Embed Size (px)
Citation preview
Preventing Diabetes and Obesity in Patients with Mental HealthPROFESSOR STEVEN C. BOYAGESTHE UNIVERSITY OF SYDNEY, TUESDAY 18 T H OCTOBER 2016WORLD FEDERATION FOR MENTAL HEALTH INTERNATIONAL CONFERENCE, CAIRNS AUSTRALIA
Outline 1. What is diabetes and its relation to obesity (prediabetes and metabolic syndrome)
2. Diabetes and Mental Health Co-Morbidity
3. Treatment of MH disorders may increase the incidence of diabetes and metabolic disorders
4. Premature vascular disease is the biggest killer of patients with MH
5. Treatment of other vascular risk factors is essential
6. Prevention and early identification of diabetes and metabolic syndrome is the key
Diabetes and Mental Health Co-Morbidity
1. Depression, anxiety disorders, dementia, schizophrenia, and bipolar disorder (BD) occur more commonly in DM patients.
2. DM may be involved in the development of the first three conditions. The exact mechanism by which DM may be linked to these conditions is not fully understood.
3. There appears to be a bidirectional relationship between DM and depression.
4. About 7% of DM cases are thought to be attributed to depression.
5. Depression is associated with a 60% to 65% increased risk of DM
6. DM appears to double the risk of dementia
Other risk factors Smoking Hypertension Hyperuricemia Hyperlipidemia Sleep apnea Drug induced diabetes
Male Gender Genetic factors
Leading cause of death is vascular disease
1. Despite the increased risk of suicide in psychiatric patients, the leading cause of death in patients with schizophrenia or BD is cardiovascular disease (CVD).
2. This is especially true in younger patients, with the risk of CVD and stroke more than two to three times greater than in a nonpsychiatric population.
3. MetS occurs in 37% to 63% of schizophrenia patients and in 30% to 49% of BD patients.
4. Psychotropic medications used for managing mental illness can contribute to the development of MetS.
Drug induced obesity and diabetes
Atypical antipyschotics (AA)Among AAs, clozapine and olanzapine are associated with the greatest weight gainQuetiapine and risperidone with intermediate weight gainAripiprazole, paliperidone, and ziprasidone with the least weight gain
Possible mechanisms for psychotropic-related WG include WG secondary to improved mood/affect; increased food cravings; alterations in resting metabolic state; sedation; increased cellular lipogenesis; and changes in neurotransmitters (e.g., 5-HT [serotonin] 1 and 2A/C receptor antagonism) and neuropeptides (e.g., leptin, ghrelin, cytokines such as TNF)
Diabetes
Prediabetes
Obesity/Metabolic Syndrome
Mechanism: Obesity is the result of long-term energy imbalance whereby energy intake surpasses expenditure
9
This imbalance may be caused by a variety of intrinsic and
extrinsic factors
Hill JO et al. Circulation. 2012;126(1):126–32
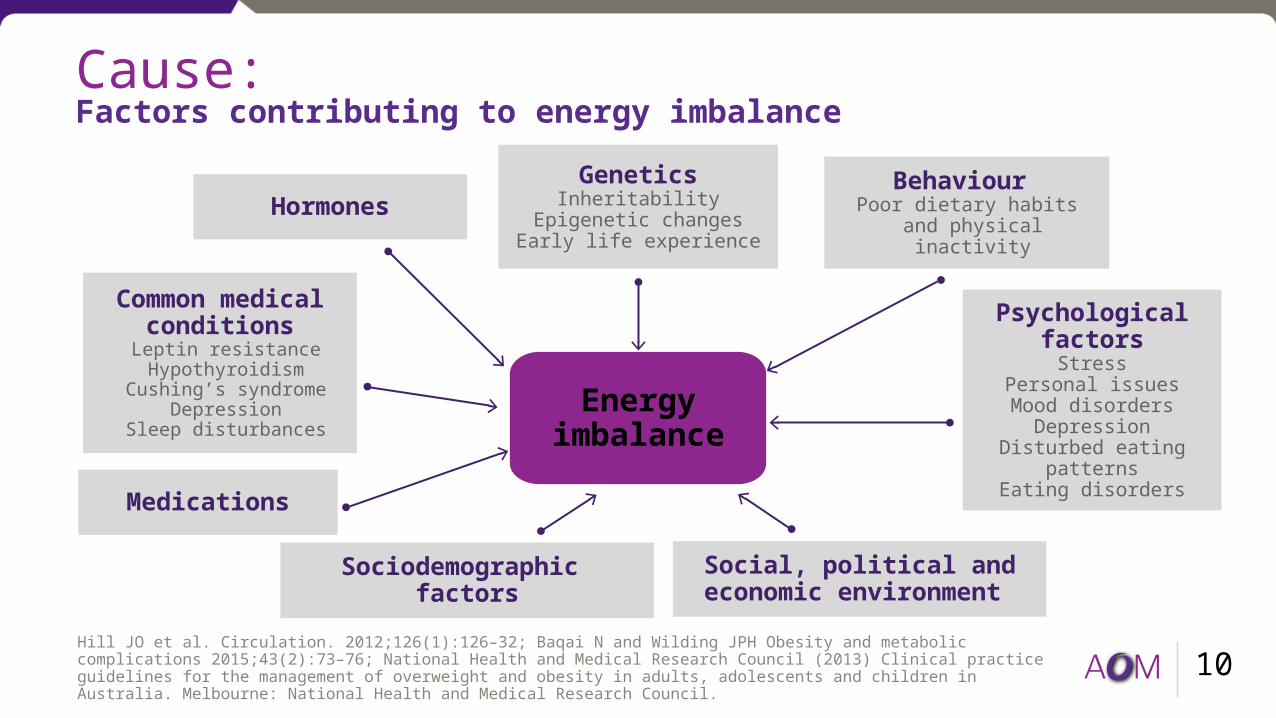
Cause: Factors contributing to energy imbalance
10
Energy imbalance
GeneticsInheritability
Epigenetic changesEarly life experience
Behaviour Poor dietary habits
and physical inactivity
Medications
Social, political and economic environment
Common medical conditionsLeptin resistanceHypothyroidism
Cushing’s syndromeDepression
Sleep disturbances
Hormones
Hill JO et al. Circulation. 2012;126(1):126–32; Baqai N and Wilding JPH Obesity and metabolic complications 2015;43(2):73–76; National Health and Medical Research Council (2013) Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia. Melbourne: National Health and Medical Research Council.
Psychological factors
StressPersonal issuesMood disorders
DepressionDisturbed eating
patternsEating disorders
Sociodemographic factors
11
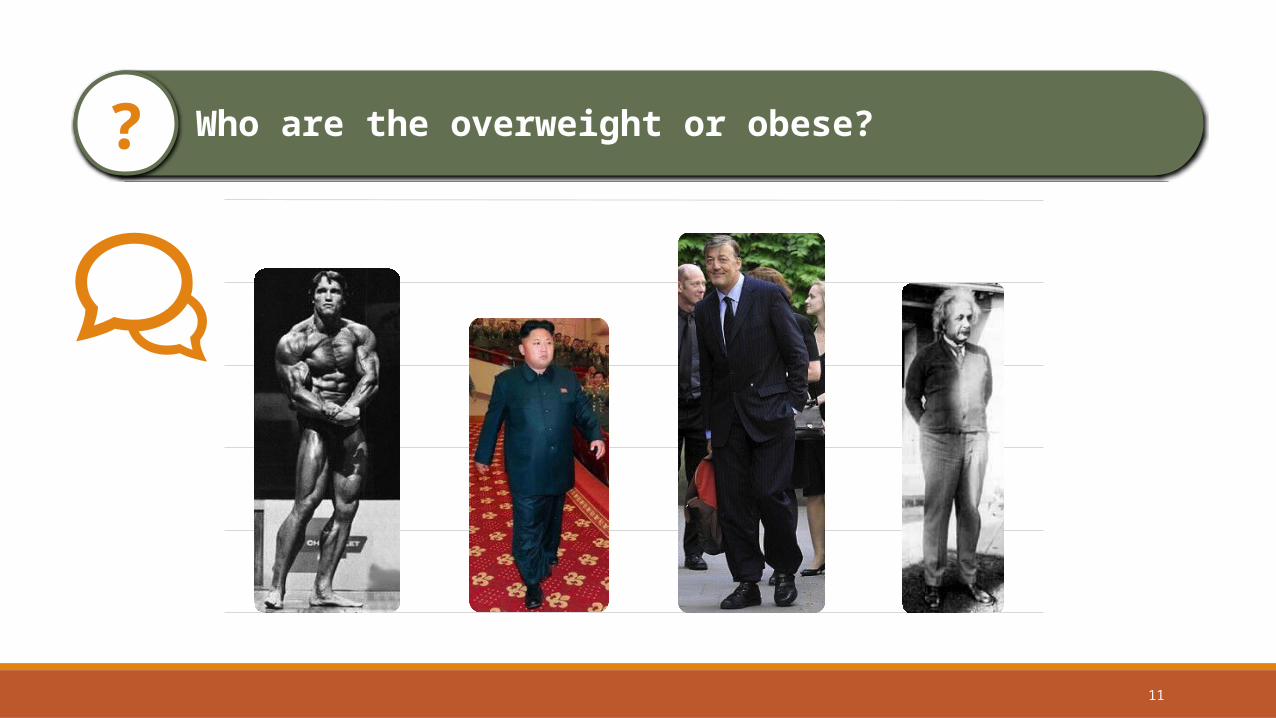
Who are the overweight or obese??
