Embed Size (px)
Citation preview


Pituitary Surgery Needs Long Term Follow Up
Presented byDr. Abhijit Chowdhury
HMO (Dept. of Endocrinology)

DEMOGRAPHIC DETAILS
Name : Mrs. XAge : 60 years Sex : FemaleMarital status : Widow Occupation : Home makerReligion : IslamAddress : Rampura, Dhaka
Date of admission : 2nd February 2015

Increased frequency of micturition for 07 days.
Fever and headache for 10 days. Low back pain for 08 years.
Presenting Complaints

History of present illness
The patient is a known case of Acromegaly (Post-operative post-radiotherapy state), and is on thyroid replacement therapy. According to her son, she was relatively well o7 days back then she gradually developed increased frequency of micturition which was associated with burning sensation and occasional lower abdominal pain. Initially the frequency was 8 - 10 times a day but for the last 2 days it increased to 15 - 20 times a day and 5 times or more at night. Her urine is high colored but there is no frank blood.

History of present illness (Cont.)
She had been suffering from high grade fever with chills and rigor for last 10 days. Maximum recorded temperature was 1030F which subsided after taking Tab. Paracetamol 500 mg orally. She was also suffering from headache which was mild, dull aching, global, aggravated by coughing and relieved after taking analgesic but not associated with vomiting or visual disturbance.

History of present illness (Cont.) She is suffering from low back pain for last 8
years. The pain is constant throughout the day which is stabbing in nature, non-radiating, increases by movement and has no obvious relieving factor. For the back pain she never consulted any doctor. She is suffering from Type: 2 DM for 20 years for which she was initially on OAD (Metformin). Later she switched to subcutaneous Insulin therapy for better control. Currently her blood glucose is well maintained only by medical nutrition therapy (MNT). She is hypertensive for 15 years for which she is on regular anti-hypertensive medication.

History of present illness (Cont.) She suffers from occasional constipation. Her
appetite is normal and sleeping pattern is disturbed due to frequent micturition at night.
She has no visual disturbance. For the above complaints she got admitted to
BIRDEM General Hospital under Dept. of Endocrinology for better management.

History of past illness
The patient presented with features of Acromegaly and
diagnosed as a case of pituitary macroadenoma in 1994.
Pituitary surgery (Trans-ethmoidal pituitary ablation from left side) was done in 1995 at BSMMU. Histopathology revealed pituitary adenoma.
She completed 2 cycles of radiotherapy in 1996 as advised.

Treatment History
Tab. Levothyroxine (50 mcg)- 1+0+0.Tab. Metoprolol (50mg)- 1+0+1.Tab. Calcium Carbonate- 0+1+0.Tab. Alendronic Acid + Vitamin D3
(70/2800) was given for 6 months in 2013 ( 1 Tab weekly).
Inj. Zolendronic Acid (5mg/100ml) was given on 30.05.2012.
Tab. No history of drug allergy.

Family history
Both of her parents were diabetic. Her father died due to RTA and mother died from cardiac disease.
She has two brothers and three sisters, all of them are alive and apparently healthy.
She is blessed with one son and two daughters, all of them are apparently healthy.

Personal history
No H/O smoking, alcoholism or illicit drug use.
She maintains her personal hygiene properly.She drinks arsenic free tube well water.Washes her hands with soap.Uses sanitary latrine.

Immunization History
Patient was not completely immunized.

Socioeconomic History
She is from low socioeconomic status.

Menstrual History
Postmenopausal- 20 years back after pituitary surgery.

General ExaminationAppearance Depressed, Pallor, Coarse face, Mild enlargement of lips and nose.Decubitus On choiceIntelligence Normal Co operation Co operativeBody built NormalNutrition Over weight (BMI:
29.82%)Height 151 cmWeight 68 kg


Anaemia MildJaundice Not presentCyanosis Not present Oedema Not present Dehydration Mild Koilonychia Not presentLeukonychia Not present Neck vain Not engorgedThyroid Not enlarged
Pulse 86 beats/mint

BP 120/80 mm HgPulse 110/min; RegularRR 16/minTemp. 1010 FSkin Cond. Thick and greasyPigmentation Not presentLymph nodes: Not palpable

Systemic Examination
Alimentary System
Oral cavity and tongue:• Large tongue.• Gaps between teeth of both jaws.


