Embed Size (px)
Citation preview
Image interpretation: spine
Dr David LisleBrisbane Private Imaging
Image interpretation
• Anatomy• Cross sectional techniques:
– CT– MRI
• Nomenclature of disc herniations and spinal stenosis
• A few cases

Image interpretation
• Anatomy• Cross sectional techniques:
– CT– MRI
• Nomenclature of disc herniations and spinal stenosis
• A few cases
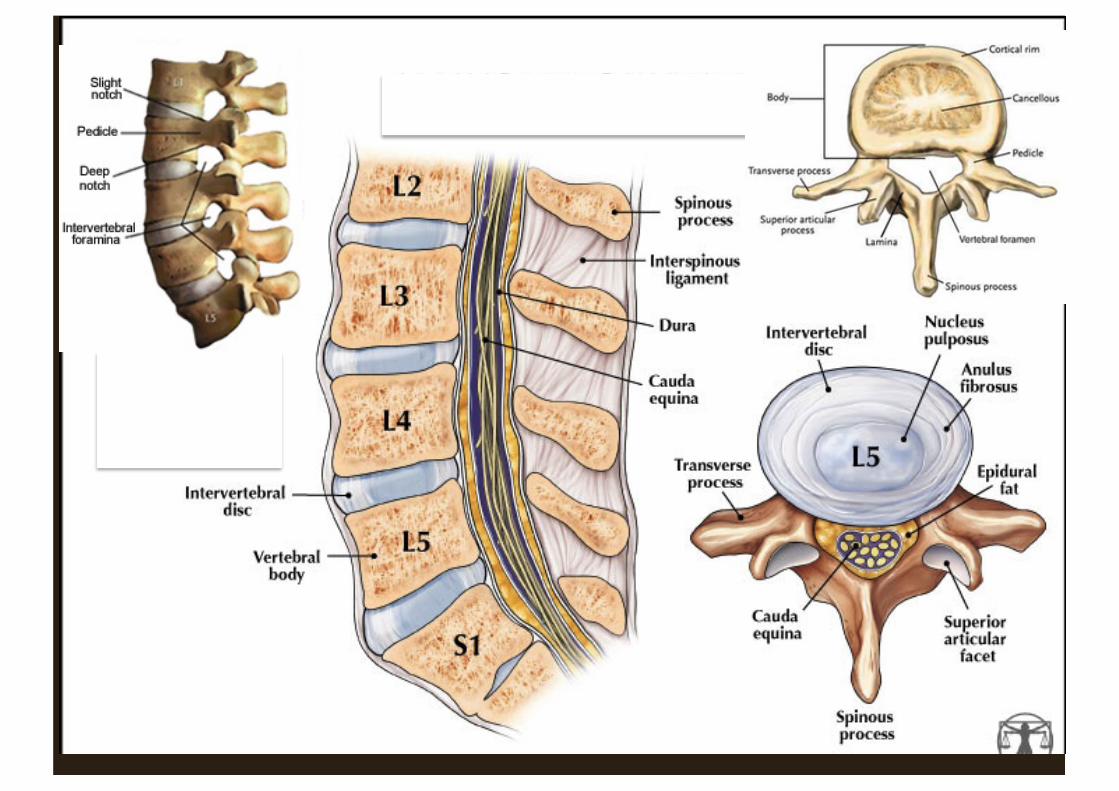
Image interpretation
• Anatomy• Cross sectional techniques:
– CT– MRI
• Nomenclature of disc herniations and spinal stenosis
• A few cases
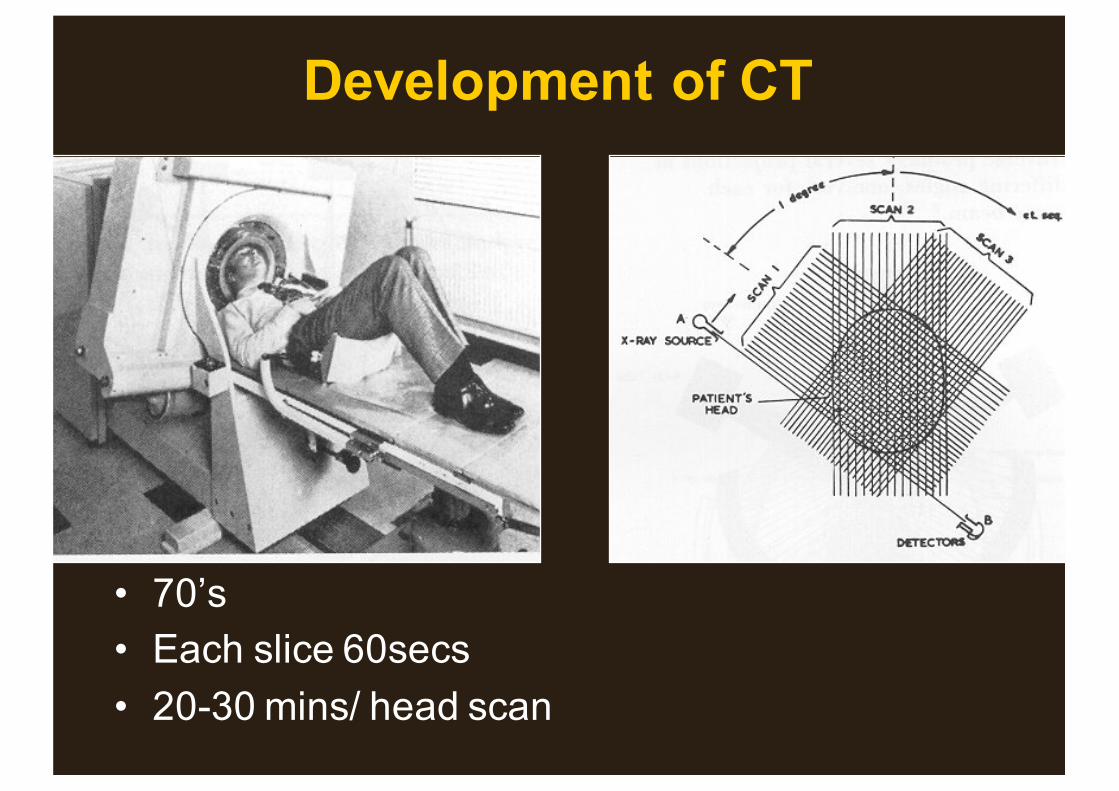
Development of CT
• 70’s• Each slice 60secs• 20-30 mins/ head scan
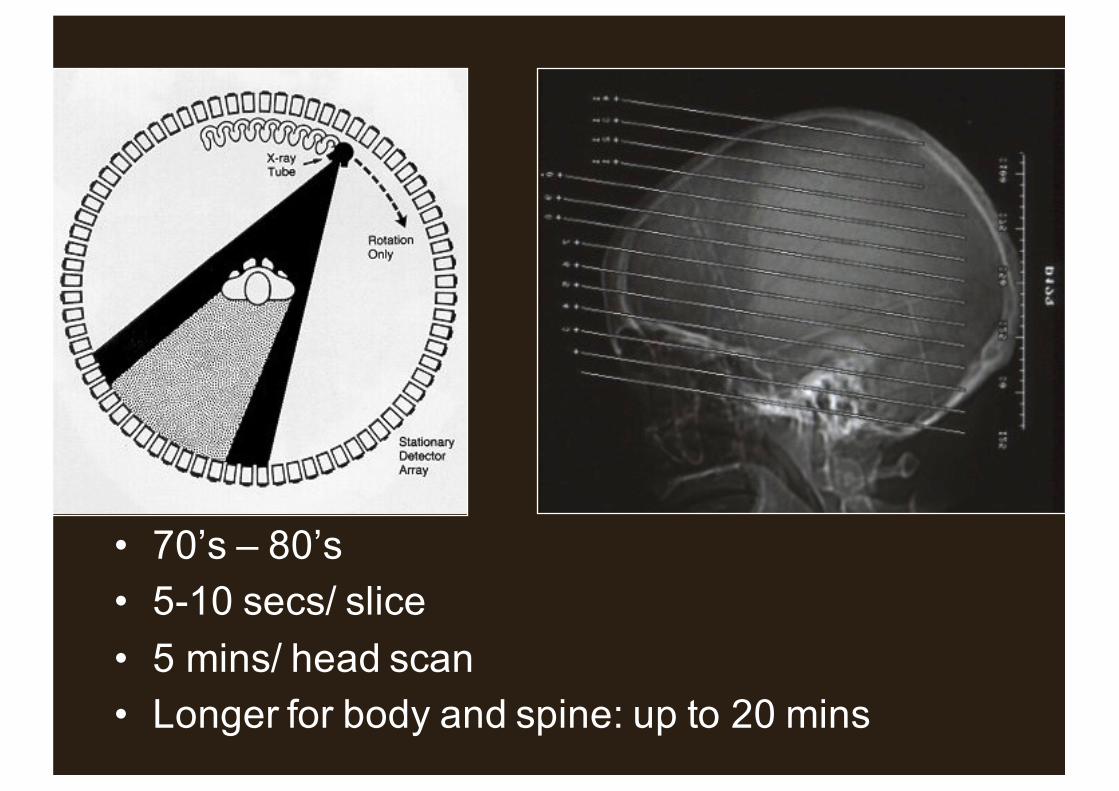
• 70’s – 80’s• 5-10 secs/ slice• 5 mins/ head scan• Longer for body and spine: up to 20 mins

