Embed Size (px)
Citation preview

Lt Col AK SinghDept of Anaesthesia
Preoperative/PreanaestheticEvaluation(PAC)

Contents
• Definition
• Goals
• Steps of Preoperative Evaluation
• Airway Assessment
• Role of primary care physician & nursing officers
• Conclusion

• This is a procedure to ensure that patient is asymptomatic from the anaesthetic risk point of view before surgery by physiological and psychological preparation.
Part 1
General consideration
Part 2
Anaesthetic implication of concurrent disease
Definition

What is Anesthesia ?
•Amnesia (reversible loss of
consciousness)
•Analgesia
•Areflexia (muscle relaxation)
Triad of

Types of Surgical Procedure
• Type A- Minimally invasive Little physiological changes e.g. cataract
• Type B- Moderately invasive Modest physiological changes e.g. TURP
• Type C- Highly invasive Significant physiological disruption e.g. THR

Goals
Quality of preoperative care
Morbidity and mortality of surgery
Cost of preoperative care
Anxiety

Problem Identification
Risk Assessment
Plan of Anesthetic Management
Preanaesthetic Instructions
Steps of preoperative evaluation

Problem Identification
History
Physical examination
laboratory investigations

History and physical examination are the
most important assessors of disease
and risk.
History

History
• First areas of concern:
– Previous anaesthetic exposure
– Unusual Bleeding
– Medication
– Personal history
– Family history
– Any other illness
– Exercise tolerance

Exercise Tolerance
• 1 MET walk 200-300 m on ground level at
3.2 to 4.8 km/hr
• 4 MET climb a flight of stairs
• 10 MET participate in strenuous
activities (swimming,cycling
tennis,football)

Exercise Tolerance in METs
• 10 METs : Excellent
• 7 – 10 METs : Good
• 4 - 6 METs : Moderate
• < 4 METs : Increased anaesthetic risk

Physical Examination:
General examination
Airway assessment
Respiratory system
Cardiovascular system
System related problems identified from
the history

Airway Assessment
Predictors of difficult intubation
• Mallampati
• ULBT
• Measurements (IID, TMD, SMD)
• Movement of the Neck
• Deformities

MALLAMPATI
PATIENT DOCTOR
Upright, maximal jaw opening, tongue protrusion without phonation

Class I = visualize the soft palate, uvula, anterior and posterior pillars.
Class II = visualize the soft palate and uvula.
Class III = visualize the soft palate and the base of the uvula.
Class IV = soft palate is not visible at all.
Mallampati Classification

ULBT
• Class 1:Lower incisors can bite upper lip
above vermillion line.
• Class 2:Lower incisors can bite upper lip
below vermillion line.
• Class 3:Lower incisors cannot bite the upper lip.

Less than or equal to 4.5 cm is
considered a potentially
difficult intubation.
Generally greater than 2.5 to 3
fingerbreadths (depending on
observers fingers)
Interincisor distance (IID)

Thyromental distance(TMD)
Upright, neck extension, mouth closed, Distance < 6.5cm difficult intubation

Sternomental Distance(SMD)
Extended head and neck, mouth closed, distance <12.5cm is a difficult intubation

Movement of the Neck

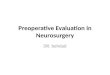
CRANIOFACIAL DEFORMITIES
Pierre Robin Goldenhar'sTreacher Collins

Why would this man’s airwaybe difficult to manage?

Laboratory Tests
•Routine or standing lab tests discouraged
•Based on history or physical examination
Disadvantage1. Increased cost2. Delay in surgery3. Medico legal problem
Advantage 1. Surgeon comfortable 2. Anaesthesiologist comfortable

Recommended test Guidelines For Asymptomatic Patient
• Age up to 49 yrs CBC
• Age 50-64yrs CBC,ECG
• Age > 65 yrs CBC, ECG, CXRUrine analysisBUN/ Cr, ElectrolyteBlood Sugar
• Type C Surg Blood Gr , ALB, Plt

