Embed Size (px)
DESCRIPTION
postpartum hemorrhage workshop part 1 by dr mohamed elsherbiny
Citation preview


Dr. Mohamed El SherbinyMD Ob.& Gyn
Postpartum Hemorrhage (PPH)
Guidelines for Immediate Action “Part I”
Damietta Specialized Hospital Workshop 25-9-2013

Pub Med.
Cochrane library.
SOGC Hemorrhagic Shock Guideline No 115 2002
RCOG Guideline P.Previa No.27 2005
Misoprostol Guidance WHO 2007&FIGO 2009
RCOG Guideline PPH No.52 May 2009
WHO Guidelines PPH 2009
SOGC PPH Guideline No 235 Octob.2009
UpToDate July 2013
Sources of Evidence


1. MetGhamr 23-6-20022. Aswan Syndicate scientific Meeting 3-20063. Dekrnes G Hospital 20064. El Sewas G Hospital Meeting 20065. Damietta Governorate meeting Syndicate 20086. Dakahlia COG Society 8-4-20107. El Manzalla G H Meeting 6-200108. Damietta Specialized Hospital 20119. Samnoud Meeting 3- 2011 10.El Mahlla Meeting 6-201111-17 Zamala 8- 2008 to 7-9-2013 6 Years
Local Scientific Meeting

1. Annual Asute Ob Gyn Conference 20042. Annual Kasr Aini Conference 2006 PPH 3. Annual conference Ob Gyn Banha 20074. Bolak Dakror Ob Gyn Conference 20075. Annual Port Saied Ob Gyn Conference 29-3-20076. Annual Ismailia Conference Ob Gyn 26-7-20077. Annual Zagazig Ob Gyn Conference 1-11-20078. Annual Kasr Aini Ob Gyn Conference 3-4-20089. Pan Arab Ob Gyn Annual Confer. 6 -11 - 2008 o
National Conference

10-Pan Arab Asnnual Conference 6 -11 - 2008 Cairo
11- Conference M C S Mansoura 9- 8 – 2007 12-Gy Obn 6 October Conference 19-3 – 2009
13-ERC RCOG Local Meeting 3-2010 Alexanderia 14- El Azhar Dumyat Annual Conference 201215-Clinical Society of Ob& Gyn, Conference
Mansoura 18-4-2013 16- The 27th Anual Scientific M. of Ob.Gyn
Alexandria 2-3 May 2013
National Conference

1 - The 7th World Congress of Perinatal Medicine in Devolving countries Alexanderia March 29th to 30th 20122 - The XX FIGO World Congress October Italy, 20123 - The 3rd Annual ERC/ELG (RCOG)March
2-3-2013
International Conference

Worldwide postpartum
hemorrhage is the commonest cause of maternal mortality.
(Especially in developing countries (

0
5
10
15
20
25
30
35
Pos
tpar
tum
hm
orrh
age
Hyp
erte
nsiv
e d
isea
se
An
tepa
rtum
hem
rrha
ge
Ru
ptur
ed u
teru
s
Ob
stru
cted
lab
our
Ces
area
n S.
An
esth
esia
Pu
lmon
ary
embo
lism
Spon
tane
ous
abor
tion
Indu
ced
abor
tion
Seps
is
Ect
opic
Oth
er d
irec
t
Direct causes of maternal death
National Maternal Study 2000

Guidelines for Immediate Action Before : PreventionA. Identify B. Management Of Established PPH 1 - Communication
2 - Resuscitation
3 - Monitoring and investigation
4 - Arresting the bleeding

Before : Prevention
I - Risk Factors for PPH
2 - Management of Third Stage

I - Risk Factors for PPH


Known Antenatal Risk
Substantial RiskO.RSignificant RiskO.R
Suspected or proven Placental abruption
13Previous PPH3
Known placenta praevia tone
12Asian ethnicity2
Multiple pregnancy5Obesity ( BMI>35 )2
Pre-eclampsia/gestational hypertension
4Anaemia ( <9 g/dl )2

Intra-Partum / Postartum risk Significant riskO.RSignificant riskO.R
Delivery by emergency C.S4 Operative vaginal delivery
2
Delivery by elective C.S2Prolonged labour (>12 hours )
2
Induction of labour2Big baby ( >4kg )2
Retained placenta5Pyrexia in labour 2
Mediolateral episiotomy5Age ( >40yeares, not multipa-rous )
1.4

