions. Stroke 33,2845—2849 (2002).
157.Day JS, Policeni BA, Smoker WR et al. Previous statin use is not associated with anincreased prevalence or degree of gradient-echo lesions in patients with acute ischemicstroke or transient ischemic attack. Stroke 42, 354—358 (2011).
158.Amarenco P, Bogousslavsky J, Callahan A et al. High-dose atorvastatin after stroke ortransient ischemic attack. N. Engl. J. Med. 355, 549—559 (2006).
159.Karam JG, Loney-Hutchinson L, McFarlane SI. High-dose atorvastatin after stroke ortransient ischemic attack: the Stroke Prevention by Aggressive Reduction in CholesterolLevels (SPARCL) Investigators. J. Cardiometab. Syndr. 3, 68—69 (2008).
160.Seghier ML, Kolanko MA, Leff AP, Jager HR, Gregoire SM, Werring DJ. Microbleeddetection using automated segmentation (MIDAS): a new method applicable to standardclinical MR images. PLoS One 6, E17547 (2011).
161.Dierksen GA, Skehan ME, Khan MA et al. Spatial relation between microbleeds andamyloid deposits in amyloid angiopathy. Ann. Neurol. 68, 545—548 (2010).
162.Staekenborg SS, Koedam EL, Henneman WJ et al. Progression of mild cognitiveimpairment to dementia: contribution of cerebrovascular disease compared with medialtemporal lobe atrophy. Stroke 40, 1269—1274 (2009).
163.Lesnik Oberstein SA, van den Boom R, van Buchem MA et al. Cerebral microbleeds inCADASIL. Neurology 57, 1066—1070 (2001).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
143

164.Mori N, Miki Y, Kikuta K et al. Microbleeds in moyamoya disease: susceptibility-weighted imaging versus T2*-weighted imaging at 3 Tesla. Invest. Radiol. 43, 574—579(2008).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
144

INDEX
INTRODUCTION,PATHOLOGY
MECHANISM OFCEREBRALHAEMORRHAGE
COMMON ANATOMICALSITES
CEREBRAL HAEMORRHAGE
Intracerebral haemorrhage (ICH) accounts for approximately 10-15% of strokes. Althoughits frequency is relatively low in comparison with that of atherothrombotic (20%) andembolic (25%) strokes, its importance stems from the generally severe neurological deficitsit causes and its often grave prognosis. In addition, ICH can be the result of severalmechanisms, and their identification implies important differences in management andprognosis. All these features make ICH a challenge to the clinician involved in the care ofthese patients.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
145

MECHANISMS & AETIOLOGY OF CEREBRAL HAEMORRHAGE
ICH has traditionally been considered to be primarily related to chronic hypertension. Thisnotion is based on the high frequency (89%) of history of hypertension in patients withICH, along with a high incidence of left ventricular hypertrophy at autopsy. As defined inthis manner, the hypertensive mechanism accounts for approximately 47-66% of ICHS,depending to some extent on the topography of the ICH, the highest frequency ofhypertensive mechanism occurring in the pontine variety. Lobar ICH, on the other hand,has been found to have the lowest frequency of hypertension.
The sources of arterial bleeding in hypertensive ICH are primarily located in the deepportions of the cerebral hemispheres and, to a lesser extent, in the cerebellum andbrainstem. This causes haemorrhages that are most frequently located in the deep graynuclei of the hemispheres (basal ganglia, thalamus) and in the subcortical white matter ofthe cerebral lobes. These locations correlate with the distribution in the brain of thehypertension-related arterial lesions that are thought to be the cause of ICH. These includelipohyelinosis and microaneurysms, lesions that often coexist in a given pathologicalspecimen, and which have their highest concentration in the deep hemispheric areas and inthe gray/white matter interface of the cerebral lobes, explaining the sites of predilection ofICH. Other, not primarily hypertensive, mechanisms are often documented as the cause ofICH. see table 1
Table 1. Non-hypertensive causes of intracerebral haemorrhage.
Cerebral hg
Cerebral hg
Cerebral hg
Cerebral hg
Cerebral amyloid angiopathy Vascular malformations Intracranial tumours Anticoagulants Thrombolytic agents Sympathomimetic drugs Vasculitis
Cerebral amyloid angiopathy
Cerebral amyloid angiopathy (CAA), also known as congophilic angiopathy, affectsexclusively the cerebral vasculature, without involvement of other areas of the body. Theamyloid substance is deposited in the media and adventitia of small and medium diameterarteries, as well as in veins, of the cortical surface and leptomeninges. The histologicaldiagnosis is made by showing areas of the vessel wall that stain with Congo red and show acharacteristic apple green birefringence under polarized light.
CAA characteristically affects the elderly, with a linear increase in frequency with age. Inroutine autopsy studies, the frequency of CAA has been 5-13% in those patients aged 60-69, 20-40% in patients aged 70-79, 35-45% in patients aged 80-89, and 45-58% inindividuals older than 90 years of age. The main clinical manifestation of CAA is ICH, but
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
146

an association with Alzheimer's disease and with a leukoencephalopathy are now wellrecognized as well.
Figure 1. Lobar hemorrhage due to amyloid angiopathy, B Microscopic section of the braincortex, section has been stained with Congo Red for amyloid viewed with polarized light.The section shows relatively preserved cortical neurons and the blood vessels showsbirefringence with polarized light. In some areas the walls of the blood vessels are yellow-green (arrow). Diagnosis: Amyloid angiopathy, also known as congophilic angiopathy.
The ICHs that occur in the setting of CAA have several characteristic features. Theseinclude:
CCA
CCA
CCA
CCA
A lobar location, due to the cortical and leptomeningeal distributionof the angiopathy.
A frequently irregular, variegated appearance on a computedtomography (CT) scan, which results from extension of thesuperficially-located haemorrhage into the adjacent subarachnoidspace.
A tendency to be recurrent, on occasion with multiple episodes oflobar ICH over periods of months or years, a feature that isexceptionally rare in ICH due to hypertension.
The occasional presence of multiple simultaneous haemorrhages, isalso a distinct rarity in ICH of hypertensive mechanism.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
147

Figure 2. Precontrast CT scan showing irregular variegated putameno-capsularhaemorrhage [left two images] and a lobar subcortical haemorrhage [right]
The ICH in patients with CAA can occasionally be related to preceding head trauma or aneurosurgical procedure, raising the possibility that mechanically-induced vascularrupture may be at times involved in its pathogenesis. Similarly, the use of anticoagulantand fibrinolytic agents is being increasingly suspected as a potential risk factor in instancesof ICH in the elderly, presumed to harbour CAA as a local vascular lesion predisposing toICH.
The actual mechanism of bleeding in CAA has not been elucidated. A factor that may berelated to bleeding is the association of this angiopathy with other vascular changes,notably fibrinoid necrosis. Such vascular lesion has been found with high frequency (71%)in instances of CAA associated with ICH, while it is not present in patients with CAA butwithout ICH. These data suggest that despite the high prevalence of CAA in the elderly, therelatively low frequency of ICH may be explained by the need to have the associatedchanges of fibrinoid necrosis in the affected vessels, in order to result in rupture and ICH.
Figure 3. Precontrast CT scan showing lobar subcorticalhaemorrhage
CA with ICH is a sporadic condition, but two rare familial forms have been described onlyin specific geographical locations in Iceland and in Holland. The latter form of familialCAA with ICH has been characterized as a biochemical abnormality in the precursorprotein of amyloid, which is also present in Alzheimer's disease and Down's syndrome.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
148

Figure 4. Precontrast CT scan showingsimultaneous cerebral and cerebellarhaemorrhage in a single patient
Other associations of CAA include Alzheimer's disease and a leukoencephalopathy. Thehistological features of Alzheimer's disease are present in approximately 40% of patientswith CAA-related ICH, and 30-40% of patients with CAA have clinical features ofdementia. The leukoencephalopathy of CAA affects the white matter of the cerebralhemispheres, with preservation of the 'U' fibres, corpus callosum, internal capsule, opticradiation, and white matter of the temporal lobes. The imaging diagnosis of thisleukoencephalopathy is greatly facilitated by the use of magnetic resonance imaging (MRI),which shows hyperintensity of the white matter in T2-weighted sequences.
Vascular malformations
These are a common cause of ICH in non-hypertensive patients, especially in the youngadult. These lesions include the arteriovenous malformations (AVMs), cavernous angiomas,capillary telangiectasias, and venous angiomas. Of these, only the first two carry asignificant risk of bleeding, especially AVMS.
Vascular malformations account for approximately 4.5% of ICHs in autopsy series, buttheir frequency in clinical series is higher, as they are frequently non-fatal. A rupturedAVM is the main cause of ICH in individuals younger than 45 years of age, a group inwhich this mechanism may account for as many as 40% of haemorrhages that have theirmechanism documented.
The ICHs due to ruptured AVMS, are at times caused by malformations that are too smallto be detected by cerebral angiography. In addition, those due to cavernous angiomascannot be documented angiographically due to the low flow of blood within the smallmalformation. Due to these facts, these small malformations (AVMs or cavernousangiomas) that are invisible to angiography, were once labeled as cryptic, their diagnosisdepending exclusively on pathological documentation, either at autopsy or after biopsy ofthe wall of a haematoma that had been drained surgically. However, this term has becomeobsolete since the introduction of CT and especially MRI, as these malformations, rupturedor unruptured, can now be readily demonstrated by their characteristic aspect.
AVMs appear as tangles of blood vessels shown as flow voids in TI -weighted sequences,often with a prominent adjacent draining vein, whereas cavernous angiomas are
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
149

characterized, in T2-weighted sequences, by a mixed (i.e. bright and low) signal center witha surrounding low-signal ring of haemosiderin, indicative of prior bleeding at theperiphery of the malformation. On CT, both malformations can show areas of calcification,and post-contrast enhancement is characteristic in AVMs but is not generally seen in thelow-flow cavernous angiomas.
Cavernous angiomas probably have a lower tendency to bleeding, in comparison withAVMS. However, their presence should be sought in patients with otherwise unexplainedICH, especially in the young adult. Cavernous angiomas represent 5-13% of the vascularmalformations in the central nervous system, and occur with equal frequency in males andfemales. Their diagnosis is generally made in patients in their 20s and 30s. Their location ispredominantly supratentorial (60-75%), favouring the temporal over the other cerebrallobes, whereas the infratentorial ones (25-40%) favour the pons over the cerebellum. Mostmalformations are single (70-90%), but occasional examples of multiple malformationsoccur, in which case familial incidence is likely. Their clinical presentation is with seizures(in 25-70% of the cases, in the supratentorial compartment), haemorrhage (10-30%), or aprogressive neurological deficit (35%), the latter occurring more often in infratentorialthan supratentorial cavernous angiomas. In cases with gradual progression of symptoms,which are probably due to repeated episodes of small haemorrhage at the periphery of themalformation, the usual diagnoses have been brainstem glioma or multiple sclerosis.
Figure 5. A, Single axial non–contrast-enhanced CT image demonstrates alarge heterogeneous-appearing lesion in the right frontal region thatprimarily is hyperdense centrally with a more diffuse area of increaseddensity peripherally resulting from calcification and small areas ofhemorrhage. B, Non–contrast-enhanced axial CT image demonstratesfindings of a large primarily hyperdense mass in the left occipital region.Note the relative lack of mass effect on the surrounding parenchyma onboth CT images. C, T1-weighted axial MRI image at a slightly differentslice angle from the CT scan demonstrates both cavernomas on the sameimage. These two heterogeneous masses have a reticulated core of highand low signal intensities surrounded by a hypointense rim ofhemosiderin. D, Gradient-echo axial MRI image demonstrates increasedconspicuity of both lesions. The hemosiderin rim demonstrates a bloomingartifact as a result of its increased magnetic susceptibility effects.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
150

Figure 6. Cavernous angioma. Images A-C demonstrate increased sensitivity of gradient-echo sequences over T1-weighted and T2-weighted images in the detection of smallerlesions. A, This T1-weighted image fails to demonstrate the multiple tiny cavernomasdemonstrated on a gradient-echo image. B, A corresponding T2-weighted axial MRI imagedoes not demonstrate well the multiple tiny cavernomas seen on a gradient-echo sequence.C, Cavernous angioma. Gradient-echo pulse MRI sequence demonstrates multiplepunctate and rounded areas of hypointensity within the periventricular and subcorticalwhite matter bilaterally. The largest lesion is seen within the periventricular frontal whitematter just anterior to the frontal horn of the left lateral ventricle near the genu of thecorpus callosum. Multiple smaller lesions are seen both anteriorly and posteriorly.
Figure 7. Cavernous angioma. A, T1-weighted MRI image demonstrates a smallhyperintense lesion in the left temporal cortex with a hypointense rim. This smaller lesionis demonstrated better and is more apparent on a T2-weighted image (see B) and on agradient-echo image (see C). B, T2-weighted image demonstrates the hypointense bloomingartifact within the lesion in the left temporal lobe, although the blooming is not nearly asmarked as seen on a gradient-echo image (see C). C, The lesion becomes obvious on thisgradient-echo image (see B). Even this relatively small temporal lobe lesion is detectedeasily on pulse sequence. Since cavernous angiomas are often multiple, a gradient-echosequence should be performed in addition to standard T1-weighted and T2-weightedsequences to carefully identify all concomitant lesions as clinically indicated.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
151

Figure 8. A, T1-weighted MRI image demonstrating a pontine cavernous angioma. Notethe slightly hypodense lesion centrally and to the right near the middle cerebellar peduncle.Given its location, a significant hemorrhage can have a clinically devastating result. Thislesion demonstrates that location, more than size, is a critical factor in predicting outcomeor sequelae of future hemorrhage. B, T2-weighted image of a pontine cavernoma. C, Minoramounts of hemosiderin can make smaller lesions evident on gradient-echo sequences, asseen in this pontine cavernoma.
Intracranial tumours
Intracerebral bleeding secondary to a brain tumour occurs in approximately 6-10% ofpatients presenting with ICH. This form of presentation of a brain tumour is characteristicof the malignant varieties, primarily glioblastoma multiforme and metastases. A benigntumour which is associated with haemorrhage relatively frequently is the pituitaryadenoma, which presents with the picture of pituitary apoplexy. Bleeding from brainmetastases is most frequently observed in instances of melanoma, choriocarcinoma, renal-cell carcinoma, and bronchogenic carcinoma.
In a patient presenting with ICH, the suspicion of an underlying tumour should besuggested by the following:
Braintumour
Braintumour
Braintumour
Braintumour
The finding of papilledema at the time of presentation with the acute ICH. An atypical location of the haemorrhage, in an area such as the corpus
callosum, which exceptionally is involved in non-tumoural haemorrhagesand, on the other hand, can occur in instances of tumours that infiltratethat structure, such as glioblastoma multiforme.
Multiple and simultaneous haemorrhages. A CT image of a ring-like hyperdensity surrounding a low density center,
as a result of bleeding from tumoural vessels at the interface between thetumour and the adjacent parenchyma.
A disproportionate amount of white matter oedema and mass effectaround an acute ICH.
Nodular post-contrast enhancement at the periphery of the ICH
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
152

Any of these features should raise the possibility of an underlying tumour, and the work-upshould proceed with MRI and, eventually, cerebral angiography. In the event of negativeresults of this test, if the diagnostic suspicion persists, consideration should be given tosurgical removal of the haematoma with biopsy of its cavity, in order to establish thediagnosis, since the treatment and prognosis of this form of ICH is different from that ofnon-tumour related ICH.
Anticoagulants
The occurrence of ICH in patients receiving oral anticoagulants is generally a seriousevent. On one hand, the risk of ICH is increased by eight to 11 fold by the chronic use ofwarfarin anticoagulation. On the other hand, this mechanism of ICH often leads to largerhaematomas than those in patients not receiving anticoagulants, a feature that correlateswith substantially higher mortality rates.
o The clinical features of ICH in patients receiving oral anticoagulants include:
Anticoagulant
Anticoagulant
Anticoagulant
Anticoagulant
A low frequency of associated bleeding elsewhere in the body. Lack of consistent association between ICH and preceding head
trauma or cerebral infarction. Larger haematoma volumes in anticoagulated patients than in non-
anticoagulated patients, as a result of more prolonged bleedingperiods.
A bad prognosis in anticoagulant-related ICHS, with mortality ratesexceeding 50-60%
Other features related to the occurrence of anticoagulant-related ICH are less consistentlyobserved, and include:
1. Duration of anticoagulation prior to onset of ICH: in some reports. mosthaemorrhages (70%) occurred within the first year of treatment, whereas in othersonly about one-third of the cases occurred within that period of time.
2. Relationship between intensity of anticoagulation and risk of ICH: in some studies.ICH was more likely with excessive prolongation of the prothrombin time, but inothers there was no clear relationship.
3. Role of hypertension in causing ICH in patients on oral anticoagulants: a strongassociation with hypertension is present.
4. Location of ICH: a relatively high frequency of cerebellar haemorrhages inanticoagulated patients has been reported in some series, but not in others.
Thrombolytic agents
Thrombolytic agents, in particular streptokinase and recombinant tissue- typeplasminogen activator (rt-PA), are widely used in the treatment of patients with acute
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
153

myocardial infarction (MI). Although the frequency of ICH is low (0.4-1.3% of treatedpatients). especially with the intravenous use of the fibrin-specific agent rt-PA, itsoccurrence is always serious and often fatal.
o The clinical and CT aspects of ICH related to the use of rt-PA in MI includethe following:
Thrombolysis
Thrombolysis
Thrombolysis
Onset soon after treatment, close to 40% of them during the rt-PAinfusion and another 25% occurring within 24 hours of onset ofinfusion in one series .
Predominantly lobar location, with rare examples of bleeding into theposterior fossa and putamen
Multiple simultaneous haemorrhages in about one-third of the cases. Mortality rate of 44-66%.
The mechanism of bleeding in the setting of rt-PA use is not clear. A potential role of theconcomitant use of intravenous heparin in the production of ICH has been suggested. TheGlobal Use of Strategies to Open Occluded Coronary Arteries as the majority of patientswith this complication have excessively prolonged activated partial thromboplastin time(APTT) ( 100 seconds) at the time of onset of the ICH. Local vascular factors with bleedingpotential, such as CAA, have been recently reported as the suspect substrate of ICH in thesetting of thrombolysis for acute MI. Other features, such as age 65 years, history ofhypertension, and previous aspirin use have been suggested as risk factors, but have notbeen clearly documented.
Sympathomimetic drugs
The use of sympathomimetic drugs has been associated with the occurrence of ICH, oftenshortly after exposure to the drug. The agents most commonly implicated include theamphetamines, phenylpropanolamine, and cocaine.
The amphetamines have been long known to promote ICH. Intravenous methamphetaminehas been the most commonly Responsible agent, and the ICH occurs within minutes to afew hours from drug exposure. The ICHs are usually lobar, but occasional examples ofbasal ganglionic haemorrhage have been reported. Their pathogenesis possibly includestransient hypertension (documented in about 50% of the reported cases), and anangiographic abnormality characterized by alternating areas of constriction and dilatationof intracranial arteries, or beading. This probably corresponds to a form of multifocalvasospasm related to the effects of the sympathomimetic agent on the arterial wall, and inonly rare occasions a true vasculitis has been histologically documented.
Phenylpropanolamine (PPA) is a sympathomimetic agent contained in more than 70 over-the-counter nasal decongestants and appetite- suppressants. Its use has been associatedwith instances of ICH and, less commonly, subarachnoid haemorrhage (SAH). Thesehaemorrhagic strokes have generally affected young adults, women more often than men,
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
154

who have had no other risk factors for intracranial haemorrhage. Acute and transienthypertension at presentation with ICH has been a feature in about one-third of the cases.The haemorrhages have occurred after 1-8 hours from the ingestion of the PPA-containingpreparations, in about 50% of the patients after first-time use of the drug. The doses ofPPA ingested have been approximately equally distributed between those recommendedfor appetite-suppression (75 mg/day) and excessive ones (100-170 mg). The radiologicalaspects of the ICHs are similar to those of amphetamine-related haemorrhages, withpredominantly lobar haematomas and angiographic beading in the majority of casesstudied. In one instance, biopsy obtained at the time of surgical drainage of an ICH showedhistological changes consistent with vasculitis. The mechanism of these haemorrhages isthought to be similar to that of amphetamine-related ICH.
Cocaine has become the most common illicit drug related to cerebrovascular complicationsin young adults. Strokes have been reported after the use of both the pure alkaloidal (freebase) form of the drug and the adulterant-containing crack. Intracranial haemorrhages,both ICH and SAH, have occurred after minutes to I hour from exposure to crack cocaine.The ICHs are both lobar and deep hemispheric (basal ganglia and thalamus), andoccasional patients have had multiple simultaneous haemorrhages.
The mechanism of ICH after cocaine use remains unknown. The angiographic beadingreported after amphetamine and PPA exposure is rarely seen in cocaine-related ICH,whereas the latter show a higher association with AVMs and aneurysms as the bleedingmechanism. This observation suggests that the acute hypertension that frequently followscocaine use may act as a precipitant of ICH in the presence of a pre-existing AVM oraneurysm. Other possible contributors to ICH after cocaine use include vasoconstrictionleading to cerebral infarction, with secondary haemorrhage after re-perfusion of ischaemicblood vessels, concomitant heavy alcohol intake and cigarette smoking as possibly additiverisk factors, and the rare observation of a true drug- induced vasculitis.
Vasculitis
Cerebral vasculitis causes cerebral infarction more often than ICH, but occasionalexamples of ICH have been reported. They have corresponded to examples ofgranulomatous angiitis of the nervous system (GANS), which is a primary cerebralvasculitis, unassociated with systemic involvement. Its course is acute or subacute, and ischaracterized by headache, progressive dementia, seizures, and episodes of cerebralinfarction. Systemic features of vasculitis, such as fever, malaise, arthralgias, myalgias,weight loss, anaemia, and elevated sedimentation rate, are absent in GANS. The diagnosisis suggested by inflammatory cerebrospinal fluid (CSF) findings, and beading in multipleintracranial arteries, at times with microaneurysm formation. A normal angiogram,however, does not exclude the diagnosis, which ultimately rests in the histologicaldemonstration of vasculitis in the leptomeninges and cerebral cortex.
The rare cases of ICH in association with GANS have generally occurred in the setting ofsubacute, progressive features of encephalopathy (headache, dementia) or myelopathy, but
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
155

occasionally ICH has been its first manifestation. The haemorrhages are isolated, rarelyrecurrent, and have a predominantly lobar location.
COMMON ANATOMICAL SITES OF CEREBRAL HAEMORRHAGE
Putamenal haemorrhage
Figure 9. Putameno-capsularhaemorrhage
This type of ICH originates in the posterior aspect of the putamen, from where it canextend into the temporal lobe, centrum semiovale, internal capsule, and ventricular system,depending on its size. Its cause is hypertension in over 60% of patients. The severity of theinitial clinical picture relates to haematoma size.
The clinical spectrum includes minimally symptomatic patients who present with puremotor hemiparesis and those who are densely hemiplegic, with a hemisensory loss, aphasia,hemianopia,and forced conjugate eye deviation to the side of the haematoma, generally inassociation with a markedly depressed level of consciousness.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
156

Figure 10. Hypertensive hemorrhage into basalganglia region (specifically: internal capsule).
Figure 11. Precontrast CT scan showingputameno-capsular haemorrhage,notice theintraventricular extension
The size of the haematoma relates directly toprognosis, and the presence of intraventricularextension of the haemorrhage is generallyindicative of poor functional and vital prognosis, asthe haematoma needs to reach a large size in orderto track across the internal capsule to gain accessinto the lateral ventricle.
Figure 12. putameno-capsular haemorrhage,noticethe intraventricular extension
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
157

Figure 13. Putameno-capsularhaemorrhage.
Caudate haemorrhage
This rare form of basal gangliahaemorrhage involves the head of thecaudate nucleus, at times extending intothe putamen, and virtually alwaysreaching the immediately adjacentfrontal horn of the lateral ventricle.
Figure 14. Caudate haemorrhage
This latter aspect often leads to the misdiagnosis of this condition as primaryintraventricular haemorrhage on CT, on account of the small intraparenchymal caudatehaematoma and the relatively more impressive amount of blood inside the ventricularsystem. This in turn is responsible for its clinical presentation with sudden onset ofheadache, vomiting, and depressed level of consciousness, with minimal or altogetherabsent focal neurological deficits, a presentation akin to that of SAH from rupturedaneurysm. When focal neurological deficits are present, they are both minimal andtransient, generally including ipsilateral Horner's syndrome and contralateral hemiparesis,reflecting extension of the haematoma inferiorly and laterally, respectively.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
158

Figure 15. Hypertensive hemorrhage intobasal ganglia with rupture into lateralventricles.
The cause of caudate ICH is often (50-60%) hypertension, but itsdifferential diagnosis should include rupture of anteriorcommunicating artery aneurysm (with upwards bleeding into theventricular system and caudate nucleus) and ruptured AVM. Theprognosis of caudate ICH is generally good, as the parenchymalhaematoma is small and the intraventricular haemorrhage isreabsorbed, at times requiring the insertion of an intraventricularcatheter for the treatment of hydrocephalus, which occurs in 75% ofpatients.
Figure 16. Caudate haemorrhage
Thalamic haemorrhage
Thalamic haemorrhage often involves the thalamus and the adjacent internal capsule,resulting in severe contralateral sensory and motor deficits. The hemisensory syndrome isoften a complete anaesthesia for all sensory modalities, and the whole hemibody is affected,including limbs, trunk, face and scalp.
Figure 17. Thalamic haemorrhage
As is the case with caudate haemorrhage, the proximity of the thalamus to the ventricularsystem results in the possibility of early extension of the haemorrhage into the third
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
159

ventricle and hydrocephalus.The clinical presentation of thalamic haemorrhage differsfrom that of putamenal haemorrhage in the prominence of the oculomotor findings thatcharacterize the former, and which correspond to the compressive effects of the thalamichaematoma on the tectum of the midbrain. These include: paresis of upward gaze, the eyesoften being deviated downward and adducted at rest (as if looking at the tip of the nose);small and unreactive pupils; conjugate horizontal eye deviation toward the affectedhemisphere or, less frequently, in the opposite direction (wrong way eye deviation); andoccasionally, ipsilateral Horner' s syndrome, skew deviation.
As in other types of ICH, the prognosis of thalamic haemorrhage is strongly dependent onthe size of the haematoma. In addition, the presence of obstructive hydrocephalus adds anelement of worse prognostic significance, but its reversal by prompt institution ofventricular drainage is at times associated with a dramatic clinical improvement, especiallyin the level of consciousness and the oculomotor abnormalities.
Figure 18. Precontrast CT scan showingintraventricular haemorrhage
Lobar haemorrhage
The clinical features of lobar ICH differ according to the cerebral lobe involved. In frontalhaemorrhages there is prominent bifrontal headache and contralateral weakness, the latterfollowing a pattern of arm or leg predominance depending on the lateral or medial locationof the haemorrhage, respectively. In large size haemorrhages, additional features ofipsilateral horizontal gaze preference and decreased level of consciousness occur. Intemporal haemorrhages, headache in front of the ear or around the eye occurs ipsilaterally,and dominant hemisphere haematomas present with fluent aphasia with poorcomprehension, prominent paraphasias, and severe anomia. In either hemisphere, acontralateral visual field defect, either hemianopic or quadrantanopic, is frequent, buthemiparesis and hemisensory loss are uncommon. Non-dominant hemisphere haematomasoften show prominent mental changes in the absence of focal neurological deficits, at timesleading to the misdiagnosis of metabolic encephalopathy or confusional state. Parietalhaemorrhages are characterized by the onset of headache in the ipsilateral temple area,prominent contralateral sensory and motor deficits, and variable occurrence of visual fielddefects. Depression of the level of consciousness correlates with haematoma size, as well aswith a more medial than lateral location of the haematoma in the parietal lobe.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
160

In occipital haemorrhages the headache is located in or around the ipsilateral eye, thepatients often complain of visual blurring, and the most consistent finding on examinationis an isolated contralateral homonymous hemianopia. On rare occasions, a syndrome ofalexia without agraphia has occurred in the setting of dominant hemisphere occipitalhaemorrhages.
Cerebellar haemorrhage
Cerebellar haemorrhage has a characteristic onset with abrupt vertigo, headache,vomiting, and an inability to stand and walk, in the absence of hemiparesis or hemiplegia.These features reflect bleeding in the area of the dentate nucleus of the cerebellarhemisphere, with involvement of ipsilateral cerebellar output tracts, along with thepotential for mass effect on the adjacent tegmentum of the pons. The clinical findings thatsuggest the diagnosis include ipsilateral limb ataxia, horizontal gaze palsy, and facial palsy,at times with ipsilateral trigeminal sensory loss, but without limb weakness.
Figure 19. Acute cerebellar hemorrhage
Figure 20. Precontrast CT scan showing cerebellar haemorrhage
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
161

The clinical picture is less well defined in instances of midline (vermian) cerebellarhaemorrhage with extension into the fourth ventricle, when the lateralized features arelacking, and the patients present with a syndrome that is indistinguishable from primarypontine haemorrhage. On occasion, a small cerebellar haemorrhage has presented withisolated vertigo and gait instability, leading to the misdiagnosis of Meniere's disease orlabyrinthitis, Suggesting that a high index of suspicion for the diagnosis is necessary.
Figure 21. A 62-year-old female withhypertension presented with acute-onset ataxia and confusion.Noncontrast CT exam of the head [leftimage] showed a large, right cerebellarhemorrhage, which was evacuated torelieve the mass effect on the brainstemand fourth ventricle. The cerebellarhemorrhage is seen hypointense on theT2 image due to Deoxyhemoglobin[right image].
Pontine haemorrhage
This is the form of ICH with the worst prognosis, as patients generally present withfeatures that reflect bilateral destruction of the basis pontis and tegmentum. Its signsinclude coma, quadriplegia, decerebrate posturing, bilateral horizontal ophthalmoplegia,pinpoint reactive pupils, ocular bobbing, respiratory rhythm abnormalities, andhyperthermia. In less severe forms, when the haematoma is small and is located on one sideof the pontine tegmentum, a Syndrome of ipsilateral cranial nerve involvement and ataxia,with contralateral hemiparesis and hemisensory loss results.
Figure 22. Precontrast CT scan studies showing three cases with pontine haemorrhage
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
162

Figure 23. Pontine haemorrhage
Other sites of brainstem haemorrhage
Brainstem haemorrhages outside the pons are rare. Mesencephalic haemorrhage has beenreported in about a dozen patients, and has been characterized by the onset of headacheand vomiting, along with either contralateral hemiparesis or ipsilateral cerebellar ataxia,and oculomotor findings. The latter have included paralysis of upward gaze, smallunreactive pupils, and palpebral ptosis, as well as third nerve palsy in instances ofprimarily unilateral tegmental haematomas. The cause of the haemorrhage has generallybeen unknown; sometimes the mechanism was hypertension, and very occasionallyruptured AVM. Medullary haemorrhage as a primary site of bleeding is extremely rare.
Figure 24. Precontrast CT scan showing midbrain haemorrhage
It presents with sudden onset of signs of predominantly unilateral tegmental or basalmedullary involvement, including vertigo, vomiting, gait imbalance, limb ataxia, and lowercranial nerve palsies. Its clinical findings can at times be similar to those of Wallenberg'slateral medullary syndrome, with the exception of contralateral hemiparesis and ipsilateralhypoglossal nerve palsy, which reflect extension of the medullary haemorrhage ventrallyand medially, respectively.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
163

Incidence [in%] of the common anatomical sites in hypertensive intracerebralhaemorrhage
IMAGING DIAGNOSIS OF INTRACEREBRAL HAEMORRHAGE
Computed tomography
The diagnosis of acute ICH is virtually 100% reliable with non-contrast CT due to thecharacteristic mass of blood of high attenuation value, due to the presence of the globincomponent of the haemoglobin molecule. Under exceptional circumstances, patients withprofound anaemia, with a haematocrit of 20% or less have presented with an acutehaematoma which was isointense to brain on account of the low haemoglobin contents ofthe fresh haematoma. Fresh blood has an attenuation value of 55-85 Hounsfield units (HU).
As the fresh clot starts to retract after 24-48 hours from onset, there is serum extrusionaround its periphery, resulting in a ring of hypointensity that surrounds the haematoma. Inthe subacute stage, the haematoma maintains its mass effect but becomes progressively lessdense, from the periphery toward the center, until reaching isointensity with the adjacentbrain parenchyma. The infusion of intravenous contrast at this stage can demonstrate anarea of ring enhancement at the periphery of the haematoma. In the chronic stage, themass effect of the haematoma is no longer present, post-contrast enhancement hasdisappeared after about 6 weeks from onset, and the residual is a hypointense cavity, attimes in the form of a slit that can be indistinguishable from an area of old cavitatedinfarction.
As the hemorrhage evolves, different characteristic appearances can be identified on CT,depending on the age of the bleed. CT findings over time are as follows:
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
164

After 7-10 days, the high density of blood begins to decrease, starting from theperiphery of the lesion.
From 1-6 weeks, peripheral enhancement can be seen, mimicking theappearance of an abscess, possibly related to hypervascularity at the periphery ofa resolving hematoma or disruption of the blood-brain barrier.
By 2-4 months, decreased density indicates cavity formation. A residual cavityis the final stage, which is reached after complete absorption of necrotic andhemorrhagic tissue.
Magnetic resonance imaging
MRI has greatly enhanced the yield of imaging in the diagnosis of ICH. This technique notonly detects small haematomas in areas where CT is unreliable on account of bonyartifacts, such as the brainstem and cerebellum, but can also accurately date the stage ofevolution of an ICH, by imaging the various stages of evolution of the haemoglobinmolecule. This allows for the distinction of hyperacute (first few hours), acute (days, up to Iweek), early subacute (weeks), late subacute (weeks to months), and chronic (months toyears) stages of haematoma evolution, which have distinct MRI characteristics in thevarious sequences used.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
165

Table 2. The MRI biochemical stages of cerebral hematomas
Biochemical substance MRI changes
Oxyhemoglobin Oxyhemoglobin lacks unpaired electrons and thus clot signalis close to normal brain parenchyma- normal to slightlylower signal on TI-weighted images and slightly higher signalon T2-weighted images
Paramagnetic intracellulardeoxyhemoglobin.
Because the deoxyhemoglobin within intact, clotted hypoxicred blood cells does not cause T1 shortening, the hematomawill have normal to slightly lower signal on TI-weighted MRimages. The concentration of red blood cells with clot and theconcentration of fibrin cause T2 shortening, with areas ofvery low signal on T2-weighted spin echo and T2 * -weightedgradient echo images
Paramagnetic intracellularmethemoglobin.
Proton-electron dipole-dipole interactions between hydrogenatoms and the paramagnetic centers of methemoglobin willcause marked TI shortening and very high signal intensity onTI-weighted images within the periphery of the hematoma.The intracellular methemoglobin will cause T2 shorteningand very low signal on T2-weighted images.
Extracellular migration ofmethemoglobin.
MR will exhibit the persistent high signal of extracellularmethemoglobin on TI - and T2-weighted images for up to ayear. The peripheral rim of hemosiderin and ferritin hasslightly low signal on Tl- and marked low signal on T2-weighted images [201 from the susceptibility effect ofhemosiderin within macrophage lysosomes.
Clot resorption begins fromthe periphery inward, anddepending on the size of thehematoma, may vary fromone to six weeks in duration.Necrotic tissue is sloughedand cystic cavities areformed over the next 6 to 12months.
Focal atrophy is characterized by a decrease in the size ofcortical gyri, with compensatory enlargement ofcerebrospinal fluid spaces and dilatation of the adjacentventricle. Cystic cavities are surrounded by gliosis andhemosiderin scarring.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
166

Table 3. The MRI biochemical stages of cerebral hematomas
Hyperacute stage [0-12Hr]
Immediately after an intracerebral bleed, the liquefied mass in thebrain substance contains oxyhemoglobin but no paramagneticsubstances. Therefore, it looks like any other proteinaceous fluidcollection.
Acute stage [4Hr -3days]
Reduction in oxygen tension in the hematoma results in the formationof intracellular deoxyhemolobin and methemoglobin in intact redcells. These substances have a paramagnetic effect that produces T2shortening. A thin rim of increased signal surrounding the hematomaon T2-weighted images represents edema.
Subacute stage [3days-3weeks]
As red blood cells lyse, redistribution of methemoglobin into theextracellular space changes the effect of this paramagnetic substanceto one of predominantly T1 shortening. The longer T2 results from(1)a combination of red blood cell lysis (T2 shortening disappears), (2)osmotic effects that draw fluid into the hematoma, and (3) therepetition times (TR) that are in general use for T2-weightedsequences, which are not sufficiently long to eliminate T1 contrasteffects in the image.
Chronic stage[3 weeks-3months]
Phagocytic cells invade the hematoma (starting at the outer rim andworking inward), metabolizing the hemoglobin breakdown productsand storing the iron as superparamagnetic hemosiderin and ferritin.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
167

