Embed Size (px)
DESCRIPTION
What do the Quality Ambitions mean for Primary Care? This session describes the ongoing innovative local improvements and national work with NHSBoards and Primary Care contractors to improve quality, efficiency and outcomes as well as the future plans for Primary Care.
Citation preview
DELIVERING QUALITY IN PRIMARY CARE: THE JOURNEY SO FAR
Sir Lewis Ritchie
Chair
DQPC Steering Group
THE JOURNEY SO FAR
Reflecting back...........




THE JOURNEY SO FAR
Putting quality on the map...........
.......a national perspective.......
The Journey So Far
Delivering Quality in Primary Care (DQPC).....
So: • What does the Quality Strategy mean for primary
care?
• What can primary care bring to the table?
The Journey So Far
• A reminder of why we set out on this journey:
- Huge challenges facing NHS – demography (60% increase in over 75s over next 20 years), money: ring fencing but still £300 million efficiencies
The Journey So Far
• A reminder of why we set out on this journey, cont…
- Primary care a critical part of the solution. 90% of
contacts; 23 million GP consultations; 1.9 million eye examinations; 91 million prescriptions dispensed, highly trained and capable resource......
- But.....a sense of a dis‑engagement in recent years. So...need to re‑engage and re‑energise.
2010 engagement process
• 6 regional events, 700 attendees from all PC players....
• Some key themes to emerge:
- Enthusiasm for the dialogue. Much scope for greater integration
- Finances a huge challenge but in every place people up for being part of the solution
- Real issues around motivation but quality seen as potential to be a key motivator
Follow up
Determined there should be actions as result – leading to a: Delivering Quality in Primary Care Action Plan
DQPC Action Plan: not an exhaustive (and exhausting) list nor a rival to the QS. But key national actions which would make the biggest difference.
Overseen by DQPC Steering Group. Bookend event – today: do stay! – to keep us honest and help refresh the plan.
Overarching themes
• Will mention a few of the actions, but first three very important overarching themes:
1 - Primary care's place at the table. Vital part of the solution. WHO has always said so. Increasingly recognised here
Overarching themesPrimary care's place at the table…
“We need to make sure people are admitted to hospital only when it is not possible or appropriate to treat them in the community ... doing all of these things will result in changes in the pattern of acute care and.. fewer acute beds and, as long as it is appropriate and as a result of the kind of service change we want to see, we should see that as a positive”
(Cabinet Secretary to Parliament, June 2011)
Overarching themes
Primary care's place at the table…
Key part in the Health Boards’ annual review process.
Today’s PC events as integral part of annual NHS Scotland event.
Overarching themes
2 – Need for grown up relationship with all independent contractors:
• For too long we’ve kept each other at arms length • Multi-professional Involvement in DQPC Steering Group, in individual actions and as day‑by‑day partners
Overarching themes
3 – The Leadership Imperative:
• Visionary and vigilance
• Enablement and encouragement
• Courage and example
What’s the bottom line?
• Actions set out in DQPC plan. Not list all now: a number, including local, will be showcased at 5.15pm
• A few highlights:
- eye care integration: potential to revolutionise primary/secondary care link
- prevention: Keep Well and Childsmile rolled out; £70m Change Fund
What’s the bottom line?
Highlights continued…
- GP access: toolkit developed with profession - developing a HEAT target on timely, accurate
info at the primary/secondary care interface - leadership: launch tomorrow of Strategic
Clinical Leadership network; plus joint RCGP/ NES initiative on leadership in primary care
What’s the bottom line?
• Looking forward to hearing your reactions on the journey so far and what lies ahead
• Meanwhile: some more detail on 3 of the key areas of activity– Primary /secondary care interface– Patient safety and – “Productive General Practice”
WHATS GOING ON OUT THERE?
PRIMARY CARE IN SCOTLAND
DR SHEENA L MACDONALDSenior Medical Adviser Scottish Government
The Complete Works of William Shakespeare (Abridged)By Adam Long, Daniel Singer and Jess Winfield
Damien Devine and Red Lion TheatresNew Red Lion Theatre
Review by Simon Sladen (2011)
Take 90 minutes, 37 plays, 3 actors, 1 famous bard, blitz them in a theatrical
blender and what do you get? An evening of pure Shakespearean fun courtesy of
The Complete Works of William Shakespeare (Abridged).
