Embed Size (px)
Citation preview

Mr Marc Laniado and Dr Tristan BarrettPut your heads together: MDT decision-making – pitfalls and patient outcomes
Bayer Radiology Academy Forum on Breast and Prostate MRI • 17 November 2017
Prescribing Information is available on request
Adverse events should be reported. Reporting forms andInformation can be found at www.mhra.gov.uk/yellowcard.
Adverse events should also be reported to Bayer plc. Tel: 01635 563500; Fax: 01635 563703; Email: [email protected]
This meeting has been organised and is fully funded by Bayer; all presenters are receiving an honorarium for their involvement.
UKGDV04170006al Date of preparation November 2017

Dr Barrett: None to declare
Mr Laniado: Share ownership in Nuada Medical - a company that provides MRI-targeted transperinealprostate biopsies equipment
Disclosures

MDT Decision Making: Pitfalls & Patient Outcomes
Tristan BarrettMarc Laniado
UKGDV04170006al;November2017

MDT meetings contribution from medical specialists, nurses & allied specialties
Clinical Nurse Specialists
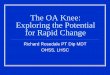
Multi-Disciplinary Meetings (MDM) aims: 1) More evidence-based practice

Multi-Disciplinary Meetings (MDM) aims: 2) Stop treatments outside accepted standards
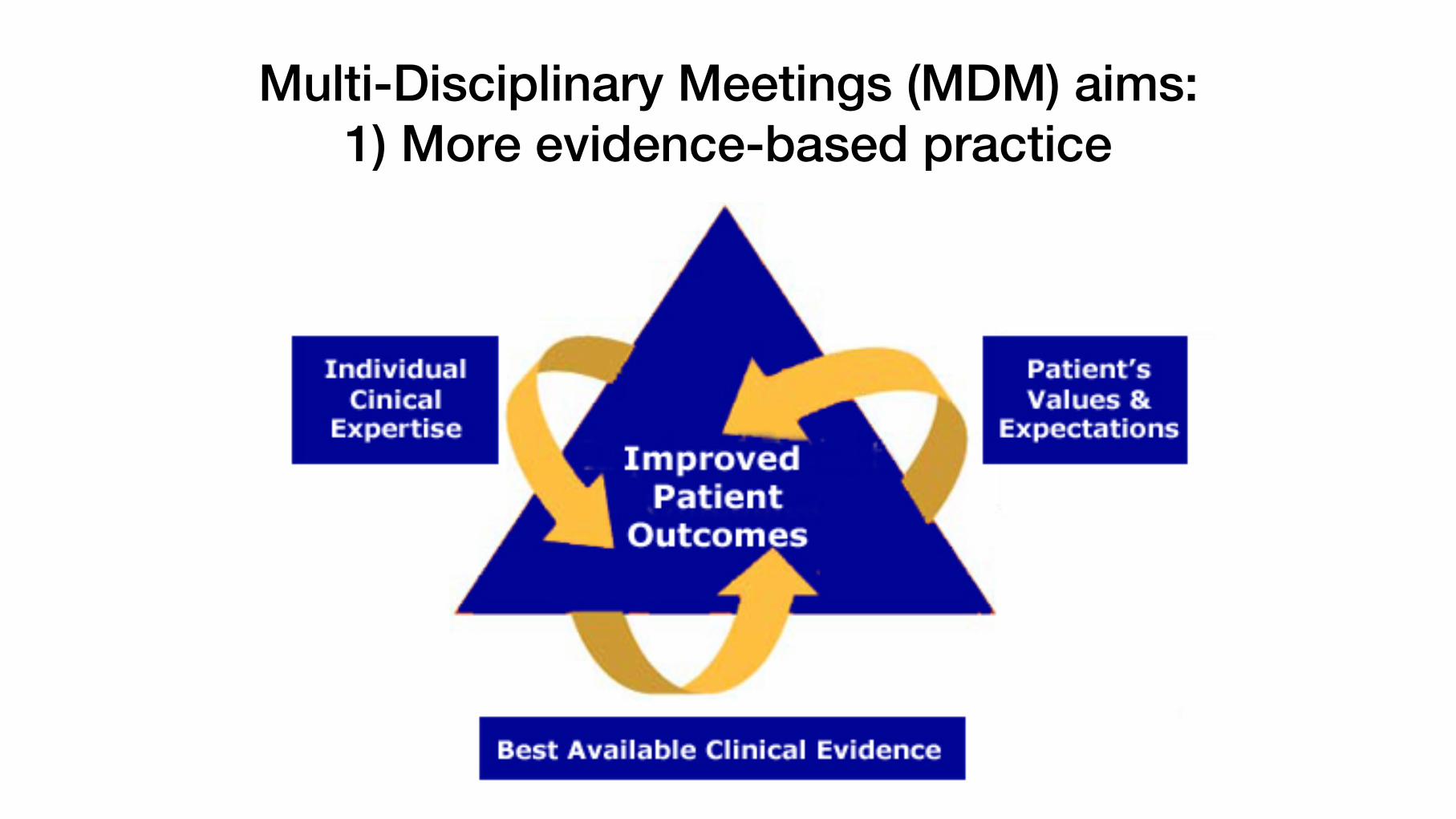
MDMs evolve into treatment-decision making meeting (MDTM) at key points in patient journey