2 - Management of
Third Stage

Active management of the 3rd stage of
labour lowers maternal blood loss and
reduces the risk of PPH by about 60%.
It should be offered to all women
Management of 3rd Stage

Low-risk Vaginal Deliveries:Oxytocin 10 iu (IM) or
Oxytocin 30 iu IV infusion in1000 mL,150 mL/h *
Management Of Third Stage
High risk V. Deliveries or CS :Oxytocin 5 iu IV over 5 minutes .OrCarbetocin (Oxytocin analogue) 100 µg IV bolus
over 1 minute *

Oxytocin 5-10 iu + Methergin 0.2mg
(Syntometrine ) may be used in the
absence of hypertension (for instance,
antenatal low haemoglobin) as it reduces
the risk of minor PPH (500-1000 ml) but
increases vomiting.
Management of Third Stage

A single 100 µg IV injection of carbetocin is as effective as a continuous 2-h infusion of oxytocin
Carbetocin Vs oxytocin for the prevention
of PP following CS:
Carbetocin is associated with a reduced
use of additional oxytocics

Oxytocics ComparisonMethyle
Ergometrine
(Methergine
OxytocinCarbetocinPabal
Oxytocin analogue Amp 1m :0.1 mg
IVIMIVIMIVIM
Onset of
action
2-3 m2-5m< 1 m3 m< 1 m< 2 m
Contraction
Time
60m3 H1 6 m30 m67 m120 m
Storage< 25°C
Dark storage
< 25°C2-8°C
(refrigerator)22
Clinically IV only

Carbetocin :PabalAt CS, carbetocin resulted in a statistically significant reduction in the need for therapeutic uterotonics compared to oxytocin, but there is no difference in the incidence of PPH. Carbetocin is associated with less blood loss compared to syntometrine in the prevention of PPH for at vaginal deliveries and is associated with significantly fewer adverse effects. Further research is needed for the cost-effectiveness of carbetocin as a uterotonic gent.
Su et al Cochrane Systematic Review Apr.2012

Misoprostol is not as effective as oxytocin
but it may be used when oxytocin is not
available, such as the home-birth setting.
Management Of Third Stage
Recommended Dosages600 µg orally or sublingually.

25
The peak of action of misoprostol is not consistent with the 3rd stage ,so it is not as effective as oxytocin

RouteOnset of action
Durationof action
Oral8 min∼2 h
Sublingual11 min∼3 hHighest area under the curve
Vaginal20 min∼4 h
Rectal20-100 min∼4 hLowest area under the curve
Pharmacokinetic Profiles of MisoprostolWhy Orally Or Sublingually?


A:Identify

I -Estimated blood loss 500- 1000 ml & No clinical signs of shock
Measures to facilitate resuscitation should it become necessary.
Close monitoring IV accessCBC ,Blood group and screen
Primary PPH: Definition
Management dependent definition
Minor PPH

II-Estimated blood loss >1000 ml or
clinical signs of shock
Protocol of measures to achieve
resuscitation and haemostasis.
Primary PPH: Definition
Management dependent definition
Major PPH

What Are the Degrees of Shock?
Compensated Hemorrhagic Shock
Mild Hemorrhagic Shock
Moderate Hemorrhagic Shock
Severe Hemorrhagic Shock
31

Compensated Hemorrhagic ShockLoss of ≤ 15% of blood volume may not be
associated with any change in blood BP, pulse, or capillary refill.
As symptoms usually precedes the sign, these symptoms may be presented :
AnxietyRestlessnessFeeling of breathlessness .
Urinary output > 30 mL/h
32

Degree of shock
Blood loss
Signs & symptoms
Mild<20%Anxiety , Sweating & Palpitation
Increased capillary refilling
Cool extremities
Moderate20% to
40%
+ Tachycardia& Tachypnea
Postural hypotension
Oliguria (< 20 mL/h)Severe>40%+ Hypotension
Agitation/confusion
Collapse& Anuria
Signs And Symptoms Of Shock
NB. Blood volume at term: ± 100 ml/kg

1.Communication
2.Resuscitation
3.Monitoring and investigation
4.Arresting the bleeding
Treatment of the underlying disorder (4Ts)
Management of Intractable PPH
Management of Established PPH4 components: undertaken simultaneously:

1-Minor PPHEstimated blood
loss 500- 1000 ml & No clinical signs of
shock(Compensated Shock)
2-Major PPH
II-Estimated blood
loss >1000 ml or
clinical signs of shock
Management Of Established PPH Depends On Degree of Blood Loss
If not at a Hospital, it must be referred
urgently

1-Minor PPHEstimated blood
loss 500- 1000 ml & No clinical signs of
shock(Compensated Shock)
Management Of Established PPH Depends On Degree of Blood Loss

2-Resusetation Minor PPH <1000
ml &CompensatedMajor PPH >1000 ml or Shock
Intravenous
access one 14-
gauge cannula
Crystalloid infusion.
AB,C : Assess: Airway,
Breathing& Circulation
O2 by mask at 10–15 L/M
14-gauge cannula x2 orange
Transfuse blood rapidly
Until blood is available, IV up
to 3.5 L crystalloid lactated Ringer (± one L of it is colloid)
Keep patient& infusions warm
She had received one L lactated Ringer solution

3-Monitoring and InvestigationMinor PPH <1000 ml
&Compensated)Major PPH >1000 ml or Shock
Venepuncture
(20 ml) for:GroupCBC Coagulation screen
Pulse and BP/15m
Venepuncture (20 ml) for:Crossmatch (≥4 units) CBC & Coagulation screenBasal renal and liver F Ts.
Continuous:P ,BP,RR
Temperature /15 m
Foley C. : urine output
2 cannulae, 14- or 16-gauge
All recorded on a flow chart

Estimated bloodloss 500- 1000 ml &
No clinical signs of shock
(Compensated Shock)
1-Minor PPHII-Estimated blood
loss >1000 ml or
clinical signs of
shock
Management Of Established PPH Depends On Degree of Blood Loss
2-Major PPH
If not at a Hospital, it must be referred
urgently

1.Communication
2.Resuscitation
3.Monitoring and investigation
4.Arresting the bleeding
Treatment of the underlying disorder (4Ts)
Management of Intractable PPH
Management Of Established PPH4 components: undertaken simultaneously:
41

1-CommunicationMinor PPH <1000 ml
&CompensatedMajor PPH >1000 ml or
Shock
Alert first-line obstetric
and anaesthetic staff
trained in the
management of PPH.
ØCall obstetric middle
grade & alert consultantØCall anaesthetic middle grade & alert consultant.ØAlert consultant clinical haematology
ØAlert blood transfusion
laboratory.

2-Resusetation Minor PPH <1000
ml &CompensatedMajor PPH >1000 ml or Shock
ØIntravenous
access one 14-
gauge cannulaØCrystalloid infusion.
ØAB,C : Assess: Airway,
Breathing& CirculationØO2 by mask at 10–15 L/MØ14-gauge cannula x2ØTransfuse blood rapidly ØUntil blood is available, IV up
to 3.5 L crystalloid lactated Ringer (± one L of it is colloid) ØKeep patient& infusions warm


2-Resusetation •Volume replacement must be undertaken on the basis that blood loss is often grossly underestimated.• Compatible blood (supplied in the form of packed RBCs) is the best fluid as soon as available,•If necessary Rh negative O blood.

Massive Blood Loss : What Are The Main Goals Of Management ?
The Main Goals is to maintain:• Haemoglobin > 8g/dl• Platelet count > 75 x 109/l• Prothrombin T < 1.5 x mean control• Activated prothrombin times (APT) < 1.5 x mean control• Fibrinogen > 100mg/dl

ComponentUsual Indicationstarting dose
Packed RBCReplacement of oxygen-carrying capacity
2– 4 Units IV
Fresh frozen plasma
Documented coagulopathy
2–6 Units IV
CryoprecipitateCoagulopathy with low fibrinogen
10–20 Units IV
PlateletsThrombocytopenia/ thrombasthenia with bleeding
6–10 Units IV
Indications For Blood Component Therapy
Packed RBC : Fresh frozen plasma: Platelets = 6:4:1

Intravenous fluid replacement with isotonic crystalloids should be used in preference to colloids for resuscitation of women with PPH.
High doses of colloids :
More expensive
May cause adverse effects
Colloids versus crystalloids ?2-Resusetation

CoagulopathyFresh frozen plasma 4 units for:
Every 6 units of red cells or
Prothrombin time > 1.5 x normal
Activated partial thromboplastin time > 1.5 x normal
(12–15 ml/kg or total 1 litres)
Platelets : if PLT count < 50 x 109 /L

• During the wait lactated Ringer :3mI for every one mI of blood lost (*)
• Ringer’s lactate is preferred over normal saline to avoid hyperchloremic acidosis(**)
• There is no place for hypotonic dextrose solutions (**)
Hypovolumeic Shock

Whole blood is needed when acute hemorrhage is catastrophic.
Whole Blood Vs Component therapy
Component therapy provides better treatment because only the specific component needed is given.