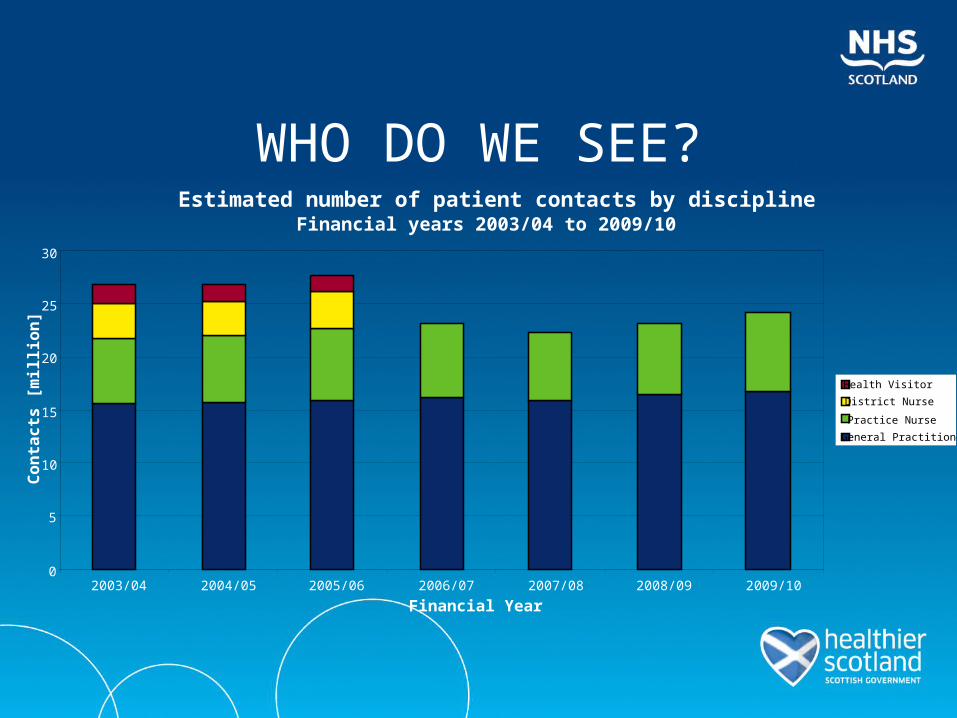
WHO DO WE SEE?Estimated number of patient contacts by discipline
Financial years 2003/04 to 2009/10
0
5
10
15
20
25
30
2003/04 2004/05 2005/06 2006/07 2007/08 2008/09 2009/10
Financial Year
Co
nta
cts
[m
illi
on
]
Health Visitor
District Nurse
Practice Nurse
General Practitioner
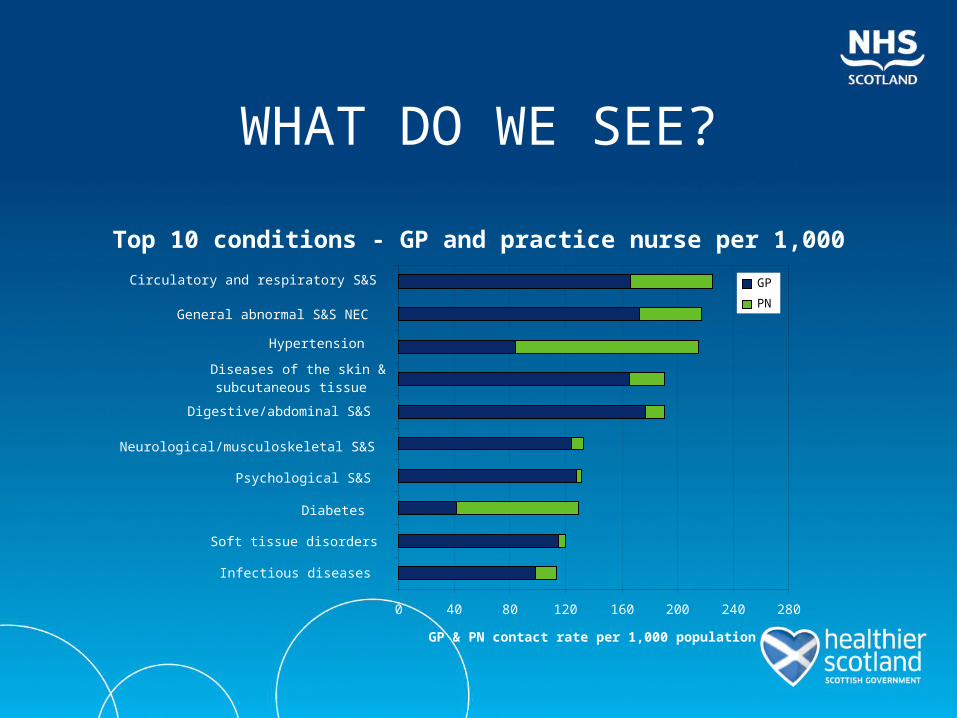
WHAT DO WE SEE?
Top 10 conditions - GP and practice nurse per 1,000
0 40 80 120 160 200 240 280
Circulatory and respiratory S&S
General abnormal S&S NEC
Hypertension
Diseases of the skin &subcutaneous tissue
Digestive/abdominal S&S
Neurological/musculoskeletal S&S
Psychological S&S
Diabetes
Soft tissue disorders
Infectious diseases
GP & PN contact rate per 1,000 population
GP
PN
WHAT HAPPENS TO THEM?
• “view the NHS as a service delivered predominantly in local communities rather than in hospitals; 90% of health care is delivered in primary care but we still focus the bulk of our attention on the other 10% - our current emphasis on hospitals does not provide the care that people are likely to need.”
Professor David Kerr 2005
WHAT HAPPENS TO THEM?