MDTM = forum for multi-disciplinary/professional advice & input on a patient’s management
Investigations Treatment
Follow up Ethical & social matters
Comorbidities
Practical problems

MDTM challenges
Too many patients Not enough time to discuss each patient
Missing information Too many meetings

MDTM transformation to be more effective

Public Health England guidance on PSA testing in asymptomatic men
Prostate Cancer Risk Management Programme, Public Health England 2016

Risk categorisation&
management options

Public Health England (& PCUK) advisedPSA threshold: 3 mcg/L, age 50 to 70
Threshold PSA: Over 50 years > 3 mcg/L45–50 > 2.5 mcg/L

Online calculator to predict chance of prostate cancer on systematic transrectal biopsy
http://www.prostatecancer-riskcalculator.com/seven-prostate-cancer-risk-calculators

mpMRI & mapping biopsies find more significant cancer compared to TRUS biopsy, so online
calculators underestimate risk
Reference standard
40% 37%
19% 0%
25%
50%
75%
100%
Transperineal mapping biopsy mpMRI +ve TRUS biopsy +ve
% o
f men
with
sig
nific
ant c
ance
r Significant

PSA>3or>2.5
(black/hardprostate/strongFH
Suspicionscore4,5
Suspicionscore1,2
Targeted±systematicprostate
biopsies
PSAmonitoring
PSAsurveillance/systematicbiopsies
No mpMRI
Suspicionscore3
50%
25%
25%
PSA density threshold = 0.15 ng/mL/cc
mpMRI
Based on PI-RADS score, go for biopsy

MRI-targeted biopsies very precise – hit the target accurately
1 Match axial T2/DCE MRI & USS
3 Biopsy on longitudinal2 Direct needle to correct location
4 Check on axial that in correct position

3 4 5
Pathologist examines slides & grades tumour severity by Gleason score
Gleason patterns
• Gleason score is sum of two Gleason patterns (a.k.a. grade)
• Two most common architectural patterns chosen

Targeted biopsies find greater amount & higher grade cancer compared with TRUS biopsies à more categorised as higher risk
4 MRI-targetedbiopsy cores
TRUS12 biopsy cores
Clinically significant (higher Gleason grade) 74% 24%
Proportion of +ve cores 44% 11%
Maximum cancer length on biopsy (MCL) 8 mm 4 mm
MRI-targeted biopsies lead to perceived prostate cancer risk inflation
Robertson 2014 Eur UrolMesko 2016 Am J Oncol

Risk classification after MRI-targeted & mapping transperineal prostate biopsies:
Gleason score & maximum cancer length
No treatment
Active surveillance
Treatment possibly
Treatment advisable
Treatment options are broad & unclear
?

Patient preferences can guide choices

Years after diagnosis
Dead from prostate cancer
Dead from other
causes
Active surveillance: 4% chance of dying after 10 y for low-risk disease in PSA era in 65 year old
Contains Gleason pattern 3 only
1 2 3 4 5
|Cuzick 2006 B J CancerAlbertsen 2007 J UrolLu-Yao 2009 JAMA

Prostatectomy more likely
Retention of urine
Urinary symptoms
Erectile dysfunctionInflammatory bowel diseaseYounger age

Radiotherapy more likely
ComorbidityScarred abdomen
Older man Short urethral length

Brachytherapy more likely
Low risk disease
Potent
Short urethral length

Focal therapy more likely
Base Mid Apex
Posterior tumours away from sphincter
Sphincter
Potent

Case 1

• 59 year old
• PSA 4.4 ng/ml• Gland volume = 30.5 ml• MRI: 10×5 mm high probability lesion at the right base PZ,
sector 2p• Pathology:
• Target cores: Right base 2/3 cores Gl 4 + 3 = 7. 50%, max core length 8 mm
• Systematic cores: Right apex 2/3 cores 3 + 3 = 6, 12%
• Systematic cores: Right base 3/3 cores 3 + 4 = 7, 25%

MRI-targeted biopsies: 4 + 3 = 7 (grade group 3)& systematic biopsies: 3 + 4 = 7 (grade group 2)
Base