Donor Compatible plasma
Compatible red cells
Compatible platelets
Compatible platelets
Recipient
ABO group
1st choice2nd choice
AA,ABA,OA,ABB,O
BB,ABB,OB,ABA,O
OO,A,B,
AB
OOA,B,AB
ABABAB,A,B,
O
ABA,B,O
Blood Component : Recipient & Donor

3-Monitoring and InvestigationMinor PPH <1000
ml &CompensatedMajor PPH >1000 ml or Shock
Venepuncture
(20 ml) for:GroupingCBC Coagulation screen
Pulse and BP/15m
Venepuncture (20 ml) for:Crossmatch (≥4 units) CBC & Coagulation screenBasal renal and liver functions
Continuous: Pulse , BP & RR
Temperature /15 m
Foley catheter: urine output
2 cannulae: 14 or 16 gauge
All recorded on a flow chart

Poor Man's" Fibrinogen Assay
• If a clot does not form within 6 m or • Clot forms and lyses within 30 m.
A coagulation defect is probably present and the fibrinogen level is
< 150 mg/dl

1.Communication
2.Resuscitation
3.Monitoring and investigation
4.Arresting the bleeding
Treatment of the underlying disorder (4Ts)
Management of Intractable PPH
Management Of Established PPH4 components: undertaken simultaneously:

Arresting The Bleeding
Causes for PPH may be considered to relate to one or more of ‘the four Ts’:
● Tone (abnormalities of uterine contraction)
● Tissue (retained products of conception)
● Trauma (of the genital tract)
● Thrombin (abnormalities of coagulation).

Postpartum HemorrhageEmptying the bladder
40 iu oxytocin in 1000 mL lactated Ringer
Firm fundal massage
Before delivery of the placenta
After delivery of the placenta
Contracted cervix
Partial separation
Placenta Accreta
Uterine Atony
Genital Tract Trauma
Coagulation Disorders

Postpartum Hemorrhage Before Delivery Of The Placenta
Brandt-Andrwes
(Controlled cord traction)Succeeded
Fundal massage &Oxytocin infusion
Continuo oxytocin infusion& fundal massageIntra-umbilical cord injection Misoprostol
(800 g)
Manual Removal
Contracted cervix
Nitroglycerin 500ug iv
Partial separation
Peeling
Placenta Accreta
Hysterectomy Piece meal removal ±Methotrexate /Anti progestrone /Embolization In all cases continue fundal massage &oxytocin infusion

Postpartum Hemorrhage after delivery of the placenta
Firm fundal massage &Oxytocin infusion
Bleeding stopped
Conservative T: Massage & oxytocin infusion
Bleeding not stopped
Firm uterus
Exploration1-Trauma
Repair of lower & upper GT up to Hysterectomy
2-Remnant:Removal
3-Coagulopathy:Reverse
Emptying the bladder
Bimanual compression
Atonic uterus
Uterotonics+
Bleeding
stopped
Bleeding not stopped
IntractablePPH
Bleeding not stopped

Bimanual Compression

Aortic Compression

Uterotonics(3 lines)
62

First Line UterotonicsFor management of PPH, oxytocin should
be preferred over :Ergometrine aloneFixed-dose combination of ergometrine and oxytocin,CarbetocinProstaglandins.

First Line Uterotonics• Oxytocin (Syntocinon®) 5 units IV over
5 m (± repeated) then
• Infusion (40 u in 500 ml L Ringer at 125 ml/hour).
• Not more than 3 L of IV fluids containing oxytocin.

First Line UterotonicsCarbetocin (Pabal®) , 100µg given as
an IV bolus over 1 minute (Can be
repeated )is an alternative
.

Second Line UterotonicsIf the bleeding does not respond to the 1st-line, Ergometrine will
be the second line:• Ergometrine (Methergin®) IM / IV (slowly): 0.2 mg • Repeat 0.2 mg IM after 15 minutes • If required, give 0.2 mg IM or IV slowly / 4 HMaximum dose :5 doses (Total 1.0 mg) Contraindications :Pre-eclampsia, hypertension, heart disease

Third Line UterotonicsIf the bleeding does not respond
to the 2nd-line treatment:
Prostaglandin / Misoprostol
should be offered.