Table 4. Effect of blood products on the MRI signal
Hyperacute stage [0-12 Hr]
Oxyhemoglobin lacks unpaired electrons and thus clot signalis close to normal brain parenchyma- normalto slightly lower signal on TI-weightedimages and slightly higher signal on T2-weighted images
Acute stage [4Hr -3days]
Deoxyhemoglobinwithin intact, clottedhypoxic red blood
No effect
T2 shortening, withareas of very lowsignal on T2-weightedspin echo and T2 * -weighted gradientecho images
Early subacute stage[3days-3 weeks]
Stronglyparamagneticintracellularmethemoglobin,
TI shortening andvery high signalintensity on TI-weighted imageswithin the peripheryof the hematoma
The intracellularmethemoglobin willcause T2 shorteningand very low signalon T2-weightedimages
Late subacute stage[3days-3 weeks]
extracellularmigration ofethemoglobin
MR will exhibit the persistent high signal ofextracellular methemoglobin on TI - and T2-weighted images for up to a year
Chronic stage[3weeks-3 months]
Focal atrophy is characterized by a decrease in the size of corticalgyri, with compensatory enlargement of cerebrospinal fluid spacesand dilatation of the adjacent ventricle. Cystic cavities aresurrounded by gliosis and hemosiderin scarring.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
168

Table 5. Effect of blood products on the MRI signal
Phase Time Hemoglobin T1 T2
Hyperacute <24hours
Oxyhemoglobin(intracellular)
Iso or hypo Hyper
Acute 1-3 days Deoxyhemoglobin(intracellular)
Iso or hypo Hypo
Early subacute >3 days Methemoglobin(intracellular)
Hyper Hypo
Late subacute >7 days Methemoglobin(extracellular)
Hyper Hyper
Chronic >14 days Hemosiderin(extracellular)
Iso or hypo Hypo
References
1. New PF, Aronow S. Attenuation measurements of whole blood and blood fractions incomputed tomography. Radiology 1976;121:635-40.
2. Atlas SW, Thulbom KR. MR detection of hyperacute parenchymal hemorrhage of thebrain. Am J Neuroradiol 1998;19:1471-507.
3. Gomori JM, Grossman RI, Goldberg HI, et al. Intracranial hematomas: imaging byhigh-field MR. Radiology 1985;157:87-93.
4. Wilberger JE, Rothfus WE, Tabas J, et al. Acute tissue tear hemorrhages of the brain:computed tomography and clinicopathological correlations. Neurosurgery 1990;27:208-13.
5. Barnett HJM, Yatsu FM, Mohr JP, Stein BM, eds.: Stroke: Pathophysiology, Diagnosis,and Management. 3rd ed. Churchill Livingstone; 1998.
6. Bradley WG Jr: MR appearance of hemorrhage in the brain. Radiology 1993 Oct;189(1): 15-26.
7. Broderick JP, Brott T, Tomsick T: Intracerebral hemorrhage more than twice ascommon as subarachnoid hemorrhage. J Neurosurg 1993 Feb; 78(2): 188-91.
8. roderick JP, Brott TG, Duldner JE: Volume of intracerebral hemorrhage. A powerfuland easy-to-use predictor of 30-day mortality. Stroke 1993 Jul; 24(7): 987-93.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
169

9. Challa VR, Moody DM, Bell MA: The Charcot-Bouchard aneurysm controversy: impactof a new histologic technique. J Neuropathol Exp Neurol 1992 May; 51(3): 264-71.
10. Chan S, Kartha K, Yoon SS: Multifocal hypointense cerebral lesions on gradient-echoMR are associated with chronic hypertension. AJNR Am J Neuroradiol 1996 Nov-Dec;17(10): 1821-7.
11. Fazekas F, Kleinert R, Roob G: Histopathologic analysis of foci of signal loss ongradient-echo T2*- weighted MR images in patients with spontaneous intracerebralhemorrhage: evidence of microangiopathy-related microbleeds. AJNR Am J Neuroradiol1999 Apr; 20(4): 637-42.
12. Gokaslan ZL, Narayan RK: Intracranial Hemorrhage in the Hypertensive Patient.Neuroimaging Clinics of North America 1992; 2: 171-86.
13. Gomori JM, Grossman RI: Mechanisms responsible for the MR appearance andevolution of intracranial hemorrhage. Radiographics 1988 May; 8(3): 427-40.
14. Nelson JS, Parisi JE, Schochet SS Jr: Principles and Practise of Neuropathology.Mosby - Year Book, Inc. St. Louis, MO; 1993.
15. Robertson CS, Contant CF, Gokaslan ZL: Cerebral blood flow, arteriovenous oxygendifference, and outcome in head injured patients. J Neurol Neurosurg Psychiatry 1992 Jul;55(7): 594-603.
16. Ruscalleda J, Peiro A: Prognostic factors in intraparenchymatous hematoma withventricular hemorrhage. Neuroradiology 1986; 28(1): 34-7.
17. Spangler KM, Challa VR, Moody DM: Arteriolar tortuosity of the white matter inaging and hypertension. A microradiographic study. J Neuropathol Exp Neurol 1994 Jan;53(1): 22-6.
18. Taveras JM, Pile-Spellman J: Neuroradiology. 3rd ed. Williams & Wilkins; 1996.
19. Welch KMA, Caplan LR, Reis DJ, Weir B, Siesjo BK, eds.: Primer on CerebrovascularDiseases. Morgan Kaufmann; 1997.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
170

INDEX |
INTRODUCTION
INTRODUCTION
Cerebral amyloid angiopathy (CAA) refers to the deposition of ß-amyloid in the media andadventitia of small- and mid-sized arteries (and less frequently, veins) of the cerebral cortexand the leptomeninges. It is a component of any disorder in which amyloid is deposited inthe brain, and it is not associated with systemic amyloidosis. CAA has been recognized asone of the morphologic hallmarks of Alzheimer disease (AD), but it also is found often inthe brains of elderly patients who are neurologically healthy. While often asymptomatic,CAA can present as intracranial hemorrhage (ICH), dementia, or transient neurologicevents. ICH is the most consistent effect of CAA. Although the vast majority of cases aresporadic, 2 familial forms exist (ie, hereditary cerebral hemorrhage with amyloidosis
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
171

[HCHWA]-Dutch type and HCHWA-Icelandic type). The severity of CAA is age related;more than 50% of patients in the tenth decade of life have evidence of CAA. Increasing ageand the presence of AD are the only identified risk factors for CAA.
Deposition of amyloid damages the media and adventitia of cortical and leptomeningealvessels, leading to thickening of the basal membrane, stenosis of the vessel lumen, andfragmentation of the internal elastic lamina. This can result in fibrinoid necrosis andmicroaneurysm formation, predisposing to hemorrhage. Some evidence suggests that theamyloid is produced in the smooth muscle cells of the tunica media as a response to damageof the vessel wall (perhaps by arteriosclerosis or hypertension). Although CAA may befound more commonly in women than men at autopsy, the incidence of ICH is the same inwomen and men. Hemorrhage occurs at the same age in men and women.
The true incidence and prevalence are hard to specify, as definite CAA can be diagnosedonly at postmortem. However, estimates can be made based on autopsy series and theincidence of lobar ICH. A series of 400 autopsies found evidence of CAA in the brains of18.3% of men and 28% of women aged 40-90 years. In a series of 117 brains of patientswith confirmed AD, 83% had evidence of CAA. The prevalence of CAA increases withadvancing age; in some autopsy series it has been found in 5% of individuals in the seventhdecade but in 50% of those older than 90 years. CAA is estimated to account for up to 15%of all ICH in patients older than 60 years and up to one half of nontraumatic lobar ICH inpatients older than 70 years (approximately 15-20 cases per 100,000 people per y). CAAand CAA-related hemorrhage are particularly common in elderly individuals with AD andDown syndrome.
Conditions associated with cerebral amyloid angiopathyo Intracerebral hemorrhage
The most consistent clinical effect of CAA is lobar ICH. Lobar ICH is associated with alower mortality rate (11-32%) and a better functional outcome than hypertensive deepganglionic bleeds. Of individuals with CAA-related hemorrhage, 25-40% have arecurrence, with the highest risk in the first year. Recurrent hemorrhages can occursimultaneously or several years later. They are associated with a high mortality rate (up to40%). Patients with a previous hemorrhage are at greater risk for subsequent hemorrhagesthan those with no history. Hypertension may exacerbate the tendency to CAA-relatedhemorrhage and vice versa. Cortical petechial hemorrhage can be epileptogenic. Familialforms of CAA are associated with hemorrhage at younger ages, by the third or fourthdecade in the Icelandic form and by the sixth decade among the Dutch kindreds.
o Dementia
Cognitive impairment of Alzheimer type is a common feature of CAA. More than 40% ofpatients with ICH-related hemorrhage have some degree of dementia. In some cases, thecognitive changes can precede the ICH. The relationship between CAA and AD is close.CAA, which is present in 80-85% of patients with AD, is severe in one third to two thirds ofthese patients. CAA is the most significant microscopic abnormality in 10-15% of patients
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
172

diagnosed with AD by clinical criteria. CAA and AD coexist pathologically at rates greaterthan predicted by chance. Arterial ß-amyloid in CAA is nearly identical to senile plaque ß-amyloid. Vascular lesions can play a significant physiopathologic role and can contribute tothe development of dementia in AD. The severity of CAA is correlated with the presence ofischemic or hemorrhagic lesions in the brains of patients with AD, and CAA is associatedwith gross strokes but not with subcortical lacunae. However, a direct causal link betweenthe 2 disorders has not been established, and the association could be due to shared riskfactors such as the presence of apolipoprotein (ApoE) e4. Some patients with CAA presentwith a progressive dementia that entails rapid cognitive decline over days or weeks. Thisrapid progression could be due to the additive effects of severe vascular amyloid, corticalhemorrhages and infarctions, white matter destruction, and accumulation of neuriticplaques.
o Vasculitis
Few cases of vasculitis of various types (giant cell arteritis, rheumatoid vasculitis, primaryangiitis of the CNS) associated with CAA have been reported. No consensus exists as towhether the pathologic abnormalities are related causally or whether the appearance ofvasculitis is a reaction to CAA-induced angiopathic changes.
o Microbleeds in cerebral amyloid angiography
Cerebral microbleeds are defined radiologically as small, rounded, homogeneous,hypointense lesions on T2*-weighed gradient-recalled echo (T2*-GRE) and related MRIsequences that are sensitive to magnetic susceptibility.[11] Scharf et al. were the first toreport on small, intracerebral black dots of signal loss on T2-weighted spin-echo MRI inpatients with hypertensive cerebrovascular disease and intracerebral hemorrhage (ICH)associated with ischemic white matter disease and lacunar infarcts.[12] They called theselesions ‘hemorrhagic lacunes’, and their further characterization using T2*-GRE MRIsequences led to the current radiologic definition of ‘microbleeds’, a term coined byOffenbacher and colleagues in 1996.[13] A key feature of Cerebral microbleeds is that theyare not seen well on conventional computed tomography or MRI scans. Availablehistopathological studies suggest that Cerebral microbleeds radiological lesions are due totiny bleeds adjacent to abnormal small vessels, being mainly affected by hypertensiveangiopathy (arteriolosclerosis – usually lipohyaline degeneration related to hypertension)or cerebral amyloid angiopathy (CAA).[14]
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
173

Figure 1. A postmortem section of the brainshowing a cortical microbleed (arrow) in apatient with Alzheimer’s disease and CAA
CLINICAL PICTURE OF CEREBRAL AMYLOID ANGIOGRAPHY
History
CAA is frequently asymptomatic. However, it can present as one of severalclinicopathologic entities. The most frequent are ICH and dementia.
CAA most often comes to clinical attention because of ICH. Symptoms may rangefrom transient weakness to coma, depending on the size and location of thehemorrhage. Patients may have recurrent episodes.
o The most common symptom at onset is headache (60-70% of patients).Frontal hematomas produce bifrontal headache pain; parietal bleeds, usuallyunilateral temple pain; temporal hematomas, ipsilateral eye and ear pain;and occipital bleeds, ipsilateral eye pain.
o Vomiting (in 30-40%) tends to occur early.o Seizures occur at onset in 16-36%. Seizures are most commonly partial, with
symptoms determined by the location of the ICH. As many as half of thepatients present in status epilepticus.
o Coma at presentation has been reported in a small proportion of patients(0.4-19%). Decreased level of consciousness, which is related to the size and
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
174

location of the hematoma, results from compression of the contralateralhemisphere or brain stem or increased intracranial pressure.
Dementia may be manifested by any of several patterns of cognitive dysfunction.Some patients present with rapid progression from a normal baseline to profounddementia in a couple of years. Other patients can have a more protracted course,which is more typical of that seen in AD.
Stereotyped transient neurologic events commonly consist of focal weakness,paresthesias, or numbness. In some cases, these events may be prodromes to largerhemorrhages.
o The symptoms spread to contiguous body parts over 2-10 minutes, and theymay involve areas in several vascular territories. These events are probablydue to small cortical petechial hemorrhages that lead to focal seizures. Therate of spread is akin to that seen in migraine; some have proposed that theymay represent spreading depression of neuronal activity.
o Some patients present with transient confusion or episodes of visualmisperceptions.
Uncommon presentations of CAAo CAA can be associated with ischemic strokes; in some of these patients, a
coexistent vasculitis can be found. The causal relationship with CAA isunclear.
o CAA is found in patients with autosomal dominant dementia, spasticity, andataxia without ICH.
o CAA is reported in patients with vascular malformations, postirradiationnecrosis, spongiform encephalopathies, and dementia pugilistica.
o CAA can present as a mass lesion; this has been related to the existence of an"amyloidoma" with accumulation of amyloid in the brain parenchyma or toedema and gliosis that result from the vascular lesion.
Physical
Physical findings depend on the clinicopathological entity associated with CAA in aparticular patient.
The features of ICH depend on the location of the bleed. Strict isolation of featuresfrom each lobe frequently is not possible because of extension of hematoma to otherlobes, mass effect, and increased intracranial pressure.
o Frontal: Depending on the size and location, frontal ICH may present withany symptoms from weakness of one limb to impaired consciousness withcontralateral hemiparesis, hemisensory loss, and horizontal gaze palsy. Lefthemispheric lesions can present with aphasia, and more anterior lesions leadto an abulic state with frontal release signs.
o Parietal: Hemisensory loss, homonymous hemianopsia, hemi-inattention, andapraxia are all signs of parietal ICH.
o Temporal: Dominant hemisphere hematomas lead to aphasia andhemianopia; nondominant hemisphere hematomas produce a confusionalstate.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
175

o Occipital: Unilateral hemianopia or quadrantanopia and visualhallucinations often accompany occipital ICH.
AETIOLOGY OF CEREBRAL AMYLOID ANGIOGRAPHY
Most cases are sporadic, although genetic predispositions exist. (eg, ApoE subtypesconfer different risk profiles.)
Most cases of CAA-related ICH are spontaneous, but they may be related to vesselwall injury by atherosclerosis and hypertension. The risk of intracranial bleedingfollowing head trauma and neurosurgical procedures is increased in patients withCAA. Some evidence suggests that CAA has a role in a substantial proportion ofanticoagulant- and thrombolytic-related hemorrhages.
Hereditary forms of CAA are due to specific gene mutations. Hereditary cerebral hemorrhage with amyloidosis-Dutch type is an autosomal-
dominant disorder with complete penetrance.o The age of onset of ICH is in the sixth decade (mean, 55 y). Eighty-seven
percent of those affected have ICH, and 13% have infarcts (deep).o Some patients develop dementia without ICH.o Amyloid deposits are found in cortical and leptomeningeal vessels;
parenchymal neurofibrillary tangles are not seen. Deposited amyloid proteinin these patients is identical to the amyloid protein seen in sporadic cases,and the likely genetic defect is in the amyloid protein precursor protein(APP) gene on chromosome 21.
Hereditary cerebral hemorrhage with amyloidosis-Icelandic type is also autosomaldominant.
o Patients present with their first episode of ICH in the third or fourth decade,with some patients dying from ICH aged as young as 15 years. A recent casereport has identified a family with late-onset dementia with and withoutICH.
o The amyloid angiopathy is more widely distributed in this type than in othertypes, involving arteries in the cerebrum, cerebellum, and brain stem.
o The amyloid protein is a mutant of the cysteine protease inhibitor cystatin C. Severity of angiopathy and fibrinoid necrosis closely correlate with the occurrence
of ICH. The Boston Cerebral Amyloid Angiopathy Group has elaborated guidelines for the
diagnosis of CAA associated with ICH. Four levels of certainty in the diagnosis ofCAA are considered: definite, probable with supporting pathological evidence,probable, and possible. The first 3 require that no other cause of hemorrhage hasbeen identified; they are yet to be validated but are clinically useful.
o Definite CAA: Full postmortem examination reveals lobar, cortical, orcorticosubcortical hemorrhage and evidence of severe CAA.
o Probable CAA with supporting pathological evidence: The clinical data andpathological tissue (evacuated hematoma or cortical biopsy specimen)demonstrate a hemorrhage with the aforementioned characteristics and somedegree of vascular amyloid deposition.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
176

o Probable CAA: Clinical data and MRI findings (in the absence of apathological specimen) demonstrate multiple hematomas (as describedabove) in a patient older than 60 years.
o Possible CAA: This is considered if the patient is older than 60 years, andclinical and MRI data reveal a single lobar, cortical, or corticosubcorticalhemorrhage without another cause, multiple hemorrhages with a possiblebut not a definite cause, or some hemorrhage in an atypical location.
GENETIC OF CEREBRAL AMYLOID ANGIOGRAPHY
The severity of the angiopathy is associated with ApoE polymorphism. The ApoE e4and e2 alleles are risk factors for CAA.
o The ApoE e2 allele also confers an increased risk of ICH in patients withCAA. The ApoE e4 allele is associated with earlier onset of first hemorrhageand carries a significant risk of concomitant AD.
o Patients with lobar ICH and the e2 or e4 allele have a greater risk of earlyrecurrence.
o These tests lack sensitivity and specificity and are not indicated as screeningor diagnostic procedures. However, they may be helpful prognostic tools inidentifying patients with a greater risk of early recurrence.
In cases of CAA-related ICH, laboratory studies should rule out other possibleetiologies.
IMAGING OF CEREBRAL AMYLOID ANGIOGRAPHY
CT scan of the braino This procedure is the first choice for patients with suspected acute ICH.o A single lobar hemorrhage with superficial location and cortical involvement
with or without local extension to the subarachnoid and intraventricularspaces is suggestive of CAA-related hemorrhage. Evidence of multiplehemorrhages restricted to lobar regions may be present.
o Hemorrhages are most common in the frontal and parietal lobes, involvingthe cortex and subcortical white matter. Over time, several lobes may beinvolved. Deep central gray nuclei, the corpus callosum, and the cerebellumare sometimes affected. CAA is rarely the cause of putaminal, thalamic, orbrain stem hemorrhage.
o Pure subarachnoid, intraventricular, and subdural hemorrhages can be seenbut are rare. CAA should never be assumed to be the cause of an isolatedsubarachnoid hemorrhage unless all other causes, particularly aneurysmal,have been excluded.
o Patients with CAA-associated dementia have a leukoencephalopathy similarto that seen in Binswanger disease. Atrophy also can be detected, particularlyin patients with cognitive impairment and a history of prior hemorrhage.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
177

MRIo MRI shows evidence of multiple cortical and subcortical large and small
petechial hemorrhages, even in patients without a history that suggestsprevious hemorrhage.
o MRI gradient-echo sequences show evidence of iron deposits, whichcorrespond to old hemorrhages. In patients who present with lobarhemorrhages, the evidence of old petechial bleeds and microbleeds can helpin the diagnosis of CAA. Gradient-echo MRI also can be used as a marker ofdisease progression and potentially can evaluate the effect of therapeuticinterventions.
o Leptomeningeal enhancement is seen in patients with associated vasculitis.o Cerebral microbleeds are commonly associated with cerebral amyloid
angiopathy, Microbleeds are lobar in location in patients with cerebralamyloid angiopathy
Figure 2. Lobar microbleeds on 3-dimensional T2*-weighted gradient-recalled echo MRI in an 80 years old manwith dementia and cerebral amyloidangiopathy.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
178

Figure 3. Example ofmicrobleeds on 3-dimensional T2*-weightedgradient-recalled echo MRIin an 80 years old man withAlzheimer dementia andcerebral amyloidangiopathy. The microbleedsare lobar in location.
HISTOPATHOLOGICAL FINDING IN CEREBRAL AMYLOID ANGIOGRAPHY
Histologic examination is required for definitive diagnosis. Pathologic samples are obtainedfrom hematoma evacuation, cortical biopsy, or postmortem specimens. The disease processmay be diffuse, so pathologic data may be lacking even in biopsy cases. The presence ofvascular amyloid is a sensitive marker for CAA-related hemorrhage. ß-amyloid consists oftwisted ß-sheet fibrils in vessel wall. It is a homogenous, intensely eosinophilic material thatgives a smudged appearance by light microscopy. When stained with Congo red andvisualized under polarized light, it gives a characteristic yellow-green (ie, apple green)birefringence. When thioflavin T and S are used and visualized with ultraviolet light,amyloid appears fluorescent. The presence of fibrinoid necrosis in amyloid-laden vessels isrelatively specific for CAA-related ICH. CAA, which involves cortical and leptomeningealvessels, is most common in the parietal and occipital lobes. The microangiopathy spareswhite matter and deep gray structures. Parenchymal features found in the brains ofpatients with CAA include patchy demyelination and loss of white matter, corticalhemorrhages and infarcts, and neuritic plaques with or without neurofibrillary tangles.Most patients with CAA-related ICH do not have AD.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
179

Figure 4. Lobar hemorrhage due to amyloid angiopathy, B Microscopic section of the braincortex, section has been stained with Congo Red for amyloid viewed with polarized light.The section shows relatively preserved cortical neurons and the blood vessels showsbirefringence with polarized light. In some areas the walls of the blood vessels are yellow-green (arrow). Diagnosis: Amyloid angiopathy, also known as congophilic angiopathy.
References
1. Case records of the Massachusetts General Hospital. Weekly clinicopathologicalexercises. Case 22-1996. Cerebral hemorrhage in a 69-year-old woman receivingwarfarin [clinical conference] [published erratum appears in N Engl J Med 1996Oct 10;335(15):. N Engl J Med 1996 Jul 18; 335(3): 189-96.
2. Ellis RJ, Olichney JM, Thal LJ, et al.: Cerebral amyloid angiopathy in the brains ofpatients with Alzheimer's disease: the CERAD experience, Part XV. Neurology 1996Jun; 46(6): 1592-6.
3. Greenberg SM, Vonsattel JP, Stakes JW: The clinical spectrum of cerebral amyloidangiopathy: presentations without lobar hemorrhage. Neurology 1993 Oct; 43(10):2073-9.
4. Greenberg SM, Finklestein SP, Schaefer PW: Petechial hemorrhages accompanyinglobar hemorrhage: detection by gradient-echo MRI. Neurology 1996 Jun; 46(6):1751-4.
5. Greenberg SM: Cerebral amyloid angiopathy: prospects for clinical diagnosis andtreatment. Neurology 1998 Sep; 51(3): 690-4.
6. Hart RG, Boop BS, Anderson DC: Oral anticoagulants and intracranialhemorrhage. Facts and hypotheses. Stroke 1995 Aug; 26(8): 1471-7.
7. Izumihara A, Ishihara T, Iwamoto N: Postoperative outcome of 37 patients withlobar intracerebral hemorrhage related to cerebral amyloid angiopathy. Stroke1999 Jan; 30(1): 29-33.
8. O'Donnell HC, Rosand J, Knudsen KA: Apolipoprotein E Genotype and the Risk ofRecurrent Lobar Intracerebral Hemorrhage. N Engl J Med 2000 Jan 27; 342(4):240-245.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
180

9. Rosand J, Hylek EM, O'Donnell HC: Warfarin-associated hemorrhage and cerebralamyloid angiopathy: a genetic and pathologic study [In Process Citation]. Neurology2000 Oct 10; 55(7): 947-51.
10. Vinters HV: Cerebral amyloid angiopathy. A critical review. Stroke 1987 Mar-Apr;DA - 19870518(2): 311-24.
11. Greenberg SM, Vernooij MW, Cordonnier C et al. Cerebral microbleeds: a guide todetection and interpretation. Lancet Neurol. 8, 165—174(2009).
12. Scharf J, Brauherr E, Forsting M, Sartor K. Significance of haemorrhagic lacuneson MRI in patients with hypertensive cerebrovascular disease and intracerebralhaemorrhage. Neuroradiology 36, 504—508 (1994).
13. Offenbacher H, Fazekas F, Schmidt R,Koch M, Fazekas G, Kapeller P. MR ofcerebral abnormalities concomitant with primary intracerebral hematomas. AJNRAm. J. Neuroradiol. 17, 573—578 (1996).
14. Fazekas F, Kleinert R, Roob G et al.Histopathologic analysis of foci of signal loss ongradient-echo T2*-weighted MR images in patients with spontaneous intracerebralhemorrhage: evidence of microangiopathy-related microbleeds. AJNR Am. J.Neuroradiol. 20, 637—642 (1999).
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
181

INDEX
INTRODUCTION &PATHOGENESIS
NEUROIMAGINGCORRELATION OFSTRUCTURAL PATHOLOGYOF MICROVASCULAR BRAINDISEASE
o Central and corticalatrophy
o Leukoaraiosis
o Lacunar infarctions
o Granular atrophy(Cortical laminarnecrosis)
o Basal ganglioniccalcifications
o Dilated Virchow-Robinspaces (VRSs)
o Cerebral microbleeds
VERTEBROBASILARECTASIA (FUSIFORMANEURYSM)
SUMMARY
INTRODUCTION & PATHOGENESIS :
Microcirculatory brain disease is a collective terminology that comprises vasculararteriolar pathology, metabolic endocrinal abnormalities and haemorheologicalabnormalities. Clinically it is characterized by the existence of cerebral ischaemic eventsthat have a peculiar tendency for recurrence and progression to multi-infarct dementia.These ischaemic events are commonly associated with increased incidence of depression,
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
182

parkinsonian manifestations, essential hypertension and blood hyperviscosity. Theassociates of the microvascular brain disease are collectively called the metabolicsyndrome. (See table 1). Microvascular brain disease is occasionally associated with aspecial subtype of large vessel disease called arterial ectasia or fusiform aneurysm of thevertebrobasilar system. 140
Table 1. Microvascular brain disease associates (the metabolic syndrome)
Microvascular associate Description
Clinical picture Stroke, TIAs, multi-infarct dementia, essentialhypertension, depression, parkinsonism
Metabolic, endocrinal changes Type VI hyperlipidaemia (Hypertriglyceridemia),hyperuricemia, type 2 diabetes, Insuline resistance,truncal obesity (The metabolic syndrome)
Vascular pathology Lipohyalinosis, astrogliosis and interstitial edema, etc
Haemorheological changesIncreased whole blood viscosity and hypercoagulabilitycharacterized by an increased plasminogen activatorinhibitor-1 (PAI-1) level.
The endocrinal and metabolic abnormalities characteristic of the microvascular braindisease include non-insulin dependent diabetes mellitus, Type IV hyperlipidaemia(increased triglyceride and reduced HDL), truncal obesity and hyperuricemia (Themetabolic syndrome).
Although the association between parkinsonian manifestations (vascular parkinsonism)and microvascular brain disease can be attributed to the pathologic findings of multiplebasal ganglia cavitations (etat crible) and infarcts (etat lacunaris) that are encountered inthe ischemic microvascular brain disease, however a link between the idiopathic parkinsondisease and type 2 diabetes was demonstrated by Hu, et al, [122]. Hu, G, et al, 122 foundthat individuals who developed type 2 diabetes have an 83% increased risk for PDcompared with the general population. The mechanism of the association between type 2diabetes and PD is, however, poorly understood. Insulin might play a role in the regulationof central dopaminergic transmission. 122 According to the study of Hu, et al, 122 Theassociation between type 2 diabetes and PD is independent of sex, smoking, alcohol andcoffee intake, and body weight. The demonstrated link between the idiopathic parkinsondisease and type 2 diabetes could result in increased incidence of the idiopathic parkinsondisease in the microvascular brain disease that is independent of any structural ischemiccerebral pathology.
Microvascular brain disease and Alzheimer disease (AD)
There seems to be a complex interrelationship between Alzheimer disease (AD) andcerebrovascular disease that extends beyond the coexistence of these 2 disease processes.Imaging features of small vessel disease are seen at higher frequency in Alzheimer's disease(AD) than in healthy controls. Cerebrovascular disease and Alzheimer disease (AD) often
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
183

coexist, whereas stroke often exacerbates preexisting, sometimes previously subclinical,disease. Furthermore, Alzheimer disease (AD), Vascular dementia and microvascular braindisease share common risk factors, such as diabetes and hypertension, as well as geneticfactors for brain tissue vulnerability (presenilins, amyloid precursor protein, APOE genes).158
Insuline resistance, the metabolic syndrome and the ischemic microvascular braindisease
The mechanisms that are responsible for the insulin resistance syndromes (IRS) includegenetic or primary target cell defects, autoantibodies to insulin, and accelerated insulindegradation. Obesity, the most common cause of insulin resistance, is associated with adecreased number of receptors and postreceptor failure to activate the tyrosine kinase.Insulin resistance plays a major pathogenic role in the development of the metabolicsyndrome that may include any or all of the following: hyperinsulinemia; type 2 diabetes orglucose intolerance; central obesity; hypertension; dyslipidemia that includes hightriglycerides (TG); low high-density lipoprotein cholesterol (HDL-C) and small, dense low-density lipoprotein (LDL) particles; and hypercoagulability characterized by an increasedplasminogen activator inhibitor-1 (PAI-1) level.
Figure 1. Diabetes,hyperlipidaemia, truncalobesity depression,parkinson disease,hyperuricaemiahypertension, etc all stemfrom one and the same root(the genetic root)
THE ISCHEMIC MICROVASCULAR BRAIN DISEASE
As a point of departure a quick over view on the cerebral microcirculation will be given.Two microvascular systems were described. The centrifugal subependymal system and thecentripetal pial system. The centrifugal subependymal microvascular system originatesfrom the subependymal arteries which are terminal branches of the choroidal arteries,then extends centrifugally outward into the periventricular gray matter (Basal ganglia andthalamus) and the immediate periventricular white matter.
The centripetal pial vascular system originate from the pial arteries then extendscentripetally inwards towards the ventricular system. This system supply the cortical gray
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
184

matter and the immediate subcortical white matter. Accordingly the microcirculation isheavily concentrated in the cortical and the immediate periventricular regions.
Figure 2. The cerebral microcirculation
The microvascular pathology includes initially vascular smooth muscle cell (VSMC)proliferation associated with increased sensitivity of the VSMCs resulting in increasedcontractibility of the microvascular smooth muscle cells. This is reflected in increasedtendency of the fine penetrating intracerebral arterioles for vasospasm. At an advancedstage microvascular remodelling occurs resulting in VSMCs degeneration coupled withexcessive deposition of the ground substance (collagen fibres and Lipohyaline material) inthe arteriolar walls resulting in what is termed pathologically lipohyalinosis. VSMCsdegeneration coupled with lipohyalinosis ultimately result in loss of the physiologicalautoregulatory process.
Figure 3. Lipohyalinosis is seen in the smallerpenetrating arteries (<200 micrometers indiameter) and occurs almost exclusively in patientswith hypertension. It has features of both atheromaformation and fibrinoid necrosis with lipid andeosinophilic fibrinoid deposition in the media.
The haemorheological changes associated with microvascular brain disease includeincrease in the whole blood viscosity and thrombotic tendency of the blood. In general asignificant increase of blood, plasma and serum viscosity and a decrease of whole bloodfilterability are observed in the metabolic syndrome, and this significantly impair flow inthe microcirculation and contribute to the development of the ischemic microvascularbrain disease. 118,119,120,121
A negative relationship is observed between directly measured whole-blood viscosity andinsulin sensitivity as a part of the insulin-resistance syndrome (The metabolic syndrome),and a positive relationship is observed between insulin resistance and whole blood viscosity.In general, obesity and insulin resistance both impair blood rheology by acting on red cell
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
185

rigidity and plasma viscosity. Whole blood viscosity reflects rather obesity than insulinresistance. 118,119,120,121
Whole blood viscosity is a collective terminology that include blood viscosityand plasma viscosity. Blood viscosity is determined by the haematocrit valueand plasma viscosity is determined by serum fibrinogen. Increase of thehaematocrit value and serum fibrinogen - even within the normal range -increases the whole blood viscosity. Increase of the platelet aggregation alsoincreases whole blood viscosity.
Figure 4. PLATELETS AGGREGATION
Reduced RBCs deformability and increased RBCs aggregability also increase whole bloodviscosity. Normally the RBCs must be deformed (they usually become parachuted) in orderto pass through the microcirculation. Reduction of the RBCs deformability results in poorRBCs flow through the microcirculation and subsequently poor tissue oxygenation.
Figure 5. RBCsdeformability [left] andrigidity [right]
It should also be noted that increased fibrinogen level, especially when associated withincrease of the RBCs and platelet aggregability, reflects a hypercoagulable state thatselectively affects the microcirculation of the brain. Microvascular occlusion can occureither by Local aggregation of hyperaggragable platelets or by red cell aggregation withimpaction of rigid red cell in the microcirculation.
Increase of the blood viscosity results in global reduction of brain perfusion, however, thisis normally compensated for by the physiological process of autoregulation. In response tocritical reduction of brain perfusion, the brain microvascular bed dilates thus increasingbrain perfusion. Normally the autoregulatory process keeps the brain perfusion at aconstant level despite the normal daily fluctuation of the whole blood viscosity.
Loss of the autoregulatory physiological process, secondary to microvascular arteriolarpathology, will simply mean that brain perfusion will fluctuate with fluctuation of thewhole blood viscosity. The micro vascular brain disease is the end result of a vicious circlethat starts at one end of the circle with loss of the autoregulatory process and restarts at theother end of the circle by increase of the whole blood viscosity. This vicious circle shouldmean that in microcirculatory brain disease there is critical and chronic reduction of wholebrain perfusion that is interrupted by frequent microvascular thrombo-occlusive episodesof sudden onset and regressive course. These episodes are secondary to the
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
186

hypercoagulable state and increased thrombotic tendency of the blood. The metabolicsyndrome, which is commonly associated with the microvascular brain disease, are socommonly associated with increased blood viscosity to the point that it can be called theblood hyperviscosity syndrome.
In general hypertension, an elevated hematocrit value above 45, increased fibrinogen level,old age, cigarette smoking and the metabolic syndrome are significantly linked with silentand symptomatic lacunar infarctions and the microvascular brain disease. Cigarettesmoking is significantly linked with the metabolic syndrome (The insulin resistancesyndrome). Smoking increases insulin resistance and is associated with central fataccumulation.
CEREBRAL PARENCHYMAL CONSEQUENCES OF MICROVASCULAR BRAINDISEASE
Central and cortical atrophy
This is secondary to chronic global reduction of brain perfusion.
Figure 6. Central andcortical atrophy secondaryto chronic global reductionof brain perfusion, Noticethe associated lacunarinfarctions
Leukoaraiosis
Leukoaraiosis is an ischaemic demyelination of the immediate periventricular white matterassociated with astrogliosis, enlarged extracellular spaces and white mattermicrocavitations. It is secondary to chronic global reduction of brain perfusion.Leukoaraiosis, which appears as an area of hyperintense signal in the white matter on MRimages, is an age-related neurodegenerative condition that, when severe, correlates withdementia. It is characterized histologically by demyelination, loss of glial cells, andspongiosis. The pathogenesis of leukoaraiosis is not yet established, but it is thought to berelated to ischemia. Periventricular venous collagenosis, thickening of the vessel wall bymultiple layers of collagen, has been reported to occur in aging brains and to be moresevere in brains with leukoaraiosis. In postcapillary venules and small veins, the stenosis
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
187

that results from severe periventricular venous collagenosis may be one contributing factorin chronic localized ischemia, with consequent cell injury and death.
Figure 7. A, Central and cortical atrophy, notice the associated leukoaraiosis and lacunarinfarctions, more on the left side. B, leukoaraiosis. The CT scan periventricularhypodensities are mainly due to astrogliosis and interstitial edema.
o Histopathology of leukoaraiosis
Postmortem studies reveal that leukoaraiosis can be due to a heterogenous assortment oftissue changes that differ in histopathologic severity. In most cases, periventricularleukoaraiosis consists of variable degrees of axonal loss, demyelination, astrocytosis, andfinely porous, spongy, or microcystic changes in the neuropil. 34,79,96 These changes arefrequently associated with arteriosclerotic vasculopathy and, in more severe cases, withfrank lacunae infarction. 54 On MR imaging the mild degree of leukoaraiosis almostalways present adjacent to the angles of the frontal horns is usually due to focal gaps in theependymal epithelium with mild underlying gliosis. 86 This change, known as ependymitisgranularis, increases in frequency with age and is believed to be due to the wear and teareffects of ventricular CSF pulsations on an ependymal lining incapable of self-repair. 82leukoaraiosis may also be related to histologic characteristics of the normal frontal hornsubependymal region (fasiculus subcallosus) where finely textured fibers may havedifferent T2-relaxation properties than the deeper white matters.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
188

