Embed Size (px)
DESCRIPTION
website: http://www.am-medicine.com Facebook page : https://www.facebook.com/pages/Am-medicine/207726329406832 Facebook group: https://www.facebook.com/groups/1409138472653811/
Citation preview

Ventilation‐perfusion in health &Ventilation‐perfusion in health & disease
Arjun SrinivasanArjun Srinivasan

Where was the beginning ?

Distribution of ventilationDistribution of ventilation
• Spatial & anatomical variation
• Rate of alveolar filling• Rate of alveolar filling
• Rate of alveolar emptying

Ventilation distribution RC tVentilation distribution‐ RC tf s
last
low
100
100
100
)
50
75
50
75
50
75
R=1 R=2C 1 %
of f
inal
)
25
50
25
50
25
50
R=1C 1
C=.5t = .5
C=1t =2
olum
e (%
00 1 2 3
00 1 2 3
00 1 2 3
C=1t = 1
v0 1 2 3
sekundy0 1 2 3
sekundy0 1 2 3
sekundyseconds

Clinical relevanceClinical relevance
• Perfusion is poor & pulsatile at apex
• P & P proportionately increases from top toPa & Pv proportionately increases from top to bottom
P h i i ll i h i• PA changes minimally with gravity
• Pressures are max at bottom – Pulm edema starts at bottom
Redistribution of blood flow to apex antler’s– Redistribution of blood flow to apex – antler’s horn

Its not just gravity!Its not just gravity!
Lung perfusion in zero gravity situations is more uniform but by no meansequally distributed
Nunn’s Applied respiratory physiology, 6 th edition

Understanding V/Q relationshipsUnderstanding V/Q relationships
C id l i l it• Consider lung as single unit
l h b l l– Relationships between PA O2, PA CO2, alveolar ventilation & pulmonary blood flow
– Alveolar gas equation
• Consider lung as multiple units of varying V/Q
– Clinical consequences in health & disease

Alveolar PO and PCOAlveolar PO2 and PCO2
D i d b h i b il i d• Determined by the ratio between ventilation and blood flow: V/Q
• PO2 and PCO2 are inversely related through alveolar il iventilation
• Increasing V/Q produces higher PAO2 and lower PACO2
• Decreasing V/Q produces lower PAO2 and higher PACO2

Gas Composition in the Alveolar SpaceGas Composition in the Alveolar SpacePiO2 = (barometric pressure‐H2O vapor pressure) xFiO2
( )= (760 – 47) x 0.21 =150 mmHg

Alveolar Gas EquationAlveolar Gas Equation
PAO2 = (PiO2) – (PaCO2/R)
PaCO2 approximates PACO2 due to the rapid diffusion of CO2
R = Respiratory Quotient (VCO2/V02) = 0.8
In a normal individual breathing room air:
PAO2 = 150 – 40/0.8 = 100 mmHg2 / g

il i / f i i ( / )Ventilation/perfusion ratio (V/Q)
V
Q

V/Q distribution in health
West JB, Respiratory Physiology, The Essentials, 6th ed. 2000, Lippincott, p. 54.

V/Q ratio in diseaseV/Q ratio in disease
obstruction alveolusvessel
40
50
40
50
40
50 “ideal”V/Q
↓30
PCO2( )
30PCO2
( )
30PCO2
( )
↓ V/Q ↑ V/Q
shunt/deadspace
10
20(mmHg)
10
20(mmHg)
10
20(mmHg)
embolus
shunt/venous
admixture
space
0
10
0 40 80 120 1600
10
0 40 80 120 1600
10
0 40 80 120 160
embolus
PO2 (mmHg)PO2 (mmHg)PO2 (mmHg)

Low V/Q Effect on OxygenationLow V/Q Effect on OxygenationOne lung unit hasOne lung unit hasnormal ventilation andperfusion, while the has inadequate ventilationhas inadequate ventilation
L↑ PCO2↓Normal Low
V/Q↓ PO2
PO2 100
PO2 50
PO2 ?PO2 100 PO2 ?

Oxyhemoglobin Dissociation CurveOxyhemoglobin Dissociation CurveCO2=(1.3 x HGB x Sat) + (.003 x PO2)
100
on
( ) ( )
16
20
00 m
l)
60
80
aturatio
12
16
t (m
l/10
40
60
glob
in S
8 Con
tent
20
% Hem
og
4 ygen
C
00
20 40 60 80 100
%
0
Oxy
0 20 40 60 80 100
PO2mmHg

Low V/Q Effect on OxygenationLow V/Q Effect on Oxygenation
LPO2 50 mmHg
Normal LowV/Q
Sat 80%O2 content 16ml/dl
PO2 100
PO2 50
PO2 100 mmHg PO2 100PO2 = 60Sat 90%O2 content 18ml/dl
2 gSat 100%O2 content 20ml/dl

HIGH V/Q Effect on OxygenationHIGH V/Q Effect on Oxygenation
HIGHPO2 130mmHg
Normal HIGHV/Q
Sat 100%O2 content 20 ml/dl
PO2 100
PO2 130
PO2 100 mmHg PO2 100PO2 = 100Sat 100%O2 content 20 ml/dl
2 gSat 100%O2 content 20ml/dl

High + low V/Q = ?High + low V/Q = ?
LPO2 50 mmHg
HIGH V/Q LowV/Q
Sat 80%O2 content 16ml/dl
PO2 130
PO2 50
PO2 130 mmHg PO2 130PO2 = 60Sat 90%O2 content 18ml/dl
2 gSat 100%O2 content 20ml/dl