MisoprostolCytotic®,Mesotac® ,Mesoprost®
The recommended dose:600 µg oral or sublingual1000 µg rectal my be used if these routes are not suitable (efficacy < 50%)

Misoprostol Versus IV Oxytocin
Sublingual misoprostol (800 µg) is clinically equivalent to IV oxytocin (40iu) when used to stop atonic PPH in women who have received oxytocin during the 3rd stage of labour.

Misoprostol Versus IV Oxytocin
In settings in which use of oxytocin is not feasible, misoprostol might be a suitable first-line treatment alternative for post-partum haemorrhage.

Misoprostol• A repeated dose should not be given
unless at ≥ 2 h since the first dose.
• If the initial dose was associated with pyrexia or marked shivering, then at least 6 hours should lapse before the second dose is given.

rFVIIaRecombinant human coagulation
Factor VIIa (rFVIIa): NovoSeven® 90 μg/kg given/2 hours bolus
infusionUnproven Effect

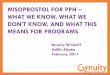
Tranexamic Acid For The Treatment Of Postpartum Haemorrhage
• Tranexamic acid decreases postpartum blood loss after vaginal birth and after CS based on two RCTs of unclear quality which reported only few outcomes.
• Further investigations are needed on efficacy and safety of this regimen for preventing PPH.

Tranexamic Acid For The Treatment Of Postpartum Haemorrhage
“The WOMAN Trial” : Waiting the result
An international randomised, double blind
placebo controlled trial.
The trial will be a large, pragmatic, randomised,
double blind, placebo controlled trial among
15,000 women with a clinical diagnosis of PPH

The patient received :1-Syntocinon 5 units IV over -5iu & (40 u in 500 ml L
Ringer at 125 ml/hour).2-Methergin 0.2 mg/slow IV and other 0.2 mg IM and
repeated after 15 minutes3-600µg misoprostol sublingually
The bleeding subsided for 30 minutes Then the uterus was not responding to treatment or massage and other ± 500 ml of blood were lost.
The case is now categorized as “Major PPH” What is the best line of management?
Return to The case Scenario

1.Communication
2.Resuscitation
3.Monitoring and investigation
4.Arresting the bleeding
Treatment of the underlying disorder (4Ts)
Management of Intractable PPH
Management Of Established PPH4 components: undertaken simultaneously:

PPH After CS : Causes 1- uterine atony 2-Placent previa &placenta accreta/ increta/percreta 3- Trauma: bleeding from the uterine incision or extensions of this incision or bleeding from vaginal or cervical tears or uterine rupture 4- Retained placenta
77

PPH After CS : ManagementUterine atony: Fundal massage and uterotonic drugs (including intrauterine injection ) Truma:Inspection for and repair of lacerations and incisional bleeding. The angles of a transverse incision should be clearly visualized and any retracted vesselsare ligated. The ipsilateral ureter should be identified before bleeding is controlled. 78

Intractable PPH About 10 % of women will not respond to the initial management steps and are considered as intractable PPH. They are caused mainly by •Uterine atony
•Placenta accreta at CS scar
• Difficult trauma repair
•Coagulopathy79

Bimanual Compression

Intractable PPH About 10 % of women will not respond to the initial management steps and are considered as intractable PPH. They are caused mainly by •Uterine atony
•Placenta Previa accretes at CS scar (PP accreta)
• Difficult trauma repair
•Coagulopathy

Intractable Postpartum Hemorrhage AlgorithmVaginal delivery
Garment balloon tampnadeArterial embolization
Local Control
Garment
Suellen Miller, 2005

Management of Uterine Atony
If pharmacological measures fail : “Intrauterine balloon tamponade “
is the first-line ‘surgical’ intervention
RCOG Guideline PPH No.52 May 2009 Grade C

Intractable Postpartum Hemorrhage AlgorithmVaginal delivery
Local Control
Garment
Gauze Pack or Balloon Tamponade
Arterial embolization
Bakri Tamponade Balloon
Sengstaken-Blakemore Tube
Condom

Sengstaken–Blakemore tube
Three lumen tube(one for drainage)Volume > 500ml

86
Rüsch Hydrostatic Balloon Catheter
Capacity >500 ml
A 60-ml bladder syringe
can be used
But It does not have a drainage channel to monitor ongoing bleeding after placement.
Available in some urologycenter for controlling prostatic bleeding.