Figure 8. Etat cribe seen in acognitively and neurologicallynormal 81-year- old woman. Fastspin echo: A, Proton densityimage. B, Second echo: dilatedperivascular spaces permeate thebasal ganglia bilaterally.
Subcortical regions of leukoaraiosis seen on MR imaging share many of the histologicfeatures characteristic of the periventricular pattern. Pathologic correlation studies basedon postmortem MR image scanning have demonstrated reduced axonal andoligodendroglial density, astrocytosis, pallor on myelin staining, diffuse neuropilvacuolation, and hyalinotic arteriolar thickening 74,91. In some cases, these diffuse changesare found to surround variably sized foci of cystic infarction. 12, 13, 66 Subcorticalleukoaraiosis, particularly when highly circumscribed or punctate, can often be explainedby dilated Virchow-Robin spaces surrounding ectatic and sclerotic arterioles. 43,55 Suchchanges may occur in 40% of patients with hypertension, 92 and, when severe, correspondsto the phenomenon of etat crible originally described by Durand-Fardel in 1843. 24
Figure 9. Neurologically normal patient with leukoaraiosisaffecting the basis pontis and tegmentum.
Rarely, patients with extensive leukoaraiosis can be diagnosed as having Binswanger'sdisease. This condition, sometimes referred to as lacunar dementia, etat lacunaire, orsubcortical arteriosclerotic encephalopathy, 75 is characterized pathologically by extensiveathero and arteriosclerosis, multiple foci of white matter infarction, diffuse white matterdemyelination with sparing of the subcortical "U" fibers, and variable evidence for cortical
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
189

infarction. 5,75 These white matter changes are more destructive than those of typicalleukoaraiosis and are clinically associated with combinations of hemiparesis, gaitdysfunction, spasticity, Parkinsonism, dysarthria, incontinence, pseudobulbar palsy, anddementia. These abnormalities generally accumulate over months or years in a nonuniformand sometimes stroke-like fashion. 6, 19, 22, 39, 51, 88 There is a tendency for patients tobe hypertensive but exceptions have been described. 19, 22, 39
Figure 10. Radiographic/histopathologic correlation for a case of diffuse and extensiveperiventricular LE occurring in an 86-year-old patient. A, Antemortem coronal MR imageof left occipital lobe. Note extensive white matter hyperintensity adjacent and superior tothe occipital horn of the lateral ventricle sparing the subcortical arcuate fibers. B,Postmortem coronal MR image of left occipital lobe. Note topographically coextensivewhite matter changes compared with A. C, Bielschowsky-stained postmortem specimen(2X) corresponding to A and B. D, Photomicrograph (hematoxylin-eosin, originalmagnification x 140) from involved white matter demonstrating perivascular parenchymalrarefaction and macrophage infiltration. E, Photomicrograph (GFAP, originalmagnification x 660) from involved white matter demonstrating reactive astrocytes. Noregions of cystic (lacunar) infarction could be identified in this case.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
190

Figure 11. Postmortem specimen.Note the topographicallyextensive periventricular whitematter changes in a hypertensivecase with evidence ofleukoaraiosis on MRI study
In contrast to the severe and necrotizing changes of Binswanger's disease, it is apparentthat the histology underlying most other forms of leukoaraiosis is far less destructive. Thisobservation may explain why individuals with radiographically widespread leukoaraiosisare often unimpaired. In MS, extensive demyelinative plaques with relative axonalpreservation can frequently evolve silently while affecting even neurofunctionally criticalregions such as the brain stem and thoracic spinal cord. 37, 38,50, 64, 72 Given thepathology associated with these clinically silent lesions, the dilated perivascular spaces,isomorphic gliosis and low-grade demyelination of leukoaraiosis might be also expected tohave limited clinical consequences.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
191

Figure 12. leukoaraiosis, MRI T2 image. The MRI T2 periventricular hyperintensities aremainly due to astrogliosis and interstitial edema.
o Pathophysiology of leukoaraiosis
Several pathophysiologic mechanisms have been proposed to explain the histology ofleukoaraiosis. In addition to ependymitis granularis and Virchow-Robin space dilatation,more extensive regions of leukoaraiosis have been attributed to the ischemic effects ofchronic oligemia and to perivascular edema and retrograde axonal degeneration.
Chronic hypoperfusion
In the severe (Binswanger's disease) form of leukoaraiosis, chronic microvascular oligemiaand intermittent thrombotic occlusion appear responsible for the observed pattern ofmultiple lacunar infarcts with interspersed areas of edema, demyelination, and gliosis.Unlike the richly collateralized cerebral cortex, the leukoaraiosis vulnerable white matter isperfused by long penetrating corticofugal endarteries with few side branches, a vasculararchitecture that provides little protection from the ischemic effects of microvascularstenosis. 22, 80
The extent to which the more common and histologically milder forms of leukoaraiosis canalso be explained by ischemic mechanisms is currently unclear. The term "incompletewhite matter infarction" has been proposed to designate regions of mild demyelination,oligodendroglial loss, astrocytosis, and axonal rarefaction that occur in proximity to cysticinfarcts or in association with arteriolar hyaline vasculopathy. 26 These changes, whichcharacterize most forms of diffuse leukoaraiosis and can be seen in association with thecystic lacunes of Binswanger's disease, may represent the long-term consequences ofchronic hypoperfusion due to senescence and hypertension-related microvascular stenosis.
Direct evidence for hypoperfusion as an explanation of leukoaraiosis pathogenesis isconflicting. Several studies have demonstrated diminished cerebral blood flow (CBF) in
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
192

white matter regions affected by leukoaraiosis, 30, 51, 18 but it is unclear whether suchhypoperfusion is itself causative or occurs as a secondary response to reduced metabolicactivity of the leukoaraiosis tissue. Using, 18 F fluoromethane positron emissiontomography (PET), one study revealed that while severe leukoaraiosis regions wereassociated with ipsilateral cortical hypoperfusion, the hypoperfused regions typicallyspared the anterior and posterior cortical watershed territories. 45 The authors use thisfinding to argue that the blood flow reductions seen in leukoaraiosis cases result from thelower metabolic demands of cortex rendered electrophysiologically isolated by subjacentzones of disrupted white matter tissue. The implication is that chronically inadequatehemispheric perfusion may not play a role in leukoaraiosis pathogenesis. While thisinterpretation gains support from the observation that hemodynamically significantextracranial carotid stenosis does not correlate with the presence of ipsilateralleukoaraiosis, 30 others have seen leukoaraiosis to progress in concert with a severelystenosed ipsilateral carotid that advanced to complete occlusion. 95 In a more recent study,an increased oxygen extraction fraction (OEF) for white matter was found in fournondemented subjects with severe leukoaraiosis. 94 If replicated, this result would supportchronic hypoperfusion as an etiologic mechanism by revealing leukoaraiosis lesions toexperience a metabolic demand out of proportion to the local CBF.
Fluid accumulation and edema
The subependymal accumulation of interstitial fluid has been proposed as an alternativeexplanation for leukoaraiosis. 16, 97 Approximately 10% to 20% of CSF may be producedintraparenchymally and transependymally absorbed 47, 78, 81 into the lateral ventricles.Such a drain age pattern might increase the water content of the periventricular region andresult in leukoaraiosis, particularly if exacerbated by the effects of age-related ependymaldegeneration (ependymitis granularis).
Feigin and Budzilovich, 3l,32 observed leukoaraiosis- like white matter changes includingdemyelination, hyalinized microvessels, cystic necrosis, and astrocytosis in the edematousregions surrounding intracerebral tumors. These authors proposed that Binswanger'sdisease might result from a self-reinforcing cycle of tissue destruction where chronichypertension combined with episodes of local hypoxia and acidosis contribute to theformation of extracellular edema. The edema would then trigger cytotoxicity, gliosis, anddemyelination and potentiate the degenerative microvascular changes. Based on this model,others have suggested that exudation of serum proteins from arterioles made leaky fromthe effects of hypertensive vasculopathy might explain the milder white matter changes ofsubcortical leukoaraiosis. 74
Axonal degeneration
Ischemic axonopathy may also account for leukoaraiosis. Ball, 7 described the presence ofleukoaraiosis with cortical layer III laminar necrosis in the postmortem brains of fourelderly patients who experienced episodic systemic hypotension during life. Because theleukoaraiosis regions consisted of rarefied white matter without necrosis or microvascularsclerosis, this author proposed that distal axonopathy secondary to cortical neuronal
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
193

ischemia was the underlying process. Supporting the hypothesis that retrogradedegenerative white matter changes can account for at least some leukoaraiosis lesions is thefinding of MR image hyperintensities within pyramidal tract locations distal and ipsilateralto internal capsule infarcts. 76
o Neuroimaging of leukoaraiosis
Radiographic LA has been correlated with a variety of neuropathological findings.Punctuate hyperintensities are caused by perivascular demyelination and gliosis, dilatedVirchow-Robin spaces, or small lacunae. Diffuse or extensive LA consists of areas of loss ofaxons and glial cells, predominantly oligodendrocytes, and myelin rarefaction (sparing theU fibers) accompanied by spongiosis. 106, 107 Multiple lacunae and multiple sclerosisplaques have also been found in areas of radiological LA. Periventricular rims, thin caps,and halos correlate with subependymal glial accumulation associated with loss of theependymal lining. The consensus is that small vessel disease is associated with LA. 108However, a variety of vasculopathies have been found to produce LA on imaging studies.Lipohyalinosis of the long penetrating arteries originating from the pial network and theventrofugal branches of the choroidal arteries is the most common abnormality in patientswith LA. Other vasculopathies can also lead to the neuropathological abnormalitiesdescribed earlier. 108 Cerebral amyloid angiopathy consisting of amyloid deposition in themedia and adventitia of small and midsized arteries of the cerebral cortex andleptomeninges is believed to lead to LA in patients with Alzheimer disease. 108 InCADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts andleukoencephalopathy) electron-dense, eosinophilic deposits are found in the media of smallvessels; this leads to lumen narrowing. 109
The implications of finding LA on computed tomographic scan or magnetic resonanceimaging are varied. Some studies have found that it is a predictor of vascular death inelderly neurological patients; when found in patients with ischemic strokes, it adds extrarisk of future strokes from large and small vessels. While some studies have found that LAis not an independent risk factor for intracerebral hemorrhage, 108 the increased severityof WMCs was found to correlate with a 7-fold increased risk of bleeding fromanticoagulation in the SPIRIT Study. 110
Lacunar infarctions
lacunar infarctions are secondary to the microvascular thrombo-occlusive episodes. Theyare most numerous in the periventricular gray matter (thalamus and basal ganglia) and theimmediate periventricular white matter. Spasm of the fine penetrating arterioles(secondary to increased VSMCs sensitivity) can also result in Lacunar infarctions.
o Background
The lacunar hypothesis proposes that (1) symptomatic lacunes present with distinctivelacunar syndromes and (2) a lacune is due to occlusion of a single deep penetrating arterygenerated by a specific vascular pathology. This concept is controversial because different
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
194

definitions of lacunes have been used. Lacunes may be confused with other empty spaces,such as enlarged perivascular (Virchow-Robbins) spaces, in which the specific small vesselpathology occasionally is absent. Originally, lacunes were defined pathologically, butlacunes now are diagnosed on clinical and radiological grounds. This problem iscompounded by the present inability to image a single penetrating artery.
Lacunes may be defined as small subcortical infarcts (less than 15 mm in diameter) in theterritory of the deep penetrating arteries and may present with specific lacunar syndromesor may be asymptomatic. Unfortunately, neither the 5 classical lacunar syndromes nor theradiological appearances are specific for lacunes. Lacunes occur most frequently in thebasal ganglia and internal capsule, thalamus, corona radiata, and pons.
o Pathophysiology
Lacunes are caused by occlusion of a single penetrating artery. The deep penetratingarteries are small nonbranching end arteries (usually smaller than 500 micrometers indiameter), which arise directly from much larger arteries (eg, the middle cerebral artery,anterior choroidal artery, anterior cerebral artery, posterior cerebral artery, posteriorcommunicating artery, cerebellar arteries, basilar artery). Their small size and proximalposition predispose them to the development of microatheroma and lipohyalinosis.
Figure 13. lacunar infarctions are secondary to the microvascular thrombo-occlusiveepisodes. They are most numerous in the periventricular gray matter (thalamus and basalganglia) and the immediate periventricular white matter.
Initially, lipohyalinosis was thought to be the predominant small vessel pathology oflacunes; however, microatheroma now is thought to be the most common mechanism ofarterial occlusion (or stenosis). Occasionally, atheroma in the parent artery blocks theorifice of the penetrating artery (luminal atheroma), or atheroma involves the origin of thepenetrating artery (junctional atheroma).
A hemodynamic (hypoperfusion) mechanism is suggested when there is a stenosis (and notocclusion) of the penetrating artery. When no evidence of small vessel disease is found on
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
195

histologic examination, an embolic cause is assumed, either artery-to-artery embolism orcardioembolism. About 25% of patients with clinical radiologically defined lacunes had apotential cardiac cause for their strokes.
o Histologic Findings
Lacunes are not examined histologically except at necropsy. Histologically, lacunes are nodifferent from other brain infarcts. Cells undergoing necrosis initially are pyknotic, thentheir plasma and nuclear membranes break down. Polymorphonuclear cells appearfollowed by macrophages, and the necrotic tissue is removed by phagocytosis. A cavitysurrounded by a zone of gliosis is the end result. Careful examination may reveal theunderlying small vessel pathology.
Figure 14. Pontine lacunar infarctions
Microatheroma causing occlusion or stenosis of a deep penetrating artery is the mostcommon small vessel pathology, usually involving the artery in the first half of its course.Histologically, microatheroma is identical to large vessel atheroma with subintimaldeposition of lipids and proliferation of fibroblasts, smooth muscle cells, and lipid-ladenmacrophages.
Lipohyalinosis is seen in the smaller penetrating arteries (<200 micrometers in diameter)and occurs almost exclusively in patients with hypertension. It has features of bothatheroma formation and fibrinoid necrosis with lipid and eosinophilic fibrinoid depositionin the media.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
196

o Neuroimaging of lacunar infarctions
Lacunar infarctions are punctate lesions mostly seen in the in the periventricular graymatter (thalamus and basal ganglia) and the immediate periventricular white matter, andare also seen in the brain stem. These lesions are hypodense on CT scan and hypointense ofT1 weighted images and hyperintense on the T2 weighted images. Contrast enhancementmight occur in acute lesions. Marked hypointensities on the T1 weighted images (blackholes) are consistent with extensive tissue damage and axonal loss.
On FLAIR images acute lacunar infarctions are diffusely hyperintense. However with thepassage of time central necrosis and cavitations occur in the lacunar infarction and theinfarction is transformed into a cavity filled with a CSF-like fluid and surrounded by agliotic wall, subsequently very old lacunar infarction is demonstrated by FLAIR images asa markedly hypointense (black) small lesion (representing the nulled CSF signal inside thecentral cavity of the lacunar infarction), this hypointense lesion (black hole) is surroundedby a hyperintense rim representing the gliotic walls of the lacunar infarction. In lacunarinfarctions, FLAIR MRI images are thus very helpful in demonstrating the age of theinfarction.
Figure 15. A, lipohyalinosis, B, lacunar infarction
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
197

Figure 16. Periventricular lacunarinfarctions and calcifications
Figure 17. Lacunes. Small cavitary infarcts, resulting from hypertension, most frequentlyinvolving the basal ganglia (caudate nucleus, globus pallidus, putamen, and amygdala) andbasis pontis. Compare right with left.
Granular atrophy (Cortical laminar necrosis )
Granular atrophy is defined pathologically as infarctions localized to the cerebral cortexand not extending to the subcortical white matter. It is characterized by the presence ofsmall punched- out foci of cavitated cicatricial softening situated entirely in the cortex andaccompanied by focal glial scar and thinning of the cortical ribbon. The lesions arebilateral and situated along the crest of the gyri. The presence of arteriolar pathology overthe cerebral convexity points to its ischemic aetiology.
Chronic brain infarcts are typically seen as low-intensity lesions on T1-weighted and high-intensity lesions on T2-weighted MR images due to prolonged T1 and T2 values 111,112. Insome infarcts, high-intensity lesions may be seen on T1-weighted images. High intensitylesions on T1-weighted MR images can be due to methaemoglobin, mucin, high proteinconcentration, lipid or cholesterol, calcification and cortical laminar necrosis. In ischemicstroke, high intensity laminar lesions can be cortical laminar necrosis, hemorrhagic
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
198

infarcts, or a combination of the two. Initially thought to be caused by hemorrhagicinfarction, histopathological examination has demonstrated these cortical short T1 lesionsto be cortical laminar necrosis without hemorrhage or calcification. Although, themechanism of T1 shortening in cortical laminar necrosis remains unclear, high corticalintensity on a T1-weighted image is believed to occur by neuronal damage and reactivetissue change of glia and deposition of fat-laden macrophages 113.
The gray matter has six layers. The third layer is the most vulnerable to depletion ofoxygen and glucose. Cortical laminar necrosis is a specific type of cortical infarction, whichusually develops as a result of generalized hypoxia rather than a local vascularabnormality. Depletion of oxygen or glucose as in anoxia, hypoglycemia, status epilepticus,and ischemic stroke has been attributed as an underlying cause of cortical laminarnecrosis. Immunosuppressive therapy (cyclosporin A and FK506), and polychemotherapy(vincristine and methotrexate) have been observed to cause laminar necrosis due tohypoxic-ischemic-insult. Hypoxic insult leads to death of neurons, glia and blood vesselsalong with degradation of proteins 114.
The cortical laminar necrosis, seen as a laminar high-signal lesion on T1-weighted MRimages, was first described by Swada et al. in a patient of anoxic encephalopathy 115. Earlycortical changes usually show low signal intensity on T1-weighted, which could be due toacute ischemic changes (tissue edema). Usually, cortical high intensity lesions on both T1-weighted and FLAIR images appear 2 weeks after the ictus indicating short T1 and long T2lesions. Proton-density images are more sensitive than T1-weighted MR images. Onproton-density images, cortical laminar necrosis may be seen as high intensity due toincreased mobile protons in the reactive tissue 116.
To conclude, cortical laminar necrosis shows characteristic chronological signal intensitychanges, and T1-weighted, FLAIR and proton-density MR images are especially helpful indepicting these changes.
Figure 18. Granular atrophy, notice laminar necrosis with early cavitation. Notepersistence of the outer most gray matter.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
199

Figure 19.Cortical laminarnecrosis. SagittalT1-weighted MRimage (A) depictsthe gyriformincreased signalarea in righttemporal andparietal region.T2-weighted MRand FLAIRimages showthese areas asdark signal areas.
Basal ganglionic calcifications
These are calcification of the the arteriolar walls within the basal ganglia.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
200

Figure 20. Basal ganglionic calcification
Dilated Virchow-Robin spaces (VRSs)
Virchow-Robin spaces (VRSs) are perivascular spaces that surround the perforatingarteries that enter the brain. The spaces are normally microscopic, but when dilated, theymay be seen on MR images. Even in the normal brain, some VRSs are usually seen in thearea of the substantia innominata at the level of the anterior commissure, and a smallnumber of dilated spaces may also be seen in the basal ganglia (BG) in up to 60% ofindividuals. Virchow-Robin Spaces can be identified by a combination of their typicallocation and their signal intensity characteristics. They are classically described asisointense to CSF on images obtained with all pulse sequences, and they are round or lineardepending on the imaging plane, although their characteristics may vary from this patternfor a number of reasons. First, the small size of the Virchow-Robin Spaces makes partial-volume effects common; therefore, measured signal intensities seldom equal those seen inpure CSF, although the changes in signal intensity between sequences are closelycorrelated. In addition, T1-weighted images with substantial flow sensitivity may show highsignal intensity due to inflow effects. Even if we allow for these effects, the measured signalintensity in the VRS often slightly differs from that of true CSF. This finding has beenattributed to the fact that Virchow-Robin Spaces around intracerebral arteries mayrepresent interstitial fluid trapped in the subpial or interpial space.
Pathologic dilatation of Virchow-Robin Spaces is most commonly associated with arteriolarabnormalities that arise due to aging, diabetes, hypercholesterolemia, smoking, andhypertension and other vascular risk factors. This dilatation forms part of a histologicspectrum of abnormalities, which include old, small infarcts (type 1 changes); scars fromsmall hematomas (type 2 changes); and dilatations of Virchow-Robin Spaces (type 3changes) (124). The presence of these abnormalities on histologic examination is believed toresult from moderate-to-severe microangiopathy characterized by sclerosis, hyalinosis, andlipid deposits in the walls of small perforating arteries 50 – 400 `im in diameter (124, 125).As the severity of the microangiopathy increases, microvessels demonstrate increasingly
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
201

severe changes, with arterial narrowing, microaneurysms and pseudoaneurysms, onionskinning, mural calcification, and thrombotic and fibrotic luminal occlusions (124–126)Although microvascular disease is common, few reliable surrogate imaging markers of itspresence have been described. The extent and severity of deep white matter (WM) andperiventricular hyperintensity on T2-weighted images have been widely studied aspotential surrogate markers for small-vessel disease. However, the correlation betweenthese abnormalities and clinical characteristics, such as diagnosis, vascular risk factor, orneuropsychological deficit, is often poor (127).
Figure 21. MRI T2 (A), MRIFLAIR (B) and precontrast MRIT1 (C) images showing dilatedVirchow-Robin Spaces associatedwith diffuse white matterchanges (leukoaraiosis)
o More details about etiology and pathogenesis of dilatation of Virchow-RobinSpaces
Virchow-Robin Spaces are potential perivascular spaces covered by pia that accompanyarteries and arterioles as they perforate the brain substance. Deep in the brain, theVirchow-Robin Spaces are lined by the basement membrane of the glia limitansperipherally, while the outer surfaces of the blood vessels lie centrally. These pial layersform the Virchow-Robin Spaces as enclosed spaces filled with interstitial fluid andseparated from the surrounding brain and CSF . Dilatation of Virchow-Robin Spacesresults in fluid filled perivascular spaces along the course of the penetrating arteries.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
202

Abnormal dilatation of Virchow-Robin Spaces is clinically associated with aging, dementia,incidental WM lesions, and hypertension and other vascular risk factors (123).Pathologically, this finding is most commonly associated with arterioscleroticmicrovascular disease, which forms a spectrum of severity graded from 1 to 3 on the basisof histologic appearances (124, 126). Grade 1 changes include increased tortuosity andirregularity in small arteries and arterioles (124) Grade 2 changes include progresssclerosis, hyalinosis, lipid deposits, and regional loss of smooth muscle in the vessel wallassociated with lacunar spaces that are histologically seen to consist of three subtypes. Type1 lacunes are small, old cystic infarcts; type 2 are scars of old hematomas; and type 3 aredilated Virchow-Robin Spaces (129). Grade 3 microangiopathy represents the most severestage and is especially related to severe chronic hypertension. Typical changes described inlower grades are accompanied by fibrotic thickening vessel wall with onion skinning, lossof muscularis and elastic lamina, and regional necrosis in the vessel walls. The brainparenchyma contains multiple lacunae, and diffuse abnormality of myelin is present in thedeep hemispheric white matter.
Several mechanisms for abnormal dilatation of Virchow-Robin Spaces have been suggested(130,131). These include mechanical trauma due to CSF pulsation or vascular ectasia (123),fluid exudation due to abnormalities of the vessel wall permeability (132), and ischemicinjury to perivascular tissue causing a secondary ex vacuo effect (133).
In the Western world, ischemic vascular dementia is seen in 8 –10% of cognitivelyimpaired elderly subjects (134) and commonly associated with widespread small ischemicor vascular lesions throughout the brain, with predominant involvement of the basalganglia, white matter, and hippocampus (134). Several groups have shown that a severelacunar state and microinfarction due to arteriolosclerosis and hypertensivemicroangiopathy are more common in individuals with IVD than in healthy controlsubjects, and they have emphasized the importance of small vascular lesions in thedevelopment of dementia (134, 135). On CT or MR imaging, white matter lesions arecommonly used as potential biomarkers of vascular abnormality. Many groups havesuggested that simple scoring schemes for white matter lesion load and distribution areuseful in the diagnosis of vascular dementia (136). Although white matter lesions are moresevere in patients with vascular dementia (136), they are more prevalent in all groups withdementia than in healthy control subjects.
Dilation of Virchow-Robin Spaces provides a potential alternative biomarker ofmicrovascular disease (small vessel disease). Virchow-Robin Spaces in the centrumsemiovale were significantly more frequent in patients with fronto-temporal dementia(FTD) than in control subjects (P .01). This finding is not associated with increases in basalganglionic Virchow-Robin Spaces and is closely correlated with measures of forebrainatrophy, suggesting that these changes are probably representative of atrophy, which ismore marked in this patient group than in those with other dementing conditions (128).
The ischaemic microvascular brain disease is the interaction between the haemorheologicalchanges, the vascular arteriolar pathology and the neuronal diminished glucose and oxygen entry
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
203

In general all the pathological consequences of the microvascular brain disease arerestricted to either the cortical zone (cortical atrophy. granular atrophy) or theperiventricular zone (central atrophy, leukoaraiosis and lacunar infarctions, dilatedVirchow-Robin Spaces). i.e. All the ischemic events occurred in the distribution of eitherthe pial or the subependymal microvascular systems. This should mean that hypoperfusion,in microvascular brain disease, is restricted to either the cortical or the periventricularbrain regions. The left cerebral hemisphere is more often and more severely affected thanthe right cerebral hemisphere.
It must be noted that in microvascular brain disease one always see a mix of pathology, i.e.in the same patient lacunar infarctions with leukoaraiosis and central and cortical atrophymight coexist.
Figure 22. Leukoaraiosis showing centralhypoperfusion on spect study
Figure 23. Left hemispherical [mainly frontal]hypoperfusion on spect study
Cerebral Microbleeds
Cerebral microbleeds are small brain hemorrhages that are presumed to result fromleakage of blood cells from damaged small vessel walls. They were first detected on MRimaging only in the mid-1990s, as MR imaging sequences sensitive to blood-breakdownproducts became available (eg, T2-weighted gradient-echo technique), which are essentialfor microbleed detection (Figure 24). 37 Histologically, these small black dots on MRimaging represent hemosiderin-laden macrophages that are clustered around small vessels(Figure 25). The choice of field strength, sequence parameters (particularly echo time), andpostprocessing (eg, susceptibility-weighted imaging technique) have all been found to havea major influence on the detection rate of cerebral microbleeds. 148,149,150,151 With theseadvances in imaging, the prevalence of microbleeds has been estimated to be more than20% in persons aged 60 years and older, increasing to nearly 40% in those older than 80years. 151 Microbleeds are also commonly asscoiated with microvascular brain disease.Microbleed location is generally divided into deep (ie, basal ganglia, thalamus) andinfratentorial versus lobar brain regions (Figure 26). In the aging population, microbleedsin lobar locations share apolipoprotein E (APOE) e4 genotype as a common risk factorwith cerebral amyloid angiopathy (CAA) and Alzheimer's disease (AD), suggestive of apotential link between vascular and amyloid neuropathology. 151,152 This link has furtherbeen corroborated by the finding that topography of lobar microbleeds in community-dwelling elderly individuals follows the same posterior distribution as is known fromamyloid disease in cerebral amyloid angiopathy (CAA) and Alzheimer's disease (AD). 153
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
204

Furthermore, some reports show that presence of microbleeds, and particularly those inlobar locations, relates to worse cognitive function, both in healthy elderly individuals 154,155 and in patients diagnosed with Alzheimer's disease (AD). 156 In contrast, deep orinfratentorial microbleeds in aging individuals are primarily linked to classiccardiovascular risk factors and are more likely caused by hypertensive vasculopathy. 151Longitudinal studies indicate that incident microbleeds commonly occur over time:annually, 3% of presumed healthy elderly individuals develop new microbleeds, increasingto more than 7% of those who already have microbleeds at baseline. 157 In comparison,these rates are doubled in patients attending a memory clinic. 157
The increasing evidence that microbleeds reflect both vascular disease as well as amyloidangiopathy has led to the belief that these may well represent the missing link between thevascular and amyloid hypotheses in the pathogenesis of Alzheimer's disease (AD).
Figure 24. Microbleed imaging. T1-weighted (left), T2-weighted (middle), and T2-weighted(right) images. Cerebral microbleeds, depicted by arrows, are visualized only on the T2-weighted image and not on the T1-weighted or T2-weighted images. The T2-weightedimage is susceptible to paramagnetic properties of hemosiderin, causing the microbleeds toappear as black dots of signal loss.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
205

Figure 25. Radiologic-pathologic correlation of cerebral microbleeds on MR imaging (3 T).Postmortem brain MR imaging shows on T2-weighted imaging a hypointense focus on thegray-white matter interface (white arrow). MR image in the middle of the isolated tissueblock containing this hypointense focus. Pathologic analysis of this tissue block(hematoxylin and eosin stain) shows macrophages containing hemosiderin (black arrows),confirming that the hypointense lesion on MR imaging is compatible with a microbleed.
Figure 26 Microbleed location. T2-weighted MR images showing microbleeds (arrows) inlobar (left), deep (middle), and infratentorial (right) locations.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
206

Table 2. Pathology of ischemic microvascular brain disease
Central and corticalatrophy
This is secondary to chronic global reduction of brain perfusion.
Leukoaraiosis (diffuseperiventricular whitematter disease)
Leukoaraiosis is an ischaemic demyelination of the immediateperiventricular white matter with axonal loss, astrogliosis andinterstitial edema. It is secondary to chronic global reduction ofbrain perfusion.
Lacunar infarctions lacunar infarctions are secondary to the micro vascular thrombo-occlusive episodes. They are most numerous in the periventriculargray matter (thalamus and basal ganglia) and the immediateperiventricular white matter. Spasm of the fine penetratingarterioles (secondary to increased VSMCs sensitivity) -can alsoresult in Lacunar infarctions.
Granular atrophy Granular atrophy is defined pathologically as infarctions localizedto the cerebral cortex and not extending to the subcortical whitematter.
Basal ganglioniccalcifications
These are calcification of the the arteriolar wall of themicrocirculation within the basal ganglia.
Dilated Virchow-Robin Spaces
Dilation of Virchow-Robin Spaces provides a potential alternativebiomarker of microvascular disease (small vessel disease).
Cerebral Microbleeds The increasing evidence that microbleeds reflect bothmicrovascular brain disease as well as amyloid angiopathy has ledto the belief that these may well represent the missing link betweenthe vascular and amyloid hypotheses in the pathogenesis ofAlzheimer's disease (AD).
VERTEBROBASILAR ECTASIA (FUSIFORM ANEURYSM, VERTEBROBASILARDOLICHOECTASIA)
A dolichoectatic vessel is one that is both too long (elongated) and too large (distended).Basilar artery elongation is present, by strict criteria, when the artery lies lateral to eitherthe clivus or dorsum sellae or terminates above the suprasellar cistern. A basilar arterylarger than 4.5 mm in diameter is defined as ectatic (too large). The term ''fusiformaneurysm'' has, unfortunately, been used interchangeably in the scientific literature withdolichoectatic change and ectasia, all referring to diffuse tortuous enlargement andelongation of an artery. Dolichoectasia occurs with greatest frequency in thevertebrobasilar system (Fig. 23) but may also involve the intracranial internal carotid andmiddle cerebral arteries. A contour deformity of the pons resulting from basilar arteryectasia is a not uncommon incidental finding on MRI in the elderly population. Traction ordisplacement of cranial nerves can, however, lead to symptoms. Depending on the segmentof the basilar artery involved, cranial nerve II, III, VI, VII, or VIII can be affected. Thelower cranial nerves can be affected with vertebral artery involvement. 140
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
207

Symptomatic vertebrobasilar dolichoectasia exists in two different patient populations:those with isolated cranial nerve involvement and those with multiple neurologic deficits.The latter population includes patients with combinations of cranial nerve deficits(resulting from compression) and central nervous system deficits (resulting fromcompression or ischemia). A tortuous, but normal-caliber, basilar artery is more likely toproduce isolated cranial nerve involvement, whereas ectasia is more likely to cause multipledeficits of either compressive or ischemic cause. Ectasia of the vertebro-basilar system isoccasionally associated with microvascular brain disease as explained above 140
Figure 27. Partially thrombosed giant intracranial aneurysm. A large low-signal intensitylesion is noted on the spin echo scan with intermediate T2-weighting (A) in the region of theleft cavernous sinus. A pulsation artifact (black arrows) is seen extending in the phaseencoding direction posteriorly from the lesion but originating from only the more medialportion. Comparison of pre(B) and postcontrast (C) T1-weighted scans revealsenhancement in only the more anterior and medial portions of the lesion (white arrow).Three-dimensional time-of-flight magnetic resonance angiography depicts a patent lumen
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
208

within the mass corresponding in position to that suggested by the pulsation artifact andcontrast enhancement. The majority of this giant aneurysm of the cavernous and distalpetrous carotid artery is thrombosed. Only a crescent of residual lumen remains. Theprecontrast scans are misleading because the clotted portion of the aneurysm has very lowsignal intensity on the T2-weighted scan and intermediate to low signal intensity on the T1-weighted scan. but normal-caliber, basilar artery is more likely to produce isolated cranialnerve involvement, whereas ectasia is more likely to cause multiple deficits of eithercompressive or ischemic cause.
Finally it should be noted that microvascular brain disease isinvariably associated with hypertensive concentric left ventricularhypertrophy with unfailing 1-1 relationship.
Figure 28. Left ventricular hypertrophy with strain pattern
Table 3. MICROVASCULAR BRAIN DISEASE & CARDIOVASCULAR ASSOCIATES
LACUNAR INFARCTION LEUKOARAIOSIS CENTRAL & CORTICAL ATROPHY GRANULAR ATROPHY SPONTANEOUS HYPERTENSIVE CEREBRAL HAEMORRHAGE BASAL GANGLIONIC CALCIFICATION
DUPLEX SCANNING OF CAROTID ARTERIESSHOWS NORMAL FINDINGS OR NONSIGNIFICANT CHANGES
LEFT VENTRICULAR HYPERTROPHY WITHSTRAIN PATTERN
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
209

SUMMARY
PATHOLOGY CT SCAN MRI
Lacunar infarctions
Leukoaraiosis
Central and cortical atrophy
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
210

Dilated Virchow-Robin Spaces
Basal ganglionic calcifications
References
1. Alavi A, Fazakas F, Chawluk JC, et al: A comparison of CT, MR and PET inAlzheimer's dementia and normal aging. J Nucl Med 29:852, 1988
2. Almkvist 0, Wahlund L, Andersonn-Lundman G, et al: White-matter hyperintensity andneuropsychological functions in dementia and healthy aging. Arch Neurol 49:626-632, 1992
3. Awad IA, Johnson PC, Spetzler RF, et al: Incidental subcortical lesions identified onmagnetic resonance imaging in the elderly. 11. Postmortem pathological correlations.Stroke 17:1090-1097, 1986
4. Awad IA, Spetzler RF, Hodak JA, et al: Incidental subcortical lesions identified onmagnetic resonance imaging in the elderly. 1. Correlation with age and cerebrovascularrisk factors. Stroke 17:1084- 1089, 1986
5. Babikian V, Ropper AH: Binswanger's disease: A review. Stroke 18:2-12, 1987
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
211

