Embed Size (px)
Citation preview

Pulmonary toxicity caused by cytotoxic drugs
DR. J. ROIG CUTILLASHOSPITAL NOSTRA SRA. MERITXELL
ANDORRA
Alkylating agents Cyclophosphamide, nitrosureas, ifosfamide, procarbazine, busulfan, melphalan, chlorambucil
Antimetabolites Methrotrexate, gemcitabine, azathioprine, 6-mercaptopurine, cytosine arabinoside, fludarabine
Antibiotics Mitomycin, doxorubicin, bleomycin, neocarzinostatin
Antimicrotubule agents
Vinca alkaloids Taxanes: paclitaxel, docetaxel
Miscellaneous Topotecan, irinotecanEtoposide, teniposideGefitinib, ATRA, arsenic trioxide
Chemotherapeutic agents and pulmonary toxicity
Roig J et al. Clin Pulm Med 2006
Chemoterapy-induced lung toxicity: differential diagnosis
• Pulmonary infection• Malignancy-related thromboembolism• Local tumor progression• Iatrogenic diffuse alveolar hemorrhage• Radiation-induced pneumonitis• O2, transfusion, other drug-induced toxicity• Postoperative complications

Chemoterapy-induced lung toxicity: clinical clues
• Time course & high index of suspicion• Not distinctive features; sometimes fever• Subacute or even abrupt onset are possible• X-ray lags behind clinical symptoms: CT• Decreased DLCO: early marker & monitor• Increased DLCO: diffuse alveolar bleeding• Nonspecific imbalance of CD4/CD8 (BAL)

Chemotherapy-induced lung toxicity: role of other factors
• Biological response modifiers• Hormonal agents• Other agents: www.pneumotox.com• Interactions with radiotherapy• Interactions in combination
chemotherapy• Thoracic surgery following
chemotherapy
Chemotherapeutic agents used in lung cancer that may cause acute pneumonitis
CyclophosphamideDocetaxelEtoposideGemcitabineIfosfamideIpomeanolIrinotecanMethotrexateMitomycin PaclitaxelProcarbazineVinca alkaloids

Tissue Reactions in Chemotherapy-induced Pulmonary Toxicity
Chronic interstitial pneumoniaDiffuse alveolar damage – Acute interstitial pneumoniaBronchiolitis obliterans organizing pneumonia (BOOP)Obliterative bronchiolitisHypersensitivity pneumoniaa
Lung fibrosisPulmonary edemaPulmonary hemorrhagePulmonary hypertensionPulmonary veno-occlusive disease
aPoorly formed granulomas in methotrexate lung toxicity

Chemotherapeutic agents used in lung cancer that may cause ADRS
GemcitabineGefitinibMethotrexateMitomycin PaclitaxelVinca alkaloids + mitomycin
Roig J et al. Clin Pulm Med 2006; Inoue A. Lancet 2003

Chemotherapeutic agents used in lung cancer that may cause pulmonary fibrosis
CyclophosphamideEtoposideMethotrexateMitomycinNitrosureas
Roig J et al. Clin Pulm Med 2006

Chemotherapeutic agents used in lung cancer that may cause pleural disease
CyclophosphamideDocetaxela
Doxorubicinb
MethotrexateMitomycinProcarbazineVinblastine + mitomycin
Roig J et al. Clin Pulm Med 2006
a Trasudative pleural effussion caused by fluid retention syndromeb Trasudative pleural effussion caused by congestive heart failure

Chemotherapeutic agents used in lung cancer that may cause an hypersensitivity reaction with
respiratory symptoms
Roig J et al. Clin Pulm Med 2006
DocetaxelEtoposideGemcitabineIfosfamide + mesnaIrinotecan
MethotrexateMitomycinPaclitaxelProcarbazineTopotecanVinca alkaloids

Bronchial artery infusion in central lung cancer and metastasis
Risk of massive hemoptysis1 to 3 months after BAIHerald: hemoptoic sputumNeed urgent arteriographyBronchial vascular fistulaRare esophageal ulcerationBronchial esophageal fistulaSpinal cord damage
Osaki T. Chest 1999; Suzuki T. J Bronchol 2001

Neglected respiratory toxicity(1)• Vincristine, procarbazine, cytarabine,
chlorambucil may cause neuropathy that might affect respiratory muscle function
• Does it imply an increased anesthesia risk ?• Risk of acute encephalopaty and respiratory
depression with ifosfamide, metothrexate in SAS and advanced COPD with hypercapnic failure
Aldrich T, Clin Chest Med 1990; Klein D, Can A Sc J 1983; Roig J, Clin Pulm Med 2006