• Around 1 in 50 GP consultations results in an emergency inpatient admission. Thus 1000 GP consultations will result in 20 emergency inpatient admissions. If all GPs were able to refer only one fewer person in 1000 consultations ( i.e. referring 19 rather than 20 individuals), it would produce a 5% reduction in GP referred emergency admissions.
Professor David Kerr 2005
LOTHIAN EXPERIENCE
• 10% of practice population contact their practice every week
• 87% managed in Primary Care for next 4 weeks• 13% - 48% OPD 6% A&E 10% admissionsi.e. 2% result in unscheduled activity or 1.3% resulting
in direct admission
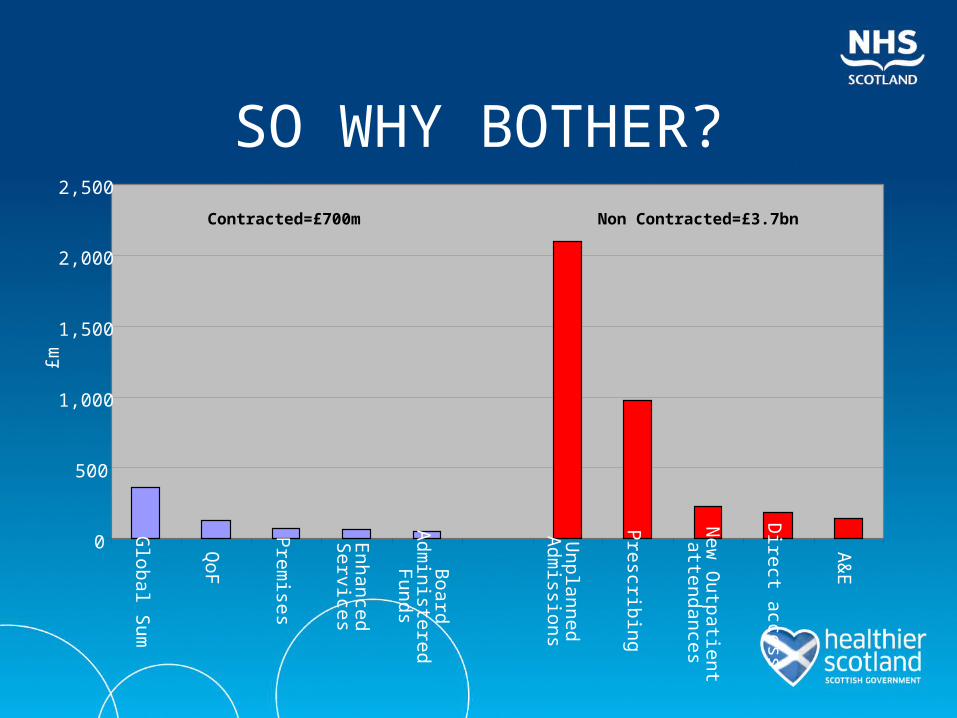
SO WHY BOTHER?
0
500
1,000
1,500
2,000
2,500
Glob
al Sum
QoF
Prem
ises
Enh
ancedS
ervices
Boa
rdA
dministered
Funds
Unplann
edA
dmissions
Prescribin
g
New
Outpa
tient
attendances
Direct access
A&
E
£m
Non Contracted=£3.7bnContracted=£700m
SO WHAT ARE WE DOING?
• The Quality Strategy & DQPC
• Closer working – look at variation and engage in a dialogue – 20% reduction in plain x-rays from one board 40% reduction in dermatology referrals form another
• QPQOF
QPQOF
• 3 work-streams – referrals, admissions and prescribing
• 3 activities – internal review of data, external peer review of data, agree on actions for prescribing and care pathways for referrals and emergency admissions
And so to the Future…
• Continue to develop QPQOF and emphasis on whole system working
• “Care delivered at the right time in the right place by the right person”
• Align local and national enhanced services to support
• Support AHP and Community Nursing to realign work priorities to support people to remain out of institutional care
Improving Patient Safety in Primary Care - The story so far
Neil Houston, NHS Forth Valley
SUB HEADING

SUB HEADING

Safety Improvement in Primary Care (SIPC 1)
Aims:
To enable 80 Primary Care teams to:
1.Identify and reduce harm to patients
2. Improve reliability of care for patients
On High Risk Medications
With Heart Failure
3.Develop safety Culture
4.Involve Patients in QI
Knowledge
• Topics• Tools• What to spread?• How to spread?
