Embed Size (px)
DESCRIPTION
Citation preview

PK/PD analysis in assessment of abuse deterrence
Megan J. Shram, PhD
Director and Principal, Altreos Research Partners Inc.
Adjunct Professor and Lecturer, Department of Pharmacology, University of TorontoINC Research Consultant
ADF Science Meeting October 30 – September 1, 2013
Bethesda, MD

Acknowledgments
• Consultant to pharmaceutical and biotech companies
• Thank you to Purdue Pharma, LP for permission to present data on reformulated OxyContin® and OXN

Outline
• Background on PK/PD in abuse potential
• What is PK/PD relationship of opioids?
– Determinants of variation
• Application of PK/PD analysis in development of abuse-deterrent formulations (ADF)

Introduction
• Draft Guidance on Assessment of Abuse Potential of Drugs (January 2010):– “Characterization of the PK/PD properties of a…product is
important for determining the abuse potential of a…product.”
• Draft ADF guidance (January 2013):– “PK data should be collected to correlate with the PD
outcomes.”
– “The rate of rise of drug onset for the intact and manipulated potentially abuse-deterrent formulation should be given appropriate weight in the overall analysis of the abuse deterrent properties.”

Introduction
• Goal of PK/PD analysis is to assist in predicting the effect of a drug over time, in relation to exposure
• In terms of abuse, the relationship between rate of rise of [drug] and effect is considered important– Fast onset, short duration of action favors repeated self-administration
– Delaying onset, extending duration of action can reduce immediate reinforcing effect and need to take more drug
+++
--
+
++

Questions
• Can PK assist in predicting subjective response to opioid?
• How can one assess if change in PK profile will be enough to affect PD response?
• eg, partial defeat of the AD mechanism

System
• Age
• Gender
• Opioid experience
• Tolerance/Dependence
• Expectations
• Genetic variations
Pharmacodynamics(CV ≈50- >100%)
• Subjective effects• Miosis• Analgesia• Respiratory depression
• Adverse events
• Behavior
Pharmacokinetics(CV ≈30%)
• Opioid, Dose
• Formulation, Route
• BBB permeability
• ADME, protein binding
• Active metabolites
• Plasma vs. Effect site
• Arterial v venous sampling/timing
PK/PD: Determinants of Variation
??EndpointsAnalysis
Interpretation
CV=coefficient of variation

Assessing the link between opioid exposure
and results of a clinical abuse potential study
Recent ADF Examples

When PK/PD relationship might exist
• Physicochemical barrier– Resistance to manipulation for oral, IN and IV*
administration
• Prodrug– Must be cleaved systemically to liberate active moiety
– Deterrence from IN and IV administration, and possibly oral if limited by saturable process
• Delivery System– Modified drug delivery to reduce diversion via
multiple routes
*not generally feasible to administer manipulated product IV

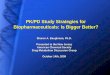
PK/PD of intranasally administered Reformulated OxyContin®
• 5-way crossover study in recreational opioid users with intranasal experience
– Coarse and fine ground OTR (30 mg)
– Positive controls: Oxy API and fine ground original OC (30 mg)
– Placebo control: lactose powder

Time course of effects
0
5
10
15
20
25
30
35
40
45
50
0 4 8 12 16 20 24
Pla
sma
oxy
cod
on
e (n
g/m
L)
Time post-dose (hr)
Oxycodone concentration
OTR fine
OTR coarse
OC
0
10
20
30
40
50
60
70
80
90
100
0 4 8 12 16 20 24D
rug
Liki
ng
VA
S (0
-10
0)
Time post-dose (hr)
Drug Liking VAS
OTR fine OTR coarse OC
Effects unrelated to drug exposure can impact experience (at the moment and overall)
Courtesy of Purdue Pharma; Perrino et al., 2012 CPDD; Harris et al., submitted

Rate of Rise: “Abuse quotient”
• Lower Cmax and longer Tmax lower Abuse Quotient
0
20
40
60
80
100
120
140
160
180
200
Cmax/Tmax
OTR fine
OTR coarse
OC
Oxy API
0
20
40
60
80
100
120
140
160
180
200
Emax/TEmax
OTR fine
OTR coarse
OC
Oxy API
Drug Liking Visual Analog ScaleOxycodone Pharmacokinetics
Data courtesy of Purdue Pharma

Exposure-Response Relationship
• For reformulated OxyContin®, delaying and lowering Cmax had significant impact on liking
• But if PK “drives” PD, what is concentration-effect relationship?