Neglected respiratory toxicity(2)• Some cases of intrathoracic extravasation• Venous thromboembolism associated with
central venous lines and subcutaneous ports
• Increased hypercoagulability of concomitant therapies (erythropoietin, megestrol acetate) and malignancy itself
Bozkurt AK.. Am J Clin Oncol 2003; Verso M. J Clin Oncol 2003; Biffi R. Cancer 2001; Bauer K. J Clin Oncol 2000; Wun T. Cancer 2003, Bolen J. A Am Med Dir Assoc 2000
Chemoterapy-induced lung toxicity: prevention in COPD
• High-risk (30%) if nitrosureas are used• Sleepness with ifosfamide, methotrexate• More risk in “overlap”: COPD + SAS• Water retention: taxotere,
ciclophosphamide• Increased risk of O2 toxicity• Sensorimotor neuropathy and interactions

Ifosfamide-induced lung toxicity
Clinical presentation
Respiratory features
Incidence Outcome
Acute Hypersensitivity reaction (mesna)Encephalopathy and respiratory depressiona
Rare acute pneum
CNS depression <12%
Usually recovery
a Concern in advanced COPD and SAS
Cameron JC. Cancer Nurs 1993; Baker WJ. Cancer 1990

Campothecin-induced lung toxicity
Agent Type Incidence Outcome
Topotecan
Irinotecan(CPT-11)
Mild dyspnea
Dyspnea Acute pneumonitis
<3%
< 22%1-13%
Reversible
Maksymiuk A, Am J Clin Oncol 1998; Masuda N, J Clin Oncol 1992;Takeda K, Br J Cancer 1999

Gemcitabine-induced lung toxicity
Clinical presentation
Respiratory features
Incidence Outcome
Acute Hypersensitivity reactionAcute pneumonitis Rarely ARDS, PVODa
<1 % Usually complete recovery except in ARDS
a Pulmonary venoocclusive disease
Proc ASCO 2000; Tempero MA. Cancer 1998; Marruchella A.Eur Resp J 1998; Nackaerts KL. Ann Oncol 1998; Vansteenkiste J.Lung Cancer 2001.

Mitomycine - induced lung toxicity Clinical presentation
Respiratory features
Incidence Outcome
Acute
Chronic, dose-related (total dose >30 mg/m2)
Acute pneumonitis
Very rarely thrombotic microangiopathy with ARDS
3 % -12 % Fatality rate 40% Increased risk if combined therapy with vinca alk.Increased risk of microangiopathy if associated with fluoruracil (highest mortality)
Rivera MP. Am J Clin Oncol 1995, Linette DC. Ann Pharm1992, Verweij J. Cancer 1987 Thompson C. South Med J 1992
A
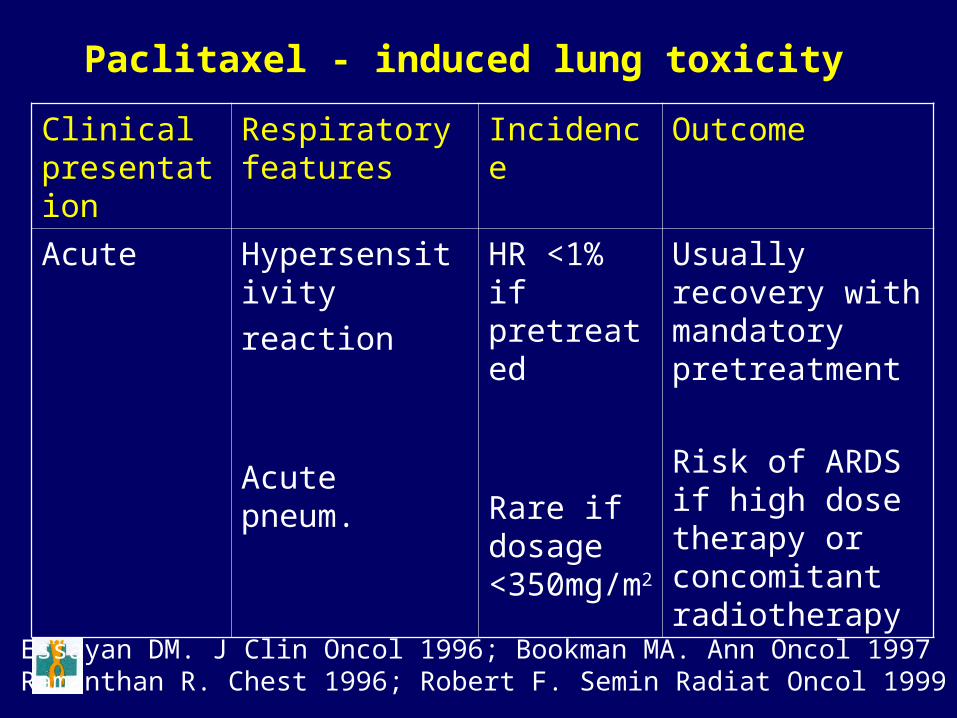
Paclitaxel - induced lung toxicity
Clinical presentation
Respiratory features
Incidence Outcome
Acute Hypersensitivityreaction
Acute pneum.
HR <1% if pretreated
Rare if dosage <350mg/m2
Usually recovery with mandatory pretreatment
Risk of ARDS if high dose therapy or concomitant radiotherapy
Essayan DM. J Clin Oncol 1996; Bookman MA. Ann Oncol 1997Ramanthan R. Chest 1996; Robert F. Semin Radiat Oncol 1999