1974 1988
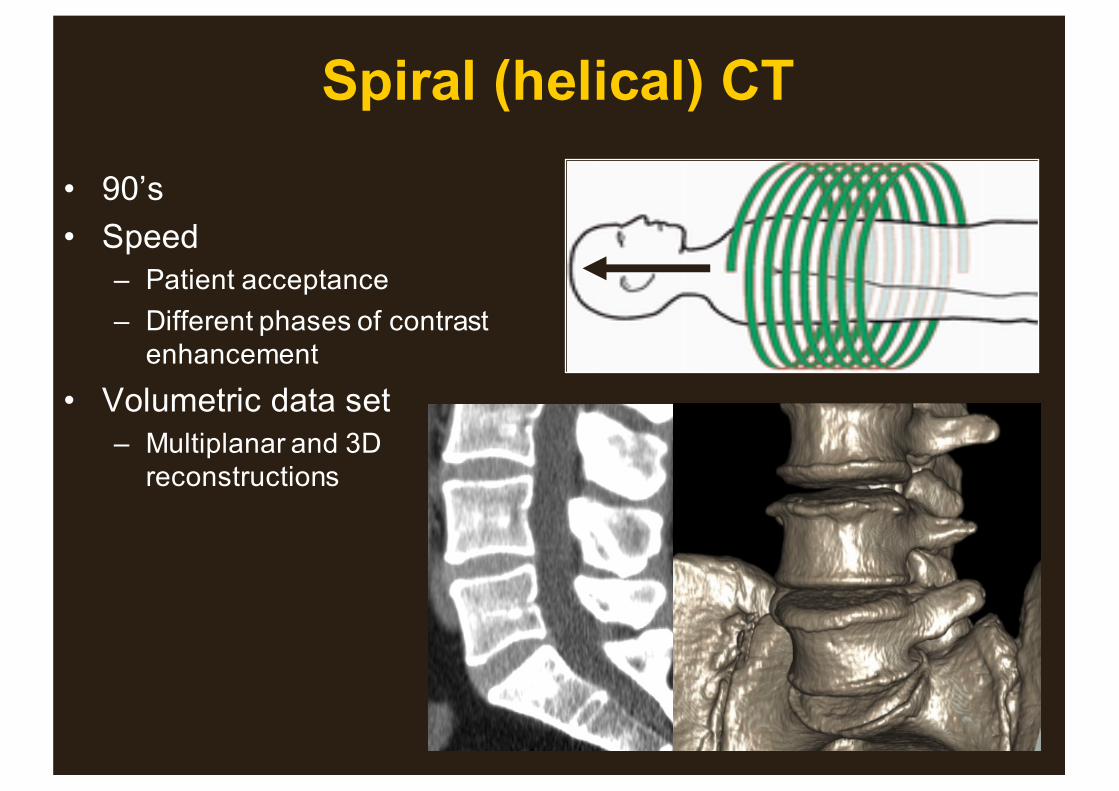
Spiral (helical) CT
• 90’s• Speed
– Patient acceptance– Different phases of contrast
enhancement
• Volumetric data set– Multiplanar and 3D
reconstructions

Multidetector (multislice) CT
• Late 90’s to present• 0.175 - few seconds scan
time• Overlapping =
reconstructions• Contiguous = speed• Original: 4 slice• 2nd generation: 16, 64• New: 256; 320
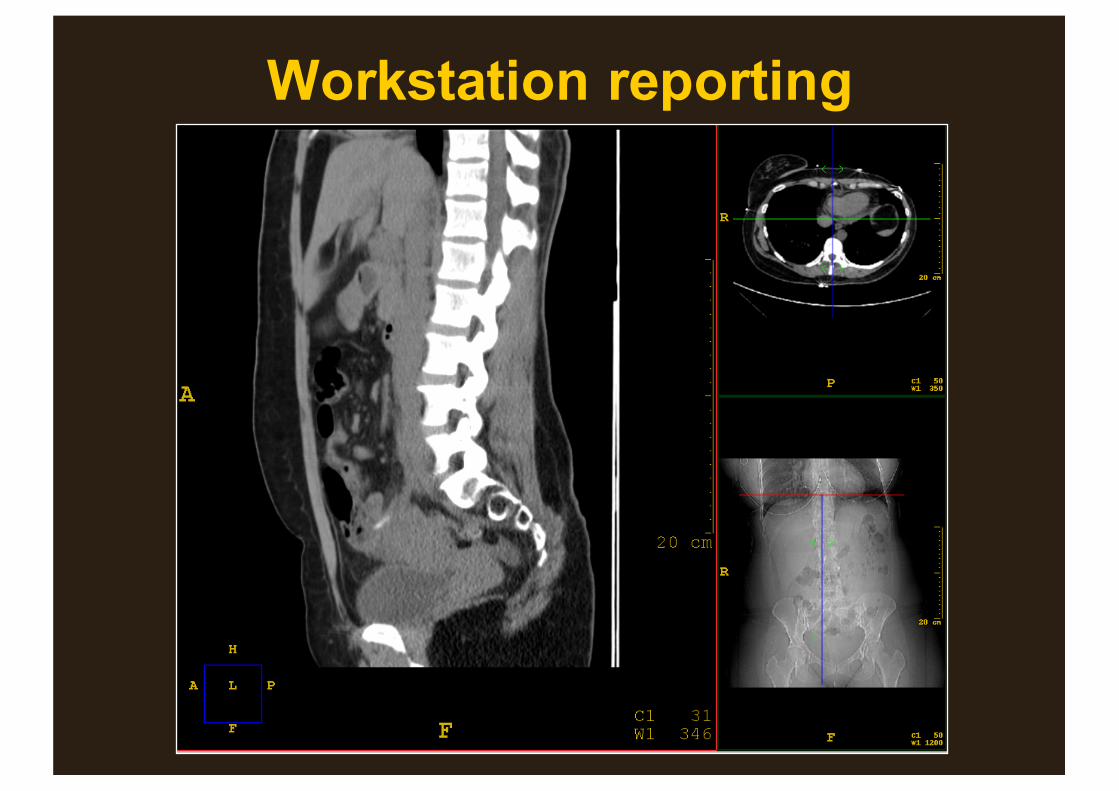
Workstation reporting




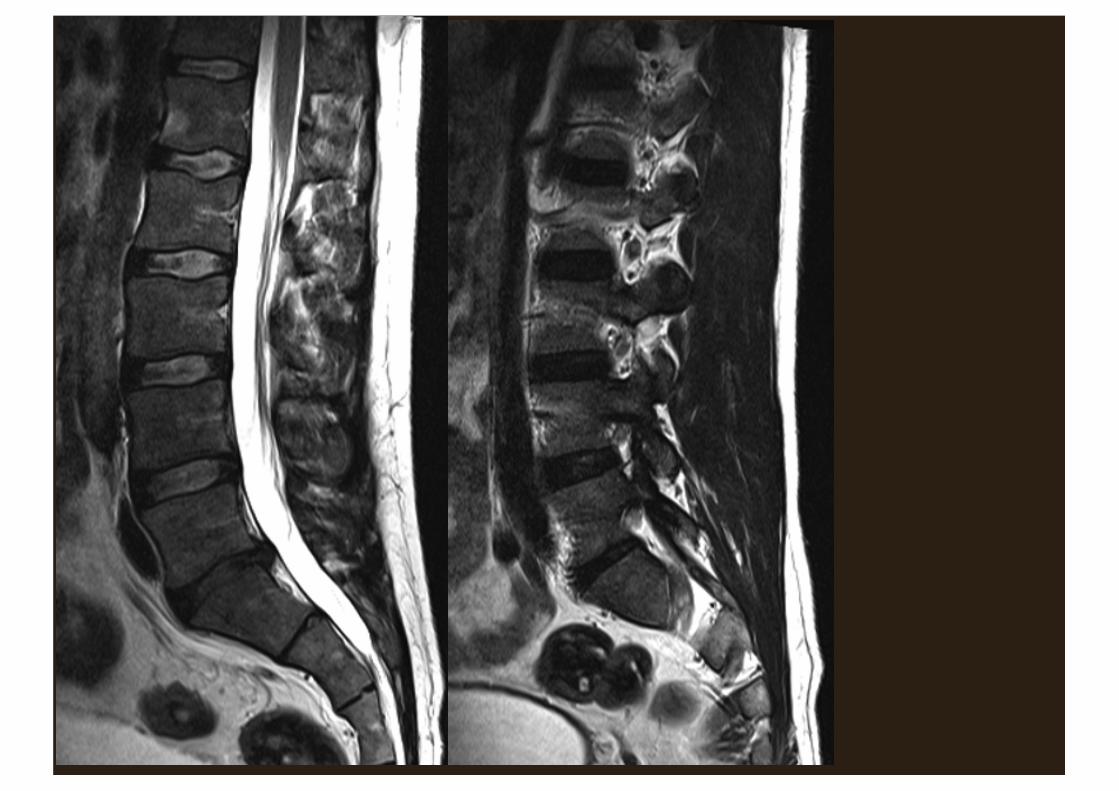
MRI: T1
– Fat bright• Bone marrow
– Bone cortex black– Anatomy

