Embed Size (px)
DESCRIPTION
Dr Ken Maclean, Clinical Geneticist, from Primary Care Genetics has presented at the Obstetric Malpractice Conference. If you would like more information about the conference, please visit the website: http://bit.ly/10xh1iO
Citation preview


• PGD is a reproductive genetic option, alongside:– Not conceiving– Donor gamete(s)– Adoption– Natural conception– Natural conception, prenatal diagnosis & termination of
pregnancy
– PGD = IVF + ICSI + embryo biopsy + genetic analysis
– Differentiates genetic constitution prior to transfer – genes & chromosomes (PGD vs PGS)

• PGD requires excellence in – Fertility Medicine
– Clinical Genetics
– Embryology
– Molecular analysis
– Embryo vitrification
– Clinical support systems
– Funding
– IVF is the foundation stone of PGD

• Improve health & wellbeing of offspring• Minimise risk of inheriting serious disability• Typically fertile couples
• Adjunct to IVF • Euploid vitrified embryo selection may:
• Increase clinical pregnancy rate per embryo transfer• Reduce miscarriage rate• Reduce risk of IVF-related birth defects
• Infertility may alter threshold for PGD• Disease predispositions


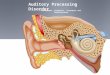
Intra-cytoplasmic sperm injection
(ICSI)
Extensive IVF & genetic work-up in PGD- karyotyping in IVFpreconceptional genetic screening
Multiple appointments & assessments

Laser-assisted hatching
Day 3 embryo: 1-2 cells
(out of 4-8 cells)
OR
D5 embryo (blastocyst)
3-5 trophectoderm cells from
(future placenta)
Inner cell mass (embryo) untouched

Methods for Preimplantation Genetic Screening and Diagnosis.
Bodurtha J, Strauss JF III. N Engl J Med 2012;366:64-73.

DNA extraction & amplification
PCRpolymerase chain
reaction
Genetic analysis done on site or remotely (transport PGD)
Blastocyst vitrification awaiting DNA test results

Array CGH testing
http://www.nature.com/scitable/topicpage/microarray-based-comparative-genomic-hybridization-acgh-45432
Figure 1
Source: Fertility and Sterility 2011; 95:953-958(DOI:10.1016/j.fertnstert.2010.09.010 )
+19/-22
-10/-16
46, XX

Contribution of individual chromosomes to aneuploidy in blastocysts
Fragouli et al. Fertil Steril 2010

Pregnancy outcomes
# embryo transfers 39
implantation rate (# implantations) 46% (18)
<38yrs 56% (9/16)
>38yrs 39% (9/23)
Clinical pregnancy rate/oocyte retrieval 62% (18/29)
<38yrs 75% (9/12)
>38yrs 53% (9/17)

PGD limitations are technical &biological
Embryo mosaicism
Untested embryoslow yield in IVF cyclefailure of laboratory testing
Discrepant results are uncommonEmbryo mosaicismLab error
Option of prenatal testing

GENE
Mutated gene
x

• absence of the mutated gene
May be a failure of DNA amplificationOccurs in 5-10% of PGD testing
x

Linkage analysis is best practice in PGD testing
• Polymorphic short tandem repeats (STRs) that flank the mutation/disease locus
• Determine phasing by family study in PGD work-up
• Highly accurate, highly reproducible: primary test in PGD
GENEMarker 1 Marker 2 Marker 3 Marker 4
Mutation
x

Linkage/marker analysis in beta-thalassaemia
affected embryo
unaffected embryo

Methods for Preimplantation Genetic Screening and Diagnosis.
Bodurtha J, Strauss JF III. N Engl J Med 2012;366:64-73.

• Single gene disorders
• Disease & disability
• Chromosome disorders
– Chromosome translocations
– Comprehensive chromosome screening (aneuploidy)
• Trait selection
• HLA matched stem cell source
• Sex selection
• Carrier status


Common PGD indications

The use of PGD is increasing



Initial PGD cycle may incur >10k out-of-pocket costs
~6-9k for subsequent cycles




• IVF 30 year history– 2-3 million babies. Many are now parents
– 1-2% Australian babies pa are conceived by IVF
• PGD 15 year history
• >1,000 Australian PGD babies


• An excess risk of birth defects in IVF and ICSI infants is biologically plausible.
• Factors associated that may increase the risk of birth defects include– the underlying causes of infertility in the couples
– factors associated with the IVF/ICSI procedures
– eg freezing and thawing of embryos
– delayed fertilization of oocytes
– culture media composition
– medications used to induce ovulation or for luteal phase support
– Endometrial milieu