What risk: low or high?
UCL definition: significant cancer
NCCN definition: unfavourable intermediate risk
SignificantTable shows NCCN risk groups for clinically localised
prostate cancer
CAPRA score: 7 (high risk)

Unfavourable intermediate risk disease requires treatment in most cases
AUA, ASTRO,
SUO 2017
guideline
Case 2
Patient on active surveillance
• Presented 2012
• Age 66 y, PSA 3.5 mcg/mL benign feeling prostate,
• Caucasian, ASA I, WHO PS 0, no FH of PCa
• Sexually active & minimal LUTS
• PMH
§ 2007 -ve transrectal prostate biopsies PSA 2.7, benign
§ 2005 low-risk, Non-Muscle Invasive Bladder Cancer (NMIBC)
§ 2007 BPH & GreenLight laser prostate ablation
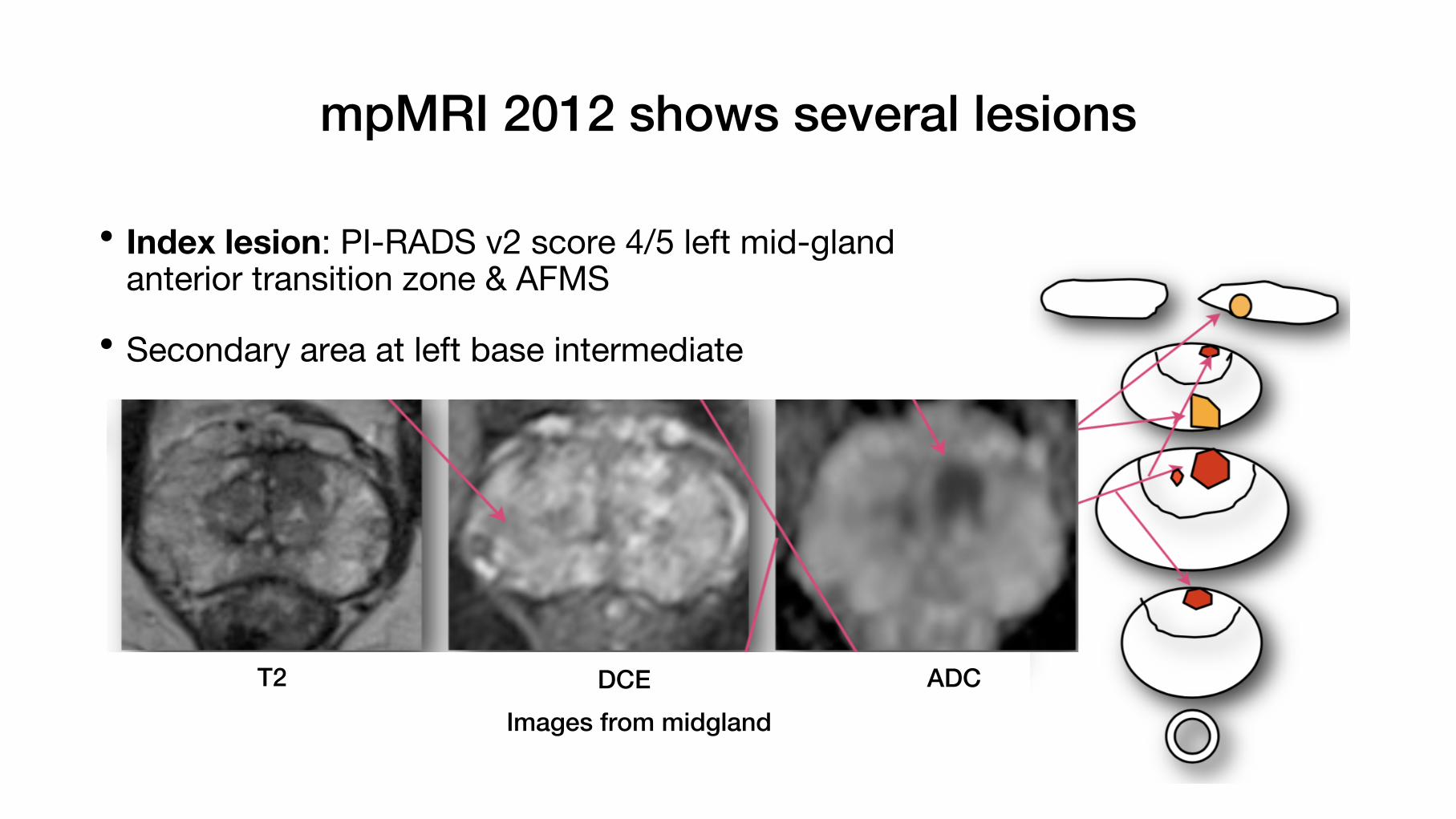
mpMRI 2012 shows several lesions
• Index lesion: PI-RADS v2 score 4/5 left mid-gland anterior transition zone & AFMS
• Secondary area at left base intermediate
T2 DCE ADCImages from midgland