6. Baker LL, Stevenson DK, Enzmann DR: End-stage periventricular leukomalacia: MRevaluation. Radiology 168:809-815, 1988
7. Ball Mj: Ischemic axonopathy: Further evidence that neocortical pathologyaccompanying cerebral hypoperfusion during systemic hypotension causes white matterrarefaction in the elderly and some people with Alzheimer dementia. J Neuropathol ExperNeurol 47:338, 1988
8. Bondareff W, Raval J, Woo B, et al: Magnetic resonance imaging and the severity ofdementia in older adults. Arch Gen Psychiatry 47:47-51, 1990
9. Boone KB, Miller BL, Lesser EM, et al: Neuropsychological correlates of white-matterlesions in healthy elderly subjects: A threshold effect. Arch Neurol 49:549-554, 1992
10. Bowen BC, Barker WW, Loewenstein DA, et al: MR signal abnormalities in memorydisorder and dementia. AJNR Am j Neuroradiol 11:283-290, 1990
11. Bradley WG, Waluch V, Brant-Zawadzki M, et al: Patchy periventricular white matterlesions in the elderly: A common observation during NMR imaging. Noninvasive MedicalImaging 1:35-41, 1984
12. Braffman BH, Zimmerman RA, Trojanowski JQ, et al: Brain MR: Pathologiccorrelation with gross and histopathology. 1. Lacunar infarction and Virchow- Robinspaces. Am j Radiol 151:551-558, 1988
13. Braffman BH, Zimmerman RA, Trojanowski JQ, et al: Brain MR: Pathologiccorrelation with gross and histopathology. 2. Hyperintense white-matter foci in the elderly.AJR Am J Roentgenol 151:559-566, 1988
14. Brant-Zawadzki M, Fein G, VanDyke C, et al: MR imaging of the aging brain: Patchywhite-matter lesions and dementia. AJNR Am j Neuroradiol 6:675-682, 1985
15. Brun A, Englund E: A white matter disorder in dementia of the Alzheimer type: Apathoanatomical study. Ann Neurol 19:253-262, 1986
16. Burger PC, Burch JG, Kunze U: Subcortical arteriosclerotic encephalopathy(Binswanger's disease)-a vascular etiology of dementia. Stroke 7:626-631, 1976
17. Caird WK, Inglis J: The short-term storage of auditory and visual two-channel digitsby elderly patients with memory disorder. j Ment Sci 107:1062-1069, 1961
18. Caplan LR, Schmahmann JD, Kase CS, et al: Caudate infarcts. Arch Neurol 47:133-143, 1990
19. Caplan LR, Schoene WC: Clinical features of subcortical arterioscleroticencephalopathy (Binswanger's disease). Neurology 28:1206-1215, 1978
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
212

20. Castaigne P, Lhermitte F, Buge A, et al: Paramedian thalamic and midbrain infarcts:Clinical and neuropathological study. Ann Neurol 10:127-148, 1981
21. de la Monte SM: Quantitation of cerebral atrophy in preclinical and end-stageAlzheimer's disease. Ann Neurol 25:450-459, 1989
22. DeReuck J, Crevits L, DeCoster W, et al: Pathogenesis of Binswanger chronicprogressive subcortical encephalopathy. Neurology 30:920-928, 1980
23. Diaz JF, Merskey H, Hachinski VC, et al: Improved recognition of leukoaraiosis andcognitive impairment in Alzheimer's disease, Arch Neurol 48: 1022-1025,1991
24. Durand-Fardel M: Memoire sur une alteration parficuliere de la substance cerebrate.Gaz Med 10:23- 38, 1842
25. Edwards MS: Comment. Neurosurgery 20:226, 1987
26. Englund E, Brun A, Persson B: Correlations between histopathologic white matterchanges and proton MR relaxation in dementia. Alzheimer Disease and AssociatedDisorders 1:156-170, 1987
27. Erkinjuntti R, Ketonen L, Sulkava R, et al: Do white matter changes on MRI and CTdifferentiate vascular dementia from Alzheimer's disease? j Neurol Neurosurg Psychiatry50:37-42, 1987
28. Esiri MM, Oppenheimer DR: Diagnostic Neuropathology. Oxford, Blackwell Scientific,1989, p 53
29. Fazekas F, Chawluk JB, Alavi A, et al: MR signal abnormalities at 1.5 T in Alzheimer'sdementia and normal aging. AJR Am J Roentgenol 149:351- 356, 1987
30. Fazekas F, Niederkorn K, Schmidt R, et al: White matter signal abnormalities innormal individuals: Correlation with carotid ultrasonography, cerebral blood flowmeasurements, and cerebrovascular risk factors. Stroke 19:1285-1288, 1988
31. Feigin 1, Budzilovich G, Weinberg S, et al: Degeneration of white matter in hypoxia,acidosis and edema. Neuropathol Exper Neurol 32:125-143, 1973
32. Feigin 1, Popoff N: Neuropathological changes late in cerebral edema: The relationshipto trauma, hypertensive disease and Binswanger's encephalopathy. Neuropathol ExperNeurol 22:500-511, 1963
33. Fein G, Van Dyke C, Davenport L, et al: Preservation of normal cognitive functioningin elderly subjects with extensive white-matter lesions of long duration. Arch GenPsychiatry 47:220-223, 1990
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
213

34. George AE, de Leon Mj, Gentes Cl, et. al: Leukoencephalopathy in normal andpathologic aging: 1. CT of brain lucencies. AJNR Am j Neuroradiol 7:561-566, 1986
35. George AE, de Leon Mj, Kalnin A, et al: Leukoencephalopathy in normal andpathologic aging: 2. MRI and brain lucencies. AJNR Am j Neuroradiol 7:567-570, 1986
36. Gerard G, Weisberg LA: MRI periventricular lesions in adults. Neurology 36:998-1001,1986
37. Ghatak NR, Hirano A, Lijtmaer H, et al: Asymptomatic demyelinated plaque in thespinal cord. Arch Neurol 30:484-486, 1974
38. Gilbert jj, Sadler M: Unsuspected multiple sclerosis. Arch Neurol 40:533-536, 1983
39. Goto K, Ishii N, Fukasawa H: Diffuse white matter disease in the geriatric population.Neuroradiology 141:687-695, 1981
40. Graff-Radford NR, Eslinger Pj, Damasio AR, et al: Nonhemorrhagic infarction of thethalamus: Behavioral, anatomic, and physiologic correlates. Neurology 34:14-23, 1984
41. Gray F, Dubas F, Roullet E, et al: Leukoencephalopathy in diffuse hemorrhagiccerebral amyloid angiopathy. Ann Neurol 18:54-59, 1985
42. Hachinski VC, Potter P, Mersky H: Leuko-araiosis. Arch Neurol 44:21-23, 1987
43. Heier LA, Bauer Cj, Schwartz L, et al: Large Virchow- Robin spaces: MR-clinicalcorrelation, AJNR Am j Neuroradiol 10:929-936, 1989
44. Hendrie HC, Farlow MR, Austrom MG, et al: Foci of increased T2 signal intensity onbrain MR scans of healthy elderly subjects. AJNR Am j Neuroradiol 10:703-707, 1989
45. Herholz K, Heindel W, Rackl A, et al: Regional cerebral blood flow in patients withleukoaraiosis and atherosclerotic carotid artery disease. Arch Neurol 47:392-396, 1990
46. Hijdra A, Verbeeten B, Verhulst JAPM: Relation of leukoaraiosis to lesion type instroke patients. Stroke 21:890-894, 1990
47. Hochwald GM, Wald A, Malhan C: The sink action of cerebrospinal fluid volume flow.Arch Neurol 33:339-344, 1976
48. Hunt AL, Orrison VVW, Yeo RA, et al: Clinical significance of MRI white matterlesions in the elderly. Neurology 39:1470-1474, 1989
49. Inzitari D, Diaz F, Fox A, et al: Vascular risk factors and leukoaraiosis. Arch Neurol44:42-47, 1987
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
214

50. Isaac C, Li DKB, Genton M, et al: Multiple sclerosis: A serial study using MRI inrelapsing patients. Neurology 38:1511-1515, 1988
51. Ishii N, Nishihara Y, Imamura T: Why do frontal lobe symptoms predominate invascular dementia with lacunes? Neurology 36:340-345, 1986
52. Jungreis CA, Kanal E, Hirsh WL, et al: Normal perivascular spaces mimicking lacunarinfarction: MR imaging. Radiology 169:101-104, 1988
53. Kertesz A, Polk M, Carr T: Cognition and white matter changes on magnetic resonanceimaging in dementia. Arch Neurol 47:387-391, 1990
54. Kinkel WR, Jacobs L, Polachini 1, et al: Subcortical arteriosclerotic encephalopathy(Binswanger's disease). Arch Neurol 42:951-959, 1985
55. Kirkpatrick JB, Hayman LA: White-matter lesions in MR imaging of clinically healthybrains of elderly subjects: Possible pathologic basis. Radiology 162:509-511, 1987
56. Kluger A, Gianutsos J, de Leon Mj, et al: Significance of age-related white matterlesions. Stroke 19:1054- 1055, 1988
56a. Kluger A, Gianutsos J, Golomb J, et al: White matter lesions in human aging:Associations with higher order motor control [abstract]. J Neuropsychiatry Clin Neurosci6:313, 1994
57. Kobari M, Meyer JS, Ichijo M: Leuko-araiosis, cerebral atrophy, and cerebralperfusion in normal aging. Arch Neurol 47:161-165, 1990
58. Kobari M, Meyer JS, Ichijo M, et al: Leukoaraiosis: Correlation of MR and CTfindings with blood flow, atrophy, and cognition. AJNR Am j Neuroradiol 11:273-281, 1990
59. Lee S, Terashi A: Progressive periventricular hyperintensity on MR imaging. Am jRadiol 152:654- 655, 1989
60. Leifer D, Buonanno F, Richardson E: Clinicopathologic correlations of cranialmagnetic resonance imaging of periventricular white matter. Neurology 40:911-918, 1990
61. Leys D, Soetaert G, Petit H, et al: Periventricular and white matter magnetic resonanceimaging hyperintensities do not differ between Alzheimer's disease and normal aging. ArchNeurol 47:524-527, 1990
62. Loes DJ, Biller J, Yuh WTC, et al: Leukoencephalopathy in cerebral amyloidangiopathy: MR imaging in four cases. AJNR Am j Neuroradiol 11:485-488, 1990
63. Lotz PR, Ballinger WE, Quisling RG: Subcortical arteriosclerotic encephalopathy: CTspectrum and pathologic correlation. AJNR Am j Neuroradiol 7:817- 822, 1986
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
215

64. Mackay RP, Hirano A: Forms of benign multiple sclerosis. Report of two "clinicallysilent" cases discovered at autopsy. Arch Neurol 17:588-600, 1967
65. Mandybur TI: The incidence of cerebral angiopathy in Alzheimer's disease. Neurology25:120-126, 1975
66. Marshall VG, Bradley WG, Marshall CE, et al: Deep white matter infarction:Correlation of MR imaging and histopathologic findings. Radiology 167:517- 522, 1988
67. Masdeu JC, Wolfson L, Lantos G, et al: Brain white- matter changes in the elderlyprone to falling. Arch Neurol 46:1292-1296, 1989
68. McComb JG: Recent research into the nature of cerebrospinal fluid formation andabsorption. J Neurosurgery 59:369-383, 1983
69. Mendez MF, Adams NL, Lewandowski KS: Neurobehavioral changes associated withcaudate lesions. Neurology 39:349-354, 1989
70. Michel D, Laurent B, Foyatier N, et al: Infarctus thalamique paramedian gauche etudede la memoire et du langage. Rev Neurol (Paris) 138:533-550, 1982
71. Miyao S, Takano A, Teramoto J, et al: Leukoaraiosis in relation to prognosis forpatients with lacunar infarction. Stroke 23:1434-1438, 1992
72. Morariu M, YJutzow WF: Subclinical multiple sclerosis. J Neurology 213:71-76, 1976
73. Morris JC, Gado MH, Grant EA, et al: Periventricular white matter lucencies: Noeffect on the natural history of senile dementia of the Alzheimer type [abstract]. AnnNeurol 24:159-160, 1988
74. Munoz DG, Hastak SM, Harper B, et al: Pathologic correlates of increased signals ofthe centrum ovale on magnetic resonance imaging. Arch Neurol 50:492-497, 1993
75. Olszewski J: Subcortical arteriosclerotic encephalopathy-review of the literature on theso-called Binswanger's disease and presentation of two cases. World Neurology 3:359-375,1962
76. Pujol J, Marti-Vilata JL, Junque C, et al: Wallerian degeneration of the pyramidaltract in capsular infarction studied by magnetic resonance imaging. Stroke 21:404-409,1990
77. Rao SM, Mittenberg W, Bernardin L, et al: Neuropsychological test findings in subjectswith leukoaraiosis. Arch Neurol 46:40-44, 1989
78. Reulen Hj, Tsuyumu M, Tack A: Clearance of edema fluid into the cerebrospinal fluid.A mechanism for resolution of vasogenic brain edema. J Neurosurgery 48:754-764, 1978
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
216

79. Rezek DL, Morris JC, Fulling KH, et al: Periventricular white matter lucencies insenile dementia of the Alzheimer type and in normal aging. Neurology 37:1365-1368, 1987
80. Roman GC: Senile dementia of the Binswanger type: A vascular form of dementia inthe elderly. JAMA 258:1782-1788, 1987
81. Rosenberg GA, Kyner WT, Estrada E: Bulk flow of brain interstitial fluid undernormal and hyperosmolar conditions. Am J Physiol 238:F42-F49, 1980
82. Salomon A, Yeates AE, Burger PC, et al: Subcortical arteriosclerotic encephalopathy:Brain stem findings with MR imaging. Radiology 165:625-629, 1987
83. Sarpel G, Chaudry F, Hindo W: Magnetic resonance imaging of periventricularhyperintensity in a Veterans Administration hospital population. Arch Neurol 44:725-728,1987
84. Steingart A, Hachinski VC, Lau C, et al: Cognitive and neurologic findings in subjectswith diffuse white matter lucencies on computed tomographic scan (leukoaraiosis). ArchNeurol 44:32-35, 1987
85. Steingart A, Hachinski VC, Lau C, et al: Cognitive and neurologic findings in dementedpatients with diffuse white matter lucencies on computed tomographic scan (leukoaraiosis).Arch Neurol 44:36- 39, 1987
86. Sze G, De Armond Sj, Brant-Zawadzki M, et al: Foci of MRI signal (pseudo lesions)anterior to the frontal horns: Histologic correlations of a normal finding. AJR Am JRoentgenol 147:331-337, 1986
87. Tatemichi TK, Desmond DW, Prohovnik 1, et al: Confusion and memory loss fromcapsular-genu infarction: A thalamocortical disconnection syndrome? Neurology 42:1966-1979, 1992
88. Tomonaga BM, Yamanouchi H, Tohgi H, et al: Clinicopathologic study of progressivesubcortical vascular encephalopathy (Binswanger type) in the elderly. J Am Geriatr Soc30:524-529, 1982
89. Tupler LA, Coffey EC, Logue PE, et al: Neuropsychological importance of subcorticalwhite matter hyperintensity. Arch Neurol 49:1248-1252, 1992
90. Valentine AR, Moseley IF, Kendall BE: White matter abnormality in cerebral atrophy:Clinicoradiological correlations. j Neurol Neurosurg Psychiatry 43:139-142, 1980
91. van Swieten JC, van den Hout JHW, van Ketal BA, et al: Periventricular lesions in thewhite matter on magnetic resonance imaging in the elderly. Brain 114:761-774, 1991
92. Weller R: Color Atlas of Neuropathology. London, H. Miller Publishers, 1984, p 26
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
217

93. Yamaguchi F, Meyer JS, Yamamoto M, et al: Noninvasive regional cerebral blood flowmeasurements in dementia. Arch Neurol 37:410-418, 1980
94. Yao H, Sadoshima S, lbayashi S, et al: Leukoaraiosis and dementia in hypertensivepatients. Stroke 23:1673-1677, 1992
95. Ylikoski. R, Ylikoski A, Erkinjuntti T, et al: White matter changes in healthy elderlypersons correlate with attention and speed of mental processing. Arch Neurol 50:818-824,1993
96. Zeumer H, Schonsky B, Sturm KW: Predominant white matter involvement insubcortical arteriosclerotic encephalopathy (Binswanger disease). J Comp Assist Tomogr4:14-19, 1980
97. Zimmerman RD, Fleming CA, Lee BCP, et al: Periventricular hyperintensity as seen bymagnetic resonance: Prevalence and significance. AJNR Am j Neuroradiol 7:13-20, 1986
98. Adams HP Jr, Brott TG, Furlan AJ, et al: Guidelines for thrombolytic therapy foracute stroke: a supplement to the guidelines for the management of patients with acuteischemic stroke. A statement for healthcare professionals from a Special Writing Group ofthe Stroke Council, American Heart. Circulation 1996 Sep 1; 94(5): 1167-74.
99. Bamford JM, Warlow CP: Evolution and testing of the lacunar hypothesis. Stroke 1988Sep; 19(9): 1074-82.
100. Gan R, Sacco RL, Kargman DE, et al: Testing the validity of the lacunar hypothesis:the Northern Manhattan Stroke Study experience. Neurology 1997 May; 48(5): 1204-11.
101. Inzitari D, Eliasziw M, Sharpe BL, et al: Risk factors and outcome of patients withcarotid artery stenosis presenting with lacunar stroke. North American SymptomaticCarotid Endarterectomy Trial Group. Neurology 2000 Feb 8; 54(3): 660-6.
102. Post-stroke Rehabilitation Guideline Panel: Post-stroke rehabilitation – clinicalpractice guideline. Gaithersburg: Aspen Publishers; 1996.
102. Pullicino PM, Caplan LR, Hommel M: Cerebral small artery disease. In: Advances inNeurology. Vol 62. 1993.
104. The National Institute of Neurological Disorders and Stroke: Tissue plasminogenactivator for acute ischemic stroke. The National Institute of Neurological Disorders andStroke rt-PA Stroke Study Group. N Engl J Med 1995 Dec 14; 333(24): 1581-7.
105. Yusuf S, Sleight P, Pogue J, et al: Effects of an angiotensin-converting-enzymeinhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart OutcomesPrevention Evaluation Study Investigators. N Engl J Med 2000 Jan 20; 342(3): 145-53.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
218

106. Munoz DG, Hastak SM, Harper B, Lee D, Hachinski VC. Pathologic correlates ofincreased signals of the centrum semiovale on magnetic resonance imaging. Arch Neurol.1993;50:492-497.
107. Chimowitz MI, Estes ML, Furlan AJ, Awad IA. Further observations on the pathologyof subcortical lesions identified on magnetic resonance imaging. Arch Neurol. 1992;49:747-752.
108. Pantoni L, Garcia JH. Pathogenesis of leukoaraiosis: a review. Stroke. 1997;28:652-659.
109. Baudrimont M, Dubas F, Joutel A, Tournier-Lasserve E, Bousser MG.Autosomaldominant leukoencephalopathy and subcortical ischemic strokes: a clinicopathologicalstudy.Stroke.1993;24:122-125.
110. The Stroke Prevention in Reversible Ischemia Trial (SPIRIT) Study Group.randomized trial of anticoagulants versus aspirin after cerebral ischemia of presumedarterial origin. Ann Neurol. 997;42:857-865.
111. Sipponen JT. Visualization of brain infarction with nuclear magnetic resonanceimaging. Neuroradiology 1984; 26:387-391.
112. Brant-Zawadzki M, Weinstein P, Bartkowski H, Moseley M. MR imaging andspectroscopy in clinical and experimental cerebral ischemia: a review. AJNR Am JNeuroradiol 1987; 8:39-48.
113. Boyko OB, Burger PC, Shelburne JD, Ingram P. Non-heme mechanisms for T1shortening: pathologic, CT, and MR elucidation. AJNR Am J Neuroradiol 1992; 13:1439-1445.
114. Bargallo N, Burrel M, Berenguer J, Cofan F, Bunesch L, Mercader M. Corticallaminar necrosis caused by immunosuppresive therapy and chemotherapy. AJNR Am JNeuroradiol 2000; 21:479-484.
115. Sawada H, Udaka F, Seriu N, Shindou K, Kameyama M, Tsujimura M. MRIdemonstration of cortical laminar necrosis and delayed white matter injury in anoxicencephalopathy. Neuroradiology 1990; 32:319-321.
116. Komiyama M, Nishikawa M, Yasui T. Cortical laminar necrosis in brain infarcts:chronological changes on MRI. Neuroradiology 1997; 39:474-479.
117. Moan A, Nordby G, Os I, Birkeland KI, Kjeldsen SE. Relationship betweenhemorheologic factors and insulin sensitivity in healthy young men. Metabolism 1994; 43:423-427,
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
219

118. Nordby G, Moan A, Kjeldsen SE, Os I. Relationship between hemorheological factorsand insulin sensitivity in normotensive and hypertensive premenopausal women. Am JHypertens 1995; 8: 439-444
119. Brun JF, Monnier JF, Kabbaj H, Orsetti A. La viscosité sanguine est corrélée àl'insulino-résistance. J Mal Vasc 1996; 21: 171-174
120. Høieggen A, Fossum E, Moan A, Enger E, Kjeldsen SE. Whole-blood viscosity and theinsulin-resistance syndrome. J Hypertens 1998; 16: 203-210,
121. Fanari P, Somazzi R, Nasrawi F, Ticozzelli P, Grugni G, Agosti R, Longhini E.Hemorheological changes in obese adolescents after short-term diet. Int J Obes RelatMetab Disord 1993; 17: 487-494
122. Hu G, Jousilahti P, Bidel S, Antikainen R, Tuomilehto J. Type 2 Diabetes and the Riskof Parkinson's Disease Diabetes Care 30:842-847, 2007 [Full text]
123. Heier LA, Bauer CJ, Schwartz L, Zimmerman RD, Morgello S, Deck MD. LargeVirchow-Robin spaces: MR-clinical correlation. AJNR Am J Neuroradiol 1989;10:929 -936
124. Hommel M, Gray F. Microvascular pathology. In: Caplan L, ed. Brain Ischaemia:Basic Concepts and Clinical Relevance. New York: Springer-Verlag Berlin; 1995:215-223
125. Furuta A, Ishii N, Nishihara Y, Horie A. Medullary arteries in aging and dementia.Stroke 1991;22:442- 446
126. Brun A, Fredriksson K, Gustafson L. Pure subcortical arterioscle- roticencephalopathy (Binswanger’s disease): a clinicopathological study. Part 2: Pathologicalfeatures. Cerebrovasc Dis 1992;2:87-92
127. Thomas AJ, O’Brien JT, Davis S, et al. Ischemic basis for deep white matterhyperintensities in major depression: a neuropatho- logical study. Arch Gen Psychiatry2002;59:785-792
128. Thacker NA, Varma AR, Bathgate D, et al. Dementing disor- ders: volumetricmeasurement of cerebrospinal fluid to distin- guish normal from pathologic findings:feasibility study. Radi- ology 2002;224:278 -285
129. Poirier J, Derouesne C. Cerebral lacunae: a proposed new classi- fication [letter]. ClinNeuropathol 1984;3:266
130. Fazekas F, Kleinert R, Offenbacher H, et al. The morphologic correlate of incidentalpunctate white matter hyperintensities on MR images. AJNR Am J Neuroradiol1991;12:915-921
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
220

131. Ogawa T, Okudera T, Fukasawa H, et al. Unusual widening of Virchow-Robin spaces:MR appearance. AJNR Am J Neuroradiol 1995;16:1238 -1242
132. Hughes W. Origin of lacunes. Lancet 1965 1:19 -21
133. Benhaiem-Sigaux N, Gray F, Gherardi R, Roucayrol AM, Poirier J. Expandingcerebellar lacunes due to dilatation of the perivascular space associated with Binswanger’ssubcortical arteriosclerotic en- cephalopathy. Stroke 1987;18:1087-1092
134. Derouesne C, Gray F, Escourolle R, Castaigne P. "Expanding cerebral lacunae" in ahypertensive patient with normal pressure hydrocephalus. Neuropathol Appl Neurobiol1987;13:309 -320
135. Pullicino PM, Miller LL, Alexandrov AV, Ostrow PT. Infrapu- taminal "lacunes":clinical and pathological correlations. Stroke 1995;26:1598 -1602
136. Jellinger KA. The pathology of ischemic-vascular dementia: an update. J Neurol Sci2002; 203-204:153-157
137. Hulette C ND, McKeel D, Morris K, Mirras SS, Sumi SM, et. a. Clinical-neuropathologic findings in multi-infarct dementia: a re- portof six autopsied cases.Neurology 1997;48:668 – 672
138. Erkinjuntti T. Diagnosis and management of vascular cognitive impairment anddementia. J Neural Transm Suppl 2002:91-109
139. Hentschel F, Kreis M, Damian M, Krumm B. Microangiopathic lesions of whitematter: quantitation of cerebral MRI findings and correlation with psychological tests.Nervenarzt 2003;74:355-361
140. Metwally,MYM: Intracranial fusiform aneurysms, A report of 9 cases. Ain- shamsmedical journal, Vol 52, No 1,2,3 2001, 201-227 [Full text]
141. Salat DH, Tuch DS, Greve DN, et al. Age-related alterations in white mattermicrostructure measured by diffusion tensor imaging. Neurobiol Aging. 2005;26(8):1215–1227
142. Sullivan EV, Pfefferbaum A. Diffusion tensor imaging and aging. Neurosci BiobehavRev. 2006;30(6):749–761
33.Vernooij MW, de Groot M, van der Lugt A, et al. White matter atrophy and lesionformation explain the loss of structural integrity of white matter in aging. Neuroimage.2008;43(3):470–477
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
221

143. Vernooij MW, Ikram MA, Vrooman HA, et al. White matter microstructural integrityand cognitive function in a general elderly population. Arch Gen Psychiatry.2009;66(5):545–553
144. Charlton RA, Barrick TR, McIntyre DJ, et al. White matter damage on diffusiontensor imaging correlates with age-related cognitive decline. Neurology. 2006;66(2):217–222
145. O’Sullivan M, Jones DK, Summers PE, et al. Evidence for cortical “disconnection” asa mechanism of age-related cognitive decline. Neurology. 2001;57(4):632–638
146. Offenbacher H, Fazekas F, Schmidt R, et al. MR of cerebral abnormalitiesconcomitant with primary intracerebral hematomas. AJNR Am J Neuroradiol.1996;17(3):573–578
147. Scheid R, Ott DV, Roth H, et al. Comparative magnetic resonance imaging at 1.5 and3 Tesla for the evaluation of traumatic microbleeds. J Neurotrauma. 2007;24(12):1811–1816
148. Vernooij MW, Ikram MA, Wielopolski PA, et al. Cerebral microbleeds: accelerated3D T2-weighted GRE MR imaging versus conventional 2D T2-weighted GRE MR imagingfor detection. Radiology. 2008;248(1):272–277
149. Sehgal V, Delproposto Z, Haacke EM, et al. Clinical applications of neuroimagingwith susceptibility-weighted imaging. J Magn Reson Imaging. 2005;22(4):439–450
150. Vernooij MW, van der Lugt A, Ikram MA, et al. Prevalence and risk factors ofcerebral microbleeds: the Rotterdam Scan Study. Neurology. 2008;70(14):1208–1214
151. Poels MM, Vernooij MW, Ikram MA, et al. Prevalence and risk factors of cerebralmicrobleeds: an update of the Rotterdam scan study. Stroke. 2010;41(Suppl 10):S103–S106
152. Mesker DJ, Poels MM, Ikram MA, et al. Lobar distribution of cerebral microbleeds:the Rotterdam Scan Study. Arch Neurol. 2011;68(5):656–659
153. Qiu C, Cotch MF, Sigurdsson S, et al. Cerebral microbleeds, retinopathy, anddementia: the AGES-Reykjavik Study. Neurology. 2010;75(24):2221–2228
154. Poels MM, Ikram MA, Van der Lugt A, et al. Cerebral microbleeds are associatedwith worse cognitive function. The Rotterdam Scan Study. Neurology, in press.
155. Goos JD, Kester MI, Barkhof F, et al. Patients with Alzheimer disease with multiplemicrobleeds: relation with cerebrospinal fluid biomarkers and cognition. Stroke.2009;40(11):3455–3460
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
222

156. Poels MM, Ikram MA, van der Lugt A, et al. Incidence of cerebral microbleeds in thegeneral population: the Rotterdam Scan Study. Stroke. 2011;42(3):656–661
157. Goos JD, Henneman WJ, Sluimer JD, et al. Incidence of cerebral microbleeds: alongitudinal study in a memory clinic population. Neurology. 2010;74(24):1954–1960
158. .Small GW, Bookheimer SY, Thompson PM, et al. Current and future uses ofneuroimaging for cognitively impaired patients. Lancet Neurol. 2008;7(2):161–172
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
223

INDEX
INTRODUCTION
Periventricular white matterchanges (leukoaraiosis)
Cortical-Subcorticalabnormality
Watershed abnormality
Normal MRI
SUMMARY
INTRODUCTION
Most patients with TIAs have normal CT scans. The incidence of associated infarction asdemonstrated by CT has varied from 0 to 20% . These CT abnormalities have frequentlyconsisted of lacunae or more extensive ill-defined periventricular regions of decreaseddensity or watershed infarctions. The gray matter enhancement associated with corticalinfarction and cerebral dysautoregulation has been an infrequent finding. Other observedCT findings have been equally nonspecific, including ventriculomegaly and corticalatrophy.
The MRI is abnormal in 70% of cases with TIAs. All abnormalities seen by CT are alsovisualized by MRI. Moreover, MRI commonly visualized more extensive involvement thanis appreciated by CT. The MRI findings can be divided into four categories according totheir anatomical distribution and morphology as follows.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
224

Periventricular abnormality Cortical-subcortical
abnormality Watershed abnormality Normal MRI
Periventricular white matter changes (leukoaraiosis)
This category is composed of the oldest patients (average age 73.8 years) and had thehighest percentage of hypertensives (75%). Of all the groups , this group tended to have amore Polymorphic appearance, being combined on occasion with cortical and subcorticalabnormalities as well as extending into clear watershed zones. Abnormalities of theimmediate periventricular area, especially bordering the dorsolateral surfaces of theventricles, are relatively nonspecific since this region may be injured by a wide variety ofdisease states .
The diversity of possible causes (embolic, hemodynamic, andhypertensive) is present within this group. The incidence of acardiac history consisting of arrhythmias (chronic atrialfibrillation and ventricular arrhythmias), mitral annularcalcifications, and aortic sclerosis, as well as myocardialinfarction and angina is very low in this group. It is ofinterest that this group has the lowest degree ofhemodynamically significant carotid stenosis. TIAs andRINDS in this group is one of the clinical manifestations ofmicrovascular brain disease.
Figure 1. CT scan image showing leukoaraiosis
Although there are a diverse number of disease states that may cause these periventricularchanges, it seems apparent that the most common etiology would be the vascular changesassociated with hypertension. Such changes perhaps are best illustrated by a commondisease, namely, subcortical arteriosclerotic encephalopathy (SAE). SAE and the highincidence of lateral periventricular abnormalities encountered have been the topic of muchdebate. Although none of the patients in this group have a symptom complex composed ofdementia, stroke, gait disturbance, ventriculomegaly, or urinary incontinence it seemsreasonable to expect that SAE may initially present with TIA or reversible ischemicneurologic deficit (RIND). This group had the highest percentage of RIND symptoms.
Cortical-Subcortical abnormality
This is the largest Population of abnormalities found, representing 43% of all abnormalstudies. The average age of this group was 66.6 years, which is considerably lower than thatof the periventricular group. This group also had a relatively large percentage of
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
225

hypertensive individuals (61%). The incidence of a cardiogenic source for the emboli suchas atrial fibrillation, ventricular arrhythmias, prolapsed mitral valve, atherosclerotic heartdisease with angina, and recent myocardial infarction is low. The incidence of significantcarotid stenosis defined as greater than 80% by carotid ultrasound or angiography is alsovery low in this group. CT scans might be abnormal in this group demonstratingperiventricular lacunae or focal gray matter enhancement. This group has the lowestpercentage of recurrent TIAS. TIAs and RINDS in this group is one of the clinicalmanifestations of microvascular brain disease.
Watershed abnormality
This category has an average age of 70.3 years and, interestingly, the lowest percentage ofhypertension (58%), comparable to the cortical-subcortical group. All of these patientshave abnormalities lying in a deep posterior wedge distribution extending posteriorly anddorsally from the lateral ventricles. Some of them have abnormalities extending along thedorsolateral aspect of the lateral ventricles. Others have the abnormality extending alongthe cortex and subcortical region between the anterior and middle cerebral arteries.Abnormalities within watershed zones, within the cerebellum and between the distributionsof the posterior inferior and superior cerebellar arteries is occasionally demonstrated.Many of these patients have significant carotid stenosis with or without coronary arterystenosis. Myocardial infarctions or ventricular arrhythmias are occasionally present. Thisgroup has the highest percentage of multiple or recurrent TIAs (67%).
Normal MRI
This group has the youngest average age (58.6 years), the second highest percentage ofhypertensives (67%), and the second highest number of recurrent TIAS. incidence ofsignificant carotid disease or cardiac disease is very low.
SUMMARY
Type Incidence Age Carotidstenosis
Hypertension Possible aetiology
Periventricularwhite matterchanges(leukoaraiosis)
Common inEgypt
73.8 Lowincidence
75% Microvascular braindisease
Cortical-Subcortical
Common inEgypt
66.6 Lowincidence
61% Microvascular braindisease
Watershed Rare inEgypt
70.8 Highincidence
Low Carotid bifurcationdisease
Normal Common inEgypt
58.6 Lowincidence
76 % Microvascular braindisease
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
226

References
1. Bhatt DL, Kapadia SR, Yadav JS, Topol EJ: Update on clinical trials of antiplatelettherapy for cerebrovascular diseases. Cerebrovasc Dis 2000; 10 Suppl 5: 34-40.
2. Bots ML, van der Wilk EC, Koudstaal PJ, et al: Transient neurological attacks inthe general population. Prevalence, risk factors, and clinical relevance. Stroke 1997Apr; 28(4): 768-73.
3. Brown RD Jr, Evans BA, Wiebers DO, et al: Transient ischemic attack and minorischemic stroke: an algorithm for evaluation and treatment. Mayo Clinic Division ofCerebrovascular Diseases. Mayo Clin Proc 1994 Nov; 69(11): 1027-39.
4. Culebras A, Kase CS, Masdeu JC, et al: Practice guidelines for the use of imaging intransient ischemic attacks and acute stroke. A report of the Stroke Council,American Heart Association. Stroke 1997 Jul; 28(7): 1480-97.
5. Davalos A, Matias-Guiu J, Torrent O, et al: Computed tomography in reversibleischaemic attacks: clinical and prognostic correlations in a prospective study. JNeurol 1988 Jan; 235(3): 155-8.
6. Dyken ML, Conneally M, Haerer AF, et al: Cooperative study of hospital frequencyand character of transient ischemic attacks. I. Background, organization, andclinical survey. JAMA 1977 Feb 28; 237(9): 882-6.
7. Feinberg WM, Albers GW, Barnett HJ, et al: Guidelines for the management oftransient ischemic attacks. From the Ad Hoc Committee on Guidelines for theManagement of Transient Ischemic Attacks of the Stroke Council of the AmericanHeart Association. Circulation 1994 Jun; 89(6): 2950-65.
8. Forbes CD: Antiplatelet therapy for secondary stroke prevention. Scott Med J 1999Apr; 44(2): 54-9.
9. Gross SB: Transient ischemic attacks (TIA): current issues in diagnosis andmanagement. J Am Acad Nurse Pract 1995 Jul; 7(7): 329-37.
10. Gustafsson D, Elg M: The pharmacodynamics and pharmacokinetics of the oraldirect thrombin inhibitor ximelagatran and its active metabolite melagatran: amini-review. Thromb Res 2003 Jul 15; 109 Suppl 1: S9-15.
11. Henneman PL, Lewis RJ: Is admission medically justified for all patients with acutestroke or transient ischemic attack? Ann Emerg Med 1995 Apr; 25(4): 458-63.
12. Johnston SC, Gress DR, Browner WS, Sidney S: Short-term prognosis afteremergency department diagnosis of TIA. JAMA 2000 Dec 13; 284(22): 2901-6.
13. Landi G: Clinical diagnosis of transient ischaemic attacks. Lancet 1992 Feb 15;339(8790): 402-5.
14. Lanska DJ: Review criteria for hospital utilization for patients with cerebrovasculardisease. Task Force on Hospital Utilization for Stroke of the American Academy ofNeurology. Neurology 1994 Aug; 44(8): 1531-2.
15. Shiozaki T, Hayakata T, Taneda M, et al: A multicenter prospective randomizedcontrolled trial of the efficacy of mild hypothermia for severely head injuredpatients with low intracranial pressure. Mild Hypothermia Study Group in Japan. JNeurosurg 2001 Jan; 94(1): 50-4.
16. Worrall BB, Johnston KC: Antiplatelet therapy in secondary stroke prevention.Curr Atheroscler Rep 2000 Mar; 2(2): 104-9.
17. Zweifler RM: Management of acute stroke. South Med J 2003 Apr; 96(4): 380-5.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
227