Abdominal Examination:Inspection- Shape - Normal. Flanks – Full. Umbilicus – Central and inverted. Palpation- Abdomen was soft but mild tenderness present in
hypogastrium. Loin tenderness- absent. Liver ,spleen- Not palpable. Kidneys – Not ballotable.Percussion – Tympanic all over the abdomen.Auscultation- Bowel sound present.

Musculoskeletal System
Hands and feet- Broaden.Fingers- Spade-like and doughy
feeling on palpation.Palpation of the spine- Normal
curvature maintained and tenderness absent.



Nervous system•Higher cerebral function- Normal.
•Cranial nerve examination- Optic nerve- Visual acuity- 6/9 in both eyes. Field of vision- Intact. Color vision- Intact Ophthalmoscopic examination- NPDR(B/E) •Other cranial nerves examination reveals no abnormality

•Motor function Test Bulk of the muscle- Normal. Tone- Normal. Movement and strength- Normal.
•Examination of reflexes- All jerks are normal.
•Examination of Sensory System- Intact.
•Co-ordination of movement- Normal.
•Gait- Normal.

Cardiovascular System
Inspection-Palpation- No abnormality.Percussion-Auscultation

Respiratory System
Inspection- Palpation- No abnormality. Percussion- Auscultation

Salient feature
Mrs. X, 60 years old lady known case of Acromegaly (Post-operative post-radiotherapy state), hypothyroidism (on replacement), DM (on MNT) and hypertension (on antihypertensive drug) hailing from Rampura, Dhaka admitted to BIRDEM on 2nd February 2015 with the complaints of increased frequency of micturition for 07 days, fever with headache for 10 days and low back pain for 8 years.

Salient feature(Cont.)
On Examination, she had Acromegalic features. She was
mildly anaemic, mildly dehydrated with depressed look.
Her Pulse- 110/min, BP- 120/80 mm of Hg, Temp- 1010 F. Skin was thick and greasy. Abdominal examination revealed mild tenderness in hypogastrium. Her Field of vision was intact and ophthalmoscopic examination revealed NPDR. All other systemic examinations revealed normal findings.

Provisional DiagnosisAcromegaly (Status post-operative post-radiotherapy) ? RecurrenceUTIHypothyroidismDiabetes MellitusHTNEarly menopauseOsteoporosisNPDR (B/E)

Investigations CBC Hb%-10.3 gm/dl ESR-26 mm in 1st hour TC-11,030/mm3 of blood DC- N: 75%, L-20%,E-01%, M-
04% Urine R\E Pus cells- 10 to 15/HPF RBC- 1 to 2/ HPF Epithelial Cells- 1 to 2/ HPF

Urine C/S
Group B Streptococcus growth.
Sensitive to Ampicillin, Nitrofurantoin, Ciprofloxacin
and Vancomycin.
Serum Creatinine- 1.1 mg/dl

Hormone analysis• GH- 0.37 ng/ml (o.o5-5.0 ng/ml)• S. Prolactin -333 mIU/L (Postmenopausal:
38.0-430.omIU/ml)• S. FSH- 3.90 mIU/ml
(Postmenopausal:26.72-133.41 mIU/ml) • S. TSH- 0.4 mIU/ml (Adult: 0.47- 5.01
uIU/ml)• FT4 - 15.79 pmol/L with 50 micro gm.
Levothyroxine. (9.14-23.18 pmol/L)

Synacthen Test
Basal cortisol - 96.30 nmol/L (101.2-690 nmol/L)
ACTH- 11 pg/ml (8.3-57.8pg/ml)