PK/PD Correlations: Subjective Effects
y = 0.5386x + 54.143R² = 0.0518
0
10
20
30
40
50
60
70
80
90
100
0 20 40 60 80 100
Dru
g Li
kin
g V
AS
(0-1
00)
Plasma oxycodone concentration (ng/mL)
OTR finey = 0.6612x + 44.435
R² = 0.1077
0
10
20
30
40
50
60
70
80
90
100
0 20 40 60 80 100
Dru
g Li
king
VA
S (0
-100
)
Plasma oxycodone concentration (ng/mL)
OTR coarse
0
10
20
30
40
50
60
70
80
90
100
0 20 40 60 80 100
Emax
of
Dru
g Li
kin
g V
AS
(0-1
00)
Cmax of oxycodone (ng/mL)
Overall R2=0.12y = 0.2782x + 72.519
R² = 0.0602
0
10
20
30
40
50
60
70
80
90
100
0 20 40 60 80 100
Dru
g Li
king
VA
S (0
-100
)
Plasma oxycodone concentration (ng/mL)
OC fine
Derived Parameters By Timepoint
Data courtesy of Purdue Pharma

PK/PD Correlations: Physiological Effects
y = -0.0509x + 5.3132R² = 0.1486
0
1
2
3
4
5
6
7
8
0 20 40 60 80 100
Pup
il si
ze (
mm
)
Plasma oxycodone concentration (ng/mL)
OTR fine
y = -0.0586x + 5.7401R² = 0.3608
0
1
2
3
4
5
6
7
8
0 20 40 60 80 100
Pupi
l siz
e (m
m)
Plasma oxycodone concentration (ng/mL)
OTR coarse
y = -0.0249x + 4.4345R² = 0.2132
0
1
2
3
4
5
6
7
8
0 20 40 60 80 100
Pupi
l siz
e (m
m)
Plasma oxycodone concentration (ng/mL)
OC fine
0
1
2
3
4
5
6
7
8
0 20 40 60 80 100
MP
C (
mm
)
Cmax of oxycodone (ng/mL)
Overall R2=0.27
Derived Parameters By Timepoint
Data courtesy of Purdue Pharma

When PK/PD might matter less
• Opioid agonist-antagonist combinations– Antagonist attenuates/reverses effect of opioid
– Does PK of antagonist help predict response to agonist?
• Aversion– Aversive agent not intended to impact exposure to
agonist
– PK would NOT predict overall response to ADF
– Might still experience high from opioid; however, product not liked

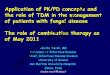
PK/PD of intranasally administered OXN
• 3-way crossover study in recreational opioid users with intranasal experience
– Crushed OXN 40/20 mg (oxycodone/naloxone)
– Positive control: Oxy API 40 mg
– Placebo control: lactose powder

Time course of effects
Data courtesy of Purdue Pharma
0
10
20
30
40
50
60
70
80
90
100
0 4 8 12 16 20 24
Pla
sma
oxy
cod
on
e (n
g/m
L)
Time post-dose (hours)
Plasma Concentration
Naloxone (ng/mL)
Oxy API - Oxycodone
OXN - Oxycodone
• At 2:1 ratio, OXN significantly reduces Drug Liking to placebo-like levels
• Rate of rise: “Abuse Quotient” (Cmax/Tmax) not applicable to opioid agonist-antagonist combinations, such as OXN
0
10
20
30
40
50
60
70
80
90
100
0 4 8 12 16 20 24
Dru
g Li
kin
g V
AS
(0-1
00
)
Time post-dose (hours)
Drug Liking VAS
OXN
Oxy API
Placebo

Antagonist PK – Agonist PD
• Highly variable concentrations and lack of concentration-effect relationship of to-be-marketed formulation
• Relationship between antagonist PK and agonist PD typically evaluated earlier in development in dose-ranging trials – ie, dose-effect
Data courtesy of Purdue Pharma
y = 0.15x + 47.987R² = 0.008
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 25 30 35
Dru
g Li
kin
g V
AS
(0-1
00
)
Plasma naloxone concentration (ng/mL)

Conclusions
• Relationship between PK and PD of abuse potential is weak and highly variable
• Effects unrelated to opioid exposure impact subject’s experience
• Clinical PD study necessary to determine potential for abuse (or its deterrence)
• PK alone cannot be used as substitute in abuse potential assessment