Local ↑ V/Q above ~1 has minimal effect on [O2]
160
160 23
120
160
PaO2(mmHg)
120
160
21
22
23
O2content
( / )120120
20
21 (ml/100 ml)
8080
18
19
4040
16
17
00.001 0.01 0.1 1 10 100
V/Q
0 150.001 0.01 0.1 1 10 100
V/Q
Thus ↑ V/Q in one part of lung can’t compensate for ↓ elsewhere

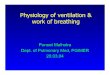
PCO in V/Q MismatchPCO2 in V/Q Mismatch
• Increased ventilation can compensate for low V/Q units
80
ml)low V/Q units
– Shape of CO2 curve
60
T (m
l/100
m
Shape of CO2 curve
• Total ventilation (VE)
40
20 CO
NTE
NT
2( )must increase for this compensation
20
0 40 60 80
CO
2
0 20 40 60 80
PCO2
(mmHg)

fi iInfinity
↑V/Q↑V/QDead space

Zero
↓V/QShuntShunt
Venous admixture

Ventilation to Perfusion MismatchVentilation to Perfusion Mismatch Pure PureShunt
Perfusion with No Ventilation
Dead SpaceVentilation withNo Perfusion
Shunt LikeUnits
Dead Space Like UnitsNo Ventilation No PerfusionUnits Like Units
shunt Dead space

3 compartment model3‐ compartment model
1
2
3

Dead spaceDead space
• Defined as wasted ventilation
• Classification– Anatomical ( 1 ml / pound of ideal body wt)
– Alveolar
– Physiological • Anatomical + alveolarAnatomical + alveolar

Physiological Dead Space by Bohr’s
V X F V X F
Method (for CO2)VT X FE = VA X FA
VT = VA + VDVA = VT – VDVT X FE = (VT – VD) X FA
VD = FA – FEVT FAVT FA
VD = PACO2 – PECO2 (Bohr Equation), so…VT PACO2
VD = PaCO2 – PECO2V PaCO P CO
VT PaCO2

Physiologic Dead Space &V/Q Mismatch
Hyperinflation Low Perfusion No PerfusionHyperinflation Low Perfusion No Perfusion
• Airway Obstruction • Low Cardiac Output • Pulmonary Embolus• Dynamic Hyperinflation • Tidal Volume• PEEP
• Pulmonary VascularInjury
• Extravascular
• Vascular Obliteration• Emphysema
Compression

Shunt equationShunt equation
Qt x CaO2 = [(Qt – Qs) x Cc’O2] + [Qs x CvO2]
22' CaOOCcQs −=
22' CvOOCcQt −

Causes of ShuntCauses of Shunt
• Physiologic shunts– Bronchial veins, pleural veins, p
P th l i h t• Pathologic shunts– Intracardiac
– Intrapulmonary• Vascular malformations
• Unventilated or collapsed alveoli

Normal shunt fractionNormal shunt fraction
• ~ 5 %
• Due to– Physiological shunt
– Gravity related V/Q mismatchy
• Contributes to A a D O• Contributes to A‐a D O2
– 10 – 15 mm hg

A a DOA a DO2
PAO2 ( l l ti ) t i l P O2• PAO2 (alveolar gas equation)‐ arterial PaO2
I t t ll ffi i t l it ith t h d V/Q• In a totally efficient lung unit with matched V/Q, alveolar and capillary PO2 would be equal
• Admixture of venous blood or V/Q scatter from low V/Q lung units will increase A a DO2V/Q lung units will increase A a DO2
• Increases ~ 3 mm hg every decade after 30 yrs of ageIncreases 3 mm hg every decade after 30 yrs of age

Shunt VS V/Q scatterShunt VS. V/Q scatter
C l l d h f i O• Calculated shunt fraction or A a DO2– Does not differentiate
• Response of pa O2 to increasing Fi O2
• V/Q scatter – Pa O2 increase with small increase in FiO2(.21‐.35)
• Pure shunt– Not much response p

MIGETMIGET
• 50 parallel gas exchange units characterized by VA‐Q ratio.
• Fit predicted PE & Pa to experimental data.
• Output: Ventilation and perfusion distributions.

Compensation of V/Q inequality ?Compensation of V/Q inequality ?
• ↑V/Q → local hypocapnia → ↑pH → local bronchoconstriction (↓V/Q )
• ↓V/Q → ↑CO → ↑ ventilation• ↓V/Q → ↑CO2 → ↑ ventilation– improves CO2 > O2 (dissociation curves)
• ↓V/Q → hypoxic pulmonary vasoconstriction

Points to remember
• Ventilation and Perfusion must be matched at the alveolar capillary
Points to remember
• Ventilation and Perfusion must be matched at the alveolar capillary level
• Most important cause of hypoxemia in most respiratory diseases• Most important cause of hypoxemia in most respiratory diseases
• V/Q ratios close to 1.0 result in alveolar PO2 close to 100 mmHg and PCO2 close to 40 mmHgand PCO2 close to 40 mmHg
• V/Q greater than 1.0 increase PO2 and Decrease PCO2. V/Q less than 1 0 decrease PO2 and Increase PCO2than 1.0 decrease PO2 and Increase PCO2
• Shunt and Dead Space are Extremes of V/Q mismatching.
• A‐a Gradient of 10‐15 Results from gravitational effects on V/Q and Physiologic Shunt