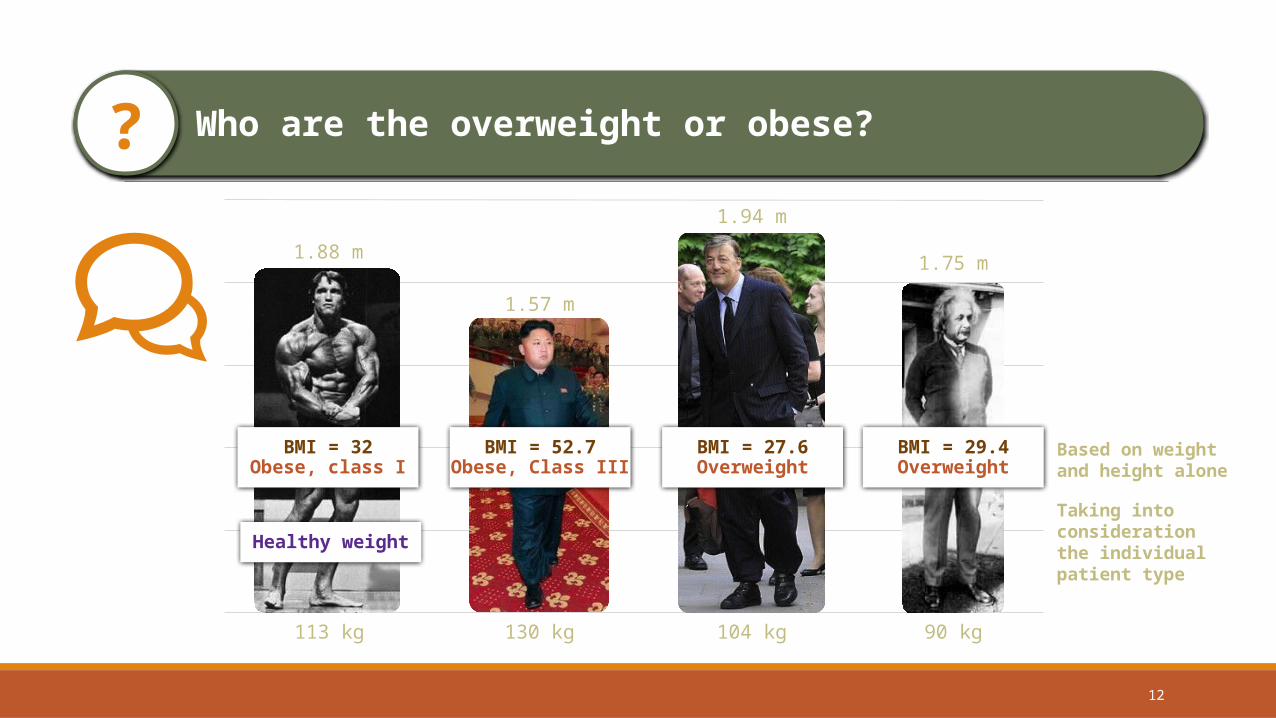
Who are the overweight or obese??
1.88 m
113 kg
BMI = 32Obese, class I
1.57 m
130 kg 90 kg
1.75 m
BMI = 29.4Overweight
BMI = 52.7Obese, Class III
Based on weight and height alone
Healthy weight
Taking into consideration the individual patient type
1.94 m
104 kg
BMI = 27.6Overweight
12
Obesity is defined by the World Health Organisation as abnormal or excessive fat accumulation that may impair health1
Definition and measure of obesity
13
1. WHO. Fact sheet 311. Updates January 2015. Available at www.who.int/. 2. National Health and Medical Research Council (2013) Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia. Melbourne: National Health and Medical Research Council.
Body Mass Index (BMI) provides the most convenient population-level measure of overweight and obesity1
Waist circumference is a good indicator of total body fat and a useful predictor of visceral fat2
Compared with BMI, waist circumference is a better predictor of cardiovascular risk, type 2 diabetes in women and metabolic syndrome2
14
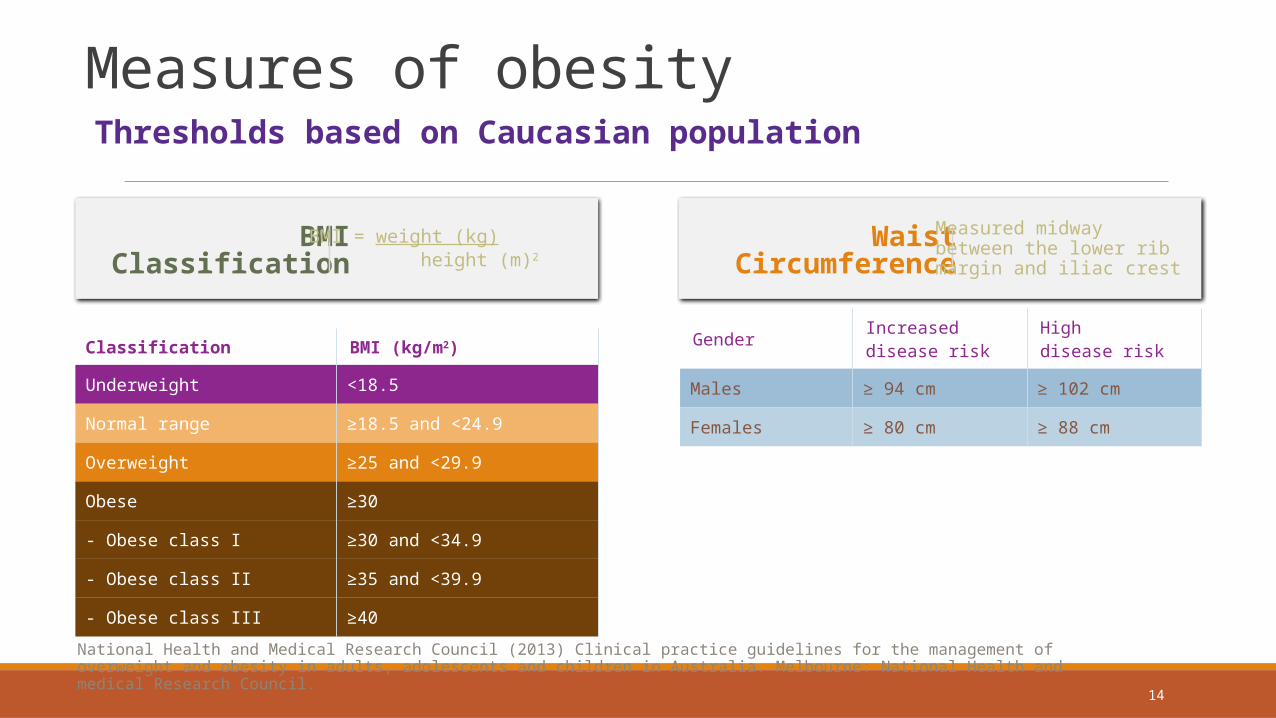
Measures of obesity Thresholds based on Caucasian population
Classification BMI (kg/m2)
Underweight <18.5
Normal range ≥18.5 and <24.9
Overweight ≥25 and <29.9
Obese ≥30
- Obese class I ≥30 and <34.9
- Obese class II ≥35 and <39.9
- Obese class III ≥40
Gender Increased disease risk
High disease risk
Males ≥ 94 cm ≥ 102 cm
Females ≥ 80 cm ≥ 88 cm
BMIClassification
WaistCircumference
Measured midwaybetween the lower ribmargin and iliac crest
BMI = weight (kg) height (m)2
National Health and Medical Research Council (2013) Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia. Melbourne: National Health and medical Research Council.