HbA1C- 7%; FBS- 4.0 mmol/L; 2HABF- 5.0mmol/L USG of W/A– Fatty change in liver.CXR P/A view- Normal.ECG- Normal.Serum Calcium- 9.3 mg/dLSerum Albumin- 41.7 g/dLSGPT- 17 IU/L; SGOT- 15 IU/L; Total
Billirubin- 0.4 mg/dL

Lipid ProfileCholesterol- 221 mg/dlHDL- 47 mg/dlLDL- 148 mg/dlTG- 132 mg/dlSerum ElectrolytesNa+ : 137 mmol/LK+ : 5.0 mmol/LCl- : 100 mmol/LPCO2: 28 mm Hg

X-ray Skull (L/V)
Sella turcica is enlarged.

MRI of the brain (Sella & Para Sellar region)
• No definite pituitary gland is seen and pituitary fossa is completely filled with CSF.
• Bilateral ethmoidal, sphenoidal and left maxillary sinusitis.

MRI of the brain (Sella & Para Sellar region)

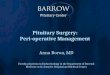
X-ray Dorso-lumbar Spine (B/V)
-Lumbar Spondylosis.-Bones are osteopenic.-Collapse of D12 vertebra.

MRI of Lumbar Spine
-Compression collapse of D 12 vertebra.
-Disc protrusion causing thecal indentation and foraminal narrowing at L4-L5 and L5-S1 level.
-Bailateral L4 and L5 nerve root compression.

Bone Mineral Density (BMD)
Osteopenia
T Score Left Femur: -1.12 Lumbar Vertebrae: -1.83

Final Diagnosis
Empty Sella with Panhypopituitarism ( ACTH, TSH, FSH)Acromegaly (Status post-operative post-radiotherapy)UTIDiabetes MellitusHTNOsteoporotic fracture of D12 vertebraNerve roots compression at L4-L5 & L5-S1 levelSinusitisNPDR (B/E)

Rx during hospital stayInfusion Normal Saline.Inj. Ciprofloxacin (200 mg) for 1 week.Inj. Hydrocortisone (100mg) 12 hourly for 5
days followed by Tab. Prednisolone (5 mg)- 1+0+1/2 continue.Inj. Zolendronic Acid (5mg/100ml) was given
on o9.02.2015.Tab. Levothyroxine (50 mcg)- 1+0+0 (B/M)

Tab. Metoprolol (50mg)- 1+0+1.Tab. Atorvastatin (10 mg)- 0+0+1 (B/M)Tab. Amoxicillin+Clavulanic Acid (1gm)-
1+0+1 Tab. Calcium Carbonate (500mg)- 1+0+1Cap. Esomeprazole (20mg)- 1+0+1 (B/M)Tab. Domperidone (10mg)- 1+1+1 (B/M)Lactulose Syrup.Tab. Paracetamol (500mg)- 1+1+1 (A/M);
when fever > 1010F.Oxymetazoline Nasal Spray- 5 days.

Rx during dischargeThe patient was discharged on 12.02.2015 with advice. Tab. Levothyroxine (50 mcg)- 1+0+0 (B/M)- Cont. Tab. Prednisolone (5 mg)- 1+0+1/2 - 10 days (A/M) 1+0+0 - 10 days ½+0+0 - Cont. Tab. Metoprolol (50mg)- 1+0+1 - Cont. Tab. Atorvastatin (10 mg)- 0+0+1 (B/M) - Cont. Tab. Amoxicillin+Clavulanic Acid (1gm)- 1+0+1 (2 weeks) Tab. Ciprofloxacin (500mg)- 1+0+1
(2 weeks) Tab. Calcium Carbonate (500mg)- 1+0+1 - Cont. Cap. Esomeprazole (20mg)- 1+0+1 (B/M) - 1 month. Salmon Calcitonin Nasal Spray- In alternate nostril daily at night- 3 months. Lactulose Syrup. Menthol vapour inhalation.

Follow up
•Patient was properly counseled and advised for follow up after 2 weeks.•Steroid card was provided.