INDEX
BERRY ANEURYSMS
PATHOGENESIS OF BERRYANEURYSMS
PERIPHERAL ANEURYSMS
MULTIPLE ANEURYSMS
COMPLICATION OFINTRACRANIAL ANEURYSMS
o HAEMATOMA
o INFARCTION
o HERNIATION
o HYDROCEPHALUS
CAROTID-CAVERNOUSANEURYSMS
VASCULAR ECTASIA (FUSIFORMANEURYSMS)
228

BERRY CEREBRAL ANEURYSMS
By far the most commonly encounteredlesion of all is the congenital saccular orberry aneurysm, arising from the circleof Willis and the medium-sized arteriesalong the base and infoldings of thebrain. Pathologic studies then formedthe basis for most of the investigationsconcerning aneurysms for more than100 years. Angiography has given moreinformation about the importance ofaneurysms and the complications oftheir rupture in living subjects.
Figure 1. COMMON ANATOMICAL SITESOF BERRY ANEURYSMS
Location IncidenceAnteriorcerebral
Anterior cerebral 5%,anterior communicating 25%
Internal carotid Ophthalmic 4%,posterior communicating 18%,bifurcation 4%Middlecerebral
25%
Posteriorcerebral
2%
Basilar Bifurcation [tip] 7%,trunk 3%Vertebral,PICA
3%
Professor Yasser Metwallywww.yassermetwally.com
229

Pathogenesis of aneurysms
The theory that intracranial aneurysms originate because of developmental defects inarterial walls is widely accepted. It is also generally recognized that an aneurysm is usuallyfound in the fork between two arterial branches. At a point of normal branching, the wallbetween the two limbs opposite the channel of the undivided vessel usually contains theaverage amount of muscular and elastic tissue in the tunica media. In addition, there areextra layers of intimal cells in the fork usually referred to as "intimal pads." A collar-likeintimal pad is also present proximal to the point of bifurcation of an artery In the cerebralvessels of man, the tunica media is often defective at the fork of a dividing vessel,containing less smooth muscle than in an average normal artery and also having poorlydeveloped elastic fibers. The finding of such medial defects constitute the bases for thedevelopment of aneurysms.
Figure 2. A, "Berry" or saccular aneurysm, posterior cerebral artery., B, Rupturedsaccular or berry aneurysm, anterior cerebral artery.
In addition to the basic anatomic defects, the age of the patient and arterial hypertensionare important factors in the initiation, growth, and rupture of cerebral berryaneurysms.With advancing age, elastic degeneration gradually increases. The degenerationappears first beneath the intimal pads around the arterial bifurcation, then in the moresuperficial lastica over the medial defects, finally becoming diffuse along the arterialtrunks. Approximately two-thirds of patients with ruptured aneuryms have hypertension.large medial defects are found to be much commoner at middle cerebral arterial forks thanat other sites, apparently accounting for the greater frequency of aneurysms at the middlecerebral bifurcation than elsewhere. Aneurysms may also develop at sites of arterial
Professor Yasser Metwallywww.yassermetwally.com
230

fenestration, when there is forking and then rejoining of a vessel not normally divided .Tunica media defects are frequently found in the forks of a fenestration.
Figure 3. Elastic stain to show defectin wall of "berry" or saccularaneurysm.
There has been considerable misunderstanding about the frequency of occurrence ofaneurysms at various sites because some think in terms of aneurysms of clinical importancethat have ruptured or caused neurological changes while others think in terms of totalincidence. If all aneurysms are considered, both ruptured and un ruptured, then themiddle cerebral bifurcation is the most common site for aneurysms to be found. Aneurysmsarising from the internal carotid artery, at the site of origin of the posterior communicatingartery, are the second most frequent.
Professor Yasser Metwallywww.yassermetwally.com
231

Figure 4. Angiography showing a posterior communicating artery aneurysm
An almost equal percentage applies to the forks between the anterior communicatingartery and the two anterior cerebral arteries. The fourth most common location is at thebifurcation of one of the carotid arteries into the anterior and middle cerebral arteries.Together, these four locations (middle cerebral, posterior communicating, anteriorcommunicating, and carotid bifurcation) account for 90% of berry aneurysms. Thedistribution of the remaining 10% comprises the basilar bifurcation (2%), the vertebralartery at the posterior inferior cerebellar arterial origin (2%), lesions of the basilar trunkprobably arising at the site of origin of one of the Pontine branches or an "experimentalvessel" (1%), distal anterior or middle cerebral artery (2%), and the proximal and distalportions of the posterior cerebral artery (3%).
Professor Yasser Metwallywww.yassermetwally.com
232

Figure 5. A,B Posterior communicating berry aneurysms, C, Anterior communicatinganeurysms
As noted above, only the minority of aneurysms rupture. The location of an aneurysmaffects the probability of its bleeding. Anterior communicating aneurysms, for example,carry the highest risk for the production of a subarachnoid hemorrhage. An aneurysm atthe site of origin of the posterior communicating artery has the second highest probabilityof bleeding among the more frequently occurring lesions, the rare peripheral aneurysmshaving a slightly higher bleeding tendency. The responsibility for a subarachnoidhemorrhage is attributable to anterior and posterior communicating aneurysms in a highpercentage of cases, this depicts not only the anatomic distribution of berry aneurysms butthe probability of an individual aneurysm having bled if there are two or more lesionspresent in different locations.
Figure 6. Aneurysm at the posterior inferior cerebellar artery
Professor Yasser Metwallywww.yassermetwally.com
233

Aneurysms have certain features in common and yet they are all different, with regard totheir shape, size, and to a lesser extent their direction of growth. It is important to assessangiographically the orifice or mouth of the aneurysm, the neck or cervical portion formedby the proximal third of the sac, the body or middle third, and the fundus or apex of thelesion. The vast majority of aneurysms rupture through the apex. Perhaps 10% rupturelaterally from the body of the sac, whereas a rupture through the neck is rare.
Figure 7. Multiloculated berry aneurysm filled by a blood clot, in general an aneurysm hasa neck, body and a fundus.
Size is also important in the assessment of rupture. The great majority of aneurysmsrupture when they are between 5 and 15 mm in diameter. It is unusual for an aneurysmless than 4 mm in its smallest diameter to produce a subarachnoid hemorrhage. Largermultiloculated aneurysms are much more likely to rupture than the smaller unilocularlesions; however, size is more important than multiloculation. Many unrupturedaneurysms also have more than one loculus at their domes. The presence of multiple apicesor secondary bubbles or pseudopods on the surface is indicative of the pattern of pastgrowth of the aneurysm but does not predict its future prospect for rupture. In addition,some loculations are caused by external structures crossing the aneurysm rather thanchanges in the wall of the lesion.
Professor Yasser Metwallywww.yassermetwally.com
234

PROBABILITY OF ANEURYSMAL RUPTURE AND BLEEDING
Factor CommentSite Anterior communication artery aneurysms, followed by the posterior
communicating artery aneurysms carry the highest probability for rupture andbleeding than other aneurysms
Size Larger multiloculated aneurysms are more likely to rupture and bleed thansmaller aneurysms with a single locule. Increase in the size of the aneurysm orthe development of more loculations greatly increase the likelihood of ruptureand bleeding
Location Proximal aneurysm are more likely to rupture than distal one
When an intracranial aneurysm ruptures, it may do so suddenly and completely. Bloodescapes from its lumen, leading to what is termed clinically "spontaneous subarachnoidhemorrhage." The blood may pass only into the subarachnoid space, or it may pass partlyinto the brain substance and partly into the subarachnoid space. The blood may, onoccasion, be entirely within the cerebral substance, forming an intracerebral hematoma.Some aneurysms, upon rupturing, tear the arachnoid and an accumulation of blood may befound in the subdural space as well as in the subarachnoid space. Aneurysms of theanterior communicating and middle cerebral arteries are often associated with anintracerebral hematoma.
Figure 8. Anterior communicating artery aneurysm hemorrhage. Axial CT scan showstypical subarachnoid hemorrhage from rupture of anterior communicating arteryaneurysm. Hemorrhage is present in the septal region (arrows). B, Ruptured anteriorcommunicating aneurysm causing intraventricular and interfrontal haemorrhage
Professor Yasser Metwallywww.yassermetwally.com
235

An aneurysm may also rupture with extravasation of blood through the intima but notbeyond the wall of the vessel. At other times a local thinning and bulging of the wall mayoccur without intramural hemorrhage; in this way the pseudopods or multiloculations ofthe surface are produced. In these cases the size of the aneurysmal sac increases rapidlyand the patient may complain of headache, or there may be involvement of the cranialnerves which are adjacent to the aneurysm .
Figure 9. Ruptured middle cerebralartery aneurysm with hemorrhageinto brain parenchyma.
Cerebral angiograms carried out as soon as the patient is brought into the hospital usuallyshow the aneurysm, and only rarely has the contrast material been seen to spurt out of theruptured sac. In this particular instance, it is possible that angiography may havecontributed to the second rupture of the aneurysmal sac. For the most part, however,cerebral angiography does not appear to cause significant deterioration of the patient'scondition when carried out at almost any stage of the clinical course .
It is very common to see arterial spasm in the region of a ruptured aneurysm. It iscommon, also, for all of the major vessels on the side of the lesion to be involved by spasmwith poor filling of minor branches. Spasm may be seen affecting the carotid systemsbilaterally, and the basilar branches as well when diffuse spasm is present; however, itoften is most severe in the neighborhood of the bleeding lesion. In occasional cases spasmmay be seen only contralateral to a ruptured aneurysm. Severe, localized spasm is oneuseful feature in deciding which aneurysm has bled, when more than one aneurysm ispresent . In cases where intracerebral bleeding has occurred and a localized hematoma hasbeen formed, the usual signs of a mass may be encountered in the angiogram. Aneurysmsof the anterior cerebral-anterior communicating artery junction rupture, not uncommonly,into the medial portion of the contralateral frontal lobe. Lesions of the medial cerebralsurface elsewhere, not adjacent to the falx, may adhere to the opposite hemisphere andrupture contralateral to their origin.
Professor Yasser Metwallywww.yassermetwally.com
236

Figure 10. Ruptured aneurysm with subarachnoidhemorrhage.
Arterial narrowing indicative of spasm is seen predominantly in the first 3 weeks afterbleeding of ruptured intracranial aneurysms and it is maximal between 6 and 12 days.Thereafter, the incidence of spastic narrowing decreases .
Spasm is much less common in patients over 50 years of age and its absence is possibly amanifestation of arteriosclerosis. From the above it is evident that the presence of spasmand an avascular mass are most important in assessing aneurysms in patients withsubarachnoid hemorrhage. In addition, the size of an aneurysm, especially an increase insize between two observations, and, in some cases, the configuration of the sac are helpfulin diagnosis.
Peripheral Aneurysms
Lesions arising from the secondary or tertiary branching or branches of the major cerebralarteries can be considered peripheral. Such an aneurysm may be congenital in origin. Theymay also be the result of embolism and trauma.
The peripheral congenital aneurysms are usually found at secondary or tertiary branchingof the anterior and posterior cerebral arteries. For some reason, they are not as frequentlyseen along the distal segments of the middle cerebral artery. The lesions are saccular intype and have the other features frequently observed with berry aneurysms of the circle ofWillis. Large aneurysms are seldom seen peripherally. Most often such lesions attain a sizeof 5 to 6 mm in diameter, which are their average proportions when the patient is seen witha subarachnoid hemorrhage. There would appear to be a very strong tendency for suchcongenital peripheral lesions to bleed; they are seldom seen as an incidental finding inpatients with brain tumors, or with aneurysms elsewhere that have bled.
Embolic aneurysms may be either infective or neoplastic. The middle cerebral arterialbranches are most commonly affected. Before the advent of antibiotics, mycotic aneurysmsaccounted for at least 5% of intracranial aneurysms. Delayed or inadequate treatment ofbacterial endocarditis is now associated with most cases, although such lesions can occur in
Professor Yasser Metwallywww.yassermetwally.com
237

drug addicts. Of the patients who have active subacute bacterial endocarditis, one-thirdhave visceral emboli and one-half of the latter are to the brain. Congenital cardiac lesionsmay be complicated by infection and result in septic emboli lodging in distal cerebralarterial branches.
In many cases, hemorrhage from a mycotic intracranial aneurysm leads to death; it is notunusual for such a patient to have no clinically recognizable embolic episode preceding thehemorrhage. At other times, however, patients with bacterial endocarditis have neurologicproblems of strokes or meningoencephalitis when first seen. If an embolic episode isrecognized, angiography after an appropriate interval is advocated. From the bestinformation available, it would appear that if a mycotic aneurysm develops, approximately3 weeks elapse between the septic embolism and rupture of the aneurysm.
A local arteritis with destruction of the vessel wall and the development of a false aneurysmis the usual sequence. Such aneurysms are remarkably round in shape and they rarelyattain a diameter of more than 5 mm before bleeding ensues. Since the hemorrhage fromsuch a destructive vascular lesion may be fatal, or a secondary infection with meningitis ora brain abscess may develop, the lesions are usually treated by surgically .
Occasionally, a sizable group of neoplastic cells will metastasize as an embolus and lodge inone of the smaller cerebral vessels. Such tumor cells often come from malignant pulmonarylesions but, occasionally, a benign intracavitary tumor of the heart, a cardiac myxoma, maybe the cause. The tumors, the majority of which arise in the left atrium, frequentlyembolize and approximately one-half of the emboli are cerebral. The myxomatous embolicause arterial occlusions and damage to the walls of the vessels. Cerebral infarction andhemorrhage are common complications. The embolic myxomatous cells invade and destroythe normal elements of arterial walls and because their growth is slow, and accompaniedby connective tissue proliferation, false aneurysms may develop.
Occasionally, somewhat similar findings may be encountered in the primary arteritis oflupus erythematosus or the secondary arteritis of bacterial meningitis and mycoticembolism .
Multiple Aneurysms
Approximately one-third of patients with aneurysms have multiple lesions. The greatmajority of these patients have two aneurysms.
It is important to be able to identify a bleeding aneurysm among multiple lesions in orderto avoid a delay in proper treatment or the institution of inappropriate treatment. Inpatients with multiple aneurysms the problem of finding angiographic clues as to whichaneurysm has caused the subarachnoid hemorrhage may arise when there are noneurologic findings to localize the hemorrhage. Through a radiologic-pathologic correlativestudy of a large number of cases of multiple aneurysms, well documented anatomically, itwas found possible to identify the ruptured aneurysm from the angiogram in 95% ofinstances. In 83% of the patients, it was found that, on the basis of major vascular
Professor Yasser Metwallywww.yassermetwally.com
238

displacements, caused by a large hematoma, or the combination of a smaller displacementand spasm, the site of hemorrhage could be identified. When an aneurysm is isolated onone main cerebrovascular system apart from a second aneurysm or other aneurysms, itmay be identified as the lesion that ruptured if there are lateralizing angiographicchanges.These would include a generalized vascular dislocation by the mass of a largehematoma, usually manifested as a midline shift or a middle cerebral artery elevation ordeformity. The situation of two aneurysms, one located on one major vascular system andthe other on another, will pertain approximately one-half of the time. In an additionalalmost 10%, more than two aneurysms will be found arranged so that the rupturedaneurysm is on one side, whereas the unruptured aneurysms are contralateral Thus, inapproximately 60% of instances, the anatomic relationships are such that if angiographiclateralization of a subarachnoid hemorrhage to the side of an isolated aneurysm is possible,this is tantamount to identification of the aneurysm that ruptured. When a rupturedaneurysm is situated on the same cerebrovascular system as other unruptured lesions,correct diagnosis is dependent upon more sharply localizing angiographic changes. Thefinding in combination of a minor mass effect of a small hematoma and localized vascularspasm of moderate to marked severity usually constitutes reliable evidence for identifyingthe aneurysm that has caused a subarachnoid haemorrhage.
A posterior communicating aneurysms is a common cause of third nerve palsy. Theaneurysms often grow backward and downward from their origin in the fork of theinternal carotid and posterior communicating vessels. Such an extension causescompression of the oculomotor nerve as it passes from the subarachnoid space into thelateral wall of the cavernous sinus, the piercing of the dura occurring between the anteriorand posterior clinoid processes. Since the oculomotor nerve is superior to the other orbitalnerves, it is the neural structure most often affected by enlarging unruptured aneurysms inthis area.
COMPLICATIONS OF CEREBRAL ANEURYSMS
The volume of blood that extravasates when an intracranial aneurysm ruptures isrelatively small in comparison with the hemorrhages from aneurysms in other parts of thebody. The acute appearance of blood in the subarachnoid space is not, in itself, a threat tolife. On the other hand, death may rapidly ensue when there is trauma to important centersin the brain by a rapidly dissecting hemorrhage. Complications more often occur laterowing to the secondary compression and displacement effects of a hematoma, theprolonged occurrence of cerebral ischemia leading to infarction or the development of bothhematoma and infarction. Infarction, through the development of associated edema, mayproduce a mass effect which at times can induces herniation .
Hematoma
The rupture of approximately two-thirds of cerebral aneurysms results in the formation ofhematomas which may be large or small. In less than one-half of patients in whom anintracerebral hematoma develops, the lesion is caused by a direct dissection of blood intothe cerebral substance from the ruptured aneurysm. In the majority of the cases there is
Professor Yasser Metwallywww.yassermetwally.com
239

first an extravasation into the subarachnoid space with subsequent or indirect dissectioninto the cerebral substance. In a small number of patients (2%) the rupture of an aneurysmmay be accompanied by tearing of the arachnoid, with direct hemorrhage into the subduralspace or dissection of subarachnoid blood between the arachnoid and dura mater . Manypatients with ruptured aneurysms have hematomas that remain confined to thesubarachnoid space, where they produce the effects of a localized extracerebral mass.
Figure 11. Massive subarachnoid hemorrhage
Certain patterns of subarachnoid hematoma formation and of intracerebral dissection arefound with aneurysms in specific locations. These patterns have been worked outpathologically and can be recognized by angiography, as described below. However, it isnow more satisfactory to diagnose and follow intracerebral hematomas by the atraumatictechnique of computerized tomography, once the cause of bleeding has been established.
Figure 12. Ruptured aneurysm with subarachnoidhemorrhage.
Aneurysms of the anterior communicating artery are not only responsible forsubarachnoid hemorrhage more often than lesions at any other single site, but the ruptureresults in an intracerebral hematoma more often than with lesions at other sites. Inferiorfrontal or olfactory hemorrhages may dissect upward, and break into a frontal horn of theventricular system.
Professor Yasser Metwallywww.yassermetwally.com
240

Figure 13. Subarachnoid hemorrhage
At other times an anterior communicating artery aneurysm may rupture into thesubarachnoid space between the medial surfaces of the frontal lobes and form aninterfrontal subarachnoid hematoma. Such hematomas may dissect upward into theseptum pellucidum, often distending the potential cavum between the layers of the septumpellucidum. At any point the dissecting subarachnoid hematoma may burst into thesubstance of the frontal lobe or into the ventricular system.
The anterior cerebral artery aneurysms are the most likely to rupture
Figure 14. A, ruptured anteriorcommunicating aneurysm inducinginterfrontal and intraventricularhaematoma, B, ruptured anteriorcommunicating aneurysm inducingcallosal haematoma. Notice thebilateral medial frontal anteriorcerebral artery infarction, mostly dueto vasospasm.
Anterior communicating artery aneurysms are also the most common lesions to produceinjury of the hypothalamus. Less frequently, extension of an interfrontal hematoma maypass around the corpus callosum to form a hematoma in the callosal sulcus or in theintercingulate region. Dissection into the corpus callosum itself may take place andoccasionally and intracerebral hematoma developing primarily in the frontal lobe, orextending into it from the subarachnoid space, may dissect laterally into the external
Professor Yasser Metwallywww.yassermetwally.com
241

capsule. Aneurysms of an anterior cerebral artery distal to the circle of Willis producehematomas in the proximity of the lesion.
Figure 15. Anterior communicating artery aneurysm hemorrhage. Axial CT scan showstypical subarachnoid hemorrhage from rupture of anterior communicating arteryaneurysm. Hemorrhage is present in the septal region (arrows). B, Ruptured anteriorcommunicating aneurysm causing intraventricular and interfrontal haemorrhage
Figure 16. Ruptured anteriorcommunicating aneurysm inducinginterfrontal and intraventricularhaematoma. Notice the bilateralmedial frontal anterior cerebralartery infarction, mostly due tovasospasm.
The more proximal anterior cerebral aneurysms most often rupture into the frontal lobesubstance, whereas the more peripheral aneurysms produce hematomas in the callosalsulcus or in the intercingulate fissure.
Aneurysms extending upward and forward from the bifurcation of the internal carotidartery often are imbedded in the frontal lobe and rupture directly into its substance; thencethe hematoma may burst into a frontal horn of a lateral ventricle. Aneurysms at thebifurcation that extend backward and upward may rupture into the hypothalamic nucleior through the lamina terminalis into the third ventricle.
Professor Yasser Metwallywww.yassermetwally.com
242

Aneurysms of the cerebral segment of the internal carotid artery, which usually arise at thesite of origin of the posterior communicating artery and extend backward, most oftenrupture into the anterior temporal lobe substance, thence into the temporal horn. At othertimes, a subarachnoid hematoma may develop above the uncus and dissect along thechoroidal fissure into a temporal horn. The hemorrhage may also extend beneath theuncus. Bleeding from the fundus of a forward pointing aneurysm may result in asubarachnoid collection beneath the frontal lobes.
Middle cerebral artery aneurysms often result in the formation of ahematoma deep in the Sylvian fissure over the central lobe or islandof Reil. Such Sylvian hematomas then may dissect into the externalcapsule There also may be direct rupture into the external capsule orinto the frontal or temporal lobe. A hematoma may dissect forwardfrom the external capsule or from the frontal horn of a lateralventricle. At other times there may be dissection backward from theexternal capsule or temporal lobe with rupture into the atrium of alateral ventricle.
Figure 17. Left sylvian haematoma
Figure 18. Ruptured middlecerebral artery aneurysmwith hemorrhage into brainparenchyma.
Correlating well with the pathologic changes described above, the frontal carotidangiogram may display following features denoting hematoma formation from rupture ofan anterior communicating artery aneurysm, an aneurysm of the carotid bifurcation, or ananeurysm of the ending portion of the anterior cerebral artery : (a) elevation of theproximal transverse limb of an anterior cerebral artery when a hematoma occurs in thesubfrontal region; (b) lateral bowing of the proximal ending portions of the anteriorcerebral arteries caused by a frontal intracerebral hematoma (in the case of anteriorcommunicating artery aneurysms that point toward the opposite hemisphere from whichthey arise, there may be cross-frontal rupture and ipsilateral bowing of the anteriorcerebral arteries); (c) widening of the space between the anterior cerebral arteries owing toseparation by an interfrontal hematoma in the subarachnoid space.
Professor Yasser Metwallywww.yassermetwally.com
243

The corresponding lateral angiogram may reveal, as a result of rupture of an aneurysm ofthe anterior communicating artery, a lesion of the carotid bifurcation or a forwardpointing aneurysm of the supraclinoid portion of the internal carotid artery, (a) backwardbowing of the cerebral segment of the internal carotid artery or "closure" of the carotidsiphon caused by a subfrontal or inferior intrafrontal hematoma; (b) elevation of theforward extending segment of the anterior cerebral artery, corresponding to the changeshown in the proximal transverse limb in the frontal view; (c) depression of the pericallosalartery if there has been dissection of a subarachnoid hematoma over the corpus callosuminto the callosal sulcus or intercingulate area. If an aneurysm situated distally on ananterior cerebral artery ruptures into the corpus callosum, or if a subarachnoid hematomadissects into this structure, the arc of the pericallosal artery may be widened or there maybe a localized elevation of this vessel. Differentiation from the wide anterior cerebral sweepof hydrocephalus may be made if there is a normally inclined thalamostriate vein. If thereis a subarachnoid hematoma between the corpus callosum and cingulate gyri or in theintercingulate fissure, the pericallosal arteries may be depressed.
Aneurysms of the internal carotid artery that project and rupture backward and rupturedaneurysms at the division of the middle cerebral artery may exhibit in the frontalangiogram, as a result of hematoma formation: (a) widening of the angle formed by thesupraclinoid portion of the carotid artery and the proximal portion of the middle cerebralartery due to the presence of a subtemporal or anterior Sylvian hematoma; (b)displacement of the anterior choroidal artery by a hematoma lateral or medial to thisstructure or as a result of tentorial herniation; (c) a deformity of the orderly columnararrangement of the middle cerebral branch loops over the island of Reil if a subarachnoidhematoma of the Sylvian fissure is present or if there is a hematoma in the externalcapsule. Of particular importance is the effect of a subarachnoid hematoma on the medialor lateral lenticulostriate arteries, or the anterior perforating ganglionic arteries. Suchhematomas produce obliteration of the perforating arteries at the point where they passthrough the pia with the result that their subarachnoid course is seen for a few millimetersin the angiogram, followed by an abrupt termination of the shadows, often along an almoststraight line.
In the lateral angiogram internal carotid artery aneurysms that rupture backward andbleeding lesions of the middle cerebral bifurcation that produce hematomas exhibit a lossof undulation, flattening, straightening, or bowing of the anterior choroidal artery,depending upon the exact location of the hematoma in relation to the vessel. When asubuncal hematoma is present, the anterior choroidal artery is elevated. A Sylvianhematoma will produce deformity of the orderly triangular arrangement of the middlecerebral arterial branches over the island of Reil. The looped arrangement is obliteratedwith straightening, stretching, and separation of the middle cerebral branches, if thehematoma is anterior. Rostral displacement and crowding of the branches may be shown ifa posterior Sylvian hematoma is present. The deformity of the Sylvian triangle isaccentuated by the presence of a hematoma in the external capsule.
Professor Yasser Metwallywww.yassermetwally.com
244

Figure 19. A CT scan revealing a rightfrontotemporal hematoma secondary to a rightMCA aneurysm rupture.
Figure 20. A CT scan revealinginterhemispheric and bilateral (right–left)inferior frontal lobe hematomas secondary toan ACoA aneurysm rupture.
Professor Yasser Metwallywww.yassermetwally.com
245

Figure 21. A CT scan revealinga left temporal lobe hematomasecondary to rupture of a leftPCoA aneurysm rupture.
Aneurysms at the rostral end of the basilar artery may rupture directly into the thirdventricle, the lesions often being imbedded in the structures forming the posterior portionof the ventricular floor. At other times a hematoma may form in the cisternainterpeduncularis. Such a subarachnoid hematoma may then dissect caudal into themidbrain and pons, following the course of perforating branches of the basilar andposterior cerebral arteries. A posterior inferior cerebellar aneurysm may produce ahemorrhage in the brainstem and in the subarachnoid cisterns. Some posterior inferiorcerebellar aneurysms are peripheral in position and produce a cerebellar hematoma in theproximity of the lesion.
Site of Ruptured Aneurysm
The most frequent site of aneurysm rupture in patients with an associated hematoma was theMCA (38% of patients) followed closely by the ACoA (36% of patients). The incidence of ahematoma was higher in patients with MCA (56%) and distal ACA aneurysms (50%), and it waslower in patients with ICA (24%) and PCoA aneurysms (15%). Intracerebral hematomas werevery rare in patients with VBA aneurysms (1%).
Professor Yasser Metwallywww.yassermetwally.com
246

Relationship Between Aneurysm Site and Hematoma Location
The types of ICH can classified into seven groups according to CT findings on admission: 1)frontal; 2) temporal, 3) sylvian; 4) basal ganglia; 5) interhemispheric; 6) callosal; and 7)cerebellar.
The location of the ICH is related to the location of the ruptured aneurysm. In patients with MCAaneurysms, the sylvian fissure was by far the most common location for hematoma occurrence.Frontal and temporal lobe hematomas also occurred in patients with MCA aneurysms (Fig. 9). Inpatients with ACoA aneurysms, frontal lobe hematomas occurred most frequently along withseveral cases of interhemispheric clots (Fig. 10). Temporal lobe hematomas were most frequentin patients with PCoA aneurysms (Fig 11). In patients with distal ACA aneurysms, ICHs weremost commonly frontal and callosal in a typical butterfly-type pattern (Fig. 12). In patients withICA aneurysms hematomas were most often found in the temporal lobe but were also associatedwith basal ganglia hematomas (Fig. 13) and one sylvian clot. Only one patient experienced ahematoma (fourth ventricle/cerebellar) that occurred in conjunction with a VBA aneurysm.
It is generally accepted that the second bleeding of an aneurysm is more apt to result inserious complications, or even a terminal event, than is the first rupture. One importantreason for the more serious prognosis is the fact that a second rupture usually occursdirectly into the brain substance, owing to the fact that the first hemorrhage producessubarachnoid adhesions in the neighborhood of the aneurysm or the development ofadhesions binding the sac of the aneurysm to the pia mater. In a high percentage of fatalintracerebral hemorrhages there is bleeding into the ventricular system. Under suchcircumstances, the ventricles may become rapidly distended with blood, which is evident onCT scan, MRI or in the venous phase of the angiogram, especially if there is impairment ofdecompression by adhesions about the foramina of the fourth ventricle and in the basalcisterns.
Professor Yasser Metwallywww.yassermetwally.com
247

Figure 22. A CT scan revealing abutterfly-pattern interhemispherichematoma secondary to rupture of adistal ACA aneurysm
Professor Yasser Metwallywww.yassermetwally.com
248

Figure 23. A CT scan revealing atemporal lobe/basal gangliahematoma (with ventricularextension) secondary to an ICAaneurysm rupture.
Table 1. Hemorrhage sites after aneurysmal rupture
ARTERY SITE OF HAEMORRHAGEANTERIORCOMMUNICATINGARTERY ANEURYSM
1-Inferior frontal, olfactory hemorrhage that may dissect intothe frontal lobes or hypothalamus
2-Interfrontal hemorrhage that may dissect into septumpellucidum, corpus callosum or intercingulate area
INTERNAL CAROTIDANEURYSM
Frontal lobe hemorrhage.
POSTERIORCOMMUNICATINGARTERY ANEURYSM
Anterior temporal lobe hemorrhage that may dissect intotemporal horns
MCA ANEURYSM Sylvian fissure haematoma that may dissect into the externalcapsule
BASILAR TIP ANEURYSM Commonly rupture into the third ventricle, pons, midbrain orcisterna interpeduncularis
PICA ANEURYSM Brain stem or cerebellar haematoma
Professor Yasser Metwallywww.yassermetwally.com
249

Infarction
Cerebral infarction is a more common fatal complication of the rupture of an intracranialaneurysm than intracerebral hematoma formation associated with ruptured aneurysms, Itis commonly pale and ischemic, not hemorrhagic in type. Cerebral infarction occurs mostoften after the rupture of aneurysms (1) of the internal carotid artery where the posteriorcommunicating vessel originates, (2) of the middle cerebral artery, (3) of the anteriorcommunicating artery, and in that order of frequency. The order is just the reverse of thatfound for intracerebral hematomas, Aneurysms at the origin of the posteriorcommunicating artery produce infarction over a wider area than other aneurysms,probably because they are more proximal on the carotid arterial vascular tree. Theinfarcted area is most often found in the distribution of the middle cerebral artery, which isthe main continuation of the internal carotid. The rupture of aneurysms at the posteriorcommunicating level also produces more ganglionic infarcts than aneurysms at other sites.Bilateral infarction occurs frequently after the rupture of aneurysms of the anteriorcommunicating artery. Such infarction is usually in the cortical distribution of the anteriorcerebral arteries and, although the survival rate is relatively high, many patients exhibitmental changes.
Table 2. Infarction sites after aneurysmal rupture
Aneurysmal site Infarction sitePosteriorcommunicatingartery aneurysm
1. Aneurysms at the origin of the posterior communicatingartery produce infarction over a wider area than otheraneurysms, probably because they are more proximal on thecarotid arterial vascular tree. The infarcted area is most oftenfound in the distribution of the middle cerebral artery, whichis the main continuation of the internal carotid.
2. The rupture of aneurysms at the posterior communicatinglevel also produces more ganglionic infarcts than aneurysmsat other sites.
Internal carotidartery aneurysm
Massive middle cerebral artery infarction.
Anteriorcommunicationartery aneurysm
Bilateral infarction occurs frequently after the rupture of aneurysmsof the anterior communicating artery. Such infarction is usually inthe cortical distribution of the anterior cerebral arteries.
There appear to be three overriding angiographic observations that can be made in thepresence of cerebral infarction, or in anticipation of an impending infarction. Recognitionof these changes may be of the utmost importance in making decisions concerningtreatment.
Professor Yasser Metwallywww.yassermetwally.com
250

1. Spasm. Infarction occurs most often along the distribution of the artery bearing aruptured aneurysm, and in many cases this is the result of prolonged spasm of the vessel.The possibility of infarction is always suggested when there is severe localized narrowing ofthe lumen, usually seen in the immediate vicinity of the ruptured aneurysm; it may alsooccur when there is only mild diffuse spasm.
2. Atherosclerosis. The existence of atherosclerosis may be an important contributingfactor to the development of infarction as a complication of hemorrhage from ananeurysm. Infarction is more probable if blood flow in a cerebral vessel is reduced bystenosis of a large atheromatous plaque.
3. Hematoma. The more common angiographic changes denoting the presence ofintracerebral or subarachnoid hematomas are described above. Subarachnoid hematomasapparently produce infarction more often by pressure on vessel while intracerebralhematomas cause early and marked spasm. Although it is possible to differentiate asubarachnoid from an intracerebral hematoma by CT scan or MRI, angiographic clues areoften found, such as elevation of the anterior choroidal artery by a subuncal hematoma,widening of the space between the anterior cerebral arteries by an interfrontal mass, or theproduction of a local deformity of the pericallosal artery by a supracallosal collection. Themost common subarachnoid hematoma to produce infarction along the arborization ofadjacent vessels occurs after rupture of an anterior communicating artery aneurysm.Other observations that can be made from angiograms do not appear to have nearly asgreat a significance as spasm, atherosclerosis, and hematoma formation.
Anomalies of the circle of Willis, the dominance of one side over the other in blood flowthrough the circle, and the overall circulation rate are not often of great value inanticipating or predicting the development of infarction. Computerized tomography is veryuseful in diagnosing cerebral infarction secondary to spasm. The infarction may or may notbe associated with angiographic signs of infarction such as vascular occlusion or earlyfilling veins, and only spasm may be present; but the computerized tomography scan [CTscan or MRI] demonstrate the typical findings of cerebral infarctions .
Herniation
The development of a herniation may be a critical event, regardless of where it occurs.Acute herniations follow most often the rapid development of massive intracerebral,intraventricular or subdural hematomas,or massive infarction associated with significantoedema .
The subfalcine herniations occurring with hematomas and infarction are similar to thosecommonly seen in association with tumors. The anterior cerebral arteries and theirbranches and the deep cerebral veins are the structures usually displaced to the greatestextent. In some cases hematomas may not only produce generalized or localizeddisplacement of the internal cerebral and basal veins but may also deform the septal andSylvian veins. Other cerebral hernias that may be seen in supratentorial tumours are notencountered in connection with rupture of aneurysms of the carotid system. In some
Professor Yasser Metwallywww.yassermetwally.com
251

instances, however, hematomas that form along the course of the vertebral-basilar systemmay cause an upward transtentorial herniation or a downward herniation at the foramenmagnum.
Figure 24. Subfalcine herniation (arrows). Subfalcial herniation is displacement of thecingulate gyrus from one hemisphere to the other, under the falx cerebri. Subfalcialherniation can compress the pericallosal arteries, causing an infarct in their distribution.
Hydrocephalus
A sizable number of patients who have a subarachnoid hemorrhage develophydrocephalus. The onset may be acute or gradual. Acute ventricular dilatation occurswhen the initial hemorrhage extends directly into the ventricular lumen. Acuteenlargement may also develop when an intracerebral hematoma dissects by pressurenecrosis through the ventricular wall. Such a gross lesion usually produces coma and,whenever angiography, CT scan or MRI are performed on a seriously ill patient after asubarachnoid hemorrhage, evidence of ventricular enlargement should be sought. In somecases, unilateral dilatation can be observed, at other times the lateral ventricles may bothbe dilated but asymmetrical, whereas in still other cases symmetrical enlargement may befound. At times, a large third ventricle may be demonstrated.
Professor Yasser Metwallywww.yassermetwally.com
252