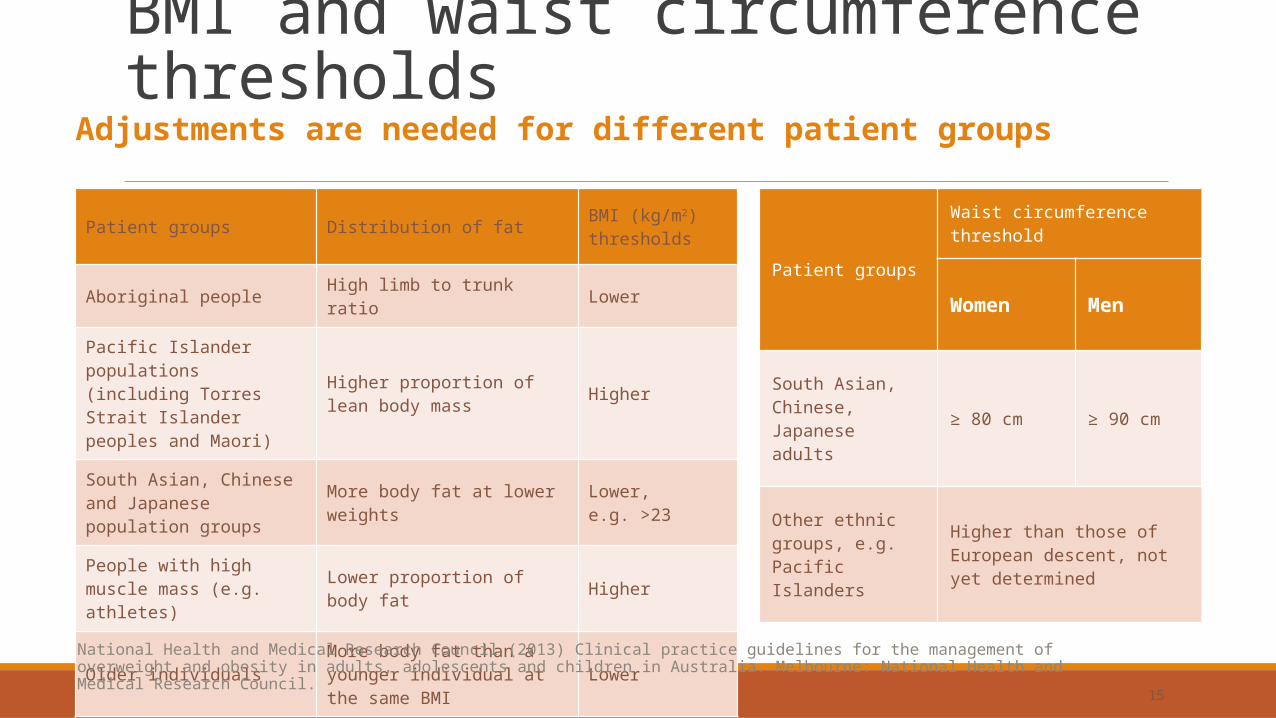
BMI and waist circumference thresholds
15
Patient groups
Waist circumference threshold
Women Men
South Asian, Chinese, Japanese adults ≥ 80 cm ≥ 90 cm
Other ethnic groups, e.g. Pacific Islanders
Higher than those of European descent, not yet determined
Patient groups Distribution of fat BMI (kg/m2) thresholds
Aboriginal people High limb to trunk ratio Lower
Pacific Islander populations (including Torres Strait Islander peoples and Maori)
Higher proportion of lean body mass Higher
South Asian, Chinese and Japanese population groups More body fat at lower weights Lower,
e.g. >23
People with high muscle mass (e.g. athletes) Lower proportion of body fat Higher
Older individuals More body fat than a younger individual at the same BMI Lower
Adjustments are needed for different patient groups
National Health and Medical Research Council (2013) Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia. Melbourne: National Health and Medical Research Council.
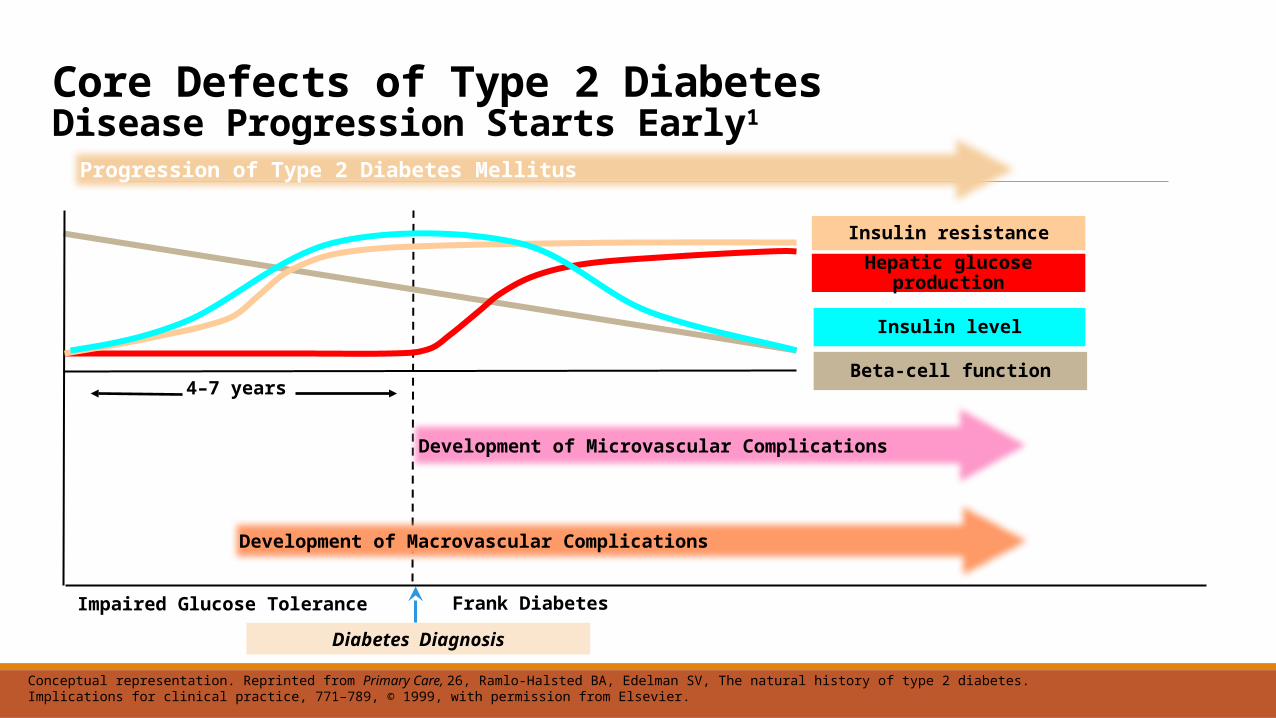
Core Defects of Type 2 DiabetesDisease Progression Starts Early1
Conceptual representation. Reprinted from Primary Care, 26, Ramlo-Halsted BA, Edelman SV, The natural history of type 2 diabetes. Implications for clinical practice, 771–789, © 1999, with permission from Elsevier.