Disease based identification Tests
Alcohol abuse CBC, PT/PTT, AST/Alkp, ECG, Plt
Adrenal cortical Disease CBC, Elec, Glu, Plt
Anemia CBC, Plt
Cancer, except skin, without known metastases
CBC, CXR, Plt
Diabetes Elec, BUN/Cr, Glu, ECG
Hematologic abnormalities CBC, T/S &AB, PT/PTT, Plt
Exposure to hepatitis AST/Alkp, BUN/Cr
Hepatic disease PT/PTT, BUN/Cr, AST/Alkp
Malignancy with chemotherapy CBC, PT/PTT, BUN/Cr, AST/Alkp, CXR, Plt
Malnutrition CBC, T/S &AB, PT/PTT, Plt
Morbid obesity BUN/Cr, Glu, ECG
Peripheral vascular disease or stroke CBC, Glu, BUN/Cr, ELEC, Plt

Disease based identification tests
Personal or family history of bleeding
CBC, PT/PTT, Plt
Poor exercise tolerance or “real age” over 60
CBC, BUN/Cr, Glu, Plt
Possibly pregnant HCG, CXR+
Pulmonary disease CBC, Elec, BUN/Cr , Glu, Plt
Renal disease CBC, Elec , BUN/Cr, Plt
Rheumatoid arthiritis CBC, ECG, CXR+, Plt
Sleep apena CBC, ECG, Plt
Smoking>40 pk/yr CBC, ECG, CXR+, Plt
Suspected UTI r prosthesis insertion U A
Systematic lupus BUN/Cr, ECG, CXR+

Therapy based indications TESTS
Radiation therapy CBC, ECG, CXR, Plt
Use of anticoagulants CBC, PT/PTT, Plt
Use of digoxin and diurectics Elec, Bun/Cr, ECG
Use of statins AST/Alkp, ECG
Use of steroid Eelc, Bun/ Cr, Glu
Procedure based indications
Procedure with significant blood loss CBC, T/S & ALB, Plt
Procedure with radiographic dye Bun/Cr
Class C Procedure CBC, T/S & ALB, Elec, Bun/Cr, Plt

• Respond specifically to the question posed
• Optimize the condition
• Indicate any new observation
• Do not suggest any anaesthetic/surgical
methods
• Statement like “cleared for surgery” or
“prevent hypoxia and hypotension
preoperatively” is not advisable .
Role of The Primary Care Physician
or Consultant

– The consulting internists’ role in
perioperative care is focused on the
elucidation of medical factors that may
increase the risk of anaesthesia and
surgery . Selecting the anaesthetic
technique for a given patient ,
procedure , surgeon , and anaesthetist
is highly individualized and remains the
responsibility of the anaesthesiologist
rather than the internist.
• As to disagreement with the primary care
American College of physician
highlights the role of primary
care physician as-:

Role of Nursing officers
• Relieve anxiety
• Find new complaint
• Follow PAC instructions
• Proper intravenous access
• Monitoring of vitals
• Patient shifted to OT at right time
• Send Patient trolley to OT as soon as informed

medical status mortality
ASA I Normal healthy patient without organic, biochemical, or psychiatric disease
0.06-0.08%
ASA II Mild systemic disease with no significant impact on daily activity e.g. mild diabetes, controlled hypertension, obesity .
Unlikely to have an impact0.27-0.4%
ASA III Severe systemic disease that limits activity e.g. angina, COPD, prior myocardial infarction
Probable impact 1.8-4.3%
ASA IV An incapacitating disease that is a constant threat to life e.g. CHF, unstable angina, renal failure ,acute MI, respiratory failure requiring mechanical ventilation
Major impact 7.8-23%
ASA V Moribund patient not expected to survive 24 hours e.g. ruptured aneurysm
9.4-51%
ASA Physical Status Classification System
For emergent operations, you have to add the letter ‘E’ after the classification.



INGESTED MATERIAL
MINIMUM FASTING PERIOD,
APPLIED TO ALL AGES (hr)
Clear liquids 2
Breast milk 4
Infant formula 6
Nonhuman milk 6
Light meal (toast and clear liquids) 6
Fasting Recommendations

Anaesthetic Plan

Conclusion
• Anaesthesia/surgical risk can be significantly reduced by combined skill of
– Surgeon
– Anaesthesiologist
– Primary care physician
– Nursing officers and Paramedics
– Patient (follow instructions )