1. Reliable Care – Care Bundles
4 or 5 elements of care
Evidence based
Across Patients Journey
Creates teamwork
Done reliably
All or nothing
Small frequent samples
Heart Failure Bundle
1.Maximise medical therapy –On a licensed B BlockerB Blocker at max tolerated dose2.Functional assessment - NYHA recorded
in last year3.Immunisation - pneumococcal vaccine
ever 4.Self Management- information given to
patient on recognition of deterioration Improve QOL Reduce admissions
Bundles - Successes
“The care bundles were useful because it identified gaps”
Revealing unreliable practice
Indicating areas for improvement

2 – Data

Seeing Improvement
“You can see week by week, month by month, whether or not you are showing
any improvement, we seem to be improving and that’s good”
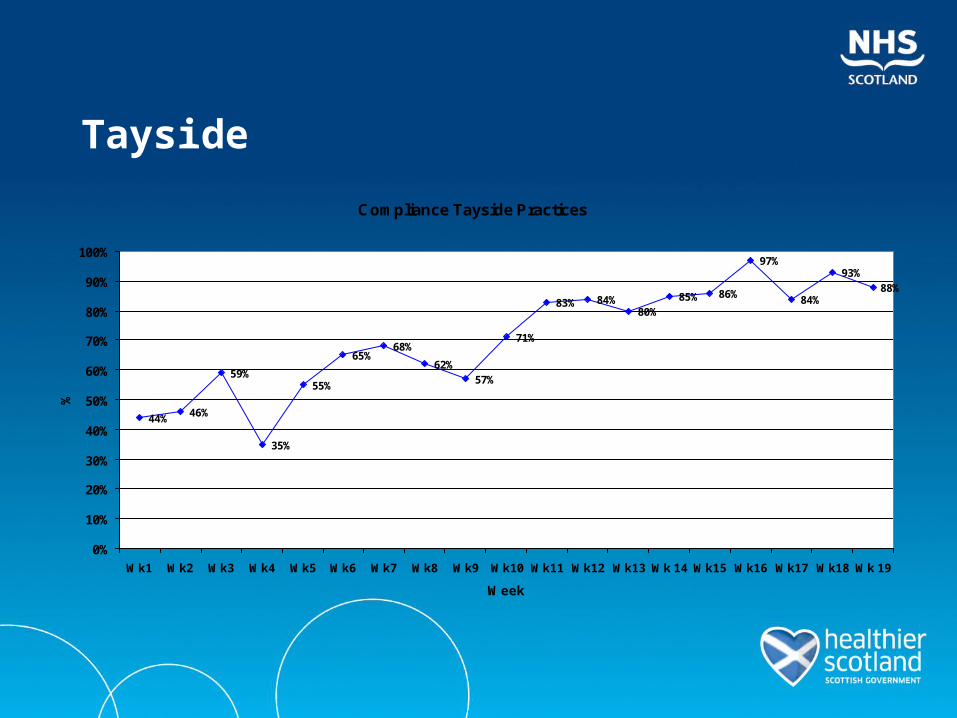
Tayside
Compliance Tayside Practices
44% 46%
59%
35%
55%
65%68%
62%57%
71%
83% 84%80%
85% 86%
97%
84%