Insulin level
Insulin resistanceHepatic glucose
production
Beta-cell function
Progression of Type 2 Diabetes Mellitus
Impaired Glucose Tolerance
Diabetes Diagnosis
Frank Diabetes
4–7 years
Development of Macrovascular Complications
Development of Microvascular Complications
Badman MK and Flier JS Science 2005;307:1909–14
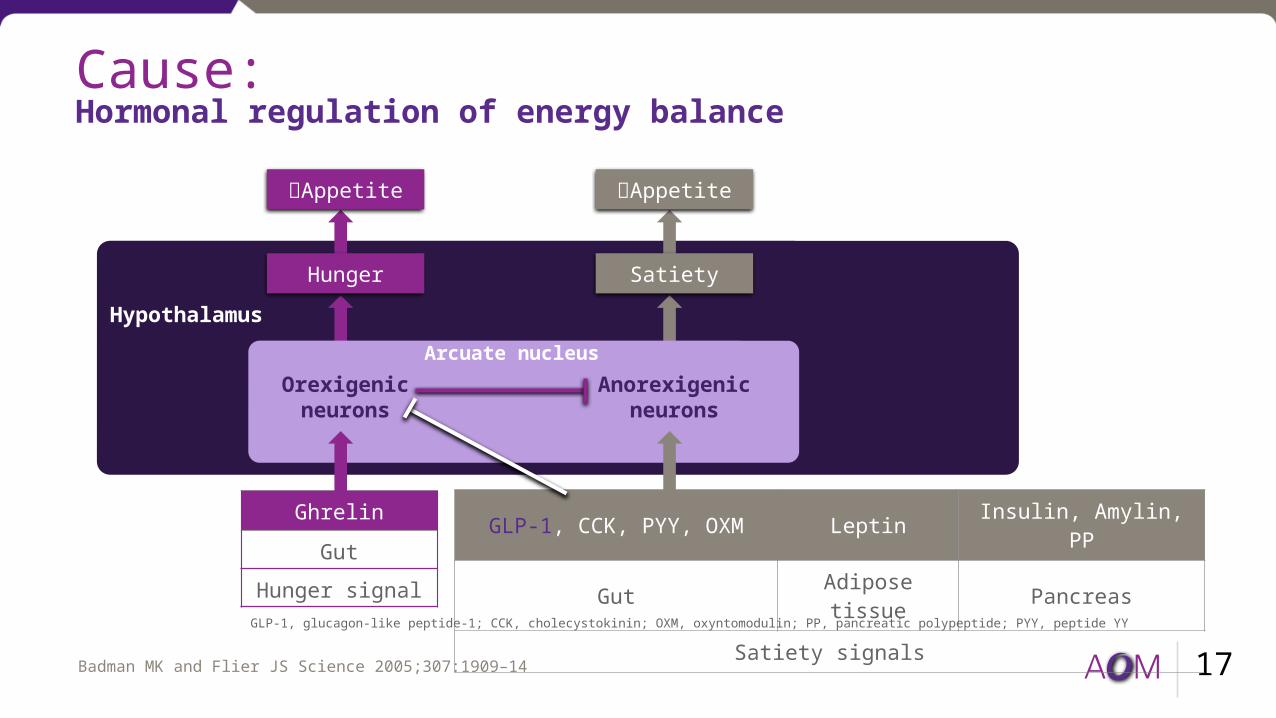
Cause: Hormonal regulation of energy balance
17
GLP-1, CCK, PYY, OXM Leptin Insulin, Amylin, PPGut Adipose tissue Pancreas
Satiety signals
Hypothalamus
GhrelinGut
Hunger signal
Anorexigenic neurons
Orexigenic neurons
GLP-1, glucagon-like peptide-1; CCK, cholecystokinin; OXM, oxyntomodulin; PP, pancreatic polypeptide; PYY, peptide YY
Appetite
Hunger
Appetite
Satiety
Arcuate nucleus
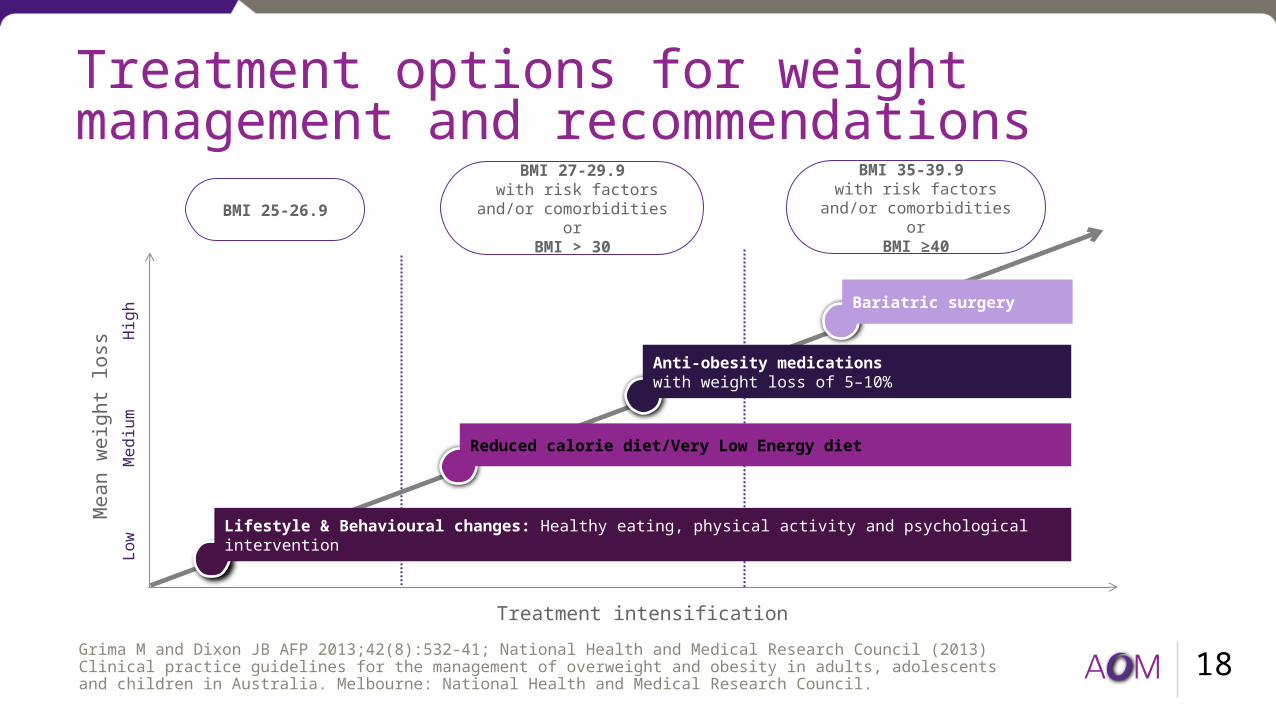
Treatment options for weight management and recommendations
18Treatment intensification
Low
Mea
n we
ight
loss
High
Med
ium
BMI 25-26.9BMI 27-29.9
with risk factors and/or comorbidities or
BMI > 30
Grima M and Dixon JB AFP 2013;42(8):532-41; National Health and Medical Research Council (2013) Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia. Melbourne: National Health and Medical Research Council.