MRI: T2
– Bone cortex black– Anatomy– Fluid bright– Fat bright
• Bone marrow– Oedema bright
• Difficult to differentiate
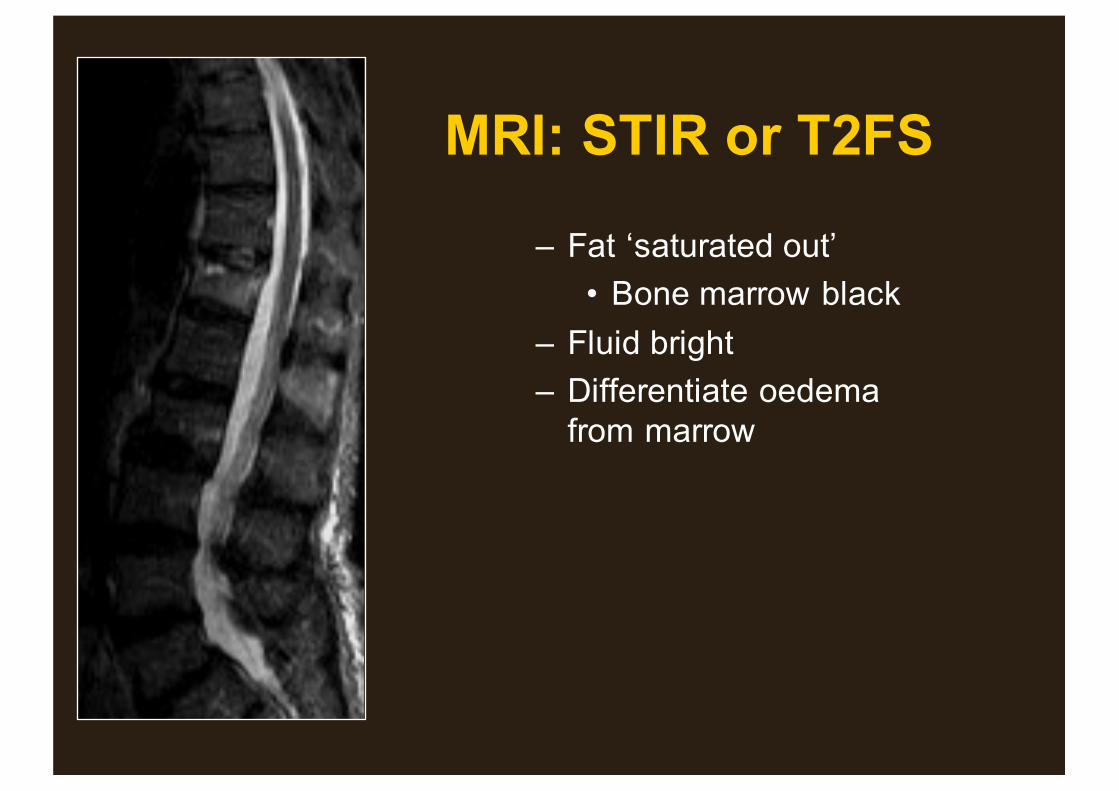
MRI: STIR or T2FS
– Fat ‘saturated out’• Bone marrow black
– Fluid bright– Differentiate oedema
from marrow

T1 T2 STIR
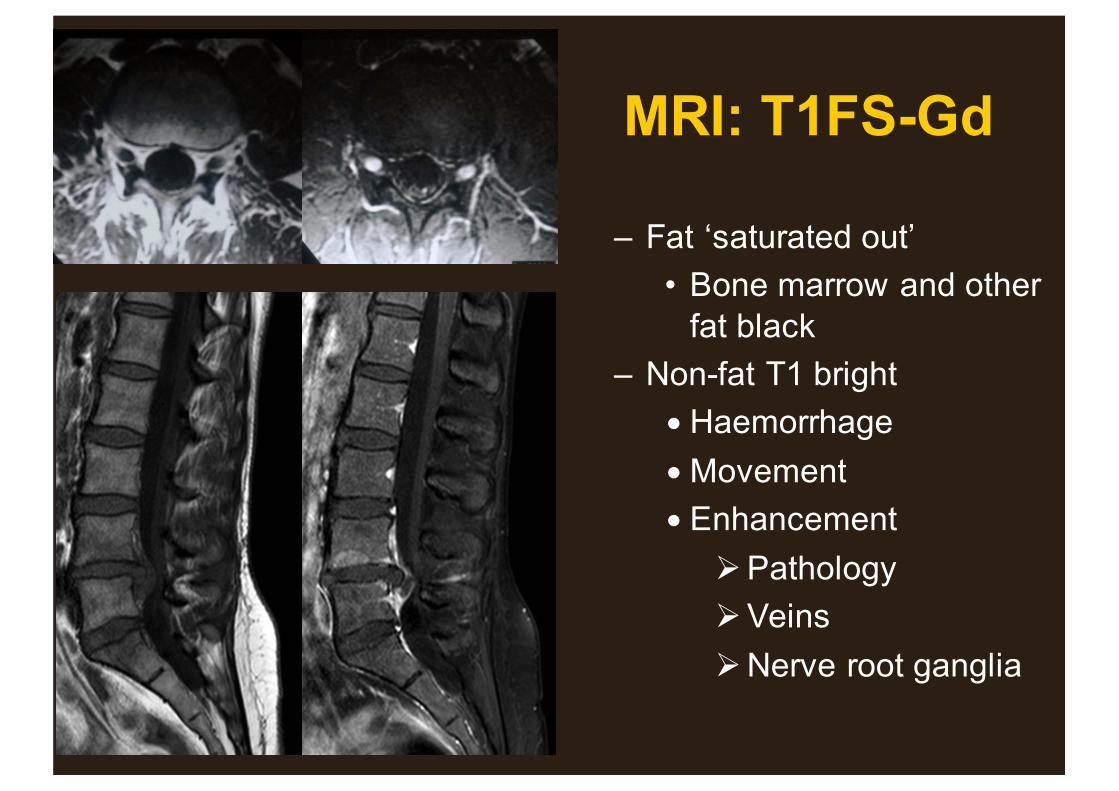
MRI: T1FS-Gd
– Fat ‘saturated out’• Bone marrow and other
fat black– Non-fat T1 bright
•Haemorrhage•Movement•Enhancement
ØPathologyØVeinsØNerve root ganglia
T1

T1
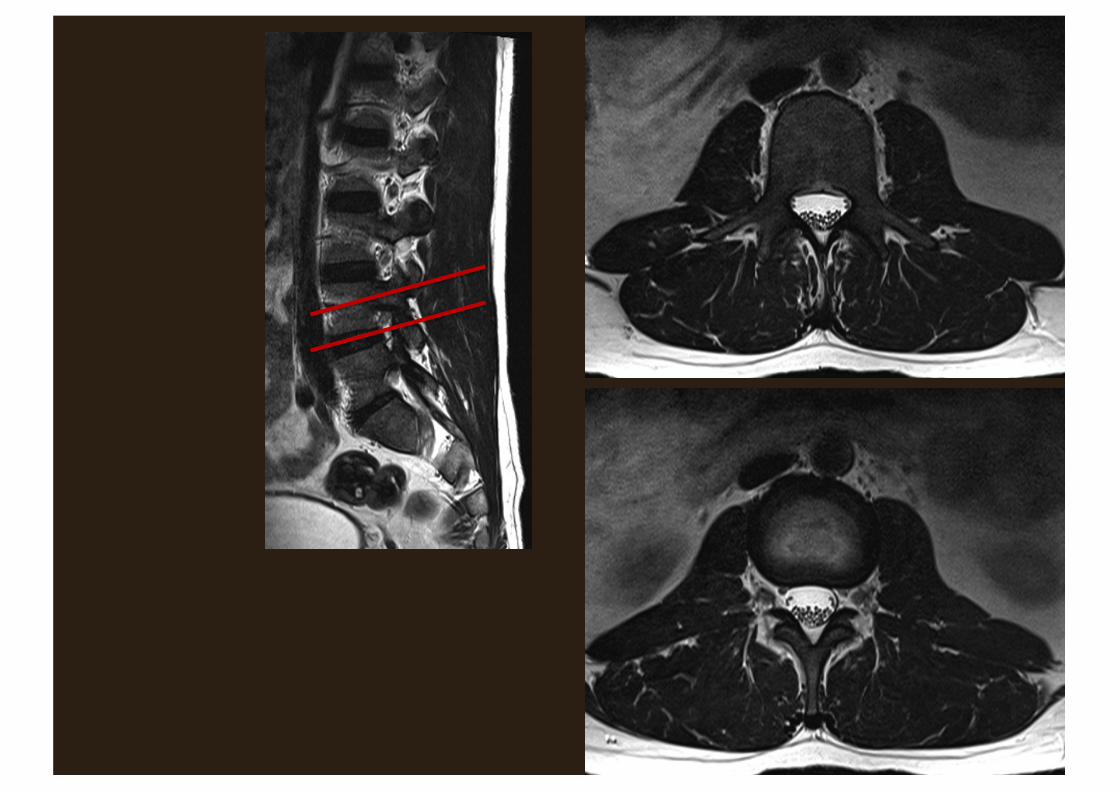

Image interpretation
• Anatomy• Cross sectional techniques:
– CT– MRI
• Nomenclature of disc herniations and spinal stenosis
• A few cases

