WELCOME
WELCOME
Date-15/6/2015
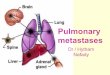
Pulmonary MetastasesDr. Manmohan Bir ShresthaMD Resident,
Phase-ADepartment of Radiology & Imaging
MetastasisMetastasis are the tumor implants discontinuous with
primary tumor.It is the hallmark of malignancy.All cancers can
metastasize with few exceptions. The major exceptions are gliomas
and basal cell carcinoma.
Pulmonary MetastasesIn about 75 % cases, presents as multiple
pulmonary nodules.
Also present as solitary pulmonary nodule/ cavitation/
calcification.
Approximately 3 % of asymptomatic pulmonary nodules are
metastases.
Site
Usually bilateral, affecting both lungs equally with a basal
predominance.
They are often peripheral and may be subpleural.
Route of spreadMost commonly - haematogenous.
Lymphatic spread - less common.
Endobronchial spread - rare
Lungs Filter like OrganSupplied by pulmonary artery containing
deoxygenated blood from right ventricle.This blood contains
lymphatic fluid from the body tissues which flows into the
lungs.
Primary siteMay originate at any site.
Approximately 80 % of pulmonary metastases arise from primary
tumours of-BreastSkeletonUrogenital system.
Clinical featuresCoughDyspnea or shortness of breathChest
painHaemoptysisHoarseness of voiceFeatures of secondary pulmonary
infection.
Radiological findingsCommonOther
patternsNodules.CavitationCalcificationPneumonia-like
consolidationA halo of ground glass
opacity.EndobronchialCannon-ball metastasesMiliary
metastasesLymphangitis carcinomatosa.
NodulesMay be solitary or multiple.Rounded nodules of variable
sizes ranging from few millimeters to few centimeters with
well-defined margin.75 % - multiple pulmonary nodules.Commonest
tumours producing solitary pulm. nodules are carcinomas of
ColonKidneyBreastTesticular tumoursBone sarcomasMalignant
melanoma.
CavitationMay occur from any site.
More common from-Squamous carcinomas from head &
neckSarcomas.May be seen after chemotherapy
Subpleural cavitation is a recognized cause of spontaneous
pneumothorax.
Absent fluid levels.
CalcificationIs seen in some cases.
Most often in Osteogenic sarcomaChondrosarcomaMucinous
adenocarcinoma.
Pneumonia-like consolidation
Adenocarcinoma metastases may destroy adjacent lung parenchyma,
resulting in pneumonia-like consolidation.
A halo of ground-glass opacity
Ground-glass opacity surrounding a mass or a nodule which
represents haemorrhage.
Seen in choriocarcinoma & angiosarcoma.
Endobronchial metastasesRareThey may occlude the airway and
cause segmental or lobar collapse.Primary sites being Kidney
BreastLarge bowel.
Cannon-ball metastasesCommonest primary sites
beingRCCChoriocarcinoma.
Miliary metastases
Commonest primary sites are-Thyroid carcinomaMalignant
melanomaRCCOsteosarcomaPancreatic neoplasms.
Lymphangitis CarcinomatosaResults from haematogenous metastases
invading and occluding peripheral pulmonary lymphatics.Commonest
primary sites areLung BreastStomachPancreasCervixprostate
ContUsually bilateral, but lung and breast cancer may cause
unilateral lymphangitis.
Chest X-rayCoarse, linear, reticular and nodular basal shadowing
often with pleural effusions and hilar lymphadenopathy.
Cont
HRCTNodular thickening of the interlobular septa and thickening
of the centrilobular bronchovascular bundles.
D/D of a solitary pulmonary
noduleMalignantBenignGranulomaInfectionPulmonary infarctPulmonary
haematoma
7.Collagen diseases8.Congenital9.Impacted
mucus10.Amyloidosis11.Intrapulmonary lymph
nodePleuralNon-pulmonary
D/D of a multiple pulmonary
noduleMalignantBenignInfectionInflammatoryVascularMiscellaneous.
D/D of a cavitating pulmonary
lesionInfectionsMalignantAbscessPulmonary infarctPulmonary
haematomaPneumoconiosis7. Developmental8. Sarcoidosis9. Bulles,
blebs10. Traumatic lung cysts11. Pneumatocele.
Approaching to the pulm. metastasesPulmonary metastases initial
finding
Unknown Primary.
Clinical presentation and clinical evaluation.
ContChest X-ray
CT Scan
PET Scan
Cont.Cytological examination of sputumCytological examination of
pleural fluidFNAC or excision biopsy of an enlarged lymph
nodeBronchoscopy- biopsy bronchoscopic alveolar lavage
cytology.
ContUSG guided FNAC of lesionCT guided FNAC of lesionSurgical
lung biopsy or open lung biopsyHRCT.
ComplicationsPneumothorax
Pleural effusion
Lung collapse.
Treatment modalitiesChemotherapyRadiotherapyPlacements of stents
in the airwaySurgicalPalliative care.
THANK YOU




![Spontaneous Regression of Pulmonary Metastases from ...downloads.hindawi.com/journals/sarcoma/2008/940656.pdfS. W. Kim and J. Wylie 3 primary tumour [13]. An activation of intrinsic](https://img.pdfslide.us/doc/110x75/5feb63bcc77d105ebe249e2a/spontaneous-regression-of-pulmonary-metastases-from-s-w-kim-and-j-wylie-3.jpg)