Lifestyle & Behavioural changes: Healthy eating, physical activity and psychological intervention
Reduced calorie diet/Very Low Energy diet
Anti-obesity medications with weight loss of 5–10%
Bariatric surgery
BMI 35-39.9 with risk factors and/or
comorbidities orBMI ≥40
Prevention of Obesity and Diabetes: Principles
1. Record weight and other measures
2. Record degree of obesity
3. Check for diabetes and prediabetes and metabolic syndrome
4. Lifestyle advice, smartphone apps
5. Physical activity
6. Smoking cessation
7. Treat hypertension and lipids
8. Medication for obesity and diabetes
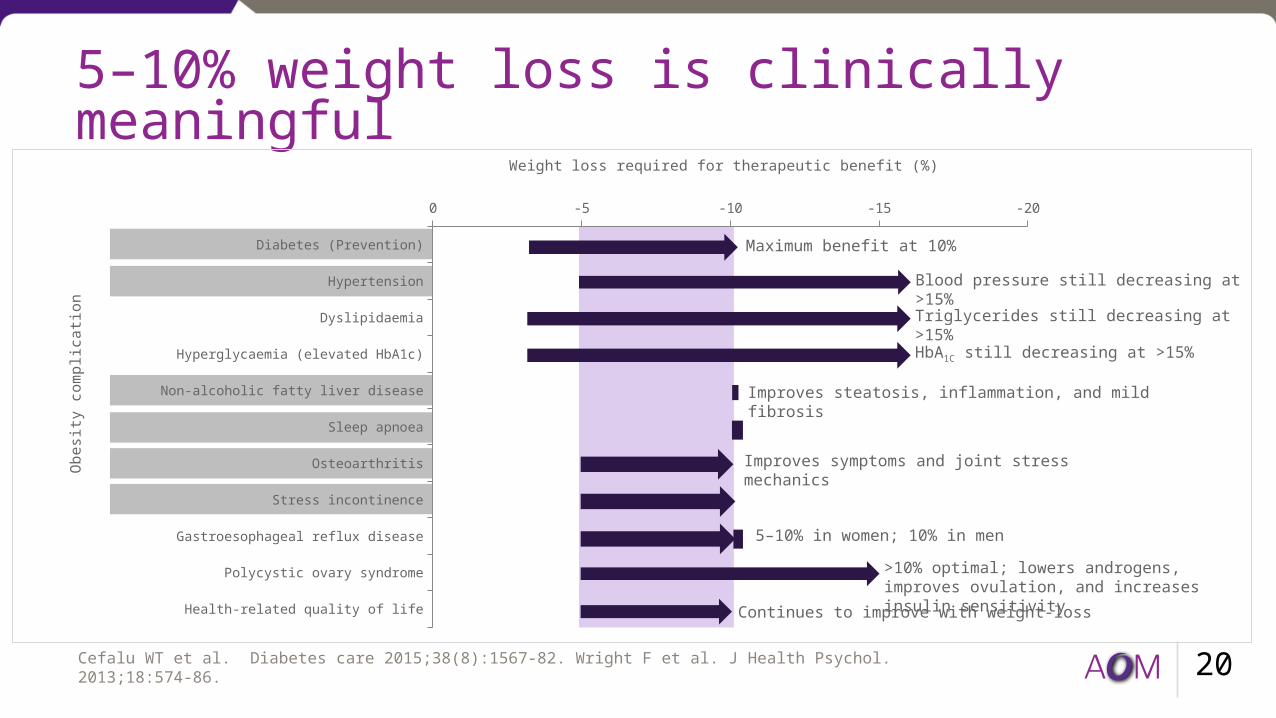
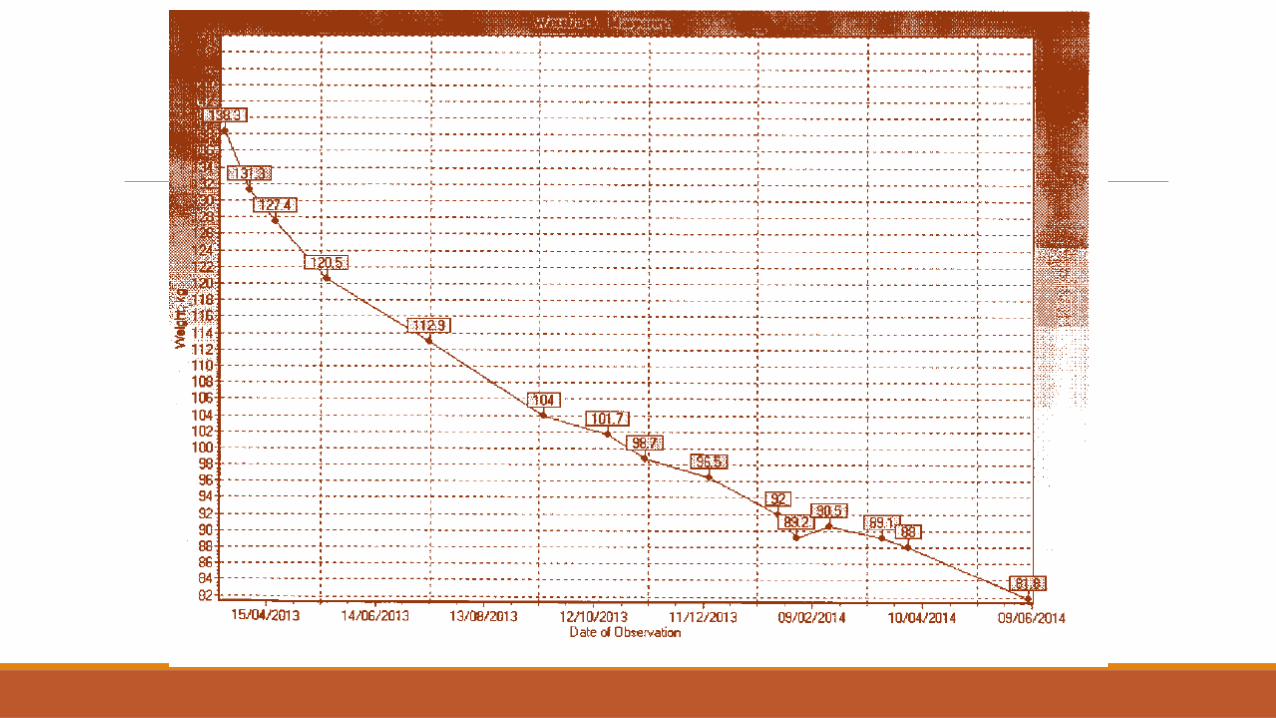
5–10% weight loss is clinically meaningful
20
Diabetes (Prevention)
Hypertension
Dyslipidaemia
Hyperglycaemia (elevated HbA1c)
Non-alcoholic fatty liver disease
Sleep apnoea
Osteoarthritis
Stress incontinence
Gastroesophageal reflux disease
Polycystic ovary syndrome
Health-related quality of life
-20-15-10-50
Weight loss required for therapeutic benefit (%)
Obes
ity c
ompl
icatio
n
Maximum benefit at 10%
Triglycerides still decreasing at >15%
HbA1C still decreasing at >15%
Improves steatosis, inflammation, and mild fibrosis
Improves symptoms and joint stress mechanics
5–10% in women; 10% in men>10% optimal; lowers androgens, improves ovulation, and increases insulin sensitivity
Continues to improve with weight-loss
Blood pressure still decreasing at >15%
Cefalu WT et al. Diabetes care 2015;38(8):1567-82. Wright F et al. J Health Psychol. 2013;18:574-86.
Approved anti-obesity medications in Australia
211. Duromine™ Approved Product Information, July 1991. 2. Metermine Approved Product Information, July 2004. 3. Xenical® Approved Product Information, April 2000
• Approved in 1991/ 2004• S4 • Private script• Sympathomimetic amine
Duromine™ / Metermine (Phentermine)1,2
• Approved in 2000• S3• Private script; available on the PBS under the Repatriation
Pharmaceutical Benefits Scheme• Potent, specific and reversible long acting inhibitor of
gastrointestinal lipases required for the systemic absorption of dietary triglycerides
Xenical® (Orlistat)3

New anti-obesity medication approved for weight management in Australia
22Saxenda® Approved Product Information, December 2015
• Approved December 2015• S4• Liraglutide is a human glucagon-like peptide (GLP-1)