Bakri Balloon
A silicone balloonIt was designed as obstetric tamponadeCapacity 500 cc of sterile salineIt has a drainage channelFDA approved
Bakri et al . Int J Gynaecol Obstet 2001;74:139–42

Bakri Balloon

In contrast to the Bakri balloon, the balloon end of the catheter is flush with the end of the balloon
BT-Cath Balloon
A silicone balloonIt was designed as obstetric tamponadeCapacity 500 cc of sterile salineFDA approved

Condom Balloon Tamponade First used by Akhter et al. 2003 at Bangladesh
A 20 women with PPH using the B-LynchA 23 were managed using the condom catheter
with success rate 100%Simple to use, inexpensive and safe.
Akhter et al . MedGenMed.2003 Sep 11;5(3):38. Bangladesh
Condom has no drainage channel to monitor ongoing bleeding.It is clean but not sterile Availability at theater ?

Condom Balloon Tamponade
Akhter et al . MedGenMed.2003 Sep 11;5(3):38. Bangladesh

Mechanism of Action of Balloon Tamponade
I- Exertion of inward to outward hydrostatic pressure against the uterine wall. This pressure may or may not be in excess of systemic arterial pressure . The net result is reduction in persistentcapillary and venous bleeding from theendometrium and myometrium.
Sinha ,Obstet Gynecol. 2003;102(3):641
Georgiou , BJOG. 2010;117(3):295
Bakri,UpToDate,Aug,2013

Mechanism of Action
II-Direct uterine artery (UA) compression
Decreased UA blood flow has been
observed on ultrasound examination in
patients with an intrauterine
Sengstaken-Blakemore tubeCho et al ,Ultrasound Obstet Gynecol. 2008;32(5):711.
Bakri,UpToDate,Mar.,2013

Indications of Balloon TamponadeIn Management of PPH
1- After vaginal delivery for
“Atonic PPH”. (Success R. :80-100%)
2- After CS with placenta
previa / accreta . (Success R.: 56%)
3-Secondary PPH

Mohamed El Sherbiny MD Ob.& Gyn. Damietta Egypt
Use of a Surgical
Glove to Control
Severe Postpartum
HemorrhageXX FIGO World Congress
October 2012

Mohamed El Sherbiny MD Ob.& Gyn.
Hafez Gewely Egyptian Board Ob Gyn
El Saeid Hammoda : Egyptian Board Ob Gyn
Mohamed El Hennawy MS Ob-Gyn
Ahmad Mohamed El Serbiny MS Ob. Gyn
Damietta Egypt

The Inverted
Glove Balloon
TapenadeEl Sherbiny et al FIGO 2012

The Inverted Glove TapenadeWith aseptic precautions knots are mad on all
fingers of a surgical glove to render it a single cavity
Then the glove is inverted to have a smooth outer surface.
98
finger knotted Inverted Glove
El Sherbiny et al FIGO 2012

El Sherbiny et al FIGO 2012

The Inverted Glove TapenadeA sterile Foleys catheter is inserted within theglove and tied near the mouth of the glove witha silk thread, and the outer end of the catheter is connected to a saline set.
El Sherbiny et al FIGO 2012

Then the glove is introduced into the uterine cavity.The cervix is grasped with ring forceps. A long dressing forceps is used to insert the glove balloon catheter into the uterine cavity.Alternatively, the catheter can be inserted manually ±)U/S
Guided(
Glove Tapenade: Insertion
El Sherbiny et al FIGO 2012

Beside the glove ,other Foleys catheter is also inserted as a drainage channel to monitor ongoing bleeding.
El Sherbiny et al FIGO 2012


El Sherbiny et al FIGO 2012

El Sherbiny et al FIGO 2012

Glove Inflation The glove is inflated with 200-500 mL
normal saline, according to need.A roller gauze is introduced into the vaginal cavity to keep the uterine
balloon in place.The glove and the catheters were kept
for 24 hours, and gradually deflated when bleeding ceased
El Sherbiny et al FIGO 2012

How To Keep The Tamponade In Situ ?
1-A roller gauze is introduced into the vagina
for packing it.
Other alternative 2-Other glove is introduced into the vaginaand inflated by warm saline. or3-Placement of adjunct cervical cerclage

Results Within 20 minutes the bleeding was
stopped in 22 out of 24 women (92%) in which the glove tamponade was used .
In 2 cases, hysterectomy was required despite successful placement of thecatheter .The fertility of these 2 patientwas not desired.