93%88%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Wk1 Wk2 Wk3 Wk4 Wk5 Wk6 Wk7 Wk8 Wk9 Wk10 Wk11 Wk12 Wk13 Wk 14 Wk15 Wk16 Wk17 Wk18 Wk 19
Week
%
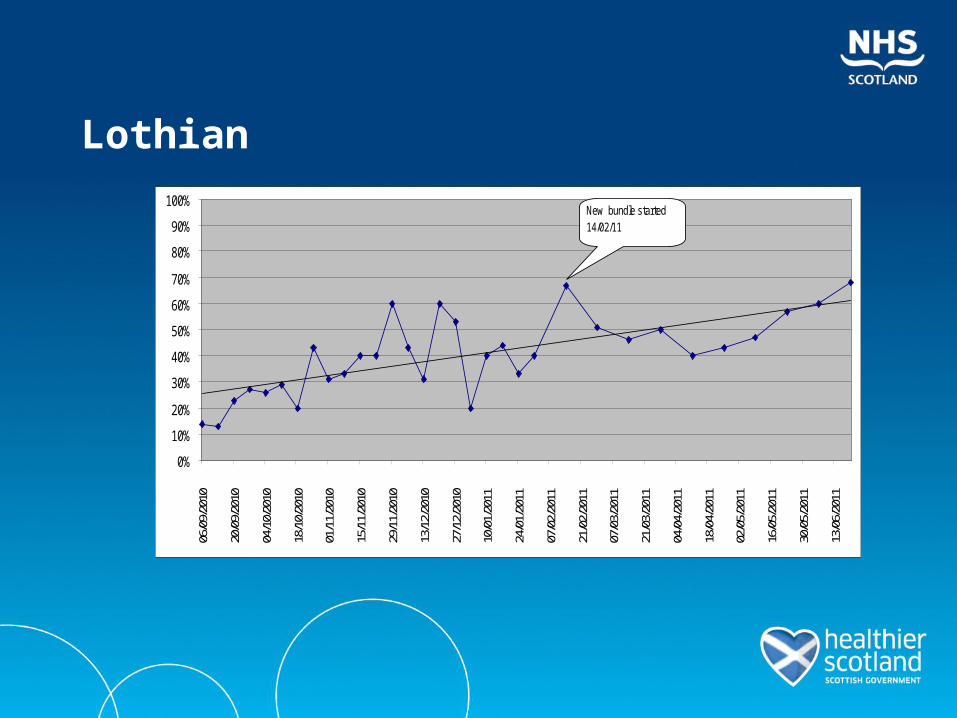
Lothian
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%06
/09/
2010
20/0
9/20
10
04/1
0/20
10
18/1
0/20
10
01/1
1/20
10
15/1
1/20
10
29/1
1/20
10
13/1
2/20
10
27/1
2/20
10
10/0
1/20
11
24/0
1/20
11
07/0
2/20
11
21/0
2/20
11
07/0
3/20
11
21/0
3/20
11
04/0
4/20
11
18/0
4/20
11
02/0
5/20
11
16/0
5/20
11
30/0
5/20
11
13/0
6/20
11
New bundle started 14/02/11
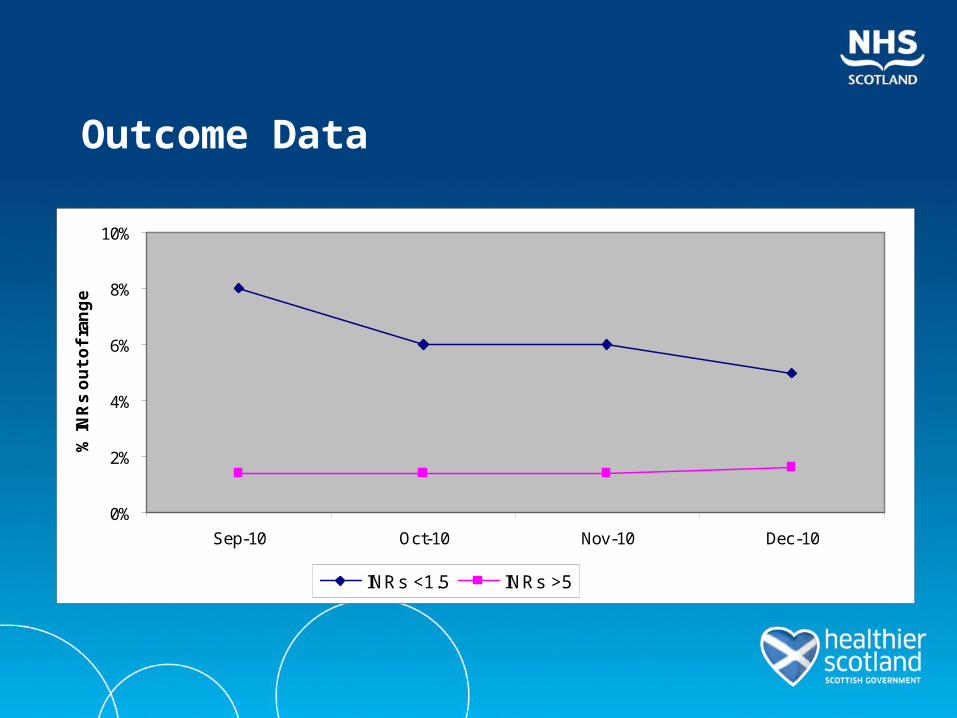
Outcome Data
0%
2%
4%
6%
8%
10%
Sep-10 Oct-10 Nov-10 Dec-10
% IN
Rs
ou
t o
f ra
ng
e
INRs <1.5 INRs >5
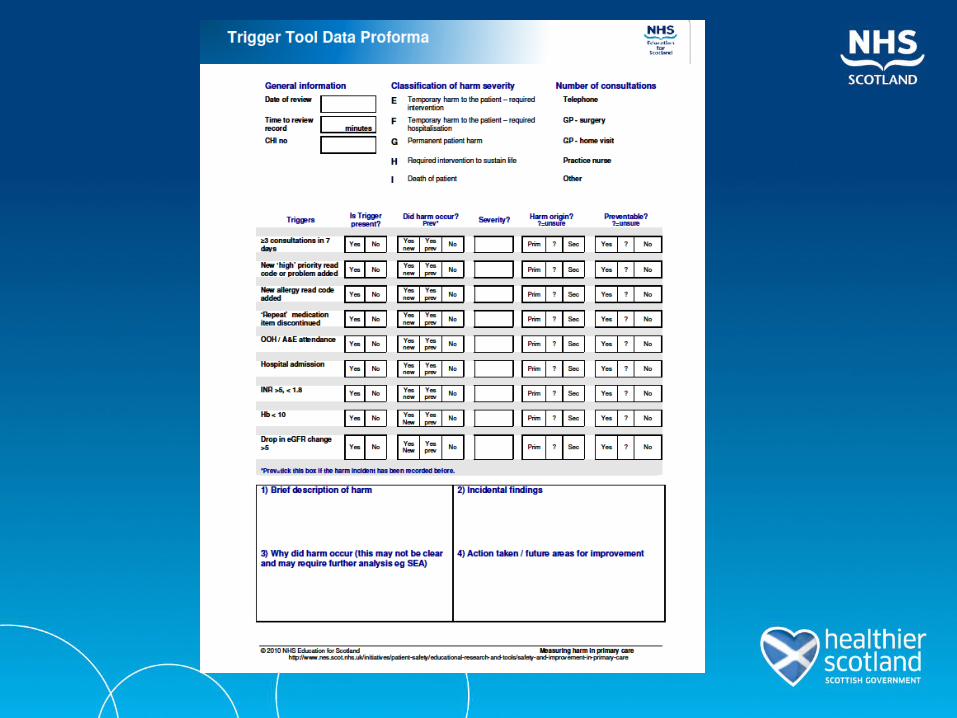
Trigger ToolsTo identify and reduce harm

SUB HEADING

SUB HEADING
Expectations
Hard to do
Time Consuming
Would not find harm
Threatening

Experience
Challenges
LogisticsTraining supportVariation?For measurement
Positives
QuickFinding HarmCultural changeImprovement
“Seemed a bit intimidating when we first had it presented to a large group … much