analogue, with 97% amino acid sequence homology to endogenous human GLP-1
• Like endogenous GLP-1, liraglutide binds to and activates the GLP-1 receptor (GLP-1R)
• GLP-1 is a physiological regulator of appetite and calorie intake
Saxenda® (Liraglutide 3.0 mg)
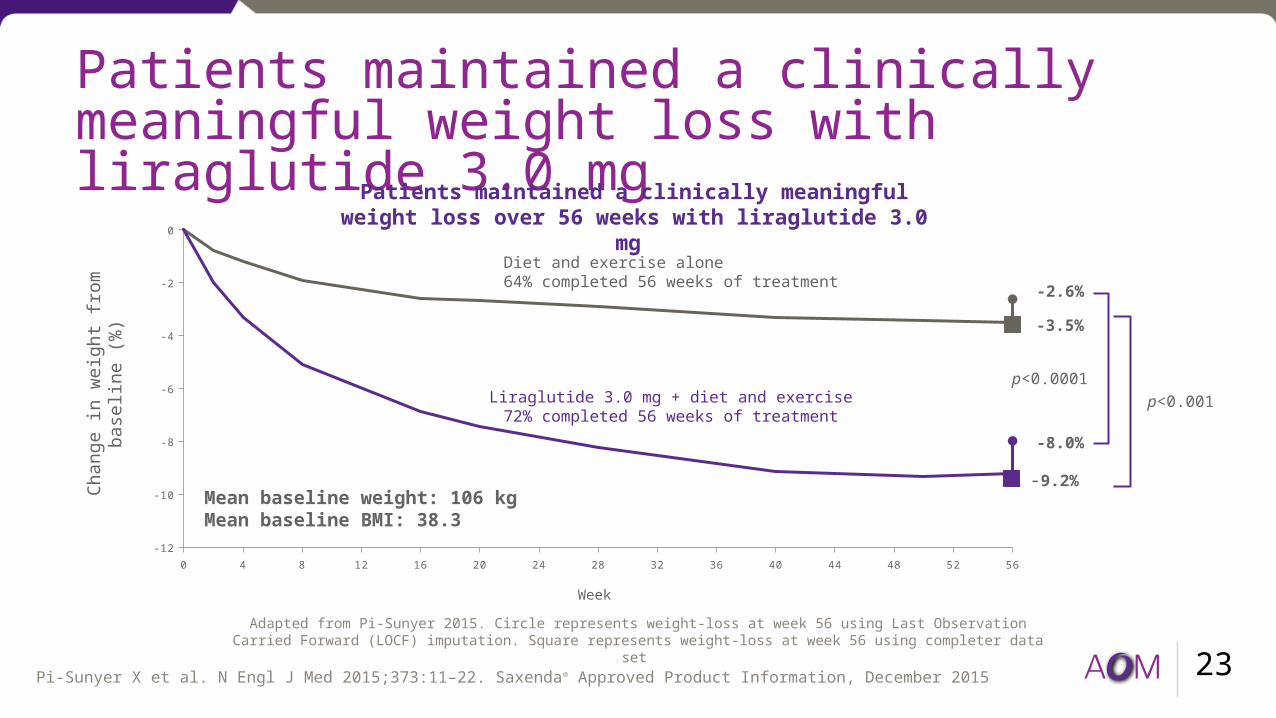
Patients maintained a clinically meaningful weight loss with liraglutide 3.0 mg
23
Week
Chan
ge in
wei
ght f
rom
ba
selin
e (%
)
p<0.0001
-8.0%
-2.6%
-9.2%
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56-12
-10
-8
-6
-4
-2
0
-3.5%
Liraglutide 3.0 mg + diet and exercise72% completed 56 weeks of treatment
Diet and exercise alone64% completed 56 weeks of treatment
p<0.001
Adapted from Pi-Sunyer 2015. Circle represents weight-loss at week 56 using Last Observation Carried Forward (LOCF) imputation. Square represents weight-loss at week 56 using completer data set
Patients maintained a clinically meaningful weight loss over 56 weeks with liraglutide 3.0 mg
Pi-Sunyer X et al. N Engl J Med 2015;373:11–22. Saxenda® Approved Product Information, December 2015
Mean baseline weight: 106 kgMean baseline BMI: 38.3
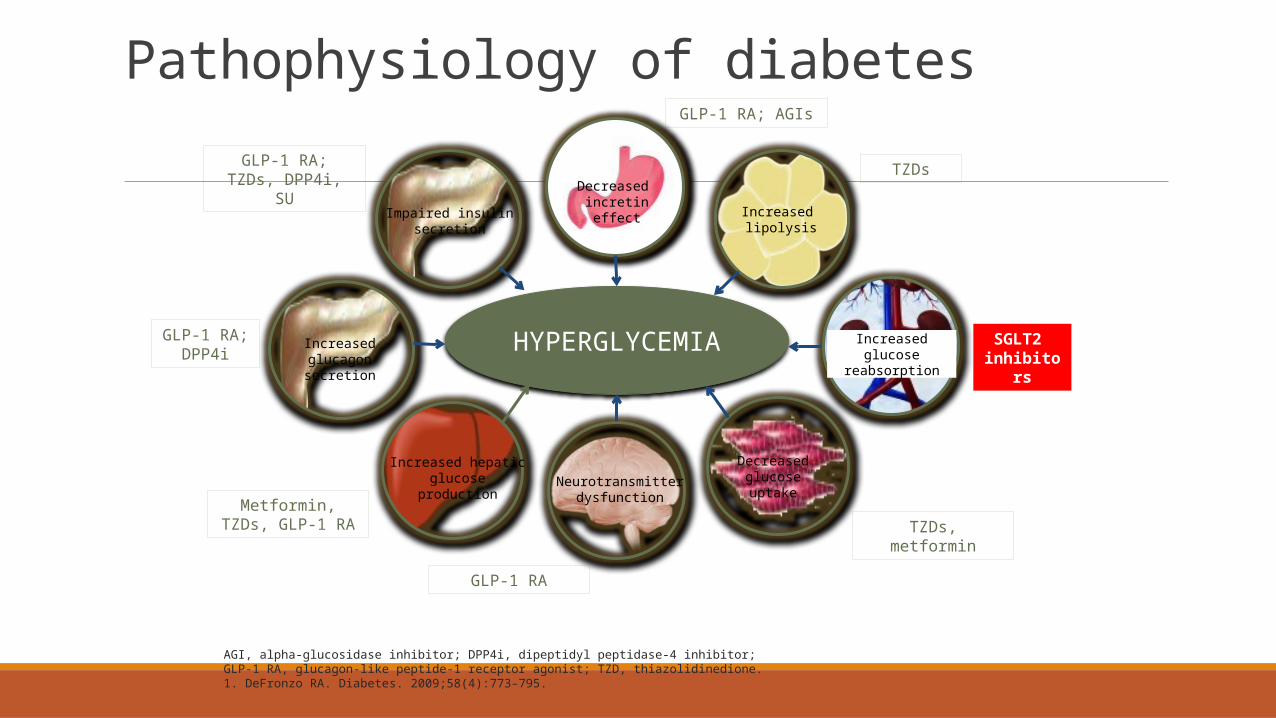
Pathophysiology of diabetes
HYPERGLYCEMIA
Decreased incretin effect Increased
lipolysis
Increased glucose reabsorption
Decreased glucose uptakeNeurotransmitter
dysfunction
Increased hepatic glucose production
Impaired insulin secretion
Increased glucagon secretion
SGLT2 inhibitor
s
TZDs
GLP-1 RA; AGIs
GLP-1 RA; TZDs, DPP4i, SU
GLP-1 RA; DPP4i
Metformin, TZDs, GLP-1 RA
GLP-1 RA
TZDs, metformin
AGI, alpha-glucosidase inhibitor; DPP4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; TZD, thiazolidinedione.1. DeFronzo RA. Diabetes. 2009;58(4):773–795.
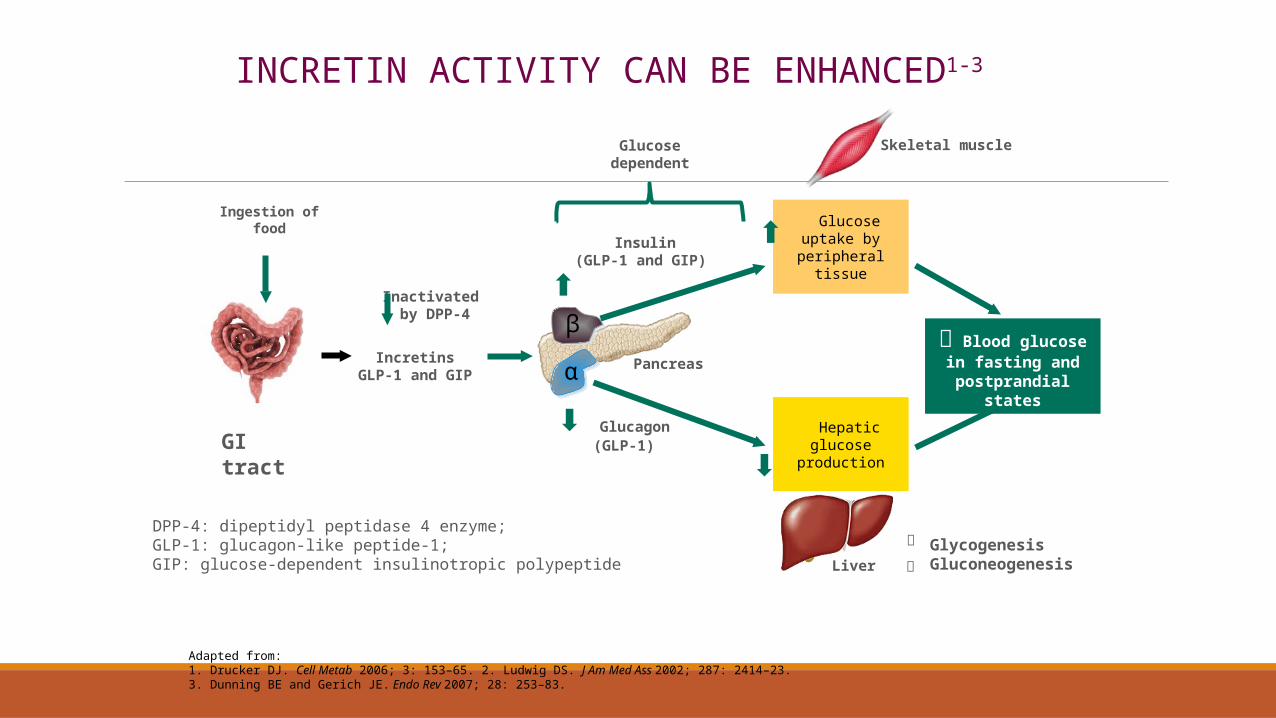
Inactivated by DPP-4
DPP-4: dipeptidyl peptidase 4 enzyme; GLP-1: glucagon-like peptide-1; GIP: glucose-dependent insulinotropic polypeptide
Glucagon(GLP-1)
Insulin(GLP-1 and GIP)
Glucose dependent
Pancreasα
β
Ingestion of food
GI tract Hepatic glucose production
Glucose uptake by peripheral
tissue
LiverGlycogenesisGluconeogenesis
IncretinsGLP-1 and GIP
Blood glucose in fasting and
postprandial states
Skeletal muscle
INCRETIN ACTIVITY CAN BE ENHANCED1-3
Adapted from: 1. Drucker DJ. Cell Metab 2006; 3: 153–65. 2. Ludwig DS. J Am Med Ass 2002; 287: 2414–23. 3. Dunning BE and Gerich JE. Endo Rev 2007; 28: 253–83.