Results None of the patients went into irreversible shock or death . There was no clinical evidence of intrauterine infection. Nine patients were followed up for subsequent pregnancy and 7 (78%) of them got pregnant within 2 years.


Conclusion The Intrauterine tamponade with a
surgical glove is a simple, safe,
inexpensive, readily available and
effective means of treating massive
atonic postpartum hemorrhage.

Combination of External Compression & Internal Tamponade
Intrauterine balloon (Bakri) can be used incombination with a B-Lynch uterine compression suture to create a "uterine sandwich," whereby the uterus is compressed between the balloon internallyand the compression suture externally
Nelson &O'Brien , Am J Obstet Gynecol. 2007;196(5):
Diemert et al.Am J Obstet Gynecol. 2012;206(1):65.e1

B-Lynch Technique

Periprocedure Monitoring And Care Patients with a negative test (ie, bleeding is not controlled) should proceed to laparotomy Broad spectrum antibiotic prophylaxis Uterotonics Adequate analgesia Monitor for blood loss( pallor, dizziness, hypotension, tachycardia, confusion) Periodic flushing of the drainage port toensure that it has not become occluded by bloodand to remove clots.

Thank YouThank You

Thank You
Thank You
Egypt

1-Minor PPHEstimated blood
loss 500- 1000 ml & No clinical signs of
shock(Compensated Shock)
2-Major PPH
II-Estimated blood
loss >1000 ml or
clinical signs of shock
Management Of Established PPH Depends On Degree of Blood Loss
If not at a Hospital, it must be referred
urgently

2-Resusetation Minor PPH <1000
ml &CompensatedMajor PPH >1000 ml or Shock
Intravenous
access one 14-
gauge cannula
Crystalloid infusion.
AB,C : Assess: Airway,
Breathing& Circulation
O2 by mask at 10–15 L/M
14-gauge cannula x2 orange
Transfuse blood rapidly
Until blood is available, IV up
to 3.5 L crystalloid lactated Ringer (± one L of it is colloid)
Keep patient& infusions warm

3-Monitoring and InvestigationMinor PPH <1000
ml &CompensatedMajor PPH >1000 ml or Shock
Venepuncture
(20 ml) for:GroupingCBC Coagulation screen
Pulse and BP/15m
Venepuncture (20 ml) for:Crossmatch (≥4 units) CBC & Coagulation screenBasal renal and liver functions
Continuous: Pulse , BP & RR
Temperature /15 m
Foley catheter: urine output
2 cannulae: 14 or 16 gauge
All recorded on a flow chart

Arresting The Bleeding
Causes for PPH may be considered to relate to one or more of ‘the four Ts’:
● Tone (abnormalities of uterine contraction)
● Tissue (retained products of conception)
● Trauma (of the genital tract)
● Thrombin (abnormalities of coagulation).

Postpartum Hemorrhage after delivery of the placenta
Firm fundal massage &Oxytocin infusion
Bleeding stopped
Conservative T: Massage & oxytocin infusion
Bleeding not stopped
Firm uterus
Exploration1-Trauma
Repair of lower & upper GT up to Hysterectomy
2-Remnant:Removal
3-Coagulopathy:Reverse
Emptying the bladder
Bimanual compression
Atonic uterus
Uterotonics+
Bleeding
stopped
Bleeding not stopped
IntractablePPH
Bleeding not stopped

1.Communication
2.Resuscitation
3.Monitoring and investigation
4.Arresting the bleeding
Treatment of the underlying disorder (4Ts)
Management of Intractable PPH
Management Of Established PPH4 components: undertaken simultaneously:

Intractable PPH About 10 % of women will not respond to the initial management steps and are considered as intractable PPH. They are caused mainly by •Uterine atony
•Placenta accreta at CS scar
• Difficult trauma repair
•Coagulopathy124

Management of Uterine Atony
If pharmacological measures fail : “Intrauterine balloon tamponade “
is the first-line ‘surgical’ intervention
RCOG Guideline PPH No.52 May 2009 Grade C

Beside the glove ,other Foleys catheter is also inserted as a drainage channel to monitor ongoing bleeding.
El Sherbiny et al FIGO 2012