Embed Size (px)
Citation preview


Dehydration in children overview
Infants and children are more likely to become dehydrated than adults because they weigh less and their bodies turn over water and electrolytes more quickly.
Dehydration in sick children is often a combination of refusing to eat or drink anything and losing fluid from vomiting, diarrhea, or fever.
Most dehydration is caused by viral infections that naturally run their course. The most dangerous problem with viruses is dehydration, which can kill infants and children.
In most cases, providing adequate fluid, either by mouth or via a drip, is all that is necessary to assure your child's complete recovery.

Dehydration pure (tissue) water loss and hypovolemia to sodium loss and thus loss of blood volume.
Loss of water from the extracellular fluid volume, vascular and interstitial fluids.
It is literally the removal of water or deficiency of fluid within an organism.
Extracellular Fluid Volume Deficit (ECFVD)
Intracellular fluid Volume Deficit (ICFVD)

Losses can be : 1. Mild – loss of 1 to 2 L of water (2% of body
weight is lost).2. Moderate – loss of 3 to 5 L of water (5% of
body weight is lost).3. Severe – loss of 5 to 10 L of water (8% of
body weight is lost).
Fluids are normally found in three spaces: Inside the cells (Intracellular) Around the cells (Interstitial) In the bloodstream (Intravascular)

Pathophysiology
Dehydration is seen when the normal compensation for fluid in the bloodstream cannot be corrected by stored fluid elsewhere. When fluids are lost from the intravascular spaces because of lack of intake or excess loss, interstitial fluids move in to restore vascular volume. Because the actual volume of fluid in the interstitial space limited, other compensation systems are initiated to restore fluid volume.
If the dehydration is not corrected, fluid is shifted from the cells into the vascular system.

Cellular Dehydration The loss of cellular fluid is dangerous because the
cells need fluid for cellular function. Intracellular fluid Volume Deficit (ICFVD) Less fluid is available for temperature regulation via
sweating, and lowered blood volume decreases the body’s ability to transport core heat to the periphery for conducive loss.
There is cerebrospinal fluid and less fluid in fat pads around the eyes. If cerebral cells become dehydrated, thought processes may be impaired.

Causes of dehydration in children
Common viral infections causing vomiting and diarrhea include rotavirus or winter vomiting disease (norovirus).
Common bacterial infections include Salmonella, E coli, Campylobacter and C.difficile.
Parasitic infections such as Giardia lamblia cause the condition known as giardiasis.
Dehydration can be caused by losing too much fluid, not drinking enough water or fluids, or both.Your body may lose too much fluids from:Excessive sweating Excessive urine outputFeverVomiting or diarrheaExercise during high heat and humidity

Clinical Manifestations of Dehydration
Clinical Manifestations
Mild Dehydration
Moderate Dehydration Severe Dehydration
Level of consciousness Alert Lethargic Obtunded
Capillary refill time 2 seconds 2-4 seconds Greater than 4 seconds, cool limbs
Mucous membranes Normal Dry Parched, cracked
Heart rate Slight increase Increased Very increased
Respiratory rate Normal Increased Increased and hyperpnea
Blood pressure Normal Normal, but orthostatic Decreased
Pulse Normal Thready Faint or impalpable
Skin turgor Normal Slow Tenting
Eyes Normal Sunken Very sunken
Urine output Decreased Oliguria Oliguria/anuria

√ Three types of dehydration based on serum sodium levels:
1.hypotonic or hyponatremic (referring to this as primarily a loss of electrolytes, sodium in particular)
2.hypertonic or hypernatremic (referring to this as primarily a loss of water)
3.isotonic or isonatremic (referring to this as equal loss of water and electrolytes).
Differential Diagnosis:
External or stress-related causes§Infectious diseasesMalnutrition

Signs :
dry or sticky mouthfew or no tears when cryingeyes that look sunken into the headsoft spot (fontanels) on top of head that looks sunkenlack of urine or wet diapers for 6 to 8 hours in an infant (or only a very small amount of dark yellow urine)lack of urine for 12 hours in an older child (or only a very small amount of dark yellow urine)dry, cool skin (poor skin turgor)
Symptoms:
excessive loss of fluid from vomiting or diarrhea if the child refuses to eat or drink.lethargy or irritabilityfatigue or dizziness in an older childthirst and discomfortloss of appetite

Skin turgor assessment – this assessment can be done on the forearm. Skin that does not flatten immediately after release is called “tenting”, an example of fluid volume deficit.
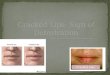
Dry and cracked lips
Sunken eyes
Thirst and discomfort

Examinations and tests
Delayed capillary refillLow blood pressurePoor skin turgor -- the skin may not be as elastic as normal and sag back into position slowly when the health care provider pinches it up into a fold (normally, skin springs right back into place)Rapid heart rateShock (hypovolemic)Complete blood count (CBC)Blood chemistries (to check electrolytes, especially sodium, potassium, and bicarbonate levels)Blood urea nitrogen (BUN)CreatinineUrine specific gravityOther tests may be done to determine the cause of the dehydration (for example, blood sugar level to check for diabetes).