easier to use in practice … it’s a remarkably effective tool for reflective
analysis on patient safety and other clinical issues …has created a lot of interest from other doctors in the practice as a tool for
professional development and for appraisals”
Doctor Gordon Cameron
GP Edinburgh
Safety Culture
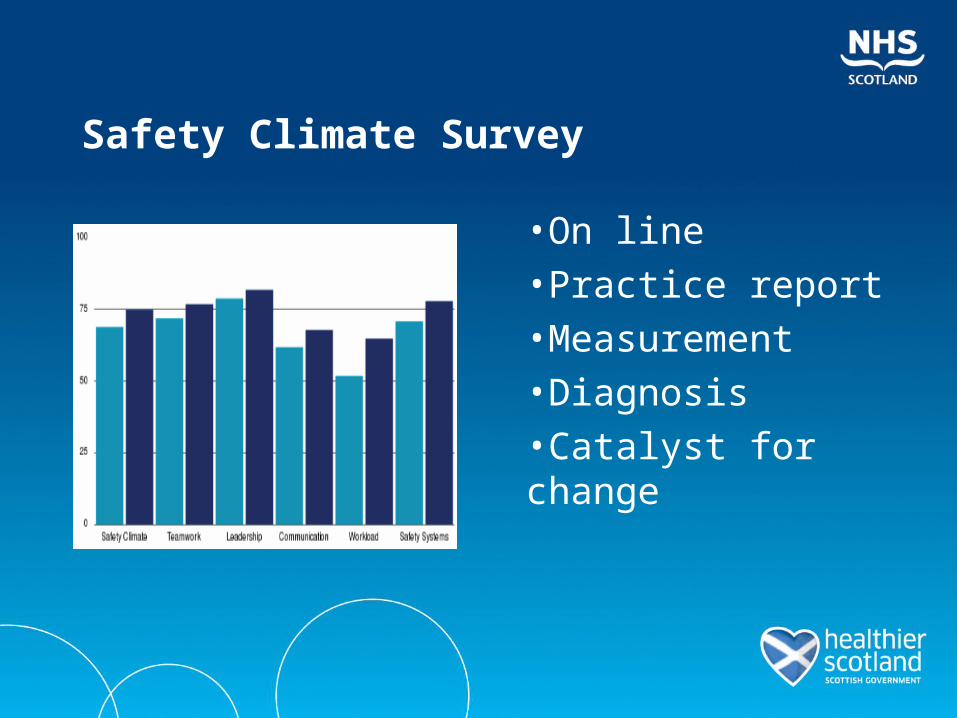
Safety Climate Survey
•On line•Practice report•Measurement•Diagnosis•Catalyst for change
Insights
“Many of us in the practice staff hadn’t really made the link that us failing to
communicate in was a threat to patient safety ….we had a lot of really good
stuff came out of it, a lot of very open discussion”
Experience so Far
Practices are interested
Acts as a catalyst
Need guidance and support
Better process and report
Challenges – understanding/using it /anonymity
Developing a Programme
• Scoping
• Develop aims/measures/tools
• Implementation strategy
• Launch 2013
• Looking for volunteers…..