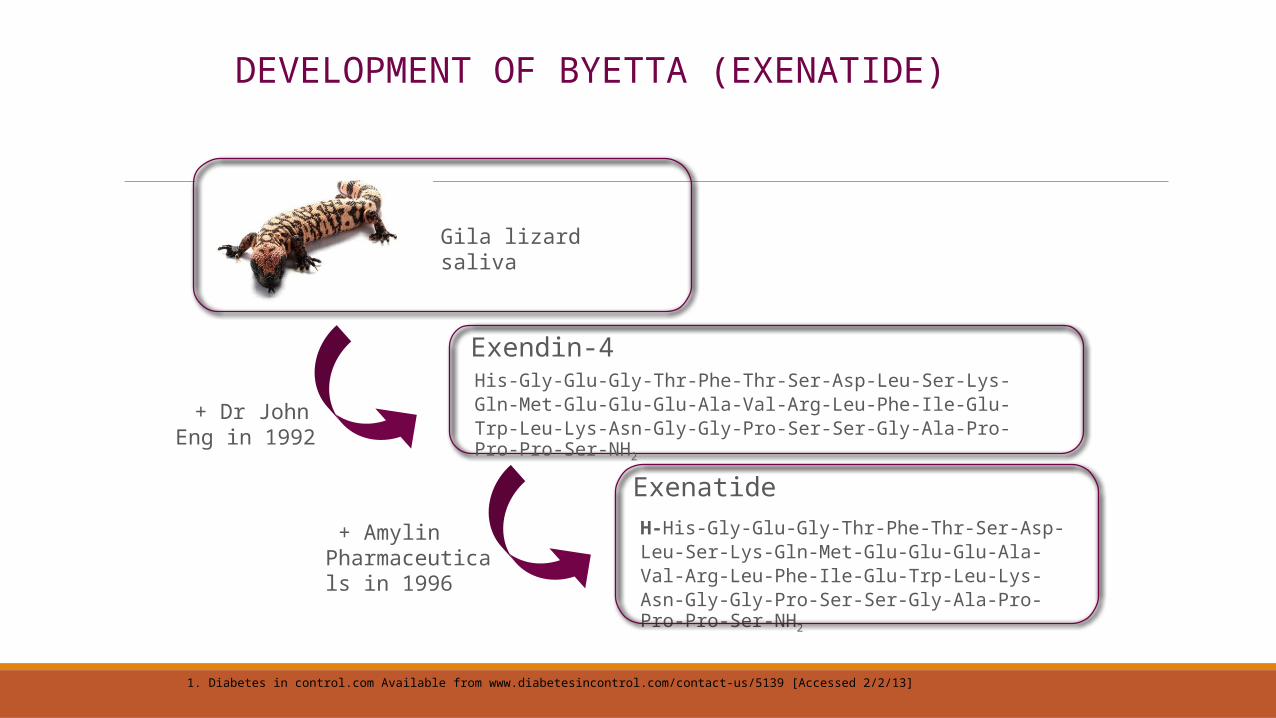
1. Diabetes in control.com Available from www.diabetesincontrol.com/contact-us/5139 [Accessed 2/2/13]
+ Dr John Eng in 1992
Exendin-4
Exenatide H-His-Gly-Glu-Gly-Thr-Phe-Thr-Ser-Asp-Leu-Ser-Lys-Gln-Met-Glu-Glu-Glu-Ala-Val-Arg-Leu-Phe-Ile-Glu-Trp-Leu-Lys-Asn-Gly-Gly-Pro-Ser-Ser-Gly-Ala-Pro-Pro-Pro-Ser-NH2
Gila lizard saliva
His-Gly-Glu-Gly-Thr-Phe-Thr-Ser-Asp-Leu-Ser-Lys-Gln-Met-Glu-Glu-Glu-Ala-Val-Arg-Leu-Phe-Ile-Glu-Trp-Leu-Lys-Asn-Gly-Gly-Pro-Ser-Ser-Gly-Ala-Pro-Pro-Pro-Ser-NH2
+ Amylin Pharmaceuticals in 1996
DEVELOPMENT OF BYETTA (EXENATIDE)

1. Klonoff DC et al. Curr Med Res Opin 2008; 24: 275–86. 2. Byetta Approved Product Information.
• Weight loss >1.5 kg per week has been observed in patients treated with exenatide2
• Weight loss of this rate may have harmful consequences2
†Secondary endpoint.1 *Byetta is not indicated as a weight reduction agent.2
BYETTA 10 μg BID PROVIDED LONG-TERM GLYCAEMIC CONTROL WITHOUT WEIGHT GAIN AND WITH WEIGHT LOSS OVER 156 WEEKS1*†
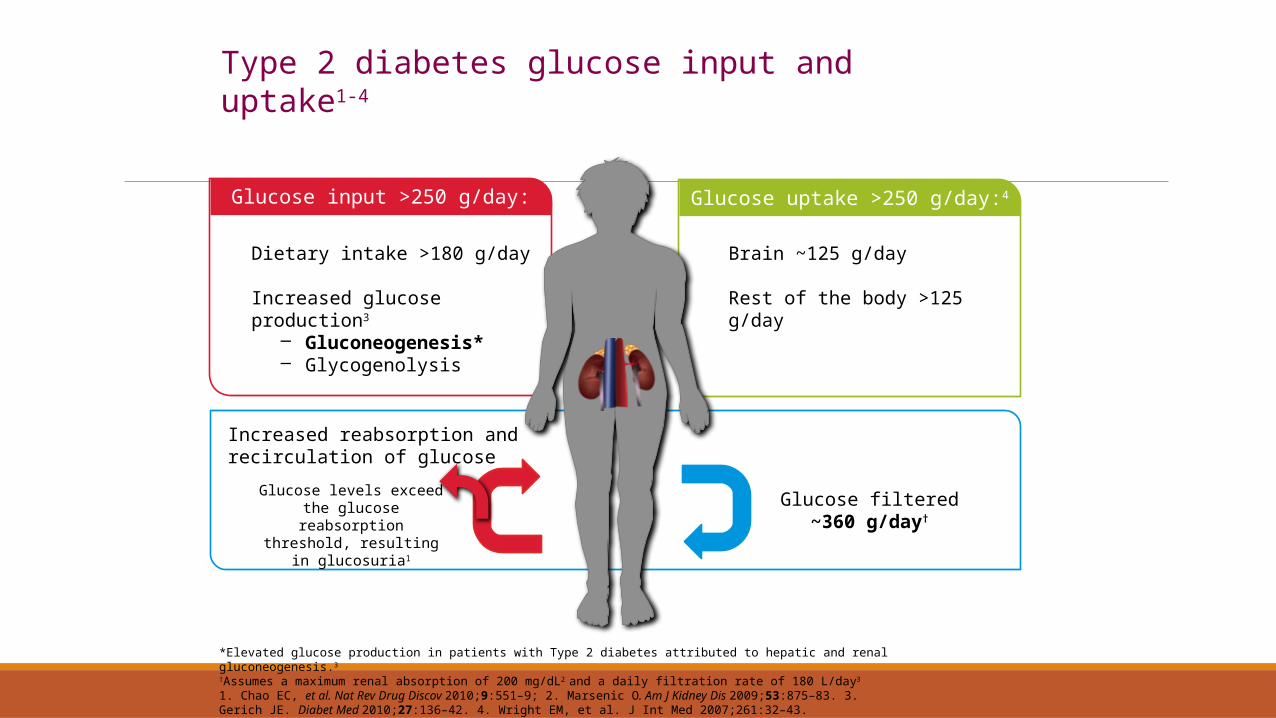
Glucose input >250 g/day: Glucose uptake >250 g/day:4
Dietary intake >180 g/day
Increased glucose production3
– Gluconeogenesis*– Glycogenolysis
Brain ~125 g/day
Rest of the body >125 g/day
Increased reabsorption and recirculation of glucose
Glucose filtered~360 g/day†
Glucose levels exceed the glucose reabsorption
threshold, resulting in glucosuria1
*Elevated glucose production in patients with Type 2 diabetes attributed to hepatic and renal gluconeogenesis.3†Assumes a maximum renal absorption of 200 mg/dL2 and a daily filtration rate of 180 L/day3
1. Chao EC, et al. Nat Rev Drug Discov 2010;9:551–9; 2. Marsenic O. Am J Kidney Dis 2009;53:875–83. 3. Gerich JE. Diabet Med 2010;27:136–42. 4. Wright EM, et al. J Int Med 2007;261:32–43.