NOMENCLATURE
• Consistent• Reflect common usage where appropriate• Surgically relevant• ‘Able to visualize over the phone’• 2 morphological characteristics:
– Nature of disc pathology– Location
• Able to add further descriptors– Neural structures– Clinical context
• www.asnr.org/spine_nomenclature/reporting
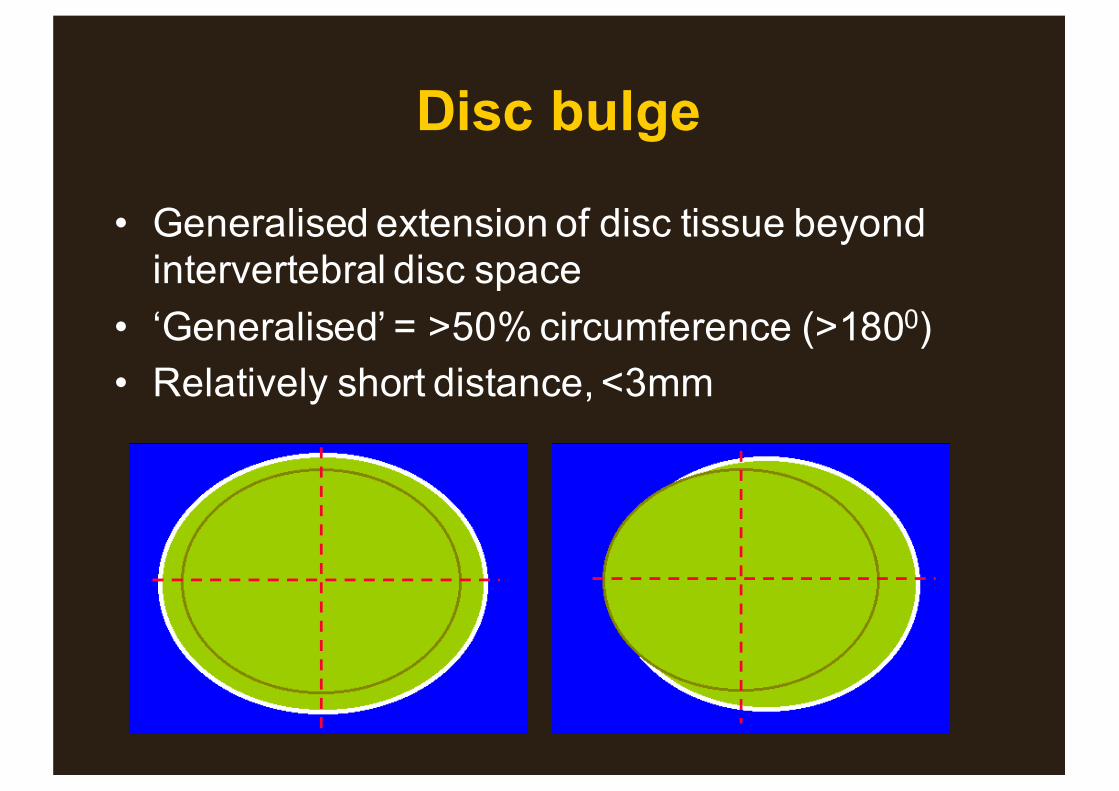
Disc bulge
• Generalised extension of disc tissue beyond intervertebral disc space
• ‘Generalised’ = >50% circumference (>1800)• Relatively short distance, <3mm

Herniated disc• Localised displacement of disc material beyond
intervertebral disc space (ie bony margins excluding osteophytes) OR break in vertebral end plate (Schmorl’s node)
• ‘Localised’ = <50% circumference (<1800)– ‘Broad based’ = 25 - 50% circumference (>900)– ‘Focal’ = <25% circumference (<900)
• ‘HNP’ not accurate– Herniation may include NP, cartilage, annulus, bone
• ‘Rupture’ tends to refer to trauma/ acute event• ‘Prolapse’ and ‘bulging disc’ outdated• ‘Localised disc bulge’ = oxymoron

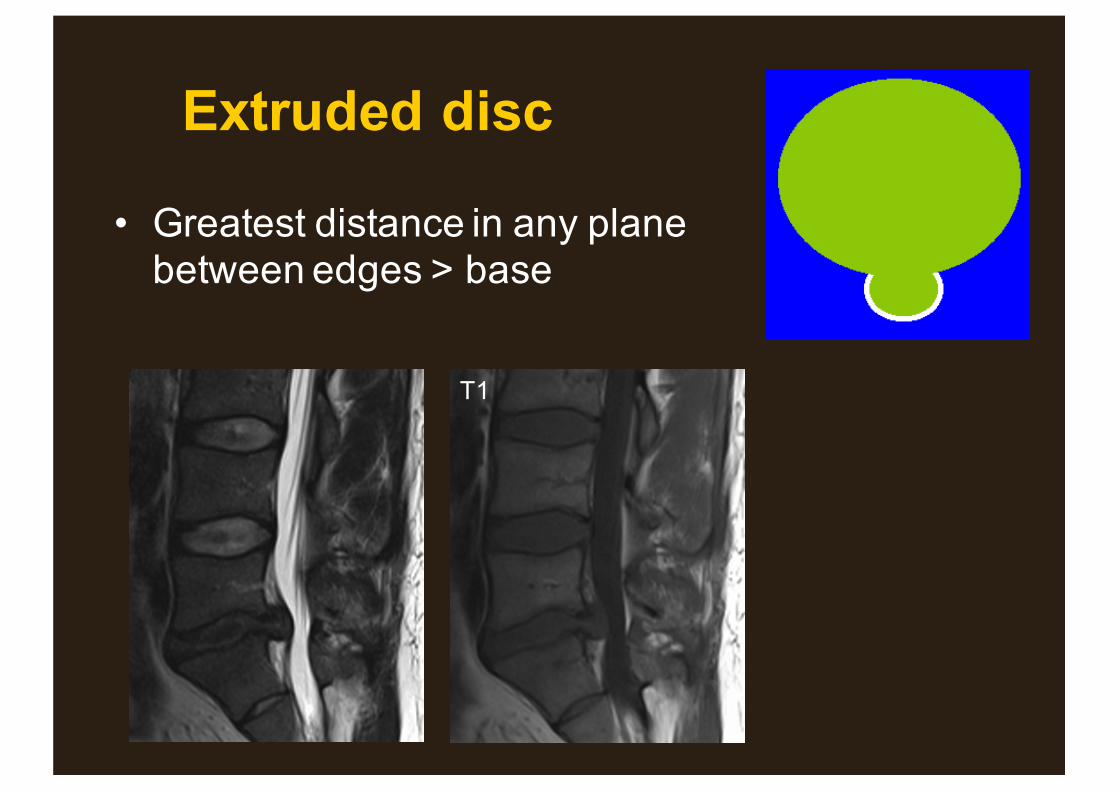
Extruded disc
• Greatest distance in any plane between edges > base
T1

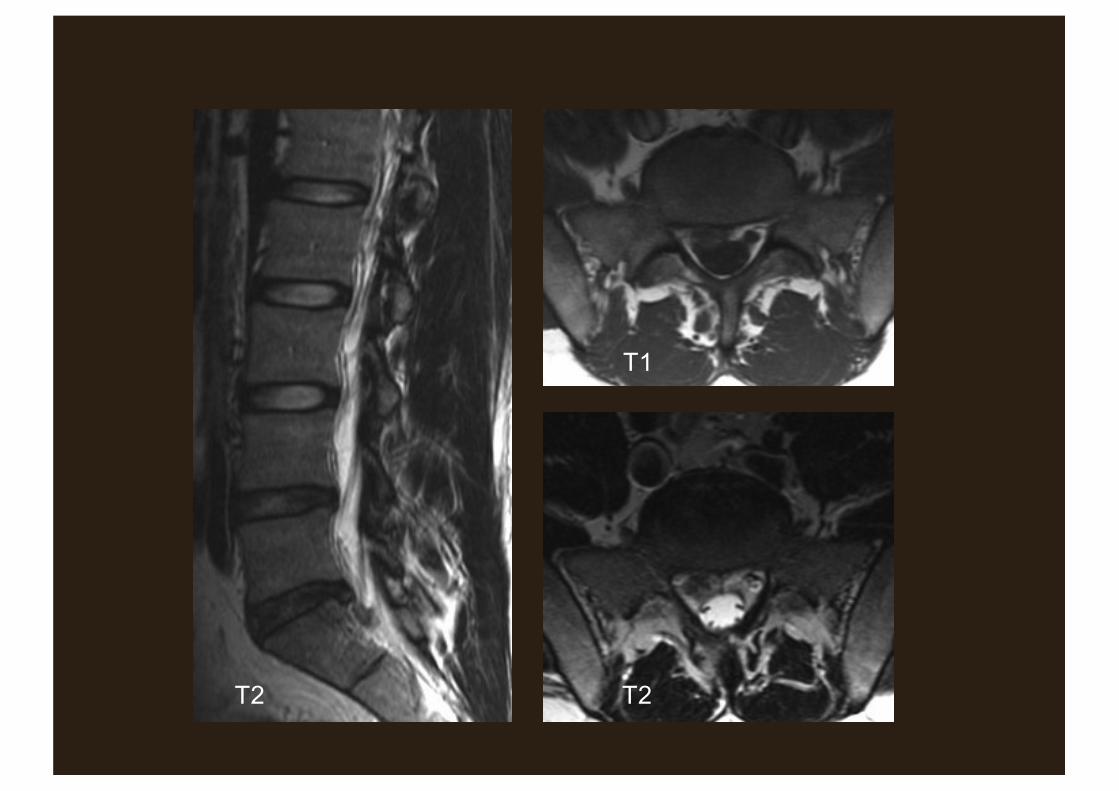
Sequestered disc
• Extruded disc material that has no continuity with the disc of origin
• = free fragment• Migrated disc:
– Disc material displaced away from site of extrusion
T2 T2
T1
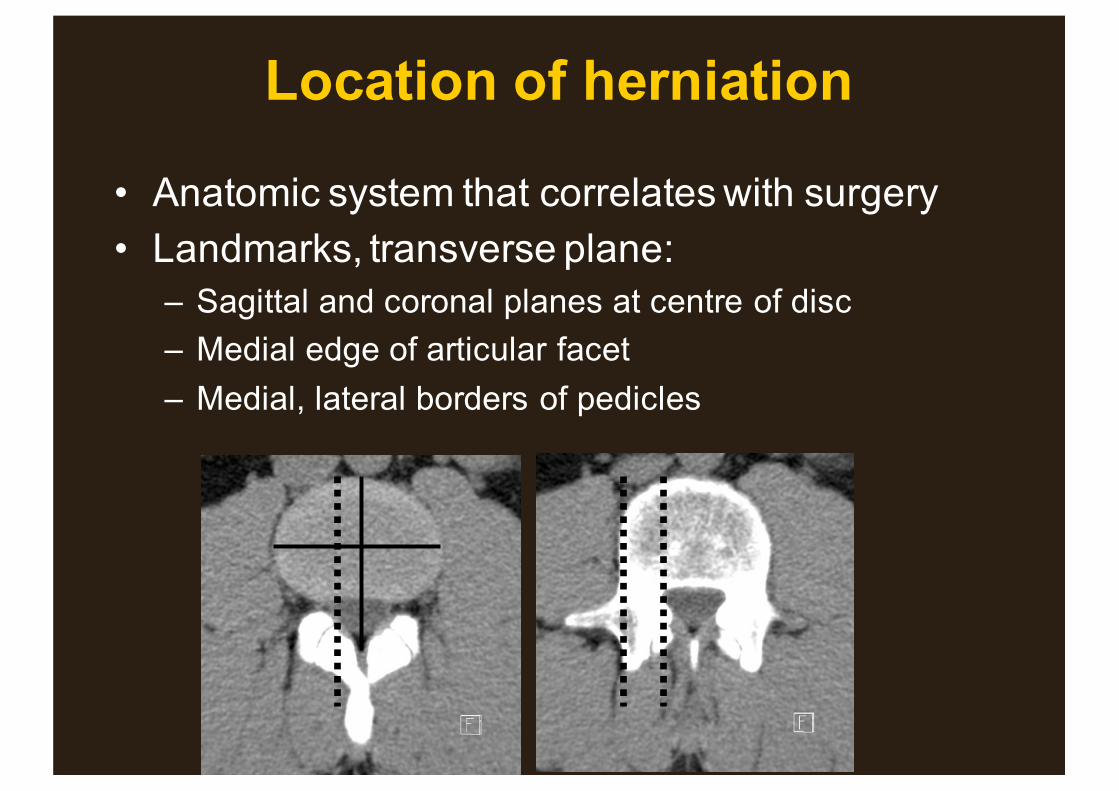
Location of herniation
• Anatomic system that correlates with surgery• Landmarks, transverse plane:
– Sagittal and coronal planes at centre of disc – Medial edge of articular facet– Medial, lateral borders of pedicles