MRI-targeted transperineal biopsies showed Gleason Score 3 + 3 = 6, MCCL 14 mm
Gleason score 3 + 3 = 6, 14 mm, grade group 1
T2
DCE
ADC

What risk: low or high?
SignificantTable shows NCCN risk groups for clinically localisedprostate cancer
UCL definition: significant cancer
NCCN definition: low risk
CAPRA score: 2 (low risk)

Low risk disease: AS or whole gland radical treatment
AUA, ASTRO,
SUO 2017
guideline

Biomarkers add more information to pathology results
Cell cycle progression score: proportional to chance of dying
Dea
ths
from
pro
stat
e ca
ncer
Years from diagnosis
Low score
High score
10
30%
0
Prolaris: Cell Cycle Progression (CCP) Score
Low Prolaris
Bostrom 2015 Eur Urol
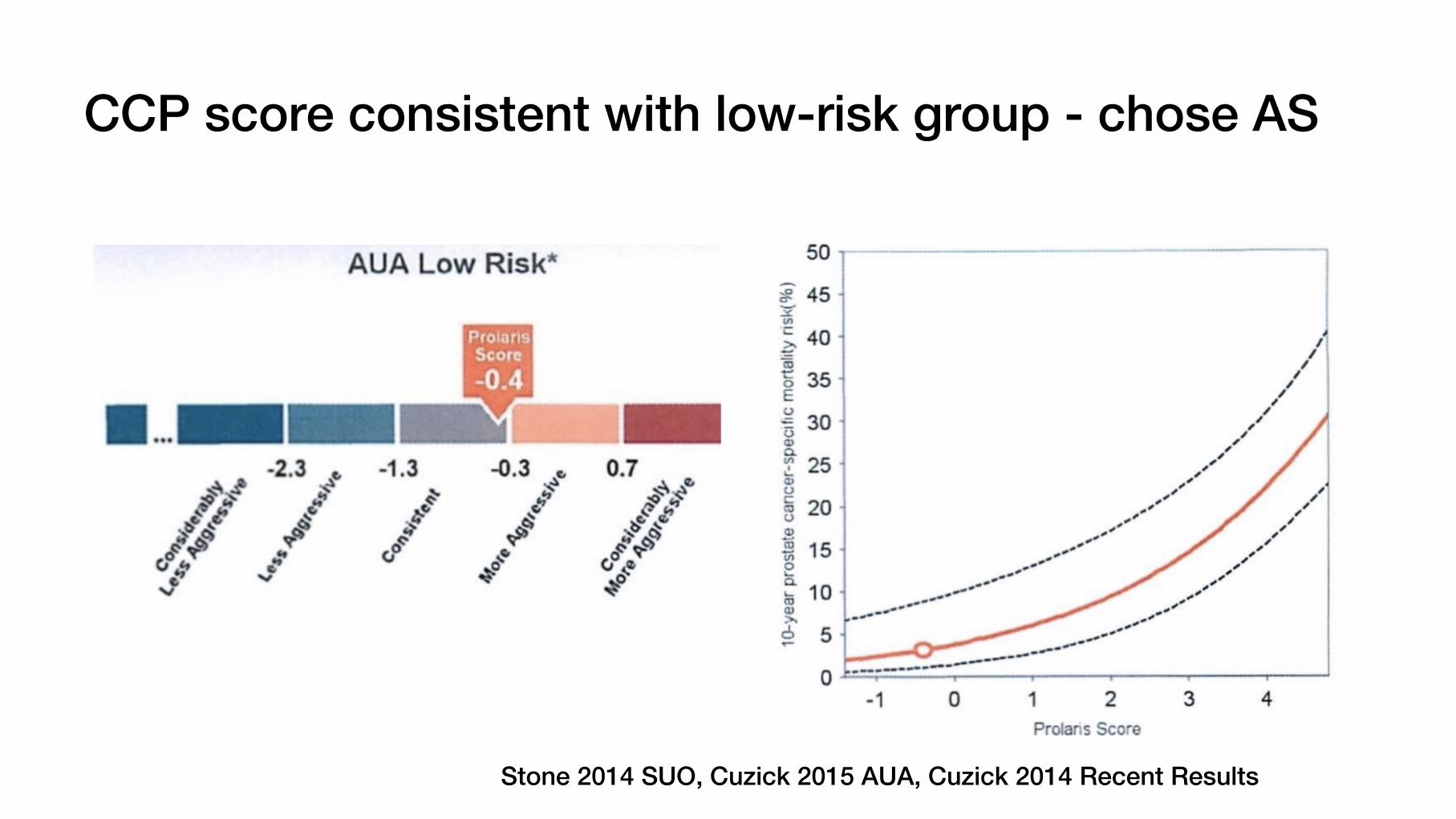
CCP score consistent with low-risk group - chose AS
Stone 2014 SUO, Cuzick 2015 AUA, Cuzick 2014 Recent Results