Figure 25. A case with ruptured anterior communicating artery aneurysm showingsubarachnoid and intraventricular haemorrhage with acute hydrocephalus
In most cases the dilatation of the ventricular system develops gradually without dramaticsymptoms. The changes often begin slowly after an interval of apparent clinicalimprovement. Patients who develop only mild ventricular enlargement may remainasymptomatic.
In most instances in which gradual hydrocephalus occurs, it begins within I month of thesubarachnoid hemorrhage. In the patients who develop symptoms, the manifestations canbe rather similar to normal pressure hydrocephalus; although there is great variability inthe speed of development, the process is progressive when untreated and slow but steadydilation of the ventricles can be found over a period of time up to 3 years. The mostprominent symptom of hydrocephalus is dementia, sometimes accompanied by gaitdisturbances and a spastic paraparesis. A surprisingly large number with more advancedhydrocephalus have epileptic seizures and develop hypertension when they had beennormotensive before the subarachnoid hemorrhage. It is felt that arterial spasm and theoccurrence of an intracerebral hematoma as well as the number of hemorrhagescontributed significantly to the development of hydrocephalus.
It has been generally believed that the most important mechanism for the development ofhydrocephalus is adhesions in the leptomeninges which cause an interference with theextracerebral circulation of cerebrospinal fluid. In some cases there may be arachnoiditisinterfering with egress of fluid from the foramina of the fourth ventricle, but changes aboutthese foramina more often result from infection. In some cases the subarachnoid blockagewas not at the incisura but in other basal cisterns, the cisterns caudal to the block beingirregularly dilated. It would also appear that mechanical blockage of cerebrospinal fluidcirculation is not the sole cause of dilatation of the ventricular system but that cellulardegenerative changes lead to a wasting of brain tissue because of anoxemic ischemia.Vasospasm is a prominent finding after subarachnoid hemorrhage in more than two-thirdsof the patients who develop hydrocephalus. Such spasm may be prolonged and severe for
Professor Yasser Metwallywww.yassermetwally.com
253

many days, as noted earlier, causing a reduction in cerebral blood flow. Oncehydrocephalus has become established it may increase further owing to elongation andstretching of the intracranial vessels reducing blood flow and the mechanical production ofperiventricular demyelination.
CAROTID-CAVERNOUS ANEURYSMS
Almost all of the lesions in the extradural group are cavernous carotid aneurysms. Thelesions are saccular in type and congenital in origin, presumably arising in connection withthe numerous intracavernous minor branching of the internal carotid artery. Inapproximately one-fourth of the cases, cavernous carotid aneurysms are bilateral.
Figure 26. Angiogram showing intracavernous carotid aneurysm
If such an aneurysm ruptures, a carotid-cavernous fistula results. In the absence of trauma,the spontaneous rupture of a saccular aneurysm is the most common cause of anarteriovenous fistula in this location. After a fistula has developed, it may be difficult orimpossible to demonstrate the original sacculation by angiography because of surroundingdural sinus opacification, unless the arterial aneurysm had attained considerable size priorto rupture.
The second principal manifestation of a cavernous carotid aneurysm is its mass effect.Occasionally, symptoms may develop because of blockage of the cavernous sinuses. Somecavernous aneurysms become extremely large. This is possible because as they expand,usually upward, they are covered by the dural wall of the sinus which helps prevent earlyrupture. Rarely, they may act as an extracerebral subfrontal tumor in the anterior fossa .More often, they expand into the suprasellar cistern; an aneurysm must always be includedin the differential diagnosis of suprasellar tumors . Less frequently, such a lesion mayextend laterally and backward. Also, infrequently, the expansion of such aneurysms may sothin the overlying dura that they rupture intracranially to produce a subarachnoidhemorrhage or intracerebral hematoma. In many cases, a large portion of the aneurysmallumen may be filled by organized thrombus, and a shell of calcium about its periphery mayallow diagnosis from plain skull films. Inspite of the organized thrombus and calcification,many such lesions continue to enlarge slowly throughout life. Erosions of the superior
Professor Yasser Metwallywww.yassermetwally.com
254

orbital fissure, the lateral aspect of the sella turcica, and of the clinoid processes aresometimes found.
Cranial nerves are often compressed because of the expanding mass of a cavernous-carotidaneurysm. The larger lesions extending into the suprasellar cistern may compress the opticnerves and chiasm producing visual impairment. These originate usually from the carotidsystem but may also arise from the basilar artery.
Within the cavernous sinus, the internal carotid artery lies chiefly below and medial to theoculomotor nerve. A rather similar relationship pertains to the trochlear nerve, whereasthe abducent nerve is very close to the lateral wall of the carotid artery, along thetransverse course of the vessel in the cavernous sinus. Extraocular movements and otherfunctions may be impaired by compression of one or more of these cranial nerves by acavernous aneurysm. A medially projecting aneurysm is occasionally seen to encroachupon the cavity of the sella turcica.
VASCULAR ECTASIA (FUSIFORM ANEURYSMS)
Fusiform lesions resulting from atherosclerosis wereamong the earliest intracranial aneurysms describedand, although they are not nearly as common ascongenital saccular lesions, they are occasionally
encountered in the course of examination of older individuals. The major vessels at thebase of the brain, particularly the basilar artery, are most commonly affected. The basilarartery is frequently found to be ectatic to a marked degree; the vessel is also usuallyelongated and tortuous.
As noted earlier, the increased mass of the artery may produce indentation of the floor ofthe third ventricle and interference with the circulation of cerebrospinal fluid.Occasionally, the vertebral artery may undergo aneurysmal atherosclerotic dilatation. Agreatly elongated and ectatic vertebral artery may press upon cranial nerves and evensimulate a cerebellopontine angle tumor clinically and at CT scan and MRI .
Figure 27. Basilar ectasia with muralthrombosis
The most common clinicalpresentation of arterial ectasia is brainstem ischaemic manifestations
Professor Yasser Metwallywww.yassermetwally.com
255

Basilar and vertebral fusiform aneurysms may displace the brainstem backward andupward; it may also be displaced laterally by eccentric aneurysmal dilatation of anelongated S-shaped basilar artery and some lesions indent and compress the brain stem.They seldom rupture, but there are often symptoms of ischemia.
Apparently the orifices of branch vessels become occluded by the intimal disease. At times,the carotid siphon is grossly ectatic and tortuous. The enlargement may extend into theproximal segments of the main branches of the internal carotid and basilar arteries andelements of the circle of Willis may be involved.
Figure 28. A, The orifices of the branching vessels of the ectatic arteries are occluded byintramural thrombosis, B, Schematic representation of a thrombosed ectatic basilar artery
At angiography, an estimation of the true size of themass may be gained from the displacements ofadjacent vessels and the circumferential course of thebasilar arterial branches around the lesion and the
displaced and deformed brainstem. Basilar artery fusiform aneurysms often imbedthemselves deeply in the anterior or anterolateral aspect of the brainstem. Long tract signsare frequently produced. The aqueduct of Sylvius may be displaced far backward andnarrowed, and the floor of the posterior part of the third ventricle may be invaginated.Narrowing of the aqueduct frequently produces hydrocephalus involving the lateral andthird ventricles.
Occlusion of the orifices of branchvessels by thrombosis might inducebrain stem infarction
Professor Yasser Metwallywww.yassermetwally.com
256

Figure 29. A, MRA, B, postmortem specimen showing basilar ectasia and basilar tipaneurysm
There also may be interference with cerebrospinal fluid circulation at the tentorialincisura. Such a large basilar artery fusiform aneurysm occasionally ruptures into thebrainstem, even after having been present for very prolonged periods of time, during whichit has acted as a slowly expanding anterior extra-axial mass. Rupture and haemorrhage is,however , extremely uncommon in fusiform aneurysms.
Some of the larger fusiform aneurysms can be identified by computerized tomography.With this technique, increased radiation absorption may be caused by a calcified shell, adensely organized mural thrombus, blood, or a blood clot in the lesion; or the density of anunclotted aneurysm may be enhanced by contrast enhancement techniques .
Figure 30. Vertebrobasilar ectasia
Neuroimaging of fusiform aneurysms
Fusiform aneurysms also are known as atherosclerotic aneurysms. These lesions areexaggerated arterial ectasias that occur due to a severe and unusual form ofatherosclerosis. Damage to the media results in arterial stretching and elongation that may
Professor Yasser Metwallywww.yassermetwally.com
257

extend over a considerable length. These ectatic vessels may have more focal areas offusiform or even saccular enlargement. Intraluminal clots are common, and perforatingbranches often arise from the entire length of the involved parent vessel. Fusiformaneurysms usually occur in older patients. The vertebrobasilar system commonly isaffected. Fusiform aneurysms may thrombose, producing brainstem infarction. They alsocan compress the adjacent brain or cause cranial nerve palsies.
Fusiform atherosclerotic aneurysms usually arisefrom elongated, tortuous arteries. Patent aneurysmsenhance strongly after contrast administration;thrombosed aneurysms are hyperdense onnoncontrast CT scans. Tubular calcification with
intraluminal and mural thrombi in the ectatic parent vessels and aneurysm wall isfrequent. Occasionally, fusiform aneurysms cause erosion of the skull base.
At angiography, fusiform aneurysms often have bizarre shapes, with serpentine or giantconfigurations. Intraluminal flow is often slow and turbulent. These aneurysms typically donot have an identifiable neck. MRI is helpful in delineating the relationship between vesselsand adjacent structures such as the brainstem and cranial nerves.
Figure 31. CT scan (upper lefttwo images), MRI T2 image(upper right image) and MRA(lower two images) showingvertebrobasilar ectasia extendingto the carotid system. Notice thearterial wall calcification and thebrain stem lacunar infarctions.
Patent aneurysms enhance stronglyafter contrast administration;thrombosed aneurysms arehyperdense on noncontrast CT scans.
Professor Yasser Metwallywww.yassermetwally.com
258

Differential diagnosis of fusiform aneurysms
True saccular aneurysms of principal arteries at the base of the brain produce mass effects,when they become large without rupturing, even more often than fusiform aneurysms,which may be silent. A large supraclinoid aneurysm of the carotid siphon frequentlyextends medially and upward to compress the optic chiasm and hypothalamus . There mayeven be obstruction at the foramen of Monro. In many instances, a large portion of theaneurysm is filled by mural thrombus so that there is much more vascular displacementthan can be accounted for by the size of the opacified lumen at angiography.
Figure 32. Calcified ectatic basilar artery
Occasionally, an aneurysm arising at the origin of the ophthalmic artery may beencountered. Such a lesion may arise either intradurally or extradurally. Similarly, itsexpansion may occur within the subarachnoid space or extradurally along the course of thevessel toward the optic foramen. In the latter instance, erosion of the inner end of the opticcanal may be visible on plain skull radiographs. Such an aneurysm can compress the opticnerve against the bony edge of its canal.
Surprisingly large aneurysms can develop along the course of the middle cerebral artery.Although many middle cerebral aneurysms bleed when they are relatively small, occasionalaneurysms along the course of this vessel over the anterior perforated substance andbetween the temporal lobe and insula become sufficiently enlarged to act as tumors.
Saccular aneurysms of the basilar artery may become very large. Their massiveproportions are probably related to the frequent development of a large organizedthrombus about the periphery of the lumen. Circulation in the lumen of the lesion mayconstitute a relatively small part of its total volume .
Professor Yasser Metwallywww.yassermetwally.com
259

FUSIFORM ANEURYSMS
Commonly involve the vertebrobasilar system and might extend to involve otherarteries around the circle of Willis
Involved arteries are diffusely dilated, tortuous, kinked, abnormally prolonged withfrequent mural thrombosis and occasional wall calcification.
Fusiform aneurysms rarely rupture or produce subarachnoid haemorrhage Fusiform aneurysms are commonly associated with microvascular brain disease The clinical presentation of fusiform aneurysms includes
o Ischemic manifestationso Pressure due to the mass effect of greatly dilated fusiform aneurysms
References
Berenstein A, Flamm ES, Kupersmith MJ: Unruptured intracranial aneurysms. NEngl J Med 1999 May 6; 340(18): 1439-40; discussion 1441-2.
Biousse V, Newman NJ: Aneurysms and subarachnoid hemorrhage. Neurosurg ClinN Am 1999 Oct; 10(4): 631-51.
Flamm ES, Grigorian AA, Marcovici A: Multifactorial analysis of surgical outcomein patients with unruptured middle cerebral artery aneurysms. Ann Surg 2000 Oct;232(4): 570-5.
Goldman: Cecil Textbook of Medicine. 21st ed W B Saunders Co; 1999. Greenberg MS: Handbook of Neurosurgery. 4th ed 1997; Theme Medical Pub,
Lakeland, FL:. Hunt WE, Hess RM: Risks and benefits of screening for intracranial aneurysms in
first-degree relatives of patients with sporadic subarachnoid hemorrhage . 1969;341(18): 1344.
Johnston SC, Wilson CB, Halbach VV, et al: Endovascular and surgical treatmentof unruptured cerebral aneurysms: comparison of risks. Ann Neurol 2000 Jul;48(1): 11-9.
Kappelle LJ, Eliasziw M, Fox AJ: Small, unruptured intracranial aneurysms andmanagement of symptomatic carotid artery stenosis. North American SymptomaticCarotid Endarterectomy Trial Group. Neurology 2000 Jul 25; 55(2): 307-9.
Kappelle LJ, Eliasziw M, Fox AJ: Small, unruptured intracranial aneurysms andmanagement of symptomatic carotid artery stenosis. North American SymptomaticCarotid Endarterectomy Trial Group. Neurology 2000 Jul 25; 55(2): 307-9.
Kremer C, Groden C, Hansen HC: Outcome after endovascular treatment of Huntand Hess grade IV or V aneurysms: comparison of anterior versus posteriorcirculation. Stroke 1999 Dec; 30(12): 2617-22.
Morey SS: AHA recommendations for the management of intracranial aneurysms.Agency for Health Care Policy and Research. Am Fam Physician 2001 Jun 15;63(12): 2465-6.
Professor Yasser Metwallywww.yassermetwally.com
260

Newell DW, Elliott JP, Eskridge JM: Endovascular therapy for aneurysmalvasospasm. Crit Care Clin 1999 Oct; 15(4): 685-99, v.
Olafsson E, Hauser WA, Gudmundsson G: A population-based study of prognosisof ruptured cerebral aneurysm: mortality and recurrence of subarachnoidhemorrhage. Neurology 1997 May; 48(5): 1191-5.
Raaymakers TW, Rinkel GJ, Ramos LM: Initial and follow-up screening foraneurysms in families with familial subarachnoid hemorrhage. Neurology 1998 Oct;51(4): 1125-30.
Raaymakers TW: Aneurysms in relatives of patients with subarachnoidhemorrhage: frequency and risk factors. MARS Study Group. Magnetic ResonanceAngiography in Relatives of patients with Subarachnoid hemorrhage. Neurology1999 Sep 22; 53(5): 982-8.
Raaymakers TW: Aneurysms in relatives of patients with subarachnoidhemorrhage: frequency and risk factors. MARS Study Group. Magnetic ResonanceAngiography in Relatives of patients with Subarachnoid hemorrhage. Neurology1999 Sep 22; 53(5): 982-8.
Speth CP: Risks and benefits of screening for intracranial aneurysms. N Engl J Med2000 Mar 9; 342(10): 739-40.
Professor Yasser Metwallywww.yassermetwally.com
261

INDEX
CLINICAL FEATURES
PATHOLOGY
IMAGING
INTRODUCTION
Cerebrovascular disease is a leading contributor to dementia worldwide. In mostpopulations which have been studied, only Alzheimer's disease (AD) is a more commoncause of dementia (8). In 1974, Hachinski et al. (24) popularized the phrase "multi-infarctdementia" (MID) to represent the syndrome of dementia accompanied by focal neurologicsigns or symptoms, characterized by stepwise deterioration, and frequently associated withhypertension. In some populations with a high prevalence of hypertension (such as AfricanAmerican men and the Japanese), MID is more common than AD (26, 56). Thenomenclature of MID is complicated by several overlapping terms. Though criteria for thediagnosis of MID were published in DSM-III-R in 1987 (2) and have been widely adopted,
INTRODUCTION
262

their reliability has been questioned and nonstandard alternatives have arisen (14).Furthermore, "vascular dementia" (VaD) has emerged as a diagnostic category thatincludes not only the multiple discrete infarcts of MID, but other dementing syndromesattributed to cerebrovascular origins. Among these is a dementia associated with diffusesubcortical white-matter disease putatively attributed to chronic subcortical ischemia. Thisstate is commonly, but controversially, known as "Binswanger's disease" or "subcorticalarteriosclerotic encephalopathy." In contrast, "Leuko-araiosis" was proposed byHachinski et al. (25) as a description of radiologic and pathologic subcortical white-matterabnormalities such as those encountered in Binswanger's disease, but these changes are notobligately associated with dementia. Other less common causes of dementia, such asvasculitides, are also considered under the rubric of vascular dementia.
MID has been considered a "subcortical dementia" (10). The term "subcortical dementia"provides a clinical shorthand for dementia with prominent motor effects and relative rarityof the "cortical syndromes" of aphasia, agnosia, and apraxia. Erkinjuntti (13) reported,however, that 65 of 79 MID patients in his series had sustained a cortical stroke and that56% of the subjects had evidence of cortical strokes alone. Mahler and Cummings (41)have subsequently considered large-vessel and small-vessel behavioral subtypes of vasculardementia. This distinction further clouds the concept of MID as a subcortical syndromebecause the behavioral neurology of large-vessel infarctions typically involves "cortical"signs. The theoretical problems inherent in a cortical-subcortical dichotomy for thedescription of dementia have also been previously addressed (61). The interpretation ofwhat constitutes MID is further complicated by a lack of specificity and uniformapplication of proposed criteria for diagnosis. Given the high prevalence ofcerebrovascular disease, strokes frequently contribute to the cognitive morbidity ofindividuals with dementia of all types, including AD. Although antemortem clinicalevaluations and imaging may confirm the presence of multiple strokes, those techniquescannot exclude the presence of AD pathology contributing to the overall condition. Forinstance, the presence of cerebral infarctions may allow the clinical expression ofAlzheimer-type dementia even though the pathologic criteria for AD are not met.Consequently, the frequency of pure MID in autopsy studies is 10-23%, comparable to thatof "mixed dementia" with changes of both MID and AD (35).
CLINICAL FEATURES
Recurrent cerebral infarctions are, by definition, the pathophysiologic basis of MID. Therisk factors for MID are, not surprisingly, those for cerebrovascular disease, especially ageand hypertension. There appear to be no risks specific for the development of MID withinthe context of cerebrovascular disease. In about 90% of pathologically verified cases ofMID there is a history of acute unilateral motor or sensory dysfunction consistent withstroke (14). There may also be a history of acute impairment of "cortical" functionsmanifest as aphasia, apraxia, or agnosia. Urinary dysfunction and gait disturbance havebeen suggested as early markers for the development of MID (38). With accumulation ofischemic brain lesions there is typically incremental impairment of memory and behavioralinitiation, along with extrapyramidal features such as facial masking and rigidity.
263

Abrupt onset 2Stepwise progression 1Fluctuating course 2Nocturnal confusion 1Relative preservation of personality 1Depression 1Somatic complaints 1Emotional incontinence 1History of hypertension 1History of strokes 2History of associated atherosclerosis 1Focal neurologic symptoms 2Focal neurologic signs 2
An "ischemic score" (IS) was proposed byHachinski et al. (23) as a means ofdistinguishing MID from primarydegenerative dementia. A number of variantshave been employed since the introduction ofthe original IS; a typical example is shown inTable 1. These scales share the commonweaknesses that they are sensitive but notspecific indicators of MID and do notaddress the presence or absence of ADpathology (8). In the clinical setting, an IS ismost useful as an instrument for suggestingthe presence of cerebrovascular contributorsto a dementia syndrome.
Table 1. Hachinski ischemia score
The diagnosis of MID depends on the establishment of dementia — that is, a sustaineddecrement from previously attained levels of cognitive ability, sufficient to interfere witheveryday activities, without an associated impairment of consciousness. Dementia may bestable or progressive. If strokes are the cause of a dementia, it is conceivable that theremight be an improvement in cognitive status as the deficits from an acute stroke resolvewithout returning to baseline. When dementia is accompanied by a history of strokestemporally linked to stepwise deterioration in intellectual abilities, the clinical diagnosis ofMID is obvious, though mixed dementia is also a possibility. A more difficult diagnosticsituation is the patient with a history of strokes not temporally associated with onset ofworsening of cognitive impairment. Recently, Chui et al. (9) proposed criteria for thediagnosis of "ischemic vascular dementia," based on the model for diagnosis of AD (44).These criteria are summarized in Table 2. An even more broadly defined set ofinternational diagnostic criteria for research studies of vascular dementia has beenproposed (52), but these have been criticized for being overly inclusive and failing toaddress the importance of temporal association of vascular events with onset of intellectualimpairment (12). Of particular note is the inability of any criteria, short of autopsyexamination, to differentiate mixed dementia from MID. These factors have led toconsiderable controversy over the clinical usefulness of the "vascular dementia" concept (7,49). Hachinski (22) has further argued that diagnostic criteria for vascular dementia fail toaccount for the fact that it is a syndromic diagnosis of multiple origins and outcomes.
264

Table 2. Criteria for the diagnosis of ischemic vascular dementia (IVD)
I. Dementia
Dementia is a deterioration from a known or estimated prior level of intellectual function sufficient to interfere
broadly with the conduct of the patient's customary affairs of life, which is not isolated to a single narrow category ofintellectual performance and which is independent of level of consciousness.
This deterioration should be supported by historical evidence and documented either by bedside mental status testing
or, ideally, by more detailed neuropsychological examination, using tests that are quantifiable and reproducible and for whichnormative data are available.
II. Probable IVD
A. The criteria for the clinical diagnosis of probable ivd include all of the following:
1. Dementia
2. Evidence of two or more ischemic strokes by history, neurologic signs, and/or neuroimaging studies (CT of
T1- weighted MRI
B. The diagnosis of probable ivd is supported by:
1. Evidence of multiple infrared in brain regions known to affect cognition
2. A history of multiple transient ischemic attacks
3. History of vascular risk factors (e.g., hypertension, heart disease, diabetes mellitus)
4. Elevated Hachinski Ischemia Scale (original or modified version)
C. Clinical features that are thought to be associated with IVD but await further research include:
1. Relatively early appearance of gait disturbance
2. Periventricular and deep white-matter changes on T2-weighted MRI that are excessive for age
3. Focal changes in electrophysiologic studies (e.g., EEG, evoked potentials) or physiologic neuroimaging studies (e.g., SPECT-ET-NMRspectroscopy)
D. Other clinical features that do not constitute strong evidence either for or against a diagnosis of probable ivd
include:
1. Periods of slowly progressive symptoms
2. Illusions, psychosis, hallucinations, delusions
3. Seizures
E. Clinical features that cast doubt on a diagnosis of probable ivd include:
265

1. Transcortical sensory aphasia in the absence of corresponding focal lesions on neuroimaging studies
2. Absence of central neurologic symptoms/signs, other than cognitive disturbance
III. Possible IVD
A clinical diagnosis of possible ivd may be made when there is:
1. Dementia
and one or more of the following:
2a. A history or evidence of a single stroke (but not multiple strokes) without a clearly documented temporal
relationship to the onset of dementia or
2b. Binswanger's syndrome (without multiple strokes) which includes all of the following:
i. Early-onset urinary incontinence not explained by urologic disease, or gait disturbance (e.g., parkinsonian, magnetic,apraxic, or "senile" gait) not explained by peripheral cause
ii. Vascular risk factors
iii Extensive white-matter changes on neuroimaging
IV. Definite IVD
Diagnosis of definite ivd requires histopathologic examination of the brain, as well as:
A. Chemical evidence of dementia
B. Pathologic confirmation of multiple infarcts, some outside of the cerebellum
V. Mixed dementia
A diagnosis of mixed dementia should be made in the presence of one or more other systemic or brain disorders
that are thought to be causally related to the dementia.
The degree of confidence in the diagnosis of IVD should be specified as possible, probably, or definite, and the other disorder(s)contributing to the dementia should be listed. For example: mixed dementia due to probable IVD and possible Alzheimer's disease, ormixed dementia due to definite IVD and hypothyroidism.
Note: If there is evidence of Alzheimer's disease or some other pathologic disorder that is thought to have contributed to the dementia, adiagnosis of mixed dementia should be made.
NEUROPSYCHOLOGICAL FEATURES
Because they are sensitive to site of dysfunction as opposed to the mechanism causing it,neuropsychological tests have been incapable of consistently distinguishing between MID,AD, and mixed dementias (41). Gainotti et al. (19) reported that AD patients were morelikely than those with MID to make "globalistic" or "odd" type errors on Raven's ColoredProgressive Matrices task, and on a design copy task were more likely to demonstrate the"closing-in" phenomenon — that is, copying figures such that they overlap the model.Mendez and Ashla-Mendez (45) suggested that unstructured neuropsychological tasks,
266

such as the Tinker Toy test, may be able to distinguish between AD and MID, because ofprominent aspontaneity in the latter. As with other neuropsychological measures, theranges of performance of AD and MID patients overlap, which limits the diagnosticspecificity in any individual patient. Furthermore, how well these results generalize to apopulations not selected for the "classic" clinical courses of the syndromes is unknown.Rothlind and Brandt (53) have proposed the use of a Frontal/Subcortical AssessmentBattery as a supplement to common bedside cognitive examinations for differentiatingdementia types characterized by prominent subcortical pathology from AD.
EPIDEMIOLOGY
The reported frequency of MID in demented populations ranges from 4.5% to 39% (34).Karasawa and Homma (33) have suggested that the prevalence of MID, at least in Japan,has decreased since 1980 as the result of fewer strokes affecting the elderly.
Jorm et al.'s (29) extensive review of previous studies provides the basis for much of thecurrent understanding of the demographics of MID. They calculated the prevalence ofMID as doubling with every 5.3 years of age, which is in contrast to a popular perceptionthat the prevalence of MID declines after age 75 because of mortality associated withrecurrent strokes (43). Men are affected with MID more frequently — as opposed to AD,which is more common among women (29). In Europe, there is also a trend toward higherrates of MID in rural populations than in urban ones (34).
Meta-studies of the epidemiology of MID have been complicated by the lack of clear-cutand uniform diagnostic criteria. Another problem in the interpretation of MIDepidemiology is that the illness is often defined on the basis of its risk factors regardless oftemporal course. As pointed out by Kase (34), in the presence of dementia, the IS items of(a) history of hypertension, (b) history of stroke, (c) evidence of associated atherosclerosis,and (d) focal findings on neurologic exam are considered sufficient to diagnose MID.Prospective studies, using uniform diagnostic criteria and paying careful attention to thetiming and character of stroke and dementia, will be required to more fully understand theepidemiology and natural history of MID.
PATHOLOGY
Tomlinson, Blessed, and Roth's landmark article (59) on the neuropathology of dementedolder individuals clarified the importance of AD pathology in senile dementia. It alsoreported a 20% frequency of multiple, discrete infarcts. These findings, along withHachinski et al.'s (24) popularization of the term MID, defined the role of focal infarctionsas a cause of dementia. Lacunar infarctions, also known as lacunes, are commonlyimplicated as a major contributor to MID because of the "subcortical" features oftenprominent in the clinical presentation of the illness. Lacunes are small cavitary lesionsattributed to the occlusion of deep penetrating arteries. There is no uniform definitionbased on size, but most lacunes are less than 2 cm in diameter. Lacunar infarctions arealmost invariably associated with lipohyalinosis of the brain microvasculature.
267

Figure 1. A, lipohyalinosis, B, lacunar infarction
Figure 2. Lacunes. Small cavitary infarcts, resulting from hypertension, most frequentlyinvolving the basal ganglia (caudate nucleus, globus pallidus, putamen, and amygdala) andbasis pontis. Compare right with left.
Lacunar infarctions are strongly associated with a history of hypertension. In Fisher's (16)report, 97% of 114 autopsy cases of lacunar infarction had a diagnosis of hypertension,though more recent studies with stricter criteria for hypertension suggest rates rangingfrom 60% to 75% (47). The importance of lacunes per se as contributors to the dementiahas been questioned. Both Tomlinson et al. (59) and Fisher (17) minimized the role of theselesions in cognitive deficits. Cases of MID with lacunes also typically show myelin-stainevidence for extensive white-matter degeneration (leukoaraiosis) (27, 48). Whether anaccumulation of lacunes themselves is able to produce dementia in the absence ofassociated noncavitary white-matter damage is unknown. Though frequently referred to asdemyelination, electron microscopy (EM) indicates that axons within the myelin-stainlesions are lost as well (63). Because the diffuse white-matter changes and the cavitarylesions almost always co-occur and share a common pathophysiology, it is unlikely thattheir differential effects will be elucidated from human clinical material. The problem indifferentiating "pure" MID pathologically is one factor contributing to the evolution of the
268

more inclusive concept of ischemic vascular dementia. Pathologically multi-infactdementia, in ischemic microvascular brain disease, often contains a mix of lacunarinfarctions, leukoaraiosis, central and cortical atrophy, granular atrophy and basalganglionic calcification in various combinations. History and or radiological / pathologicalstudies often show evidence of hypertensive hemorrhagic changes in MID patients.
Figure 3. Lacunar infarctions
Two other types of discrete infarctions contribute to many cases of MID. Large-vesselinfarctions are usually identifiable by history with features of hemiparesis, hemianopia,aphasia, and so on. These are also unequivocally evident on CT or MRI. The volume oftissue loss from such lesions is an important factor in the development of dementia.Tomlinson et al. (59) reported that all their autopsy subjects with greater than 100 ml oftissue loss were demented. However, it is clear that dementia can follow much smallerlosses of brain tissue if these are strategically located (11). The second type of cortical lesioncontributing to MID is the micro-infarct. These have been reported as the sole basis ofdementia (32, 59) and consist of 0.5-to 2-mm-diameter lesions within the cortical ribbon.They are associated with a history of transient ischemic attacks (48).
269

Figure 4. Postmortem specimen.Note the topographicallyextensive periventricular whitematter changes in a hypertensivecase with evidence ofleukoaraiosis on MRI study
Other factors which predispose to the development of multiple cerebral infarctions areassociated with MID or vascular dementia. Conditions leading to thromboembolic showers,such as endocarditis or atrial myxoma, can lead to the rapid development of a dementedstate often after a period of acute encephalopathy or coma. Autoimmune vasculitides, suchas in systemic lupus erythematosus or granulomatous angiitis of the central nervoussystem, contribute to areas of cerebral ischemia and infarction. They can be associatedwith long-term cognitive impairments. Tertiary Lyme disease and syphilis can also causedementia on the basis of vasculitic thromboses. Cerebral amyloid angiopathy, though oftenlinked to AD, may lead to multiple intracerebral hemorrhages and play a significant role inthe development of vascular dementia (28). One other lesion of vascular origin which canpresent as dementia is chronic subdural hematoma. These intracranial fluid collections canmimic the fluctuating, stepwise cognitive deterioration and prominent motor symptomscharacteristic of MID, and they are largely reversible with surgical drainage of fluid andrelief of mass effect.
270

Figure 5. A case of multi-infarct dementia. There are multiple cystic spaces consistent withsmall remote infarcts. These are predominantly in the subcortical white matter (blackarrows) and basal ganglia (red arrow). In other sections more could be seen in thethalamus too. Note how small the basal ganglia are on the right vs. the left. There is also adilatation of the lateral ventricles. In this case it is probably due to loss of tissue rather thanincrease in CSF, hence it is called hydrocephalus ex vacuo. Finally there is moderateatherosclerosis of the middle cerebral artery on the right (yellow arrows).
PATHOGENESIS
To date, there remains no concise explanation for the pathogenesis of MID except forinfarctions causing loss of brain volume or loss of strategic, localized, areas integral tonormal cognition, or a combination of these two factors.
Although CBF is diminished in MID, this is a feature common to most dementia andprobably represents a response to reduced cerebral metabolism, rather than the cause ofthe cognitive impairment. Some MID patients show foci of elevated regional oxygenextraction fraction (rOEF) suggestive of areas of chronic compensated ischemia (21).
271

Rogers et al. argued (51) that a state of insufficient blood flow to the brain precedes theonset of dementia in MID patients by up to 2 years. Brown and Frackowiak (6) havecautioned, however, that such rOEF changes are not common among MID patients andtherefore cannot be the major factor in the development of most MID. Two conditionsassociated with global diminution in CBF — cardiac disease (58) and hypertension (3) —have nonetheless been long recognized as contributors to impairment onneuropsychological testing. Meyer et al. (46), for example, reported that careful control ofblood pressure improved cognition in some in MID patients, but overcontrol (withpresumed diminution of CBF) worsened cognitive performance. Increased whole bloodviscosity often contributes to diminished brain perfusion in MID patients. Increased wholeblood viscosity is very common in essential hypertension.
MID and, more inclusively, vascular dementia are associated with changes in the blood-brain barrier (BBB). Elevated cerebrospinal fluid (CSF) concentrations of albumin andimmunoglobulin G (IgG) have been reported for MID patients (40), though other studieshave found no difference for albumin (1) or IgG (5). Interestingly, Blennow et al. (5) alsoreported increased CSF/serum ratios for albumin in AD patients with white-matter lesionsor vascular risk factors. This indicates that BBB dysfunction in vascular dementia mayresult from risk factors for cerebrovascular disease rather than represent a uniquecontributor to MID. Wallin and Blennow (60) have argued that, because myelin lipids aresignificantly reduced in vascular dementia, the myelin sheath is a primary lesion site. Theyfurther hypothesize that the high metabolic demands of the oligodendrocytes render themprone to ischemic damage. These views are at odds with (a) the PET data, which suggestthat chronic ischemia is not a contributor to MID (6), and (b) the EM studies, which showaxonal loss in areas of noncavitary demyelination (63). Although myelin loss and BBBdysfunction may contribute to some vascular dementia syndromes, their causative role inMID is questionable. One of the difficulties in assessing the pathophysiology of vasculardementia is the considerable frequency of dementia with findings of both vascular diseaseand AD. Although this may simply represent the co-occurrence of two common illnesses,there is evidence that links cerebrovascular disease and AD pathology. Kalaria et al. (31),for instance, found that cerebral ischemia promotes deposition of potentially neurotoxicamyloid in the brain. Sofroniew et al. (57) reported that focal cerebral damage causesneuronal loss in the nucleus basalis of Meynert similar to that observed in AD.Furthermore, such changes in the basal forebrain, when associated with AD, have beenlinked to alterations of cerebral vascular regulation and diminution of CBF (54). Thesynthetic sites for the biogenic amines are also affected in AD (42, 50). Degeneration inthese sites, the locus coeruleus and dorsal raphe nuclei, may adversely affectcerebrovascular function, because norepinephrine and serotonin also influence vascularautoregulation (53). The distinction between causes of vascular and "primarydegenerative" dementias may therefore be more difficult than is commonly accepted.
272

Table 3. Pathological /clinical associates of multi-infarct dementia
Vascular risk factors Hypertension, NIDDM, type IV hyperglycaemia, old age, andLVH are common in MID patients.
Hypertensive vascularpathology
Lipohyalinosis and arteriolar wall fibrosis are common in MIDpatients
Pathological findings Neuronal degeneration, ischaemic demyelination, diffuselacunar state, and leukoaraiosis are common in MID patients
Haemorheological profile Increased whole blood viscosity and increased thrombotictendency are common in MID patients
ANIMAL MODELS
Although a number of animal models for the development of MID have been employed,none have been satisfactory. Rodents tend not to have profound long-lasting behavioraleffects from cerebral infarctions, and the multiple or diffuse, gradually acquired lesionscharacteristic of MID in humans have not been reproduced. The promising technique ofinducing embolic ischemia in rats by injecting 35-m-diameter microspheres into ratcarotid arteries produced effects on memory, but these were not sustained (37).
IMAGING
As with most central nervous system diseases, imaging studies have an important role inthe diagnosis of MID. In contrast to the diagnosis of AD, in which cerebral images are usedto "rule out" structural changes contributing to the dementia, the images in MID canclearly identify significant pathology. In the neuropathologically verified series ofErkinjuntti's group (14), 74% of MID patients had cortical infarcts and 13% had deepinfarcts on x-ray computed tomography (CT). Magnetic resonance imaging (MRI) is moresensitive to lesions in the brain than CT, but this is not necessarily an advantage in thediagnosis of MID. Cavities present on T1-weighted images are consistent with cerebralinfarction, but many of the changes observed on MRI may represent the effects of healthyaging, such as dilated perivascular spaces. The typical changes include small, focal areas ofincreased signal as well as patchy or confluent periventricular white-matter hyperintensityon T2-weighted images. These nonspecific changes are the basis of the term"leukoaraiosis" (LA). It is important to recognize that a large volume of diffuse signalchange may be present on CT or MRI without meaningful impairment of cognition.Nonetheless, LA is a frequent correlate of MID. In Erkinjuntti et al.'s (15) clinical series,72% of MID patients had LA, as opposed to 19% of AD patients.
273