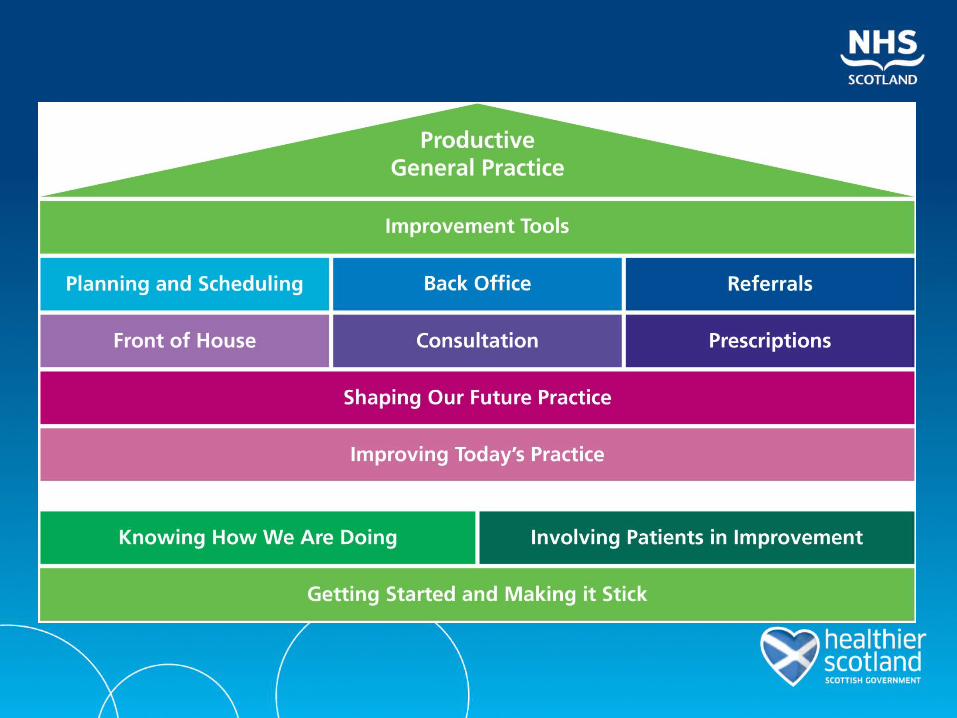
Productive General PracticeSusan Bishop & Mary Freel
Aim
• Introduce the Lean context for Productive General Practice and describe PGP’s structure
• Explain how it can support you in Delivering Quality in Primary Care
• Describe how it’s being used and some examples of the benefits it offers
Productive General Practice uses Lean Principles Specify what does & does not add value – from the
patient’s perspective.
Identify steps necessary to design, order and produce across the whole value stream.
Make those actions flow without interruption, detours, waiting or rework.
Only make what is pulled by the patient.
Strive for perfection by continually improving & removing wastes as they are uncovered.
Why is it relevant?
• Lean is a systematic approach to reducing waste through a process of continuous improvement
• Waste is anything other than the minimum amount of Practice equipment, materials, space and time which are essential to add value to the patient or service.
• A Lean ‘Goal’ is to supply a product or service to the patient’s demand with 100% quality
• Making the right thing easier to do – for every person, every time
The benefits it offers…Stanley Medical Group, County Durham
• Reviewed their recall system for patients needing routine drug monitoring
• Applied lean principles to understand the current process and design an improved process
• Existing system lead to inconsistencies, waste and patient safety risk
• Results:– Patient Safety (faster lead time and higher degree of accuracy)– Time (35 hours/month to 0.53 hours/week)– Patient experience (increased HCA patient facing time)– Money (£4150/year) Stanley Medical Group, County Durham
Source: Iain Smith, Corporate Improvement Team, North East Transformation System
“Streamlining this process has saved us time but the real benefit has been that we have improved patient safety and the patient experience, as we are now able to offer more appropriate appointments”
Sue Elsbury, Practice Manager
The benefits it offers.. William Brown Centre, Peterlee
• Practice nurse team applied 5S, a fundamental lean tool to their working environment
• Impact– Reduction in inventory– Reduction in interruptions to consultations– Improved efficiency (e.g. staff walking distances reduced from
174 steps/ patient cycle to 18 steps/ patient cycle
“By using simple tools to make simple changes you can made a lot of difference and I would recommend it to anyone thinking of using this approach”
Dr Russell, GP
Source: Iain Smith, Corporate Improvement Team, North East Transformation System
The background to PGP in Scotland
• Focus on improving both quality and efficiency
• Delivering Quality in Primary Care Action Plan
• Working partnership – Scottish Government– Institute for Innovation and
Improvement – RCGP Scotland– Quality Improvement Hub– Primary Care Leads
Productive General Practice in Scotland
• UK launch in November• Grampian, Tayside and Glasgow developing, or testing
modules• Early Adopters in Grampian and Tayside starting August• www.evidenceintopractice.scot.nhs.uk• Expert advice and coaching Quality & Efficiency Support
Team & RCGP
The Crescent Medical PracticePatient survey response 96%
Overall P atient E x perienc e S urvey R es ults
0
20
40
60
80
100
120
140
R es pec ted P leas ed V alued C ared for Involved Not lis tenedto
Hurried F rus trated Anxious
Ac c es s ing appointment
Arriving and c hec king in
Information
Waiting
C ons ultation and nexts teps
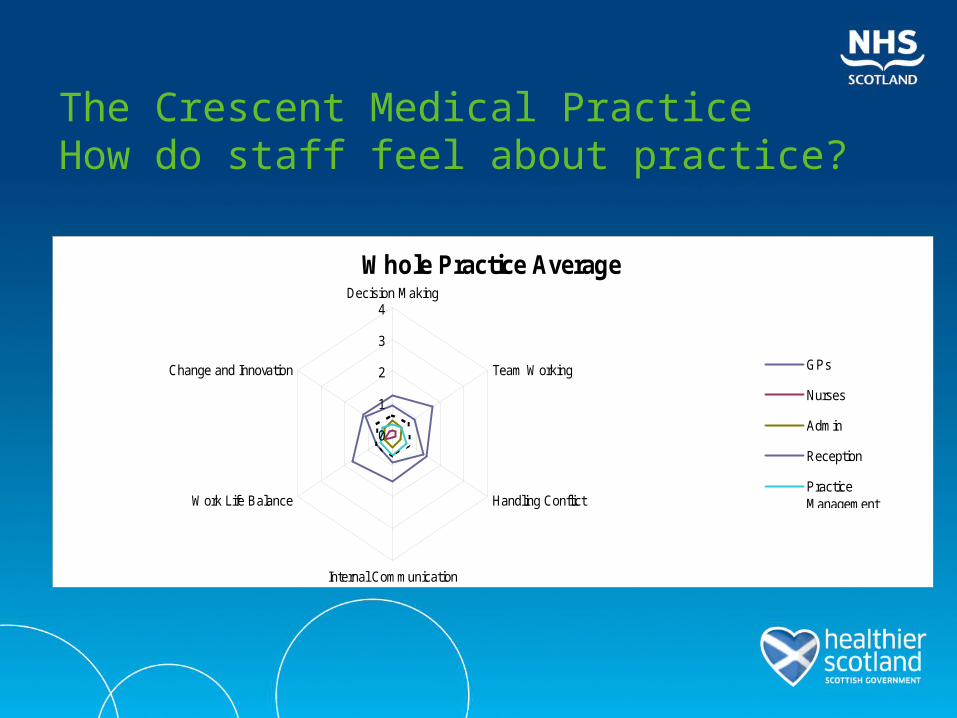
The Crescent Medical PracticeHow do staff feel about practice?