PSA values rising slowly over time

2017 (age 72): PSA 5.6, 10% free PSA, PSA density 0.13 ng/mL/cc
MRI shows enlarging anterior lesion
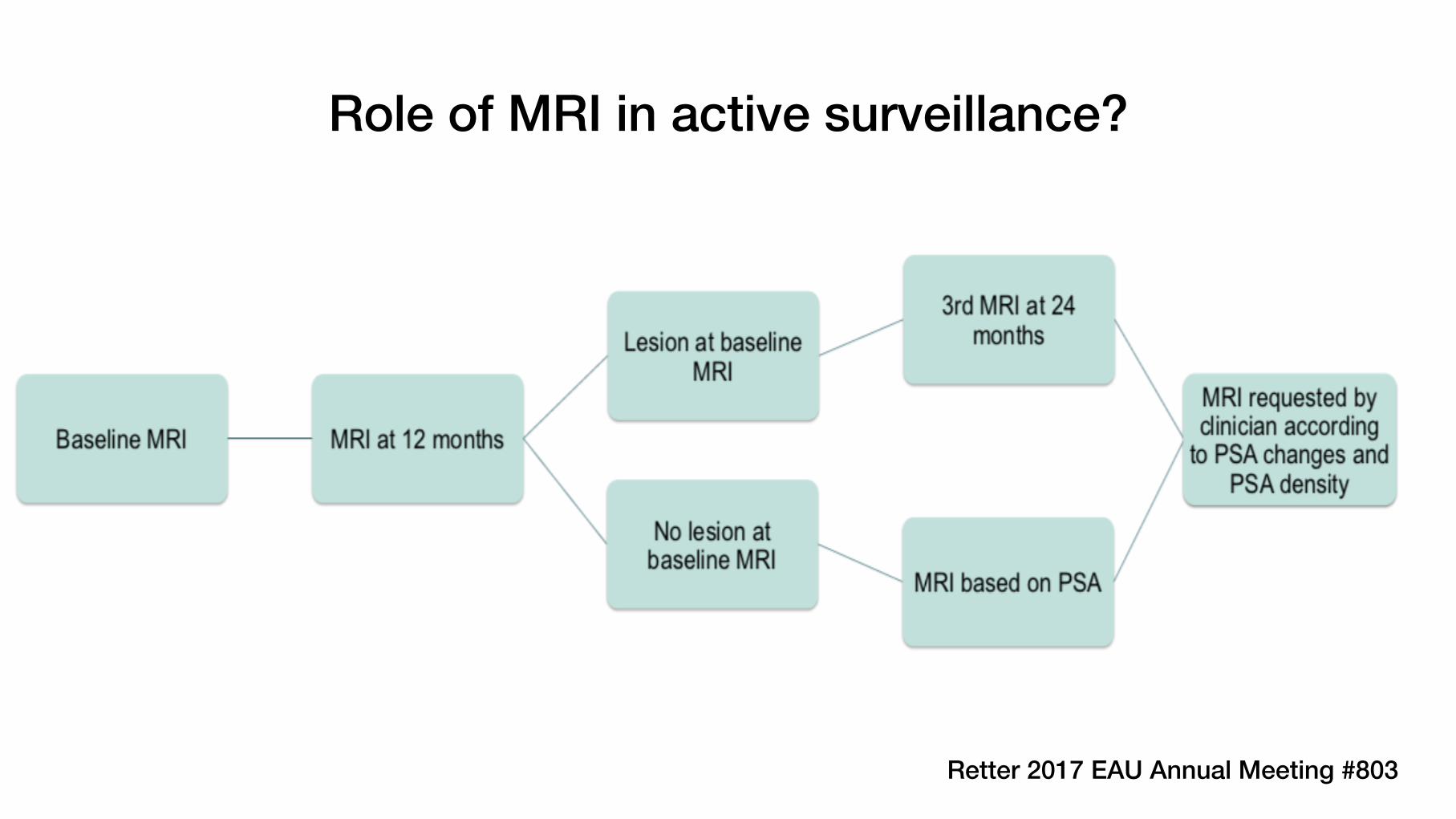
Role of MRI in active surveillance?
Retter 2017 EAU Annual Meeting #803