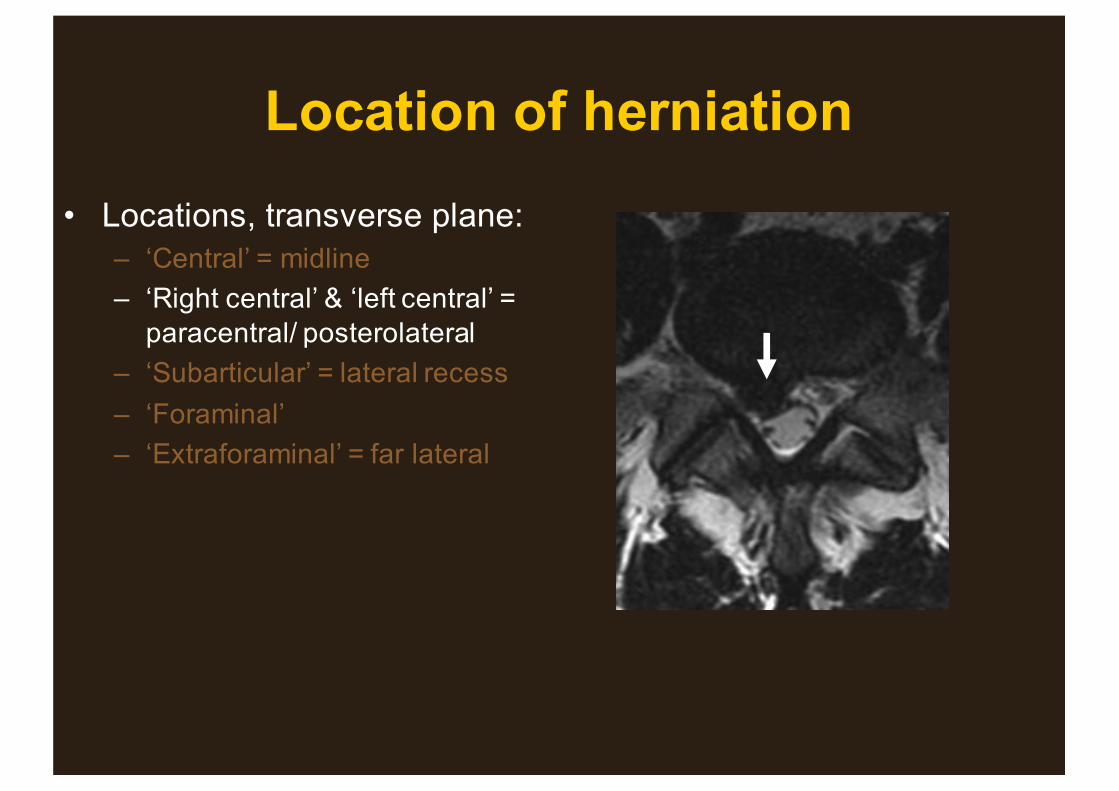
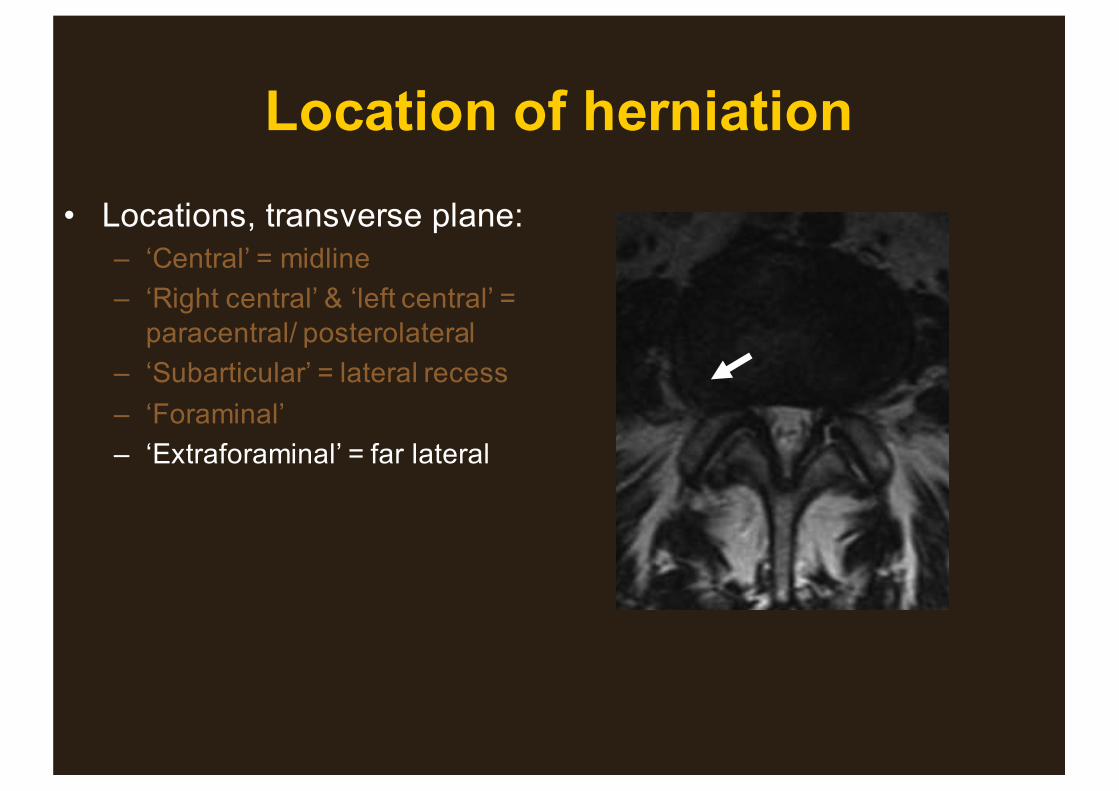
Location of herniation• Locations, transverse plane:
– ‘Central’ = midline– ‘Right central’ & ‘left central’ =
paracentral/ posterolateral– ‘Subarticular’ = lateral recess– ‘Foraminal’– ‘Extraforaminal’ = far lateral
Location of herniation• Locations, transverse plane:
– ‘Central’ = midline– ‘Right central’ & ‘left central’ =
paracentral/ posterolateral– ‘Subarticular’ = lateral recess– ‘Foraminal’– ‘Extraforaminal’ = far lateral

Location of herniation• Locations, transverse plane:
– ‘Central’ = midline– ‘Right central’ & ‘left central’ =
paracentral/ posterolateral– ‘Subarticular’ = lateral recess– ‘Foraminal’– ‘Extraforaminal’ = far lateral