Whole P rac tic e Averag e
0
1
2
3
4Dec is ion Making
Team Working
Handling C onflic t
Internal C ommunic ation
Work L ife B alanc e
C hange and Innovation G P s
Nurs es
A dmin
R ec eption
P rac tic eManagement Whole P rac tic e
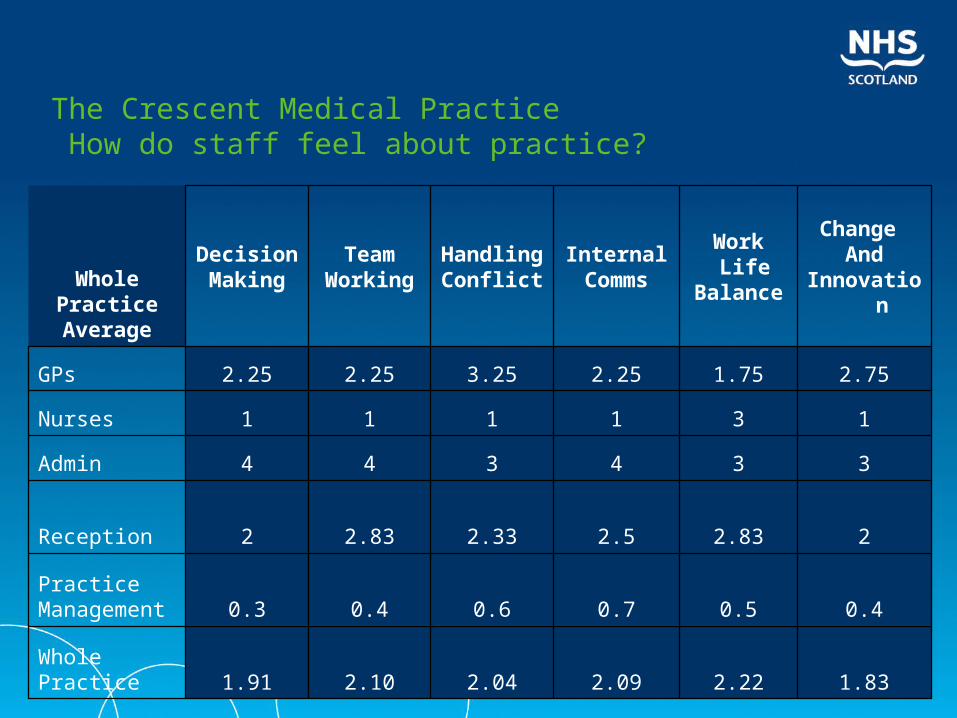
The Crescent Medical Practice How do staff feel about practice?
1.832.222.092.042.101.91WholePractice
0.40.50.70.60.40.3PracticeManagement
22.832.52.332.832Reception
334344Admin
131111Nurses
2.751.752.253.252.252.25GPs
Change And
Innovation
Work Life
Balance
InternalComms
HandlingConflict
TeamWorking
DecisionMakingWhole
PracticeAverage
NHS Lothian’s PC Forward Group
Duncan Miller General Manager, Primary Care Contracts, NHS Lothian
DELIVERING QUALITY IN PRIMARY CARE: THE JOURNEY SO FAR
Closing thoughts......

Securing success….
• Empowered patients – high quality preventive and reactive health care
• Enabled professionals – innovative multi-professional teamwork – pulling together
• Effective leadership – vision, courage and encouragement
• Excellence in practice – pressing on
Success is a journey….. not a destination!

Thank youfor listening
Thank youfor coming andparticipating

Reminder Invitation
You will be most welcome to attend our Delivering Quality in Primary Care Fringe Session ......
4:45-7pm today
• Questions/ thoughts/ comments…?