Case 3
• 79 year old
• Presenting PSA 10.98 ng/ml
• Gleason 4 + 3 left base PZ
• Underwent HIFU focal therapy 18 months ago
• Current PSA stable at 1.43 ng/ml
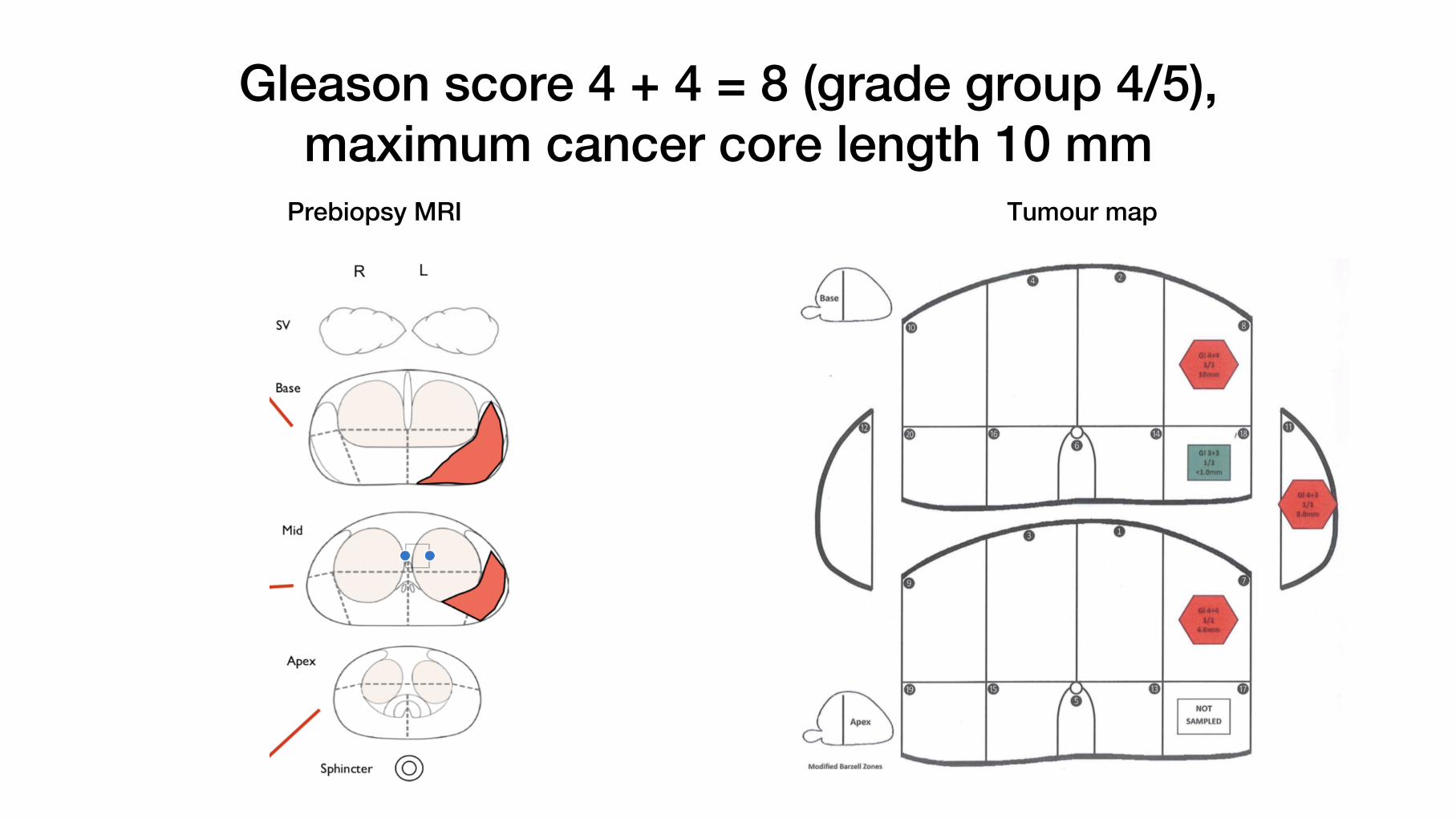
Gleason score 4 + 4 = 8 (grade group 4/5),maximum cancer core length 10 mm
Prebiopsy MRI Tumour map

What risk: low or high?
NCCN definition: high risk
SignificantTable shows NCCN risk groups for clinically localised
prostate cancer
CAPRA score: 6 (high risk) UCL definition: significant cancer