ManagementMild and Moderate Dehydration:1. Fluid Restoration Oral Rehydration
› Oral Rehydration Solution “ORS”› Standard home solutions
Intravenous Rehydration Monitoring for complications of fluid
restoration Monitor Intake and Output for fluid
replacement Nutritious food and supplements

Severe Dehydration:1. Laboratory evaluation and intravenous rehydration
are required. The underlying cause of the dehydration must be determined and appropriately treated.
Phase 1 focuses on emergency management. Severe dehydration is characterized by a state of hypovolemic shock requiring rapid treatment. o IV fluido Tachycardia, capillary refill, urine output, and mental status
all should improve. Phase 2 focuses on deficit replacement, provision of
maintenance fluids, and replacement of ongoing losses.
Maintenance fluid requirements are equal to measured fluid losses

Solution Contents Uses Comments
Hypotonic
5% dextrose in water (D5W)
50g dextrose
No electrolytes
Replaces deficits of total body water.
Not used alone to expand ECF volume because dilution of electrolytes can occur.
Supplies 170 kcal/L and free water
Distilled water cannot be given IV because it would cause hemolysis of RBCs.
Dextrose is metabolized on first pass through liver, leaving a solution of water but without hemolytic problems.
Isotonic
0.9% NaCl (normal saline olution, NS, 0.9% NS)
154 mEq/L Na and Cl ECF deficits in clients with low serum levels of Na or Cl and metabolic alkalosis
Before and after infusion of blood products
Not used for routine administration of IV fluids because it contains more sodium than ECF
Expands plasma and interstitial volume and does not enter cells
Lacteted Ringers
Solution (LR)
130 mEq/L Na
4 mEq/L K
3 mEq/L Ca
109 mEq/L Cl
28 mEq/L lactate
ECF deficits, such as fluid loss with burns and bleeding and dehydration from loss of bile or diarrhea
Solution is roughly isotonic to plasma but does not contain magnesium or phosphate
Lactate is equivalent to bicarbonate and solution can be used to treat many forms of acidosis
Cannot be used in people with alkalosis
Intravenous Water and Electrolyte Solutions

Hypertonic
Lactated Ringer’s
Solution with 5% dextrose (D5/LR)
5o g dextrose
130 mEq/L Na
4 mEq/L K
3 mEq/L K
109 mEq/L Cl
28 mEq/L lactate
FCF deficits, such as fluid loss with burns and bleeding and dehydration from loss of bile or diarrhea
Provides modest calories (170 kcal)
Solution hypertonic because it is combination of two solutions (D5W and LR)
5% dextrose and normal saline (D5/o.9 NS)
50g dextrose
154 mEq/L Na and Cl
ECF deficits in clients with low serum levels of Na or Cl and metabolic alkalosis
Before and after infusion of blood products
Provides modest calories (170 kcal)
Solution is hypertonic because it is combination of two solutions (D5W and NS)
5% dextrose and 0.45% normal saline (D5/0.45 NS; D5/1/2 NS)
50g dextrose
77 mEq/L Na and Cl
Can be used as an initial fluid for hydration because it provides more water than sodium
Provides modest calories (170 kcal)
Commonly used as a maintenance fluid
5% dextrose and 0.225% normal saline
(D5/0.2 NS; D5/1/4 NS)
50g dextrose
34 mEq/L Na and Cl
Can be used as an initial fluid for hydration because it provides more water than sodium
Provides modest calories (170 kcal)
Commonly used as a maintenance fluid

Nursing Management Keep fresh water or other fluids in an easily accessible location. Provide fluids of choice Encourage family members to assist the client Provide oral care every 2 hours to help decrease discomfort from dry mucous membranes Record intake and Output of the client Educate client how to self-care at homeMonitor for signs of Hypovolemic shock

Preventive measures
Even when you are healthy, drink plenty of fluids every day. Drink more when the weather is hot or you are exercising.
Carefully monitor someone who is ill. If you believe that the child is getting dehydrated, call your health care provider before the person becomes dehydrated. Begin fluid replacement as soon as vomiting and diarrhea start -- DO NOT wait for signs of dehydration.
Always encourage a child who is sick to drink fluids. Remember that fluid needs are greater with a fever, vomiting, or diarrhea. The easiest signs to monitor are urine output (there should be frequent wet diapers or trips to the bathroom), saliva in the mouth, and tears when crying.
Encourage adequate rest balanced with moderate activity. Promote adequate nutritional intake.

TreatmentOral re-hydration solutions (ORS) Fluid replacementIntravenous rehydration therapyAlternative therapiesProper food intakeAdequate rest and sleep patternMonitor intake and outputSevere cases: IVF/ NGTMedical treatment:
In cases of severe dehydration, admission to hospital may be required. Fluid may be given through a tube through the nose or saline drip intravenously.

Complications
Untreated severe dehydration may lead to:DeathPermanent brain damage Seizures Cholera Gastroenteritis Shigellosis Fever Electrolyte disturbance
Hypernatremia (also caused by dehydration)Hyponatremia, especially from
restricted salt diets

Let children
Thank you and God Bless




![Presentation1.ppt [โหมดความเข้ากันได้] · Title: Microsoft PowerPoint - Presentation1.ppt [โหมดความเข้ากันได้]](https://img.pdfslide.us/doc/110x75/5ec776d210d7bd5f6f00774b/aaaaaaaaaaaaaaaaaa-title-microsoft-powerpoint.jpg)