Type 2 diabetes glucose input and uptake1-4
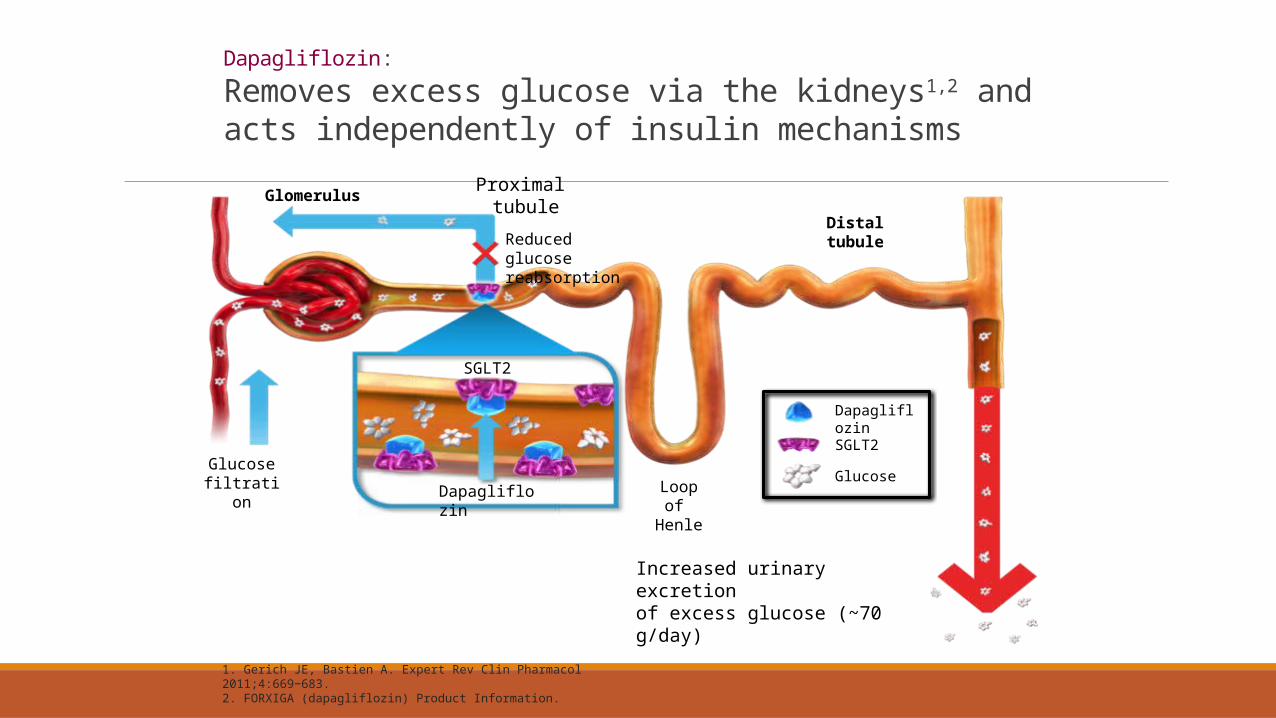
Dapagliflozin:Removes excess glucose via the kidneys1,2 and acts independently of insulin mechanisms
1. Gerich JE, Bastien A. Expert Rev Clin Pharmacol 2011;4:669−683. 2. FORXIGA (dapagliflozin) Product Information.
Increased urinary excretion of excess glucose (~70 g/day)
Glucose filtration
SGLT2
SGLT2
Dapagliflozin
Glucose
Dapagliflozin
Reduced glucose reabsorption
Distaltubule
Loop of Henle
Glomerulus Proximal tubule
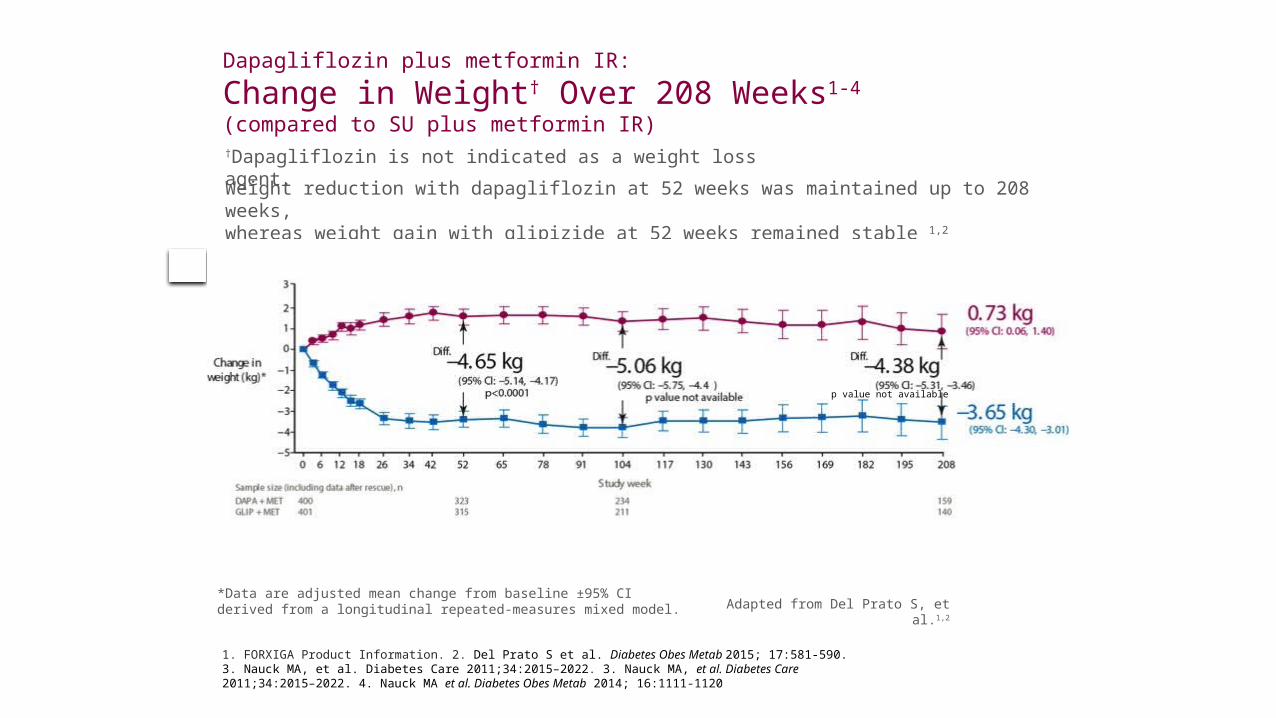
Dapagliflozin plus metformin IR: Change in Weight† Over 208 Weeks1-4(compared to SU plus metformin IR)
1. FORXIGA Product Information. 2. Del Prato S et al. Diabetes Obes Metab 2015; 17:581-590. 3. Nauck MA, et al. Diabetes Care 2011;34:2015–2022. 3. Nauck MA, et al. Diabetes Care 2011;34:2015–2022. 4. Nauck MA et al. Diabetes Obes Metab 2014; 16:1111-1120
*Data are adjusted mean change from baseline ±95% CI derived from a longitudinal repeated-measures mixed model.
Weight reduction with dapagliflozin at 52 weeks was maintained up to 208 weeks, whereas weight gain with glipizide at 52 weeks remained stable 1,2
Adapted from Del Prato S, et al.1,2
†Dapagliflozin is not indicated as a weight loss agent.
p value not available
Prevention of Obesity and Diabetes: Principles
1. Record weight and other measures
2. Record degree of obesity
3. Check for diabetes and prediabetes and metabolic syndrome
4. Lifestyle advice, smartphone apps
5. Physical activity
6. Smoking cessation
7. Treat hypertension and lipids
8. Medication for obesity and diabetes