High risk disease requires treatment in most cases even in older men
AUA, ASTRO,
SUO 2017
guideline
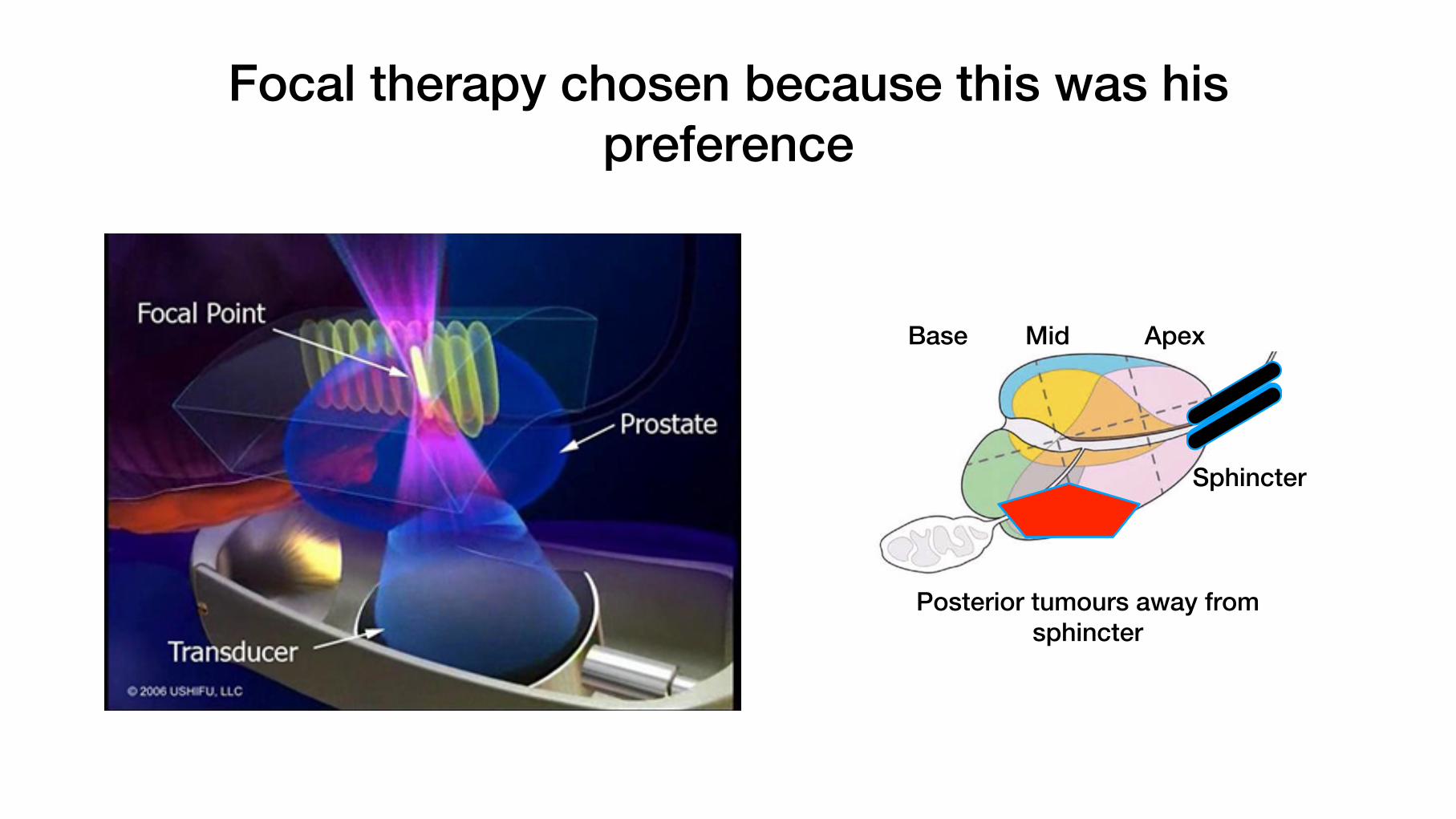
Focal therapy chosen because this was his preference
Base Mid Apex
Posterior tumours away from sphincter
Sphincter
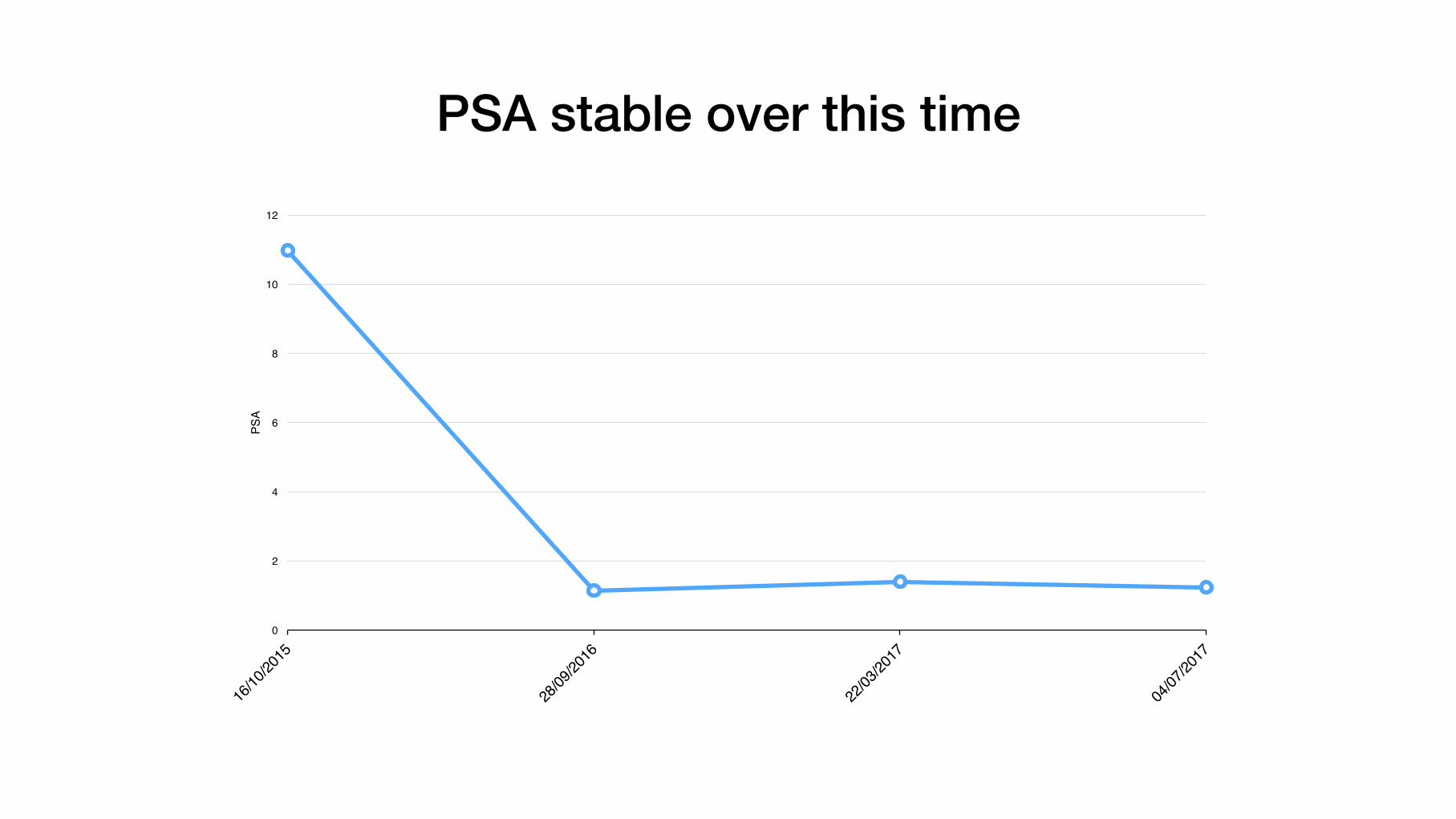
PSA stable over this time
0
2
4
6
8
10
12
PSA