Location of herniation• Locations, transverse plane:
– ‘Central’ = midline– ‘Right central’ & ‘left central’ =
paracentral/ posterolateral– ‘Subarticular’ = lateral recess– ‘Foraminal’– ‘Extraforaminal’ = far lateral
Location of herniation• Locations, transverse plane:
– ‘Central’ = midline– ‘Right central’ & ‘left central’ =
paracentral/ posterolateral– ‘Subarticular’ = lateral recess– ‘Foraminal’– ‘Extraforaminal’ = far lateral
Volume: degree of canal compromise
• X-sectional area at site of maximal narrowing• ‘Mild’: <1/3• ‘Moderate’: 1/3 – 2/3• ‘Severe’: > 2/3• Same grading for foraminal narrowing as seen in
sagittal plane• Other descriptors such as compression of
specific neural structures
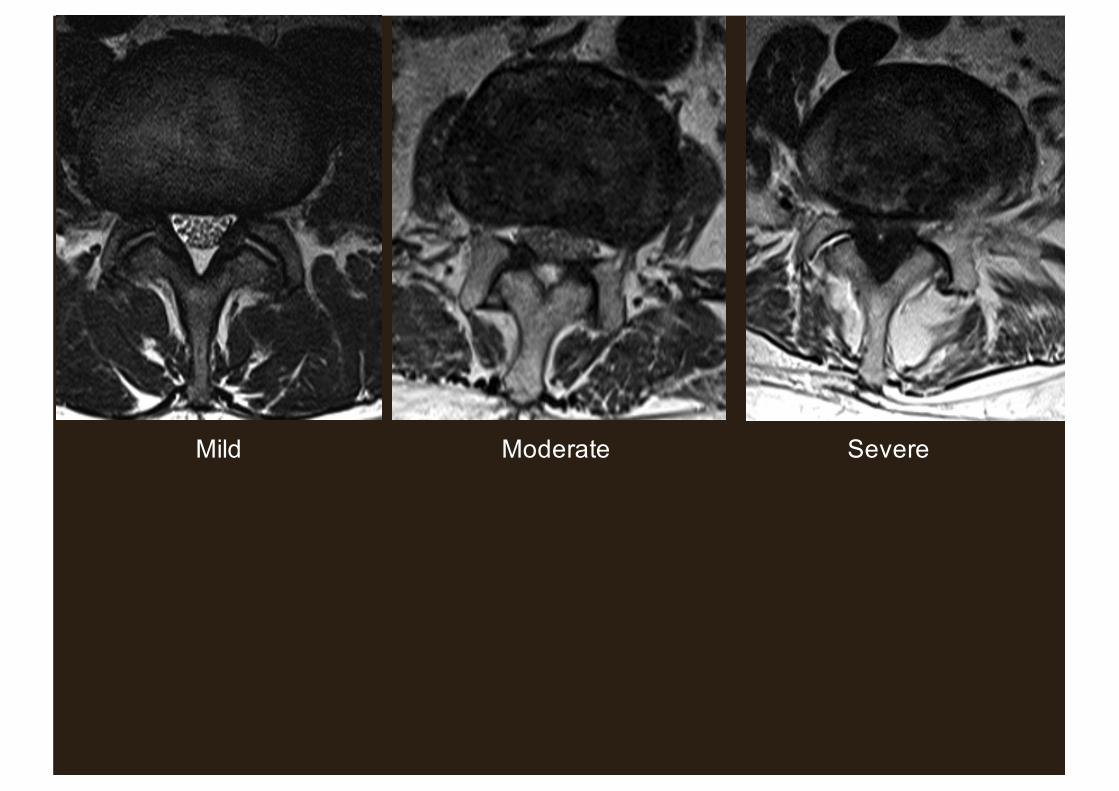
Mild Moderate Severe
Image interpretation
• Anatomy• Cross sectional techniques:
– CT– MRI
• Nomenclature of disc herniations and spinal stenosis
• A few cases

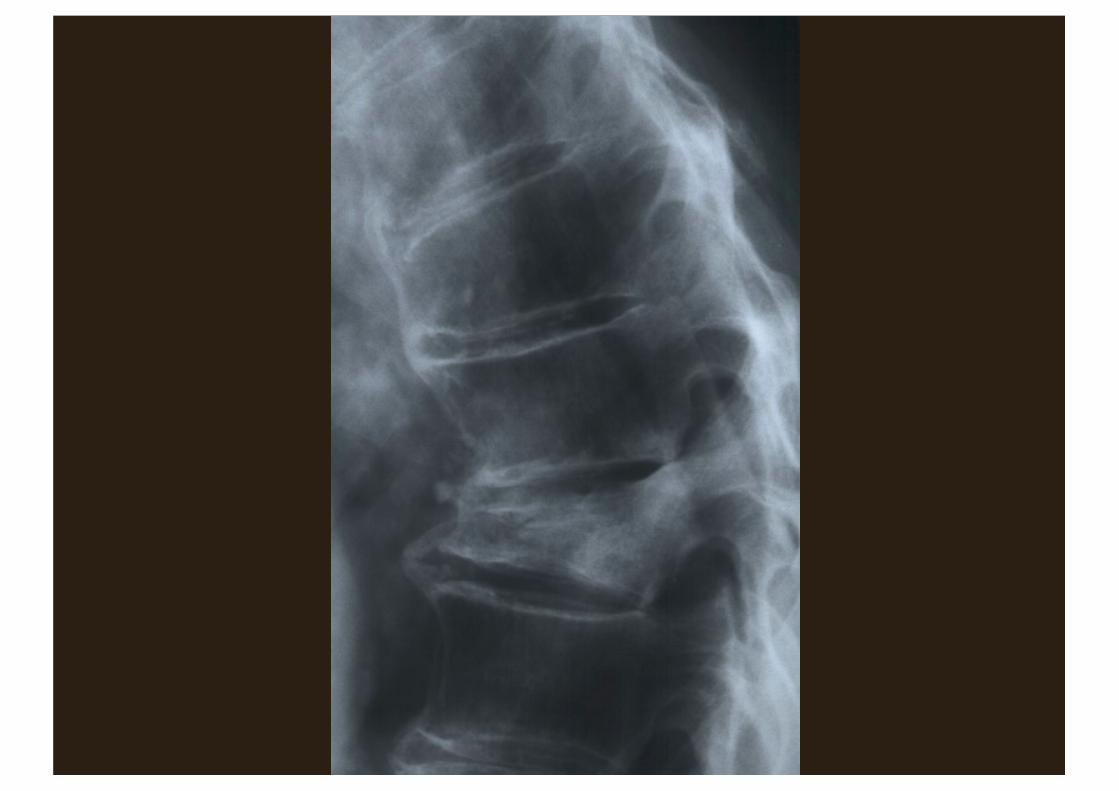
• 85 year old female• Severe acute on chronic mechanical back pain
– Can’t sleep– Limited walking to only a few steps
• Spontaneous onset• No known trauma
What is the most likely diagnosis?
1. Acute disc herniation2. Facet joint degeneration3. Crush fracture secondary to osteoporosis4. Metastatic cancer
What is the most appropriate imaging modality?
1. Plain film2. CT3. Scintigraphy (bone scan) 4. MRI
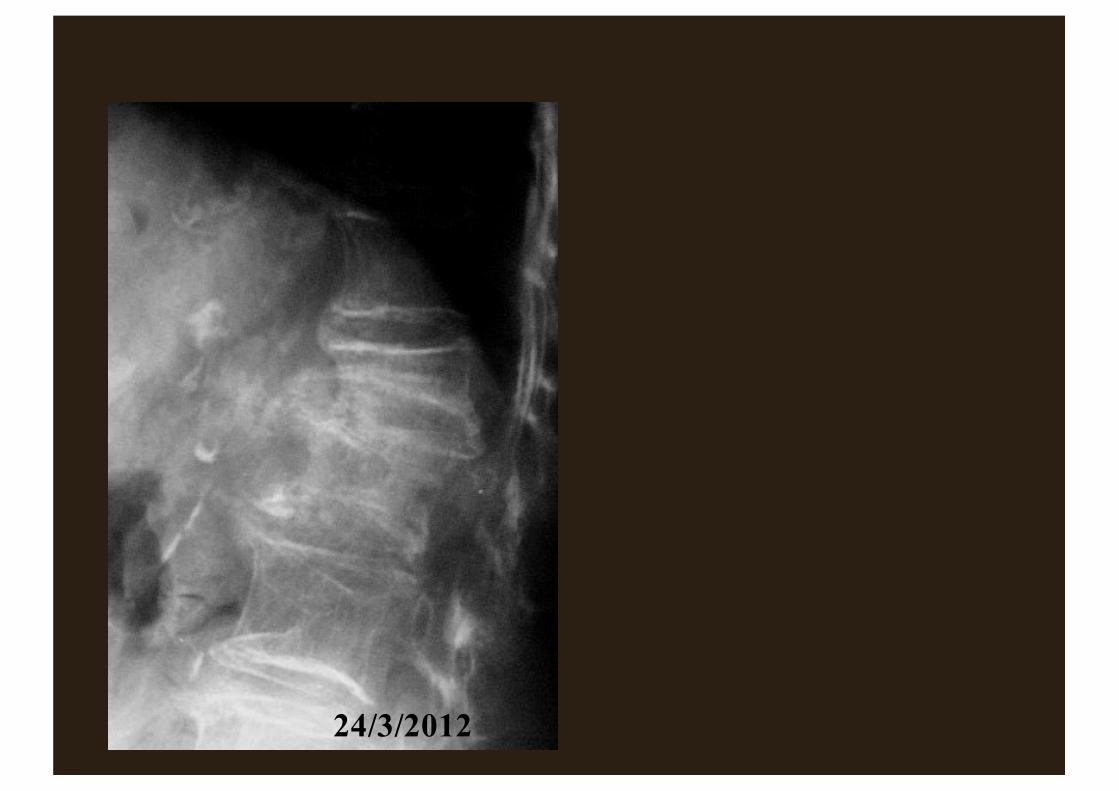
24/3/2012