Docetaxel - induced lung toxicity
Clinical presentation
Respiratory features
Incidence Outcome
Acute
Chronic
Acute pneumonitis
Fluid retention syndrome
Very rare
Increased risk of retention if >400 mg/m2
Usually complete recovery
Etienne B. Rev Mal Respir 1998; Briasoulis E. Respiration 2000

DIFF. DIAGNOSIS: ALGORITHMIC APPROACH
Chest symptoms + abnormal X-ray
Clinical evaluation
Non-infectious cause
Infection not excluded
Appropriate treatment
Non-invasive work-up
Early antibiotic
No impr. Improved
Continue AbInvasive proc. Keep Ab
+ -

Invasive diagnostic work-up•FOB: bronchial aspirates, PSB, BAL, TBB•Transthoracic needle aspiration (TNA)•Lung biopsy – VATS•Open lung biopsy: minithoracotomy
Dorca J. 1995: ultrathin (25G)TNA in 97 cases of non-mechanically ventilated pneumoniaTransient hemoptysis: 5 cases (5.2%)Self-limited partial pneumothorax: 3 cases (3%)Sensitivity 60.9%; PPV 100%; modified treatment in 30%

HRCT in patients with dyspnea, fever of unknown origin and normal X-ray
• Immunocompromise, severe emphysema
• May detect an unsuspected alveolar infiltrate or a subtle interstitial pattern
• Guide for FOB techniques ► better yield
Brown MJ. Acute lung disease in the immunocpmpromised host: CT and pathologic findings. Radiology 1994; Ramila E. Bronchoscopy guided by HRCT for the diagnosis of pulmonary infections in patients with hemathologic malignancies and normal plain chest X-rays. Haematologica 2000

Reliability of transbronchial biopsy• High utility only in case of:
–Sarcoidosis–Lung cancer and some mestastases–Opportunistic infections in
immunocompromised host–Lung transplantation
Gal A. Adv Anat Pathol 2005

Lymphatic carcinomatosis may mimic severe bronchial asthma
• Mendeloff A. Severe asthmatic dyspnea as the sole presenting symptom of generalized endolymphatic carcinomatosis: report of two cases with autopsy findings and review of the literature. N Eng J Med 1945
• Masson RG. Pulmonary microvascular cytology in the diagnosis of lymphangitic carcinomatosis. N Eng J Med 1989

Microscopic pulmonary tumor embolism may cause respiratory failure
• Sometimes is the initial, subacute presentation of occult malignancy
• Clue: precapillary pulmonary hypertension without thromboembolic disease and negative usual complementary tests
• Value of wedge aspiration cytology
Masson RG. Pulmonary microvascular cytology. A new diagnostic application of the pulmonary artery catheter. Chest 1985; Stucky A. A rare cause of fatal right heart failure. Eur J Intern Med 2006

Chemoterapy-induced lung toxicity: therapeutic approach
• Early detected, non-severe cases: cessation• Severe cases: steroids on a timely fashion• Dosage & tapering: individualized basis• Transplant? (Santamauro JT, Chest 1994)• Desensitization possible, not recommended• Premedication mandatory with some agents• Future: Gene therapy? (West J, Chest 2001)