1 week post focal HIFU MRI DCE shows the area treated
UnaffectedNeurovascular
bundle
Ablated cancer
Nerve bundle

Subtypes of FT: How focal?
• Hemi-ablation:treathalfthegland• Focal/zonal:treat≥2lesionsin1areaofthegland• Targeted/Indexlesion:treatthelargesttumour

• 1–2 weeks: ↑ in gland size • Reactive oedema and inflammation
• Amount depends on “focality” of treatment
• 3+ months: ↓ in gland size • Coagulative necrosis replaced with fibrosis
• Capsular retraction, scarring
Post treatment findings

Post treatment scarring/atrophyBaseline
4 months

Case 4

• 67 year old. PSA 9.6 ng/ml
• AP resection for ulcerative colitis 1981
• HoLEP in 2012 – benign histology
• Diagnostic problem – no rectal access
• Cannot perform DRE
• Cannot perform TRUS biopsy
• Cannot perform Transperineal US/MRI fused biopsy

Approaches adopted
• US-guided TP biopsyPCa in 7/7 with MRI Likert score 4–5 (1 case GS 6; 6 cases GS ≥7). 2 score 3 and 2 negative = no cancer
• MRI assisted CT-guided transgluteal2/2 case
• Other approachesUS: transperineal, transabdominal, or transurethralMRI: transgluteal