Figure 6. Periventricularlacunar infarctions. Noticecentral and /or corticalatrophy.
Figure 7. Periventricularlacunar infarctions andcalcifications
For many years, "cerebral arteriosclerosis" was considered an important component ofmost senile dementia — hence the popular use of the phrase "hardening of the arteries" asa synonym for dementia. This perception understandably led to extensive study of cerebralblood flow and metabolism, but with little concern over clinical differentiation of dementiatypes. The earliest studies employed inert gas measures of global cerebral metabolic rate
274

for O2 (CMRO2). Such studies demonstrated diminished cerebral metabolism in dementedsubjects, both with and without known cerebrovascular disease (39).
Figure 8. leukoaraiosis, CT scan images showing periventricular diffuse hypodensity,which is mainly due to astrogliosis and interstitial edema. Notice central and /or corticalatrophy.
Developing technology subsequently allowed regional cerebral blood flow (CBF)measurements using the gamma-emitter 133Xe and multiple extracranial radiationdetectors for planar or tomographic imaging. Simultaneously, a greater understanding ofdementia subtypes improved the discriminative abilities of the techniques. Patients withvascular dementia, including MID, demonstrate patchy, irregular areas of decreased CBFconsistent with areas of infarction or ischemia, whereas AD patients have more uniformfrontal, parietal, and temporal decreases in CBF (36, 62). There is no general agreementthat diminished CBF by 133Xe methods correlates with dementia severity. Some studieshave found good correlation in MID only (23), and others have reported it in AD only (62);however most studies have found it in both (6).
275

Figure 9. leukoaraiosis, MRI T2 image. The MRI T2 periventricular hyperintensities aremainly due to astrogliosis and interstitial edema. Notice central and /or cortical atrophy.
Positron emission tomography (PET) using 15O allows detailed mapping of O2metabolism. Neither AD nor MID patients typically demonstrate chronic ischemia by thismethod (18). Despite early enthusiasm for [18F]fluorodeoxyglucose (FDG) PET as a usefultechnique for the differentiation of MID and AD (4), subsequent investigations have notbeen as conclusive (6).
Single photon emission computed tomography (SPECT) is more widely available than PETand has been used clinically to differentiate MID from AD, though the validity of SPECTfor this purpose is not known. Neither of the two isotopes in general use, 123I-labeledamphetamine (IMP) and 99mTc-labeled hexamethylpropylene amine oxime (HMPAO), hasbeen shown to be superior in the differential diagnosis of dementia (20). As with otherimaging modalities, MID patients tend to show patchy or multifocal hypoperfusionwhereas AD patients show more diffuse changes, but there is sufficient overlap to preventdiagnostic surety in any individual patient (55).
276

Table 4. Pathological / radiological findings in multi -infarct dementia
Pathology descriptionCentral and corticalatrophy
This is secondary to chronic global reduction of brain perfusion.
Leukoaraiosis Leukoaraiosis is an ischaemic demyelination of the immediateperiventricular white matter with axonal loss, astrogliosis andinterstitial edema. It is secondary to chronic global reduction ofbrain perfusion.
Lacunar infarctions lacunar infarctions are secondary to the micro vascular thrombo-occlusive episodes. They are most numerous in the periventriculargray matter (thalamus and basal ganglia) and the immediateperiventricular white matter. Spasm of the fine penetratingarterioles (secondary to increased VSMCs sensitivity) -can alsoresult in Lacunar infarctions. It is commonly associated withlipohyalinosis of the microvascular brain bed.
Granular atrophy Granular atrophy is defined pathologically as infarctions localizedto the cerebral cortex and not extending to the subcortical whitematter.
Basal ganglioniccalcifications
These are calcification of the the arteriolar wall of themicrocirculation within the basal ganglia .
TREATMENT
Drugs of many classes and presumed mechanisms of action have been tried in thetreatment of the cognitive symptoms in MID, but none have consistently beendemonstrated to be effective. No agent has been approved for such use in the United States.There are, however, potential means of symptomatic treatment. Improvement amongselected MID patients on a screening instrument for cognition, the Cognitive CapacityScreening Exam (CCSE), was reported with treatment of vascular risk factors such ashypertension and smoking. Similar treatments did not affect the cognition of AD patientsin the same paradigm (46). In systemic conditions that decrease CBF, such as valvularheart disease and hypertension, neuropsychological test performance can improve withtreatment of the causative factor(s) (30).
Alteration of the course of the illness may also be accomplished. Reduction of bloodpressure is a primary goal of treatment in order to diminish the risk for recurrent stroke(43). Other risk factors, such as smoking and diabetes mellitus, can be addressed to reverseor slow the progression of vascular pathology. Any treatment approach that reduces thelikelihood of stroke, such as carotid endarterectomy in moderate stenoses or the use ofaspirin or ticlopidine in primary and secondary prevention, is likely to alter the course ofMID, but no definitive analyses have been reported. It is important, however, to emphasizethat many of the vascular changes contributing to strokes are the result of long-termpathologic processes which are not reversed with treatment. As Meyer et al. (46) found,
277

overreduction in blood pressure can actually worsen cognition. That risk factormodification can affect the course of MID after diagnosis has not been conclusivelydemonstrated, but a reduction in vascular dementia prevalence has been attributed toattention to risk factors (26).
CONCLUSIONS
Multi-infarct dementia is a syndrome which varies according to the site, size, nature,number, and timing of the lesions. Although criteria for the diagnosis of vascular dementiaas a whole have been proposed, the long-term utility of such criteria has been questioned(22). No specific risk factors beyond those for cerebral ischemia have been identified, but itis likely that with control of the risk factors, progression of the illness, and perhaps currentfunction, can be affected. The challenge lies in the early identification of those at risk forsubsequent development of cognitive impairments and intervention. Prevention of vasculardementia through risk factor management may have further impact because of potentialinteractions between cerebral ischemia and the expression of AD.
FUTURE DIRECTIONS
Hachinski (22) has claimed that "Few areas in medicine are as ripe for action as thevascular dementias." The success of further efforts to understand vascular dementiadepends on several factors. Included among them are (a) a commonly accepted definition ofwhat constitutes vascular dementia and (b) the recognition that multiple, potentiallytreatable causes contribute to a final common clinical state of dementia. Early recognitionof risk, and subsequent intervention, are then possible before the evolution of the dementia.The development of more useful animal models and new techniques of functional imagingto understand the pathogenesis of dementia in the face of vascular compromise will be vitalin settling many of the controversies surrounding the field today. Despite thosecontroversies, and the impediments to progress engendered by them, it is apparent thatprevention and treatment of vascular dementia is an achievable goal
REFERENCES
1.Alafuzoff I, Adolfsson R, Bucht G, Winblad B. Albumin and immunoglobulin in plasmaand cerebrospinal fluid, and blood-cerebrospinal fluid barrier in patients with dementia ofAlzheimer type and multi-infarct dementia. J Neurol Sci 1983;60:465-472.
2.American Psychiatric Association Committee on Nomenclature and Statistics. Diagnosticand statistical manual of mental disorders (DSM-III-R), 3rd ed. (revised). Washington, DC:American Psychiatric Association, 1987.
3.Apter NS, Halstead WC, Heimburger RF. Impaired cerebral functions in essentialhypertension. Am J Psychiatry 1951;107:808-813.
278

4.Benson DF, Kuhl DE, Hawkins RA, Phelps ME, Cummings JL, Tsai SY. Thefluorodeoxyglucose 18F scan in Alzheimer's disease and multi-infarct dementia. ArchNeurol 1983;40:711-714.
5.Blennow K, Wallin A, Fredman P, Karlsson I, Gottfries CG, Sverrholm L. Blood-brainbarrier disturbance in Alzheimer's disease is related to vascular factors. Acta Neurol Scand1990;81:323-326.
6.Brown WD, Frackowiak RSJ. Cerebral blood flow and metabolism studies in multi-infarct dementia. Alzheimer's Dis Assoc Disord 1991;5:131-143.
7.Brust JCM. Vascular dementia is overdiagnosed. Arch Neurol 1988;45:799.
8.Chui HC. Dementia: a review emphasizing clinicopathologic correlation and brain-behavior relationships. Arch Neurol 1989;46:806-814.
9.Chui HC, Victoroff JI, Margolin D, Jagust W, Shankle R, Katzman R. Criteria for thediagnosis of ischemic vascular dementia proposed by the State of California Alzheimer'sDisease Diagnostic and Treatment Centers. Neurology 1992;42:473-480.
10.Cummings JL, Benson DF. Dementia: a clinical approach. Boston: Butterworth, 1983.
11.del Ser T, Bermejo F, Portera A, Arredondo JM Bouras C, Constantinidis J. Vasculardementia: a clinicopathological study. J Neurol Sci 1990;96:1-17.
12.Drachman DA. New criteria for the diagnosis of vascular dementia: do we know enoughyet? Neurology 1993;43:243-245.
13.Erkinjuntti T. Types of multi-infarct dementia. Acta Neurol Scand 1987;75:391-399.
14.Erkinjuntti T, Haltia M, Palo J, Sulkava R, Paetau A. Accuracy of the clinical diagnosisof vascular dementia: a prospective clinical and post-mortem pathological study. J NeurolNeurosurg Psychiatry 1988;51:1037-1044.
15.Erkinjuntti T, Ketonen L, Sulkava R, Vuorialho M, Palo J. CT in the differentialdiagnosis between Alzheimer's disease and vascular dementia. Acta Neurol Scand1987;75:262-270.
16.Fisher CM. Lacunes: small, deep, cerebral infarcts. Neurology 1965;15:774-784.
17.Fisher CM. Lacunar strokes and infarcts: a review. Neurology 1982;32:871-876.
18.Frackowiak RSJ, Pozzilli C, Legg NJ, et al. Regional cerebral oxygen supply andutilization in dementia: a clinical and physiological study with oxygen-15 and positrontomography. Brain 1981;104: 753-778.
279

19.Gainotti G, Parlato V, Monteleone D, Carlomagno S. Neuropsychological markers ofdementia on visuospatial tasks: a comparison between Alzheimer's type and vascular formsof dementia. J Clin Exp Neuropsychol 1992;14:239-252.
20.Gemmell HG, Sharp PF, Besson JAO, Ebmeier KP, Smith FW. A comparison of Tc-99m HM-PAO and I-123 IMP cerebral SPECT images in Alzheimer's disease and multi-infarct dementia. Eur J Nucl Med 1988;14:463-466.
21.Gibbs JM, Frackowiak RSJ, Legg NJ. Regional cerebral blood flow and oxygenmetabolism in dementia due to vascular disease. Gerontology 1986;32(Suppl):84-88.
22.Hachinski V. Preventable senility: a call for action against the vascular dementias.Lancet 1992;340:645-648.
23.Hachinski VC, Iliff LD, Zilhka E, et al. Cerebral blood flow in dementia. Arch Neurol1975;32:632-637.
24.Hachinski VC, Lassen NA, Marshall J. Multi-infarct dementia: a cause of mentaldeterioration in the elderly. Lancet 1974;2:207-210.
25.Hachinski VC, Potter P, Merskey H. Leuko-araiosis. Arch Neurol 1987;44:21-23.
26.Homma A, Hasegawa K. Recent developments in gerontopsychiatric research on ageassociated dementia in Japan. Int Psychogeriatr 1989;1:31-49.
27.Ishii N, Nichihara Y, Imamura T. Why do frontal lobe symptoms predominate invascular dementia with lacunes. Neurology 1986;36: 340-345.
28.Jellinger K. Cerebrovascular amyloidosis with cerebral hemorrhage. J Neurol1977;214:195-206.
29.Jorm AF, Korten AE, Henderson AS. The prevalence of dementia: a quantitativeintegration of the literature. Acta Psychiatr Scand 1987;76:465-479.
30.Juolasmaa A, Outakoski J, Hirvenoja R, Tienari P, Sotaniemi K, Takunen J. Effect ofopen heart surgery on intellectual performance. J Clin Neuropsychol 1981;3:181-197.
31.Kalaria RN, Bhatti SU, Palatinsky EA, et al. Accumulation of the beta amyloidprecursor protein at sites of ischemic injury in rat brain. Neuroreport 1993;4:211-214.
32.Kaplan JG, Katzman R, Horoupin DS, Field PA, Mayeux R, Mays AP. Progressivedementia, visual deficits, amyotrophy and microinfarcts. Neurology 1985;35:789-796.
33.Karasawa A, Homma A. Recent changes in the prevalence of dementia in the Tokyometropolis. In: Hasegawa K, Homma A, eds. Psychogeriatrics: biomedical and socialadvances. Tokyo: Excerpta Medica, 1990;24-29.
280

34.Kase CS. The epidemiology of multi-infarct dementia. Alzheimer's Dis Assoc Disord1991;5:71-76.
35.Katzman R, Lasker B, Bernstein N. Advances in the diagnosis of dementia: accuracy ofdiagnosis and consequence of misdiagnosis of disorders causing dementia. In: Terry RD,ed. Aging and the brain. New York: Raven Press, 1988;17-62.
36.Kitigawa Y, Meyer JS, Tachibana H, Mortel KF, Rogers RL. CT-CBF correlations ofcognitive deficits in multi-infarct dementia. Stroke 1984;15:1000--1009.
37.Kiyoto Y, Miyamoto M, Nagayoka A, Nagawa Y. Cerebral embolization leads tomemory impairment of several learning tasks in rats. Pharmacol Biochem Behav1986;24:687-692.
38.Kotsoris H, Barclay LL, Kheyfets S, Hulyalkar A, Dougherty J. Urinary and gaitdisturbances as markers for early multi-infarct dementia. Stroke 1987;18:138-141.
39.Lassen NA, Munck O, Tottey ER. Mental function and cerebral oxygen consumption inorganic dementia. Arch Neurol Psychiatry 1957;77:126-133.
40.Leonardi A, Gandolfo C, Caponetto C, Arata L, Vecchia R. The integrity of the blood-brain barrier in Alzheimer's type and multi-infarct dementia evaluated by the study ofalbumin and IgG in serum and cerebrospinal fluid. J Neurol Sci 1985;67:253-261.
41.Mahler ME, Cummings JL. The behavioral neurology of multi-infarct dementia.Alzheimer's Dis Assoc Disord 1991;5:122-130.
42.Mann DMA, Yates PO, Hawkes J. The noradrenergic system in Alzheimer and multi-infarct dementias. J Neurol Neurosurg Psychiatry 1982;45:113-119.
43.Marshall J. Vascular dementias. In: Whitehouse PJ, ed. Dementia. Philadelphia: FADavis, 1993;215-236.
44.McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinicaliagnosis of Alzheimer's disease: report of the NINCDS-ADRDA work group under theauspices of the Department of Health and Human Services Task Force on Alzheimer'sDisease. Neurology 1984;34:939-944.
45.Mendez MF, Ashla-Mendez M. Differences between multi-infarct dementia andAlzheimer's disease on unstructured neuropsychological tasks. J Clin Exp Neuropsychol1991;13:923-932.
46.Meyer JS, Judd BW, Tawaklna T, Rogers RL, Mortel KF. Improved cognition aftercontrol of risk factors for multi-infarct dementia. JAMA 1986;256:2203-2209.
47.Miller VT. Lacunar stroke: a reassessment. Arch Neurol 1983; 40:129-134.
281

48.Munoz DG. The pathological basis of multi-infarct dementia. Alzheimer's Dis AssocDisord 1991;5:77-90.
49.O'Brien M. Vascular dementia is underdiagnosed. Arch Neurol 1988;45:799.
50.Reinikainen KJ, Paljarvi L, Huuskonen M, et al. A post mortem study of noradrergic,serotonergic and GABAergic neurons in Alzheimer's disease. J Neurol Sci 1988;84:101-116.
51.Rogers RL, Meyer JS, Mortel KF, Mahurin RK, Judd BW. Decreased cerebral bloodflow precedes multi-infarct dementia, but follows senile dementia of the Alzheimer type.Neurology 1986;36:1-6.
52.Roman GC, Tatemichi TK, Erkinjuntti T, et al. Vascular dementia: diagnostic criteriafor research studies; report of the NINDS-AIREN International Workshop. Neurology1993;43:250-260.
53.Rothlind JC, Brandt J. A brief assessment of frontal and subcortical functions indementia. J Neuropsychiatry Clin Neurosci 1993;5:73-77.
54.Sato A, Sato Y. Regulation of regional cerebral blood flow by cholinergic fibersoriginating in the basal forebrain. Neurosci Res 1992:242-274.
55.Sharp PF, Gemmell HG, Besson JAO, Smith FW. Perfusion patterns in dementia. JNucl Med 1986;27:1939-1940.
Smyth K, Whitehouse PJ, Rust M, Kahana J. Epidemiology, diagnosis, and management ofAlzheimer's disease and related disorders: implications for minority populations. HealthMatrix 1988;4:28-32.
57.Sofroniew MV, Pearson RCA, Eckenstein F, Cuello AC, Powell TPS. Retrogradechanges in cholinergic neurons in the basal forebrain of the rat following cortical damage.Brain Res 1983; 289:370-374.
58.Spieth W. Cardiovascular health status, age and psychological performance. J Gerontol1964;19:277-284.
59.Tomlinson BE, Blessed G, Roth M. Observations on the brains of demented old people.J Neurol Sci 1970;11:205-242.
60.Wallin A, Blennow K. Pathogenetic basis of vascular dementia. Alzheimer's Dis AssocDisord 1991;5:91-102.
61.Whitehouse PJ. The concept of subcortical and cortical dementia: another look. AnnNeurol 1986;19:1-6.
282

62.Yamaguchi F, Meyer JS, Yamamoto M, Sakai F, Shaw T. Noninvasive regional bloodflow measurements in dementia. Arch Neurol 1980;37:410-418.
63.Yamanoucki H, Suguira S, Tomonage M. Decrease in nerve fibers in cerebral whitematter in progressive vascular encephalopathy of Binswanger type: an electron microscopystudy. J Neurol 1989;236:382-387.
The author: Professor Yasser Metwally
Professor Yasser Metwally, Ain Shams university, Cairo, Egypt
www.yassermetwally.com February 26, 2012
283

INDEX
INTRODUCTION &PATHOLOGY & AETIOLOGY
MR IMAGING OF SINUSTHROMBOSIS
RADIOLOGICAL PATHOLOGY OF CEREBRAL VENOUS & DURAL SINUSTHROMBOSIS
In the last 30 years, the introduction and widespread use of cerebral angiography, CT ofthe brain, and MRI have allowed early diagnosis of CVT, completely modifying ourknowledge of this condition.
More common than previously thought, CVT is remarkable by its large spectrum ofclinical presentation, its highly variable mode of onset, its numerous causes, and its
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
284

unpredictable but usually favorable outcome. CVT does remain a diagnostic andtherapeutic challenge for the clinician, however, because of its often misleadingpresentation and sometimes difficult treatment.
Dural sinus thrombosis accounts for approximately 1% to 2% of acute strokes in youngadults. Dural sinus thrombosis is associated with local and systemic diseases. Local diseasesinclude infectious processes, such as mastoiditis, sinusitis, osteomyelitis, and meningitis;trauma involving a dural sinus; neoplasms such as meningioma and calvarial andmeningeal metastases; and subarachnoid hemorrhage. Systemic processes includepregnancy, puerperium, and oral contraceptives; collagen vascular diseases such assystemic lupus erythematosus; and hematologic disorders, such as polycythemia,leukemia/lymphoma, sickle cell anemia, and other coagulopathies. Systemic diseases thatcause a hypercoagulable state are among the most common causes of dural sinusthrombosis. At least one third of cases are associated with pregnancy.
Depending on the degree and rate of the involvement of the cerebral veins, degree ofrecanalization, and collateral venous formation, the presentation can vary from a slowprocess to an acute episode. Signs and symptoms are nonspecific. Headache is the mostcommon presenting symptom and is seen in about 75% of patients. Other symptomsinclude nausea and vomiting, papilledema, and decreased level of consciousness.Involvement of the cerebral veins may cause hemorrhagic infarction, hemiplegia, andseizures. Rarely, patients may present with symptoms simulating transient ischemic attacksor subarachnoid hemorrhage.
Dural sinuses are formed by dural duplications and are fixed to the osseous skull. Becauseof absence of valves, blood can flow in different directions. The superior sagittal sinus joinsthe straight and lateral sinuses posteriorly forming the confluence of the sinuses. Lateralsinuses drain blood from the cerebellum, brain stem, and posterior parts of thehemispheres. The basal vein of Rosenthal drains both cortical and deep territories. Thecortical territory includes the posterior part of the frontal lobe, parahippocampal gyrus,anterior part of the cingulate gyrus, and part of the temporo-occipital cortex. The deepterritory includes the thalamus, basal nuclei, and deep brain structures. The basal vein ofRosenthal and internal cerebral veins join and form the vein of Galen, which drains intothe straight sinus.
RELEVANT VENOUS ANATOMY
Blood from the brain is drained by cerebral veins which empty into dural sinuses,themselves drained mostly by internal jugular veins.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
285

Dural Sinuses
Figure 1. Thevenousanatomy
The most commonly affected by thrombosis are the superior sagittal sinus, lateral sinuses,cavernous sinuses, and straight sinus.
o Superior Sagittal Sinus (SSS).
The SSS, triangular in cross-section, lies in the attached border of the falx cerebri. It startsat the foramen cecum and runs backward toward the internal occipital protuberance,where it joins with the straight sinus (SS) and lateral sinuses (LS) to form the torcularHerophili. Its anterior part is narrow or sometimes absent, replaced by two superiorcerebral veins that join behind the coronal suture. This is why the anterior part of the sinusis often poorly visualized at angiography and its isolated lack of filling is not sufficient toindicate thrombosis .
The SSS receives superficial cerebral veins and drains the major part of the cortex. It alsoreceives diploic veins, themselves connected to scalp veins by emissary veins, whichexplains some cases of SSS thrombosis after cutaneous infections or contusions. SSS andother sinuses play a major role in CSF circulation because they contain most of thearachnoid villi and granulations (Pacchionian bodies) in which CSF absorption takes place.The clear-cut consequence is a direct dependency of CSF pressure upon the intracranialvenous pressure, accounting for the frequently raised intracranial pressure in SSSthrombosis.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
286

o Lateral Sinuses (LS)
These extend from the torcular Herophili to jugular bulbs and consist of two portions: thetransverse portion, which lies in the attached border of the tentorium, and the sigmoidportion, which runs on the inner aspect of the mastoid process and is thus susceptible toinfectious thrombosis in patients with mastoiditis or otitis media. LS drains blood from thecerebellum, brain stem, and posterior part of the cerebral hemispheres. They also receivesome of the diploic veins and some small veins from the middle ear, another possible sourceof septic thrombosis.
There are numerous LS anatomic variations that may be misinterpreted as sinus occlusionat angiography. In particular, the right LS is frequently larger than the left, which receivesmost of its supply from the straight sinus. An isolated lack of filling of the transverseportion of left LS is thus more suggestive of hypoplasia than thrombosis.
o Cavernous Sinuses
Cavernous sinuses consist of trabeculated cavities formed by the separation of the layers ofthe dura and located on each side of sella turcica, superolaterally to the sphenoid airsinuses. The oculomotor and trochlear cranial nerves, along with the ophthalmic andmaxillary branches of the trigeminal nerve, course along the lateral wall of the cavernoussinuses, whereas the abducent nerve and the carotid artery with its surroundingsympathetic plexus are located within the center of the sinus itself.
Cavernous sinuses drain the blood from the orbits through the ophthalmic veins and fromthe anterior part of the base of the brain by the sphenoparietal sinus and the middlecerebral veins. They empty into both the superior and inferior petrosal sinuses andultimately into the internal jugular veins. Because of their situation, cavernous sinuses areoften thrombosed in relation to infections of the face or sphenoid sinusitis and, by contrastto other varieties of sinus thrombosis, infection is still the leading cause. Rarely injected oncarotid angiograms, cavernous sinuses are now well visualized on CT scans and MRI.
o Straight Sinus
Formed by the union of the inferior sagittal sinus and the great vein of Galen, it has atriangular lumen and runs caudally in the junction between the falx cerebri and thetentorium cerebella to join the torcular at the internal occipital protuberance.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
287

Figure 2. Sagittal contrast-enhanced MR venogram MIP image of the deep cerebral veinsand dural sinuses in a normal patient. SSS = superior sagittal sinus; To = torcularherophili or confluence of sinuses; S = straight sinus; G = great vein of Galen; I = inferiorsagittal sinus; TH = thalamostriate veins; ICV = internal cerebral veins; R = basal vein ofRosenthal; L = vein of Labbe; TS transverse sinus; SG = sigmoid sinus; SP superiorpetrosal sinus; IP = inferior petrosal sinus; CS = cavernous sinus; sps = spheno-parietalsinus; PP = pterygoid plexus of veins; J = internal jugular vein; sov superior ophthalmicvein; C = internal carotid artery; and B = basilar artery,
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
288

Figure 3. Coronal contrastenhanced MR venogram MIPimage shows many of the duralsinuses and a few of the deepcerebral veins. SSS = superiorsagittal sinus; To = torcularherophili or confluence ofsinuses; R = basal vein ofRosenthal; L = vein of Labbe;DMV = deep middle cerebralvein; TS = transverse sinus; SG= sigmoid sinus; SPS =superior petrosal sinus; J =internal jugular vein; Cinternal carotid artery; V =vertebral artery; JB jugularbulb; IJ = internal jugularvein; CV cortical veins.
Cerebral Veins
Three groups of veins drain the blood supply from the brain:
o Superficial Cerebral Veins (or cortical veins)
Some of these - the frontal, parietal, and occipital superior cerebral veins - drain the cortexupward into the SSS, whereas others, mainly the middle cerebral veins, drain downwardinto the cavernous sinuses. These veins are linked by the great anastomotic vein of Trolard,which connects the SSS to the middle cerebral veins, which are themselves connected to theLS by the vein of Labbe. These cortical veins have thin walls, no muscle fibers, and novalves, thereby permitting both dilation and reversal of the direction of blood flow whenthe sinus in which they drain is occluded. They are linked by numerous anastomoses,allowing the development of a collateral circulation (angiographically visible as "cork-screw" vessels) and probably explaining the good prognosis of some CVT. Since thenumber and location of cortical veins are inconstant, the angiographic diagnosis of isolatedcortical vein thrombosis is extremely difficult and sometimes impossible.
o Deep Cerebral Veins
Blood from the deep white matter of the cerebral hemispheres and from the basal gangliais drained by internal cerebral and basal veins, which join to form the great vein of Galenthat drains into the straight sinus. By contrast to the superficial veins, the deep system isconstant and always visualized at angiography, so its thrombosis is easily recognized.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
289

o Posterior Fossa Veins
The veins of the posterior fossa may be divided into three groups ,superior draining intothe galenic system, anterior draining into petrosal sinus, and posterior draining into thetorcular and neighboring straight and lateral sinuses. They are variable in course, andangiographic diagnosis of their occlusion is extremely difficult.
Pathophysiology of cerebral sinus thrombosis and its parenchymal changes
The pathophysiology of brain parenchymal involvement in venous occlusion differs fromthat in arterial occlusion. Parenchymal changes may be secondary to cytotoxic edema,vasogenic edema, or intracranial hemorrhage. The primary underlying mechanism is likelyto be increased venous pressure. If collateral pathways of venous drainage are insufficient,especially in the presence of cortical venous involvement, subsequent parenchymal changesmay occur. If venous pressure continues to increase, with a consequent diminishment inarterial perfusion pressure, cell death may ensue. If adequate collateral pathways developor recanalization occurs before cell death or intracranial hemorrhage, the parenchymalchanges may resolve partly or completely. Vasogenic and cytotoxic edema patterns maycoexist
Table 1. Effect of increased intracranial venous pressure due to sinovenous thrombosis.
Comment
Venous thrombosis produce effects on the vein that include increase in diameter andlength of the thin walled vein, kinking, folding, stenosis, and sometimes occlusion. Thishas been described as a hemodynamic effect caused by pressure and flow of arterialblood in a vein.
In the presence of venous thrombosis, a subpial or cortical vein dilates, lengthens, andmay kink at the junction with the sinus. It may also balloon to the point of rupture orthromboses The deep venous collector in the galenic malformations (the embryonicprecursor to the vein of Galen) typically shows a dilatation and focal stenosis at the outletto the straight sinus or a falcine sinus. Occasionally, this structure spontaneouslythromboses.
Under normal conditions, there is negative venous pressure in the dural sinuses relativeto the heart. There are no valves and pulsatile flow in the sinuses. Blood is effectivelysucked through the shunt rather than pushed. An increased resistance to flow occurswhen the venous pressure rises. This may occur transiently during a Valsalva maneuveror chronically in severe right heart failure or when there is a stenosis in the venoussinuses due to sinus thrombosis. When there is increased venous pressure, there is acorresponding decrease in water resorption by the arachnoid granulations, which isreflected in an increased amount of water in the ventricles and subarachnoid spaces. Thethird and lateral ventricles become prominent, and the cerebral sulci enlarge. If thefontanelles are open, the head enlarges (macrocrania). Normally, the posterior fossadrainage relies on the petrosal sinuses draining anteriorly to the cavernous sinus andcaudally to the jugular bulb. In the absence of anterior drainage and restricted caudal
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
290

drainage, there is an increase in cerebellar water, which results in a small fourthventricle and tonsillar herniation.
With persistent increase of the venous pressure due to venous thrombosis, there will bereduction of the venous return, stasis of blood, or even reversal of flow of blood (cerebralvenous reflux) depending on the degree of venous pressure rise. Stasis of blood in thevenous sinuses predisposes to further thrombosis. Cerebral venous reflux predisposes todilatation of superficial, deep venous system, transcerebral vein, white matter congestiveencephalopathy with edema, petechial haemorrhages and mass effect. Increase ofintravenous pressure often results in venous wall remodelling with increase in diameterand length of the thin walled vein, kinking, folding, stenosis, and sometimes occlusion ofthrombosis.
Venous infarction or ischemic cerebral changes can occur due to increased venouspressure -secondary to venous thrombosis, the mechanism for venous infarction isobstruction of venous drainage with increasing venous pressure in the affected region ofthe brain. The venous congestion results in significant extravasation of fluid into thebrain, producing focal cerebral edema and hemorrhage. The edema may be transient, ifvenous flow is re-established, or be associated with permanent tissue infarction if theincreased venous blood pressure eventually exceeds the arterial blood pressure. In thelatter situation, there is insufficient delivery of arterial blood and regional ischemicinfarction. MR imaging studies utilizing diffusion-weighted imaging (DWI) havedemonstrated cytotoxic edema early in acute venous thrombosis, preceding the onset ofvasogenic edema. These findings support the presence of primary neuronal injury earlyin venous infarction.
Under normal conditions, there is negative venous pressure in the dural sinuses relative tothe heart. There are no valves and pulsatile flow in the sinuses. Blood is effectively suckedthrough the shunt rather than pushed. An increased resistance to flow occurs when thevenous pressure rises. This may occur transiently during a Valsalva maneuver orchronically in severe right heart failure or when there is a stenosis in the venous sinusesdue to sinus thrombosis. Venous hypertension probably passes into three stages dependingupon the degree of venous hypertension and the chronicity of the condition.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
291

Table 2. Stages of cerebral venous hypertension
Stage I
Absence of anyparenchymalchanges
When there is increased venous pressure, there is a correspondingdecrease in water resorption by the arachnoid granulations, which isreflected in an increased amount of water in the ventricles andsubarachnoid spaces. The third and lateral ventricles become prominent,and the cerebral sulci enlarge. If the fontanelles are open, the headenlarges (macrocrania). Normally, the posterior fossa drainage relies onthe petrosal sinuses draining anteriorly to the cavernous sinus andcaudally to the jugular bulb. In the absence of anterior drainage andrestricted caudal drainage, there is an increase in cerebellar water, whichresults in a small fourth ventricle and tonsillar herniation. At this stagethe thrombosed sinus will show the characteristic MRI signal changes butwithout any parenchymal changes.
Stage II
Early cerebralcongestiveencephalopathywith reversibleparenchymalchanges
With persistent increase of the venous pressure due to venous thrombosis,there will be reduction of the venous return, stasis of blood, or evenreversal of flow of blood (cerebral venous reflux) depending on the degreeof venous pressure rise. Stasis of blood in the venous sinuses predisposesto further thrombosis. Cerebral venous reflux predisposes to dilatation ofsuperficial, deep venous system, transcerebral vein, white mattercongestive encephalopathy with edema, petechial haemorrhages and masseffect. Increase of intravenous pressure often results in venous wallremodelling with increase in diameter and length of the thin walled vein,kinking, folding, stenosis, and sometimes occlusion of thrombosis.Parenchymal changes in this stage are due to reversible edema edemaand petechial hemorrhage once venous flow is restored
Stage III
Late cerebralcongestiveencephalopathywith irreversibleparenchymalchanges
Venous infarction or ischemic cerebral changes can occur due toincreased venous pressure -secondary to venous thrombosis, themechanism for venous infarction is obstruction of venous drainage withincreasing venous pressure in the affected region of the brain. The venouscongestion results in significant extravasation of fluid into the brain,producing focal cerebral edema and hemorrhage. The edema may betransient, if venous flow is re-established, or be associated withpermanent tissue infarction if the increased venous blood pressureeventually exceeds the arterial blood pressure. In the latter situation,there is insufficient delivery of arterial blood and regional ischemicinfarction. MR imaging studies utilizing diffusion-weighted imaging(DWI) have demonstrated cytotoxic edema early in acute venousthrombosis, preceding the onset of vasogenic edema. These findingssupport the presence of primary neuronal injury early in venousinfarction.
Acute dural sinus thrombosis leads to distinct stages of parenchymal changes, the severityof which depends on the degree of venous congestion, which, in turn, is closely related tointradural sinus pressure. As intradural sinus pressure increases, progression from mild
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
292

parenchymal change to severe cerebral edema and/or hematoma may occur if thrombolysisis delayed.
In the analysis of 29 patients with dural sinus thrombosis (by MRI, and dural sinuspressure measurement using a Tracker 18 end-hole catheter proximal to the thrombus andconnected to a pressure transducer at ear level with the waveform displayed on either anAlpha 9 pressure monitor) , Fong, at al, [30] could identify five stages of brain parenchymalchanges secondary of sinus thrombosis, each stage relates to the dural intrasinus pressure.See table (3)
Table 3. Parenchymal changes, and intrasinus pressure in dural sinus thrombosis [30]
Acute dural sinus and cerebral venous thrombosis may lead to various stages ofparenchymal changes of venous infarction, with the degree of severity depending on thedegree of venous congestion and elevated dural sinus pressure. The prognosis of venousthrombosis depends to a significant extent on the use of thrombolytics. Severe neurologicsymptoms, including coma, may be reversible if treatment with thrombolytics is startedbefore massive cerebral edema or hemorrhage has developed. Stage I may be treated withanticoagulants alone; however, if the patient deteriorates clinically, prompt thrombolysis isprobably needed. All other stages should be treated with thrombolysis. A progression frommild brain swelling to severe cerebral edema and/or hemorrhage from increasing duralsinus pressure may occur if treatment with thrombolysis is delayed. [30]
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
293

Table 4. Biochemical stages of sinus thromboses
STAGE MRI PICTURE
The acutedeoxyhemoglobinstage of bloodproducts
(days I through5)
In the acute stage of thrombus formation (0–5 days), the signal ispredominantly isointense on T1-weighted images and hypointense onT2-weighted images because of deoxyhemoglobin in red blood cellstrapped in the thrombus. A venous thrombus in the acute stage mayhave a signal intensity that mimics a normal flow state, and such afinding may lead to diagnostic error. The signal may be veryhypointense on T2-weighted images and may be mistakenly thought toindicate a flow void. According to some estimates, in 10%–30% of casesof sinus thrombosis, the thrombus at initial presentation or imagingexamination is in the acute stage of formation. Contrast-enhanced MRvenography or CT venography is usually necessary to achieve adefinitive diagnosis at this stage.
The subacuteextracellularmethemoglobinstage of bloodproducts (fromday 5 throughday 15)
In the subacute stage of thrombus development (6–15 days), the signal ispredominantly hyperintense on both T1-weighted images and T2-weighted images because of methemoglobin in the thrombus. Subacute-stage thrombus has been found in 55% of patients at clinicalpresentation with cerebral venous thrombosis. This stage of formation isthe easiest stage at which to detect a thrombus on MR images, as thesignal intensity of the sinus is most different from that in normal flowstates. The finding of increased signal intensity on both T1-weightedimages and T2-weighted images is almost always abnormal.
Chronic duralsinus thrombosis
The thrombus becomes hypointense and heterogeneous because ofpartial resolution and recanalization and might enhance aftergadolinium administration. Enhancement within the occluded duralsinus is due to organization of the thrombus.
Chronic thrombosis with incomplete recanalization of the sinus maypresent a diagnostic challenge at MR imaging. As many as 15% ofpatients in whom sinus thrombosis is diagnosed at MR imaging mayhave a chronic (>15-day-old) thrombus. Compared with the MR signalin normal brain parenchyma, the signal in a chronic thrombus istypically isointense or hyperintense on T2-weighted images andisointense on T1-weighted images; however, significant variability inthrombus signal intensity exists. The signal intensity may be similar tothat of very slowly moving oxygenated blood.
Sinus enhancement in sinus thrombosis is presumably secondary to an organized thrombuswith intrinsic vascularization as well as to slow flow in dural and intrathrombus collateralchannels.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
294