24/3/2012 16/12/2011
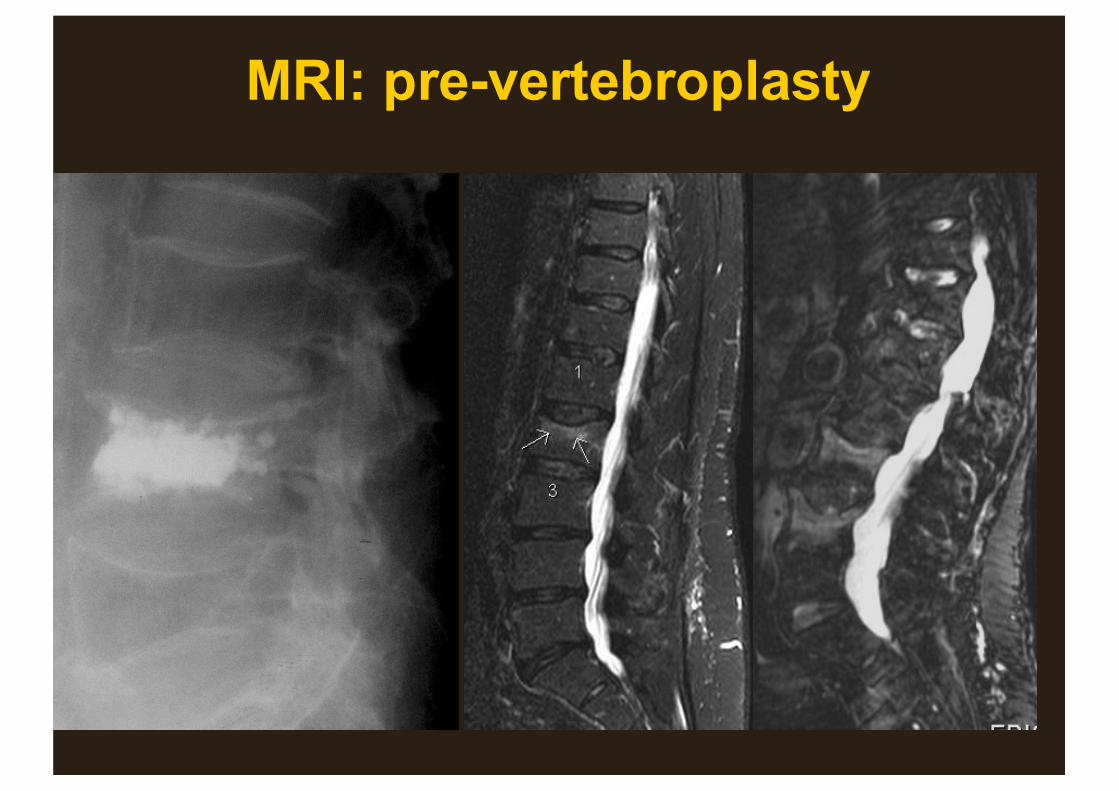
MRI: pre-vertebroplasty
STIR
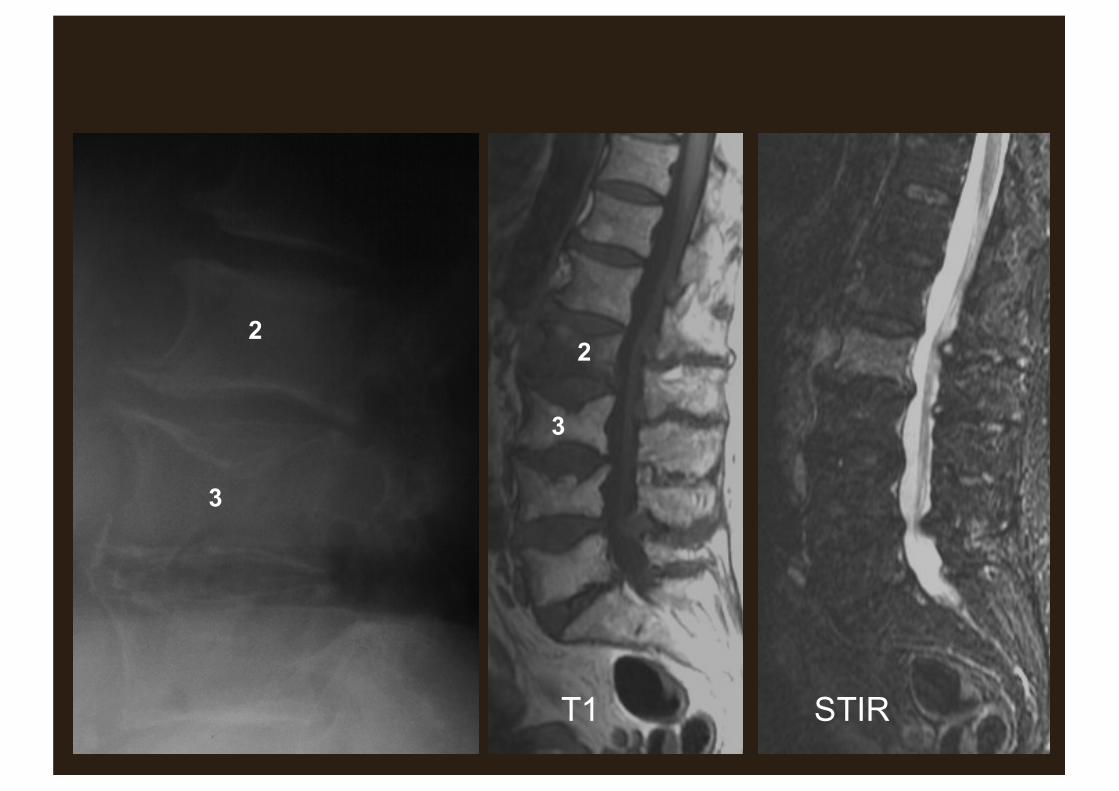
2
3
2
3
T1 STIR