The risk of major birth defects after intracytoplasmic sperm injection and in vitro fertilisationHansen et al NEJM 2002;346 (10):725-730
Methods
• Data obtained from three registries in Western Australia on births, births after assisted conception, and major birth defects in infants born between 1993 and 1997.
• Assessed the prevalence of major birth defects diagnosed by one year of age in infants conceived naturally or with use of intracytoplasmic sperm injection or in vitro fertilization.
Results
• Twenty-six of the 301 infants conceived with intracytoplasmic sperm injection (8.6 percent) and 75 of the 837 infants conceived with in vitro fertilization (9.0 percent) had a major birth defect diagnosed by one year of age, as compared with 168 of the 4000 naturally conceived infants (4.2 percent; P<0.001 for the comparison between either type of technology and natural conception)
.
• As compared with natural conception, the odds ratio for a major birth defect by one year of age, was 2.0 (95 percent confidence interval, 1.3 to 3.2) with intracytoplasmic sperm injection, and 2.0 (95 percent confidence interval, 1.5 to 2.9) with in vitro fertilization.
• Infants conceived with use of assisted reproductive technology were more likely than naturally conceived infants to have multiple major defects and to have chromosomal and musculoskeletal defects.

• Systematic review all papers published by March 2003 with data relating to the prevalence of birth defects in infants conceived following IVF and/or ICSI compared with spontaneously conceived infants
• Twenty-five studies were identified for review. Two-thirds of these showed a 25% or greater increased risk of birth defects in ART infants.
• Size of ART group in each study ranged from 32-9111 infants
• Additionally results of meta-analyses of the seven reviewer-selected studies and of all 25 studies suggest a statistically significant 30–40% increased risk of birth defects associated with ART.
• Pooled results from all suitable published studies suggested that children born following ART are at increased risk of birth defects compared with spontaneous conceptions
• 1.3-fold risk

• Data analysed from the National Birth Defects Prevention Study, a population-based, multicenter, case–control study of birth defects.
• NBDPS;10 states, investigates environmental and genetic risk factors for 30 major birth defects
• Included mothers of fetuses or live-born infants with a major birth defect (case infants) and mothers who had live-born infants who did not have a major birth defect (control infants), delivered during the period October 1997–December 2003.
• Study compared mothers who reported ART use (IVF or ICSI) with those who had unassisted conceptions.
• 4792 control infants, 9584 case infants.
• ART was reported by 51 (1.1% ) of all control mothers and 230 (2.4%) case mothers
Among singleton births, ART was associated with septal heart defects (adjusted odds ratio [aOR] 2.1, 95% confidence intervals [CI] 1.1–4.0), cleft lip with or without cleft palate (aOR 2.4, 95% CI 1.2–5.1), oesophageal atresia (aOR 4.5, 95% CI 1.9–10.5) and anorectal atresia (aOR 3.7, 95% CI 1.5–9.1).
Among multiple births, ART was not significantly associated with any of the birth defects studied.
Findings suggest that surgically important birth defects occur more often among infants conceived with ART





Epigenetic disorders
Possible link to embryo culture


National Health and Medical Research Council
Ethical Guidelines on the use of assisted reproductive technology in clinical practice and research
S11: Do not select sex for non-medical purposes
• Sex selection is an ethically controversial issue.
• The Australian Health Ethics Committee (AHEC) believes that admission to life should not be conditional upon a child being a particular sex. Therefore, pending further community discussion, sex selection (by whatever means) must not be undertaken except to reduce the risk of transmission of a serious genetic condition….
• Regulatory powers – clinic accreditation

State Laws Regulating Assisted Reproduction
• NSW: Assisted Reproductive Technology Act 2007 & Assisted Reproductive Technology Regulations 2009
• Victoria: Assisted Reproductive Treatment Act 2008 & Assisted Reproductive Treatment Regulations 2009
• South Australia: Assisted Reproductive Treatment Act 1988 & Assisted Reproductive Treatment Regulations 2010
• Western Australia: Human Reproductive Technology Act 1991 & Human Reproductive Technology Act Directions 2004

– http://www.retinaaustralia.com.au/images/X-linkedRecessive.gif
Post-PGD risk (at 99% accuracy) 0.25%Post-PGD risk (at 90% accuracy) 2.5%


Victorian Assisted Reproductive Treatment Act 2008
• Sex selection is prohibited in the following terms:
s28 (1) A person carrying out a treatment procedure must not use gametes or an embryo, or perform the procedure in a particular way, with the purpose or a purpose of producing or attempting to produce a child of a particular sex.
Penalty: 240 penalty units or 2 years imprisonment or both.
(2) Subsection (1) does not apply if—
(a) it is necessary for the child to be of a particular sex so as to avoid the risk of transmission of a genetic abnormality or a genetic disease to the child; or
(b) the Patient Review Panel has otherwise approved the use of the
gametes or embryo for the purpose or a purpose of producing or attempting to produce a child of a particular sex.

JS and LS v Patient Review Panel [2011] VCAT 856
• “In our view, arguments based on completion of family, replacement of a child, or family balance do not advance the welfare or interests of a child born to fulfil that end.”