Parenchymal changes secondary to congestive encephalopathy are shown by MRI assubcortical white matter precontrast T1 hypointensity, with patchy, irregular and linearenhancement and T2 hyperintensity mixed with linear and patchy hypointensity and signalvoid structures. Changes are due to edema, petechial hemorrhages and dilated veins.Parenchymal changes commonly show positive mass effect and are usually focal ratherthan diffuse. Bilateral parenchymal changes are not uncommon. Although parenchymalchanges may occur in areas of the brain that are directly drained by the occluded venoussinus, in some patients the parenchymal changes may not closely correlate with the locationof venous occlusion.
Parenchymal swelling without abnormalities in attenuation or signal intensity on imagesmay occur in as many as 42% of patients with cerebral venous thrombosis. Sulcaleffacement, diminished cistern visibility, and a reduction in ventricular size may occur.Patients with brain swelling and without parenchymal signal intensity changes tend to haveintrasinus pressures in the intermediate range (20–25 mm Hg); however, intrasinuspressures also may be markedly elevated. Such patients typically have more prominentclinical symptoms than would be expected on the basis of imaging findings.
In view of the variable nature of the parenchymal abnormalities that may occur in cerebralvenous thrombosis, the use of the term venous infarct in reference to these lesions should bediscouraged because that term implies irreversibility. In contrast with arterial ischemicstates, many parenchymal abnormalities secondary to venous occlusion are reversible. It ismuch better to refer to these parenchymal changes secondary to cerebral sinus thrombosisas cerebral venous encephalopathy. Persistence of parenchymal MRI signal changes over along time might warrant the usage of the terminology venous infarction.
Parenchymal hemorrhage in cerebral sinus thrombosis
Parenchymal hemorrhage can be seen in one-third of cases of cerebral venous thrombosis.Flame-shaped irregular zones of lobar hemorrhage in the parasagittal frontal and parietallobes are typical findings in patients with superior sagittal sinus thrombosis and shouldprompt additional imaging evaluations (eg, with MR venography or CT venography).Hemorrhage in the temporal or occipital lobes is more typical of transverse sinus occlusion.Hemorrhage in cerebral venous thrombosis is typically cortical with subcortical extension.Smaller zones of isolated subcortical hemorrhage also may be seen and may beaccompanied by minimal edema. MR imaging with GRE sequences is sensitive in thedepiction of these zones of parenchymal hemorrhage.
The mechanism of hemorrhage in cerebral venous thrombosis is multifactorial.Hemorrhage may be precipitated by continued arterial perfusion in areas of cell death, ascan be seen at reperfusion in arterial ischemia. Elevation of venous pressure beyond thelimit of the venous wall also is likely operative. Hemorrhage was noted in patients withintrasinus pressures higher than 42 mm Hg but not in those with lower pressures.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
295

Contrast Enhancement
Parenchymal enhancement in 1%–29% of cases of cerebral venous thrombosis has beenreported. The enhancement is typically gyral in location and may extend into the whitematter. Parenchymal enhancement, which indicates disruption of the blood-brain barrier,may be seen in areas of cytotoxic or vasogenic edema and in the presence of eitherirreversible or reversible brain abnormalities. Increased tentorial enhancement (likelyrelated to dural venous collaterals), adjacent leptomeningeal enhancement, and prominentcortical venous enhancement (secondary to venous congestion) also may be visible after theadministration of contrast material.
Figure 4. Axial MR image series with a color overlay represents the majorsuperficial cortical venous drainage territories. Most of the superior cerebrum(green) is drained primarily into the superior sagittal sinus, which also receivesdrainage from the parasagittal cortical regions at lower levels. The sylvian veinsdrain blood from the peri-insular region (yellow) into the basal dural sinuses. Thetransverse sinuses receive blood from the temporal, parietal, and occipital lobes(blue). The Labbé vein, if dominant, may drain much of this territory. Parenchymalabnormalities such as hemorrhage or edema in this territory may be indicative ofthrombosis of the transverse sinus or Labbé vein.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
296

Figure 5. Axial MR imagewith color overlay showsthe drainage territory ofthe deep cerebral veins(internal cerebral vein,vein of Galen) (pink), inwhich parenchymalabnormalities due to deepvenous occlusion typicallyare found. The deepwhite matter (medullary)venous drainage territory(blue) also is shown.
PATHOLOGY
Pathologic findings have been extensively described in the past. They vary with the site ofthrombosis and the interval between the onset of symptoms and death.
The thrombus itself is like other venous thrombi elsewhere in the body. When it is fresh, itis a red thrombus rich in red blood cells and fibrin and poor in platelets; when it is old, it isreplaced by fibrous tissue sometimes showing recanalization. Its formation is due to theusual pathogenetic factors: venous stasis, increased clotting tendency, changes in the vesselwall, and, less frequently, embolization. Its location and extension are variable. In autopsyseries, extensive thrombosis of SSS and tributary veins is the most frequent finding, butthis pattern of involvement no longer reflects the real distribution of CVT.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
297

Figure 6. Bilateral hemorrhagic venous infarction (A) due to superior sagittal thromboses(B)
The consequences of CVT on the brain are again highly variable. The classic picture is thatof SSS thrombosis with extensive bilateral hemorrhagic infarcts affecting the cortex andadjacent white matter. CT scan and MRI studies have now convincingly shown, however,that sinus thrombosis can induce varying degrees of edema without infarction and can evenhave no detectable effect on the brain.
Figure 7. Superior sagittal sinus thromboses (A), with dilated thrombosed cortical veinsradiating to the thrombosed sinus and forming what is termed radiologically the "cordsign".
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
298

INCIDENCE
The true incidence of CVT is totally unknown in the absence of specific epidemiologicstudies. In most autopsy series, the incidence was found to be extremely low. It has beensuggested that the incidence of CVT is higher in females and in the aged, reflecting theoverall greater incidence of thromboembolic diseases in these categories. The agedistribution is uniform in men, whereas in women it frequently occurred between 20 and35. This probably reflects the frequency of specific causes such as pregnancy and oralcontraceptive use in young women.
ETIOLOGY
Numerous conditions can cause or predispose to CVT. They include all surgical, gyneco-obstetric, and medical causes of deep vein thrombosis as well as a number of local orregional causes, either infective or noninfective, such as head trauma, brain tumors, andarterial infarcts. Although infection still constituted the major identifiable cause ,theincidence of septic CVT has greatly diminished in developed countries since theintroduction of antibiotics. Cavernous sinus thrombosis remains the most common form ofseptic thrombosis, usually following an infection of the middle third of the face due toStaphylococcus aureus. Other sites of infection include sphenoid or ethmoid sinusitis,dental abscess, and, less often, otitis media. In chronic forms, gram-negative rods and fungisuch as Aspergillus species are more commonly isolated. Among general causes, parasiticinfections such as trichinosis and more recently HIV and CMV infections have been addedto the long list of infective conditions possibly leading to CVT.
In young women, CVT occurs more frequently during puerperium than pregnancy andremains very common in developing countries, whereas in developed countries the role oforal contraceptives is more important.
Among the numerous noninfective medical causes of CVT, malignancies,and inflammatorydiseases such as Behcet's disease and connective tissue diseases are the most frequent.Although rare, hereditary antithrombin III, protein C,and protein deficiencies should besystematically looked for in the absence of obvious cause because they imply a family studyand a long-term treatment.
In neonates and children, the etiology of CVT is characterized by the frequency of regionalinfections (otitis, mastoiditis), neonatal asphyxia, severe dehydration, and congenital heartdisease.
Despite the continuous description of new causes, the proportion of cases of unknownetiology constitute about one third of cerebral venous thrombosis.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
299

TOPOGRAPHIC DIAGNOSIS
Thrombosis most frequently affects (in order of decreasing frequency) SSS, LS, andcavernous sinus. In most cases, thrombosis affects several sinuses or sinuses and cerebralveins. Thrombosis of the galenic system is rare.
The frequent association of sinus and cerebral vein thrombosis explains the lack of well-defined topographic clinical syndromes, similar to those described in arterial occlusions.Thus, SSS thrombosis can present with any of the above described patterns; this alsoapplies to LS thrombosis, in which isolated intracranial hypertension is probably evenmore frequent and, among focal signs, dysphasia is not unusual. Thrombosis of the petrosalsinuses was described in the old literature and was characterized mainly by a fifth nervepalsy for the superior sinus and by a sixth nerve palsy for the inferior one.
As already stressed, angiographic diagnosis of isolated cortical vein thrombosis isextremely difficult, but there are old reports of anatomic or surgical cases in patientspresenting with an acute or rapid onset of focal deficits, seizures, or both. The classicpicture of deep cerebral venous thrombosis is that of an acute coma with decerebration orextrapyramidal hypertonia leading to death in a few days or resolving, but with heavysequelae such as akinetic mutism, dementia, bilateral athetoid movements, vertical gazepalsy, and dystonia. Recent reports have illustrated benign forms presenting mainly withconfusion. The few reported cases of cerebellar vein thrombosis are mainly anatomic butwe reported a patient presenting with a 3-month history of cranial nerve palsies, cerebellarincoordination, and papilledema simulating a posterior fossa tumor.
MR IMAGING OF SINUS THROMBOSIS
On contrast-enhanced computedtomography (CT) and MR imagingdural sinus thrombosis typicallyappears as a filling defect in thedural sinus, also known as emptydelta sign. The empty delta sign isdue to enhancement of thesurrounding falx with thehypodense central clot. A similarfindings can be observed in MRimaging.
The empty delta sign has high specificity but low sensitivity. It is seen in only 30% of casesof sagittal sinus thrombosis. Hyperdense cortical veins (cord sign) may also be present. CTand MR imaging may also detect causes such as infection, trauma, or neoplasm. Imagingstudies can also be helpful in the detection of complications such as diffuse edema orvenous infarctions, which are often hemorrhagic. On MR imaging, dural sinus thrombosisis most commonly manifested as lack of the normal flow void within the dural sinuses.Affected dural sinuses demonstrate abnormal intraluminal signal, which varies depending
Empty delta sign 21%
Contrast enhancement of falx ortentorium
19%
Small ventricles 52%
Enlarged ventricles 3%
Spontaneous hyperintensity 20%
Hypointensity 33%
Gyral enhancement 25%
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
300

on the stage of the thrombus. In the acute stage (days I through 5), the thrombus isisointense to the brain on Tl-weighted images and strongly hypointense on T2-weightedimages because of the deoxyhemoglobin stage of blood products. Because of the low signalof acute thrombus on T2-weighted images, acquisition of only T2-weighted images maygive a false impression of normal flow void.
Figure 8. Coronal contrast-enhanced Tl -weighted images showisointense thrombus (arrow) within the superior sagittal sinuswith increased enhancement of the superior sagittal sinusleaves indicating increased vascularization without evidence ofrecanalization. There is also enhancement of the left transversesinus reflecting partial thrombosis. There is peripheralenhancement of the right parietal infarct (open arrows). Thedura, falx cerebri, and tentorium cerebella show irregularenhancement.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
301

Figure 9. MRI T1postcontrast study showingwidespread enhancement ofthe dural sinuses andcortical veins. Intra-sinuseshypointense filling defectsare due to nonenhancementof the thrombus. Signalchanges in the upper brainstem is probably due toischemia
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
302

In the subacute stage (from day 5 through day 15), the thrombus is hyperintense on bothTl-weighted and T2-weighted images because of the extracellular methemoglobin stage ofblood products. Signal changes evolve from the periphery to the central portion of thethrombus. By the third week, signal changes of the thrombus are different from anintracranial bleed. The thrombus becomes hypointense and heterogeneous because ofpartial resolution and recanalization.
Figure 10. A, Sagittal T1 -weighted images show increased signal intensity in the superiorsagittal sinus (arrowheads), anterior portion of the straight sinus (small arrow), and vein ofGalen (big arrow), consistent with subacute thrombosis, B MRI T1 precontrast and , C,MRI T2 image showing right parasagittal subcortical hemorrhagic infarct in the parietallobe. The superior sagittal sinus shows isointense signal intensity consistent with thrombusin methemoglobin stage a case of dural sinus thrombosis with subcortical hemorrhagicinfarct of the right parietal region
Dural sinus thrombosis may beassociated with venous infarctions,which are frequently hemorrhagic.Venous infarctions
characteristically have a subcortical location and do not follow a major arterial vascularterritory. Infarctions resulting from thrombosis of the internal cerebral vein or straightsinus are usually deep within the brain, such as the thalami. Dilated collateral cortical andmedullary veins may be visible as prominent signal voids. On contrast-enhanced MRimaging, the empty delta sign representing the intraluminal clot may be seen. Withorganization and recanalization of the thrombus, enhancement of the thrombus may beseen. The tentorium and falx may also show enhancement resulting from vascularcongestion in the collateral venous channels. With obstruction of the venous system,cerebral edema and infarction may develop. It can be manifested as increased signalintensity on T2-weighted images. It may be associated with hemorrhage, which is mostcommonly seen in the parietal and parieto-occipital areas. The underlying venous stasis canlead to abnormal enhancement of the cortical or deep venous structures.
Infarctions resulting from thrombosis of the internalcerebral vein or straight sinus are usually deep within thebrain, such as the thalami.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
303

Figure 11. MRI T2 (A,B,C) and FLAIR studies (D,E,F,G,H,I)showing bilateral deep cerebral, paraventricular, basal ganglionicand thalamic signal changes representing subacute venousinfarctions due to thrombosis of the deep venous systems
Flow in the dural sinuses may be depicted with MR venography using different techniques,such as time-of-flight, phase-contrast, or gradient-echo imaging sensitive to flow.Intraluminal hyperintensity seen with subacute thrombus cannot be distinguished from
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
304

flow hyperintensity on time-of-flight images; therefore this technique should be usedcautiously when there is intraluminal increased signal intensity on Tl-weighted images. Toavoid saturation of the venous structures, contrast-enhanced three-dimensional time-of-flight MR angiography may improve the visibility of the venous structures.
Table 5. Biochemical stages of sinus thromboses
STAGE MRI PICTURE
The acute deoxyhemoglobin stage ofblood products
(days I through 5)
The thrombus is isointense to the brain on Tl-weighted images and strongly hypointense on T2-weighted images because of the deoxyhemoglobinstage of blood products. Because of the low signal ofacute thrombus on T2-weighted images, acquisitionof only T2-weighted images may give a falseimpression of normal flow void.
The subacute extracellularmethemoglobin stage of bloodproducts (from day 5 through day15)
The thrombus is hyperintense on both Tl-weightedand T2-weighted images because of the extracellularmethemoglobin stage of blood products. Signalchanges evolve from the periphery to the centralportion of the thrombus. By the third week, signalchanges of the thrombus are different from anintracranial bleed. The thrombus becomeshypointense and heterogeneous because of partialresolution and recanalization.
Chronic dural sinus thrombosis
The thrombus becomes hypointense andheterogeneous because of partial resolution andrecanalization and might enhance after gadoliniumadministration. Enhancement within the occludeddural sinus is due to organization of the thrombus.
Figure 12. MRI FLAIR study (A)showing bilateral deep cerebral,paraventricular signal changesrepresenting subacute venousinfarctions due to thrombosis of thedeep venous systems. B, MRI T1postcontrast showing the emptydelta sign.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
305

There are a number of pitfalls in the diagnosis of dural sinus thrombosis that should beconsidered. Flow-related enhancement occurs when unsaturated protons enter the imagingplane and produce increased signal intensity relative to the more saturated protons in theadjacent soft tissues. It is identified on Tl- weighted images within dural venous structuresoriented perpendicular to the scanning plane. It is more commonly seen in the sigmoidsinus and jugular bulb. The same findings may be seen in the cortical veins near thesuperior sagittal sinus on sagittal images. Changing of slice orientation with constantsequence parameters resolves the flow artifact. With normal flow, the signal intensitywithin the dural sinus changes . Extremely slow flow can also produce an intraluminalsignal.
Figure 13. MRI T1 postcontrast study showing dural sinus, cortical venous dilations andenhancement due to widespread dural sinus & cerebral venous thrombosis. The enhancedcortical veins are seen forming the hyperdense cord signs which are seen radiating to thedilated and thrombosed dural sinuses. Also notice parenchymal subcortical hypointensitiesand patchy, irregular enhancement which could be due to edema, infarction or ischemia.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
306

Increasing TR and TE diminishes this artifact. The anterior portion of the superior sagittalsinus may be hypoplastic or completely absent. The transverse sinuses are typicallyasymmetric, with the right usually larger than the left. One of the transverse sinuses maybe completely absent. Hypoplasia or absence of a dural venous structure may result in afalse positive result.
Figure 14. MRI T1 postcontrast study showing enhancement and dilation of thethrombosed superior sagittal sinus with central hypointense filling defects which could bedue to the intraluminal thrombi. Dilated enhanced cortical veins are seen pouring in thethrombosed sinus, subcortical parenchymal hypointensity could be due to edema orinfarction
In patients with chronic dural sinus thrombosis, the thrombus enhances after gadoliniumadministration. Enhancement within the occluded dural sinus is due to organization of thethrombus. The thrombus is vascularized as a result of invasion by fibroblasts andcapillaries. This vascularization could lead to false negative results in patients with chronicdural sinus thrombosis using contrast-enhanced MR and time-of-flight MR Angiographytechniques. Phase-contrast (with or without contrast) and time-of-flight (without contrast)MR angiography are preferred methods for evaluation of patients with dural sinusthrombosis.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
307

Figure 15. MRI T2 images (A,B) and FLAIR (c) showing diffuse left hemisphericalcortical/subcortical hyperintensities and mass effect due to widespread dural sinuses &cortical veins thromboses. Signal changes are due to edema, ischemia and infraction. Mostof the parenchymal signal changes are due to edema in the acute stage of sinus thromboses.
SUMMARY
Radiological sign Comment
Empty delta sign Thrombosis typically appears as a filling defect in the dural sinus,also known as empty delta sign. The empty delta sign is due toenhancement of the surrounding falx with the hypodense centralclot left unenhanced.
Hyperintense(precontrast MRI T1 )cortical veins (cordsign)
Dilated collateral cortical and medullary veins may be visible asprominent signal voids when not thrombosed. However whenthese veins are thrombosed they follow the same time-sensitivesignal changes of the thrombosed dural sinuses. In the subacutestage of extracellular methemoglobin these veins are dilated andhyperintense on noncontrast MRI T1 studies. Enhancement of thecortical veins may also form the cord sign.
Edema With obstruction of the venous system, cerebral edema maydevelop. It can be manifested as increased signal intensity on T2-weighted images and can result in herniations.
Venous infarctions Hemorrhagic venous infarctions characteristically have asubcortical location and do not follow a major arterial vascularterritory. Infarctions resulting from thrombosis of the internalcerebral vein or straight sinus are usually deep within the brain,such as the thalami, the basal ganglia or the paraventricularregions.
Affected dural sinuses 1. In the acute stage (days I through 5), the thrombus is
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
308

demonstrate abnormalintraluminal signal,which varies dependingon the stage of thethrombus.
isointense to the brain on Tl-weighted images and stronglyhypointense on T2-weighted images because of thedeoxyhemoglobin stage of blood products.
2. In the subacute stage (from day 5 through day 15), thethrombus is hyperintense.
3. The thrombus becomes hypointense and heterogeneousbecause of partial resolution and recanalization and mightenhance after gadolinium administration. Withorganization and recanalization of the thrombus,enhancement of the thrombus may be seen.
Dural enhancement The tentorium and falx may may show enhancement resultingfrom vascular congestion in the collateral venous channels.
Venous stasis The underlying venous stasis can lead to abnormal enhancementof the cortical or deep venous structures. It can also result inedema, ischemia of cerebral infarctions.
Thrombusenhancement
Enhancement within the occluded dural sinus is due toorganization of the thrombus. The thrombus is vascularized as aresult of invasion by fibroblasts and capillaries.
Parenchymalenhancement
Could be due to cerebral ischemic changes, or frank cerebralvenous infarction (it occurs due to vascular endothelial damage)
Parenchymal T2hyperintensities,precontrast T1hypointensities
Could be due to cerebral edema, ischemia or cerebral venousinfarctions. Parenchymal signal changes in the acute stage of sinusthromboses (especially when associated with mass effect) aremainly due to cerebral edema and might completely disappearlater on.
MEDICATION
Heparin should be considered seriously in the management of CVT. Conversion towarfarin as maintenance therapy is then suggested. Subcutaneous low-molecular-weightheparin (Lovenox) also has been used in patients with venous sinus thrombosis.
Thrombolytic therapy may be useful, but all studies so far describe its use only with localinstillation by microcatheter or direct instillation at the time of surgical thrombectomy.
Drug Category: Anticoagulants - These medications are used to prevent propagation of theclot to more extensive areas of the cerebral venous system. Studies indicate a tendencytoward better outcome in patients treated with anticoagulant therapy than in those who arenot treated with anticoagulants. In Einhaupl's study, even patients with cerebralhemorrhage appeared to benefit from anticoagulation.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
309

Drug Name
Heparin (Hep-Lock)- Increases the action ofantithrombin III, leading to inactivation ofcoagulation enzymes thrombin, factor Xa, andfactor IXa. Thrombin is the most sensitive toinactivation by heparin. Because heparin is notabsorbed from the GI tract, it must be givenparenterally. When given IV, effect is immediate.Metabolism of heparin is complex; rapid zero-order metabolism is followed by slower first-orderrenal clearance. Zero-order process is saturable,leading to an increase in half-life from 30-150min as dose increased. Weight-based protocolnow often used for dosing. When choosing thistherapy, risks of its contraindications must beweighed against potential benefits.
Adult Dose
Loading dose: 80 U/kg IV bolus followed byinfusionInitial infusion: 18 U/kg/h IV; aPTT checked in 6h and q6h after any dosage change, as well asqam; adjust dose according to followingparametersaPTT = <1.2 times control: 80 U/kg bolus withincrease of 4 U/kg/haPTT = 1.2-1.5 times control: 40 U/kg bolus withincrease of 2 U/kg/haPTT = 1.5-2.3 times control: No change ininfusion rate neededaPTT = 2.3-3 times control: Decrease infusionrate by 2 U/kg/haPTT >3 times control: Hold infusion for 1 h anddecrease rate by 3 U/kg/h
Pediatric DoseLoading dose: 50 U/kg IV; increase by 15-25U/kg/h to maintain aPTT at 1.5-2.5 times baseline
Contraindications
Documented hypersensitivity, aneurysm, active orrecent bleeding, coagulopathy, endocarditis,hemophilia, hepatic disease, hypertension,inflammatory bowel disease, lumbarpuncture/spinal anesthesia, sulfitehypersensitivity, surgery, thrombocytopenia
Interactions
Digoxin, nicotine, tetracycline, and antihistaminesmay decrease effects; NSAIDs, aspirin, dextran,dipyridamole, and hydroxychloroquine mayincrease toxicity
Pregnancy C - Safety for use during pregnancy has not been
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
310

established.
Precautions
Monitor platelet count for development ofthrombocytopenia; severe hyperkalemia mayoccur with concomitant use of ACE inhibitors;increased bleeding risk occurs with many drugs,including platelet inhibitors, NSAIDs, valproicacid, Ginkgo biloba, and probenecid
Drug Name
Warfarin (Coumadin)- Interferes with action ofvitamin K, a cofactor essential for convertingprecursor proteins into factors II, VII, IX, and X.Does not affect activity of coagulation factorssynthesized prior to exposure to warfarin.Depletion of these mature factors by normalmetabolism must occur before therapeutic effectsof newly synthesized factors can be seen, thusmay take several days to become effective.Dose influenced by differences in absorption,metabolism, and hemostatic responses to givenconcentrations; dose must be monitored closelyby following PT and INR. Higher initial doses donot appear to improve time required to achievetherapeutic levels but do increase bleeding risk.
Adult DoseInitial: 5 mg PO qd; adjust dose by monitoringINR (target, 2.5)
Pediatric DoseInitial: 0.2 mg/kg PO up to 10 mgMaintenance: 0.1 mg/kg/d; INR must bemonitored to determine maintenance dose
Contraindications
Documented hypersensitivity, alcoholism,aneurysm, bleeding, breastfeeding, endocarditis,pregnancy, hemophilia, lumbar puncture,thrombocytopenia, hypertension, leukemia,polycythemia vera, intracranial bleeding, vitaminC deficiency, vitamin K deficiency
Interactions
Monitor INR whenever a medication is added ordiscontinued; drugs that may decreaseanticoagulant effects include griseofulvin,carbamazepine, glutethimide, estrogens, nafcillin,phenytoin, rifampin, barbiturates, cholestyramine,colestipol, vitamin K, spironolactone, oralcontraceptives, and sucralfate; medications thatmay increase anticoagulant effects include oralantibiotics, phenylbutazone, salicylates,sulfonamides, chloral hydrate, clofibrate,
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
311

diazoxide, anabolic steroids, ketoconazole,ethacrynic acid, miconazole, nalidixic acid,sulfonylureas, allopurinol, chloramphenicol,cimetidine, disulfiram, metronidazole,phenylbutazone, phenytoin, propoxyphene,sulfonamides, gemfibrozil, acetaminophen, andsulindac; supplements such as ginger and Ginkgobiloba should be avoided; green leafy vegetableshave high levels of vitamin K, which maydecrease INR
Pregnancy X - Contraindicated in pregnancy
Precautions
May cause uncontrolled bleeding and should notbe used in conditions in which bleeding would bedifficult to control, leading to a more catastrophicoutcome; medications that inhibit platelet functionshould be avoided, including aspirin, NSAIDs,and valproic acid; patients with protein S or Cdeficiency may become transientlyhypercoagulable (anticoagulate patient withheparin and then convert to warfarin); do notswitch brands after achieving therapeuticresponse; caution in active tuberculosis ordiabetes; patients with protein C or S deficiencyare at risk of developing skin necrosis
Drug Category: Thrombolytics - These agents cause lysis of the clot. All studies concerningthe use of these agents in CVT involve either direct instillation into the sinus at the time ofsurgery or the use of microcatheters to reach the venous sinus.
Drug Name
Alteplase (Activase)- Biosynthetic form of humantissue plasminogen activator. Tissue plasminogenactivator exerts effect on fibrinolytic system toconvert plasminogen to plasmin. Plasmindegrades fibrin, fibrinogen, and procoagulantfactors V and VIII. Not given as IV infusion totreat CVT. Refer patient to facility with expertiseto perform venous sinus catheterization.
Adult Dose1 mg/cm infused via venous sinus catheterthroughout clot, then 1-2 mg/h
Pediatric Dose Not established
Contraindications
Documented hypersensitivity, aneurysm,arteriovenous malformation, bleeding,coagulopathy, endocarditis, diabetic retinopathy,mitral stenosis, recent surgery, pregnancy,
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
312

breastfeeding
Interactions
Drugs that alter platelet function (eg, aspirin,dipyridamole, abciximab) may increase risk ofbleeding prior to, during, or after alteplasetherapy; may give heparin with and after alteplaseinfusions to reduce risk of rethrombosis; eitherheparin or alteplase may cause bleedingcomplications
PregnancyC - Safety for use during pregnancy has not beenestablished.
Precautions
Monitor for bleeding, especially at arterialpuncture sites, with coadministration of vitamin Kantagonists; control and monitor BP frequentlyduring and following alteplase administration(when managing acute ischemic stroke); do notuse >0.9 mg/kg to manage acute ischemic stroke;doses >0.9 mg/kg may cause intracranialhemorrhage
Drug Name
Urokinase (Abbokinase)- Produced by kidney,converts plasminogen to plasmin by cleavingarginine-valine bond in plasminogen. Degradationproducts of fibrin and fibrinogen exert clinicallysignificant anticoagulant effect. Erythrocyteaggregation and plasma viscosity also are reportedto decrease.Given in CVT by catheterization of venous sinusor by direct instillation at surgery duringthrombectomy. Not currently available in US.
Adult Dose
250,000 U/h instilled directly or via venous sinuscatheter; additional doses of 50,000 U; total dose1,000,000 U over 2 hNot currently available in the US
Pediatric Dose Not established
Contraindications
Documented hypersensitivity, aneurysm,arteriovenous malformation, bleeding,coagulopathy, endocarditis, diabetic retinopathy,mitral stenosis, recent surgery, pregnancy,breastfeeding
InteractionsEffects increased with coadministration ofaminocaproic acid, anticoagulants, antineoplastic
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
313

agents, antithymocyte globulin, cefamandole,cefoperazone, Ginkgo biloba, NSAIDs, plateletinhibitors, porfimer, strontium-89 chloride,sulfinpyrazone, tranexamic acid, valproic acid
PregnancyB - Usually safe but benefits must outweigh therisks.
Precautions
Caution in patients receiving IM administration ofmedications or with severe hypertension or traumaor surgery in previous 10 d; do not measure BP inlower extremities, because may dislodge DVT;monitor therapy by performing PT, aPTT, TT, orfibrinogen approximately 4 h after initiation oftherapy
Drug Name
Streptokinase (Kabikinase, Streptase)- Facilitatesthrombolysis through formation of an activatorcomplex with plasminogen. Indirectly cleavesarginine-valine bond in plasminogen, formingplasmin. Plasmin degrades fibrin, fibrinogen, andprocoagulant factors V and VIII. Degradationproducts of fibrin and fibrinogen have significantanticoagulant effect.
Adult Dose Instilled directly or via venous sinus catheter
Pediatric Dose
Only anecdotal reports describe use in children,and that in arterial occlusion; doses used were asfollowsLoading dose: 1000-3000 IU/kg; followed byinfusion of 1000-1500 IU/kg/h; in CVT,administered by direct infusion via catheter
Contraindications
Documented hypersensitivity, aneurysm,arteriovenous malformation, bleeding,coagulopathy, endocarditis, diabetic retinopathy,mitral stenosis, recent surgery, pregnancy,breastfeeding
Interactions
Effects are increased with coadministration ofaminocaproic acid, anticoagulants, antineoplasticagents, antithymocyte globulin, cefamandole,cefoperazone, Ginkgo biloba, NSAIDs, plateletinhibitors, porfimer, strontium-89 chloride,sulfinpyrazone, tranexamic acid, valproic acid
PregnancyC - Safety for use during pregnancy has not beenestablished.
PrecautionsCaution in severe hypertension, IM administrationof medications, trauma or surgery in previous 10
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
314

d; measure hematocrit, platelet count, aPTT, TT,PT, or fibrinogen levels before therapy isimplemented; either TT or aPTT should be <2times the normal control value following infusionof streptokinase and before (re)instituting heparin;do not take BP in lower extremities, as possibleDVT may be dislodged; PT, aPTT, TT, orfibrinogen should be monitored 4 h after initiationof therapy; in addition to bleeding complicationsinherent in thrombolytic agents, repeatedadministration of streptokinase can result intolerance as well as hypersensitivity
References
1. A'Alise, MD: Sagittal sinus thrombosis following minor head injury treated withcontinuous urokinase infusion. Surgical Neurology 1998; 49(4): 430-435.
2. Adams WM, Laitt RD, Beards SC: Use of single-slice thick slab phase-contrastangiography for the diagnosis of dural venous sinus thrombosis. Eur Radiol 1999;9(8): 1614-9.
3. Ameri A, Bousser MG: Cerebral venous thrombosis. Neurol Clin 1992 Feb; 10(1):87-111.
4. Ayanzen RH, Bird CR, Keller PJ: Cerebral MR Venography: Normal Anatomy andPotential Diagnostic Pitfalls. Am J Neuroradiol 2000; 21: 74-78.
5. Benamer HTS, I Bone: Cerebral venous thrombosis: anticoagulants or thrombolytictherapy? J Neurol Neurosurg Psychiatry 2000; 69: 427-430.
6. Cipri S: High-dose heparin plus warfarin in non-traumatic dural sinus thrombosis.A clinical and neuroradiological study. J Neurosurg Sc 1998; 42(1): 23-32.
7. Daif A, Awanda A, al-Rajeh S: Cerebral Venous Thrombosis in Adults. A Study ofForty Cases from Saudi Arabia. Stroke 1995; 26(7): 1193-1195.
8. Davis, KR, Kistler, JP, Buonanno, FS: Clinical Neuroimaging Approaches toCerebrovascular diseases. Neurologic Clinics 1984; 2(4): 635-665.
9. de Bruijin, SF: Increased risk of cerebral venous sinus thrombosis with third-generation oral contraceptives. Lancet 1998; 351(9113): 1404.
10. Einhaupl KM, Villringer A, Meister W: Heparin Treatment in Sinus VenousThrombosis. Lancet 1991; 338(8772): 958.
11. Ekseth K, Bostrom S, Vegfors M: Reversibility of severe sagittal sinus thrombosiswith open surgical thrombectomy combined with local infusion of tissueplasminogen activator: technical case report. Neurosurg 1998 Oct; 43(4): 960-5.
12. Gold Standard Multimedia: Urokinase, Altevase, Streptokinase, Heparin, Warfarin.Clinical Pharmacology 2000;.
13. Gomez CR, Misra VK, Terry JB: Emergency endovascular treatment of cerebralsinus thrombosis with a rheolytic catheter device. J Neuroimaging 2000 Jul; 10(3):177-80.
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
315

14. Jacobs K, Moulin T, Bogouslavsky MD: The Stroke Syndrome of Cerebral VeinThrombosis. Neurology 1996; 47(2): 376-382.
15. Meyer-Lindenberg A: Fatal Cerebral Venous Sinus Thrombosis in Heparin InducedThrombotic Thrombocytopenia. European Neurology 1997; 37(3): 191-192.
16. Smith, A. Gordon, Cornblath, Wayne T., Devekis, John P.: Local ThrombolyticTherapy in Deep Cerebral Venous Thrombosis. Neurology 1997; 48(6): 1613-1619.
17. Towbin A: The syndrome of latent cerebral venous thrombosis: its frequency andrelation to age and congestive heart failure. Stroke 1973 May-Jun; 4(3): 419-30.
18. Bousser MG, Chiras J, Bories J, et al: Cerebral venous thrombosis-a review of 38cases. Stroke 16:199-213, 1985
19. Buonanno FS, Moody DM, Ball MR, et al: Computed cranial tomographic findingsin cerebral sinovenous occlussion. J Comput Assist Tomogr 2:281-290, 1978
20. Chakeres DW, Schmalbrock P, Brogan M, et al: Normal venous anatomy of thebrain: Demonstration with gadopentetate dimeglumine in enhanced 3-D MRangiography. AJNR Am j Neuroradiol 11:1 107-1118,1990
21. Dermont D, Sag K, Biondi A, et al: Gadolinium-enhanced MR of chronic duralsinus thrombosis. AJNR Am j Neuroradiol 16:1347-1352, 1995
22. Hart RG, Easton JD: Dissections of cervical and cerebral arteries. Neurol ClinNorth Am 1:255-262, 1983
23. Lensee C, Reul J, Thron A:.Magnetic resonance imaging of thrombosed duralsinuses. Stroke 25:29-34, 1994
24. Provenzale J, Joseph G, Barboriak D: Dural sinus thrombosis: Findings on CT andMR imaging and diagnostic pitfalls. AJR Am J Roentgenol 170:777-783, 1998
25. Roncallo F, Turtulici L Bisio A, et al: Cerebral venous thrombosis: Prognostic andtherapeutic significance of an early radiologic diagnosis. Neuroradiol 11:479- 505,1988
26. Schievink WI, Mokeri B, Piepgras DG: Spontaneous dissections of cervicocephahcarteries in childhood and adolescence. Neurology 44:1607-1612, 1994
27. Sze G, Simmons B, Krol G, et al: Dural sinus thrombosis: Verification with spin-echo techniques. AJNR Am j Neuroradiol 9:679-686,1988
28. Virapongse C, Cazenave C, Quisling R, et al: The empty delta sign: Frequency andsignificance in 76 cases of dural sinus thrombosis. Radiology 162:779- 785,1987
29. Zimmerman R, Ernst R: Neuroimaging of cerebral venous thrombosis.Neuroimaging Chn North Am 2: 463-485,1992
30. Fong Y. Tsai, Ay-Ming Wang, Violet B. Matovich, Mark Lavin, Bruce Berberian,Tereasa M, at al: MR Staging of Acute Dural Sinus Thrombosis: Correlation withVenous Pressure Measurements and Implications for Treatment and Prognosis. AmJ Neuroradiol 16:1021–1029, May 1995
Professor Yasser Metwallywww.yassermetwally.com
www.yassermetwally.com
316