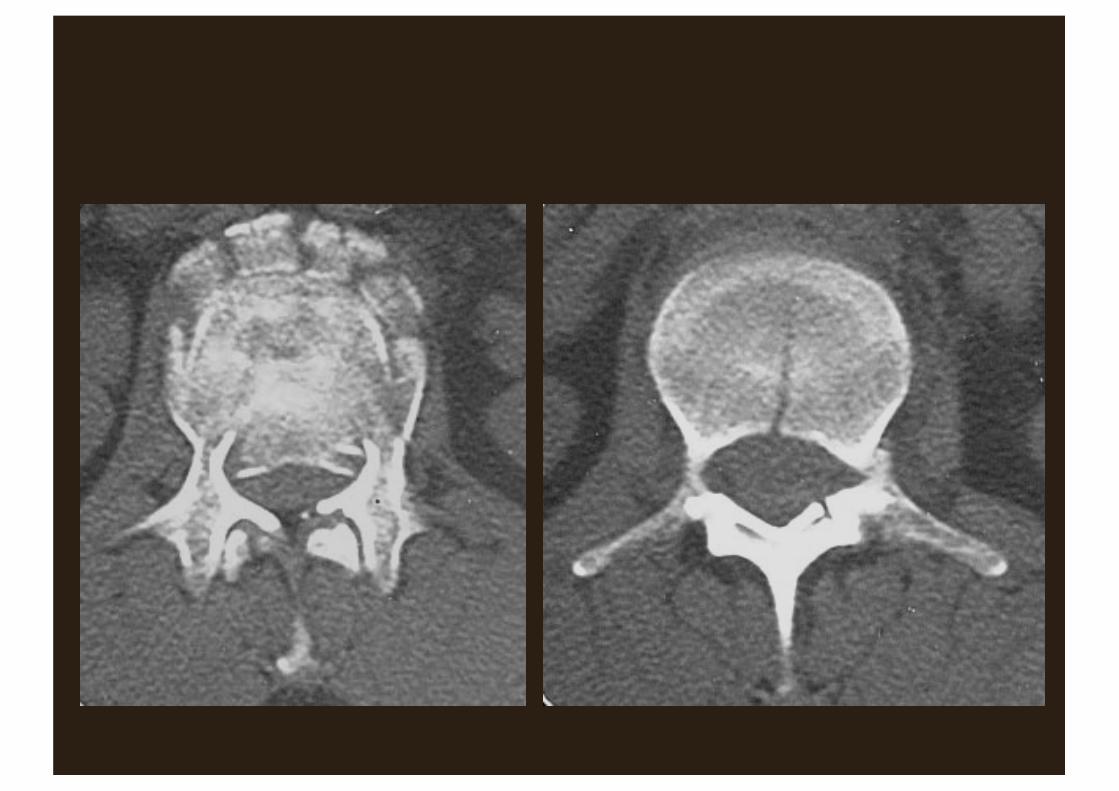
• 68M• Sudden onset bilateral leg pain and weakness• Urinary retention
What is the most likely diagnosis?
1. Guillain Barre syndrome2. Cauda equina syndrome3. Crush fracture secondary to osteoporosis4. Discitis/ osteomyelitis
What is the most appropriate imaging modality?
1. Plain film2. CT3. Scintigraphy (bone scan) 4. MRI
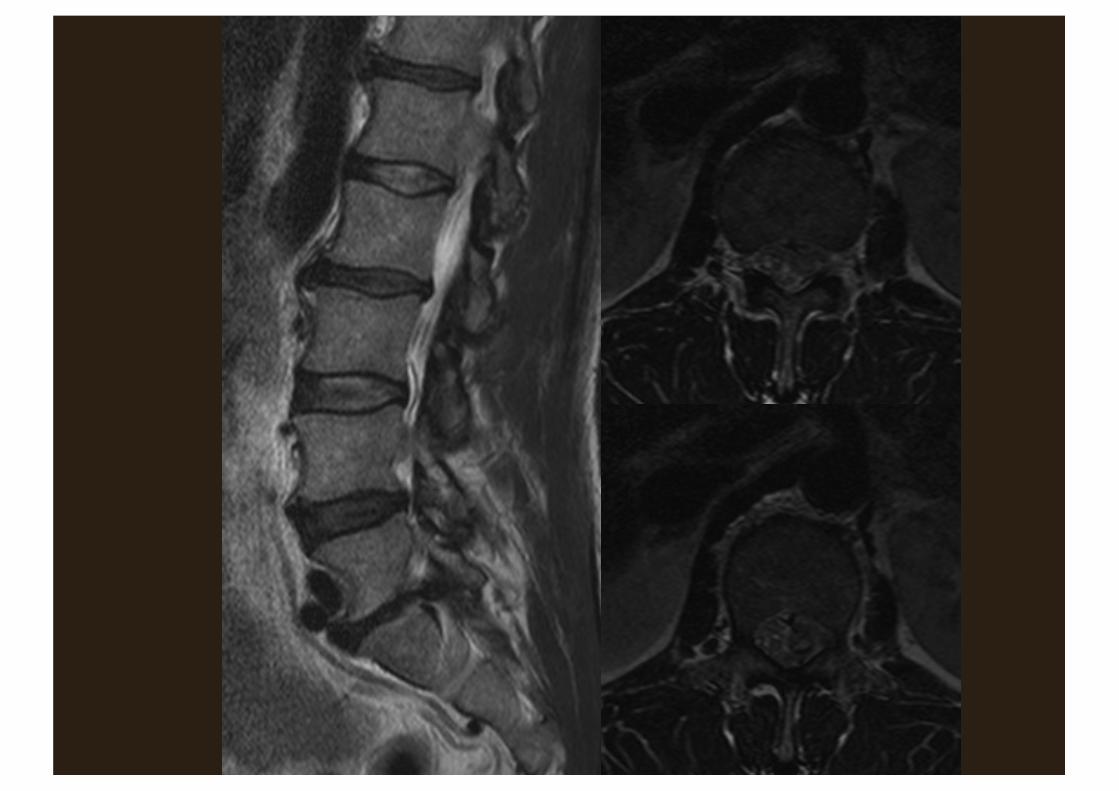
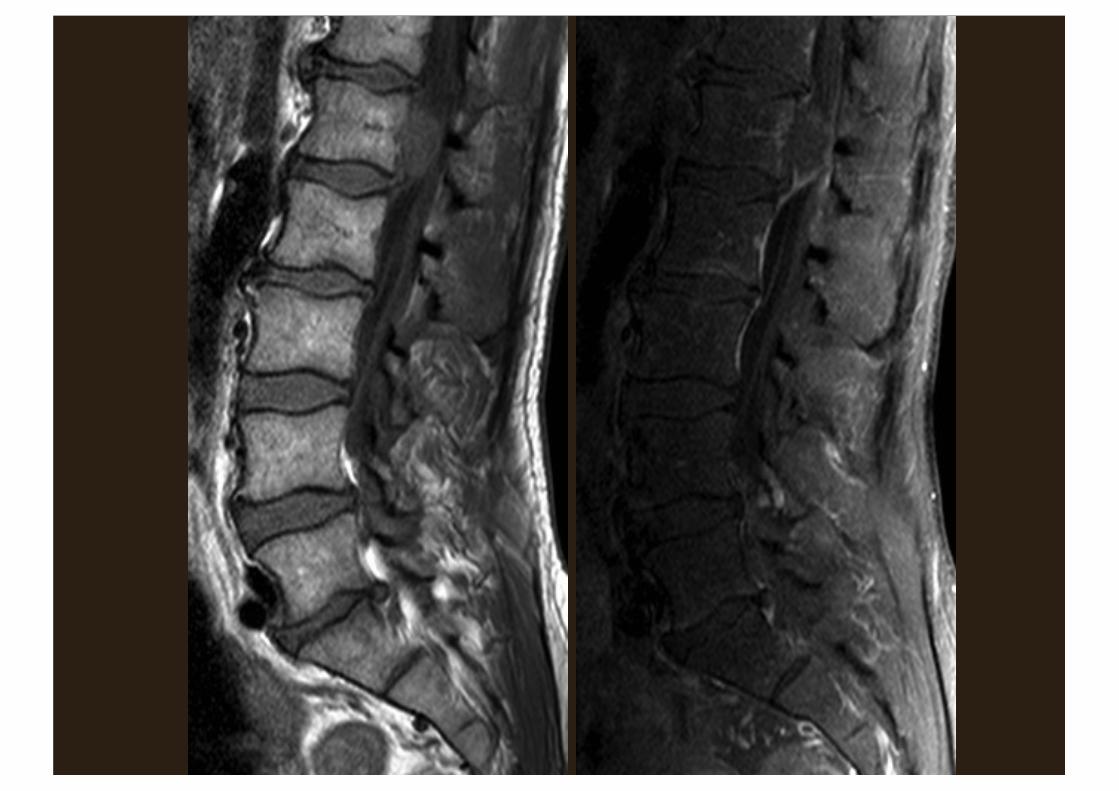
• Dx: Cauda equina syndrome• Cause: massive sequestration• Other causes:
– Tumour• Primary of lower cord: ependymoma• Primary of nerve: BPNST• Primary of dura: meningioma• Primary of vertebral body: chordoma, giant cell
tumour• Secondary
– Trauma
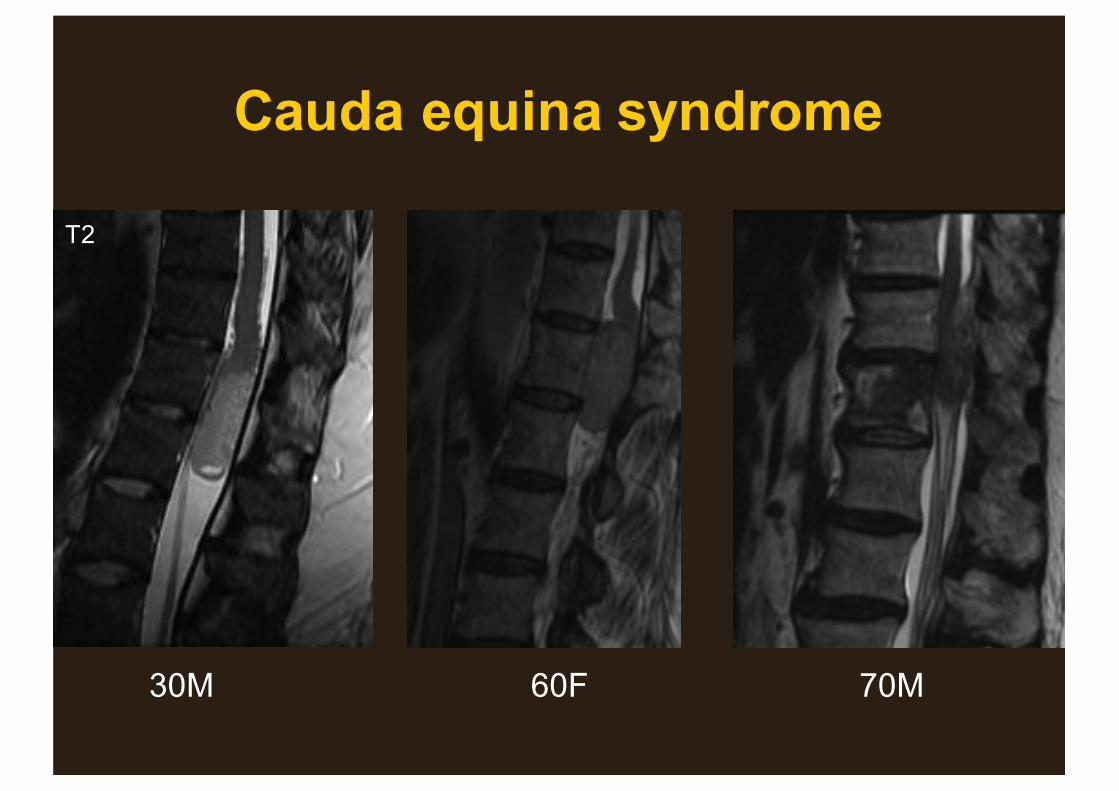
Cauda equina syndrome
30M 60F 70M
T2
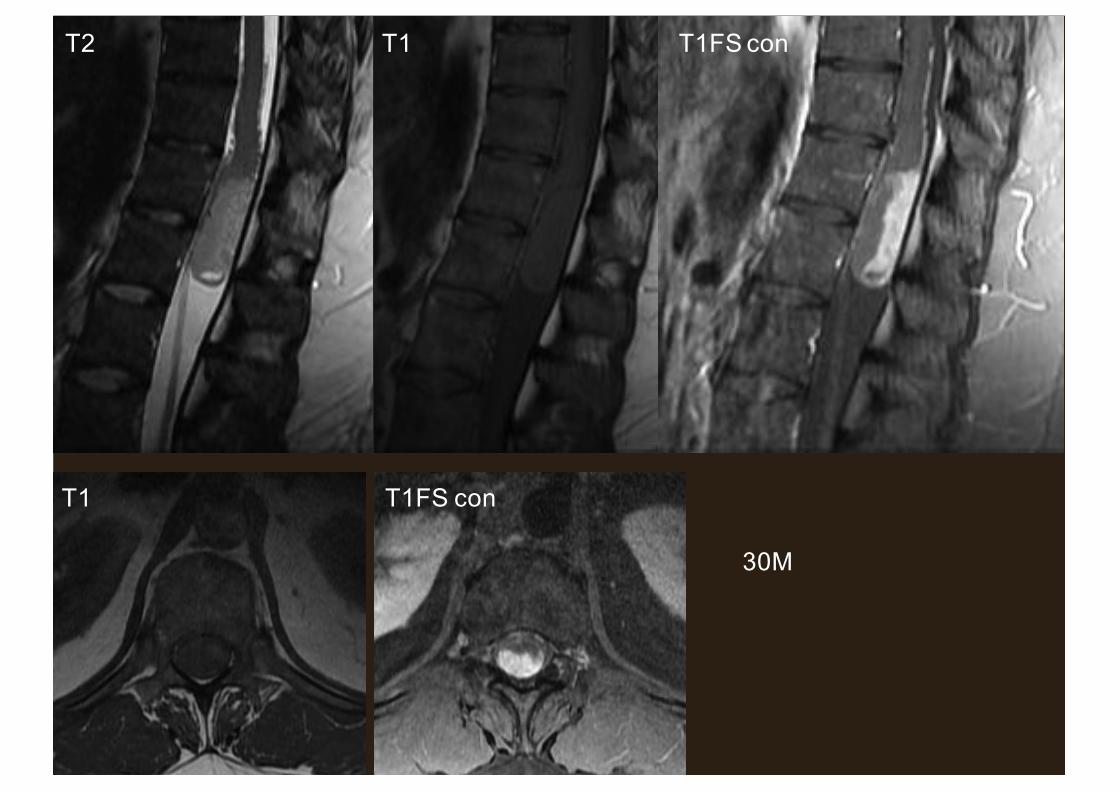
30M
T2 T1 T1FS con
T1 T1FS con





























