Embed Size (px)
Citation preview
Tasmania’s unique eMM journey –progress, achievements and lessons
from a whole-of-state approach
Peter FowlerClinical Lead, State-wide Medication Management Projects, DHHS

Unique Tasmania
Tasmania’s approach to eMM
A system overview
Some major / key achievements
Lessons learned
Tasmania’s unique eMM journey
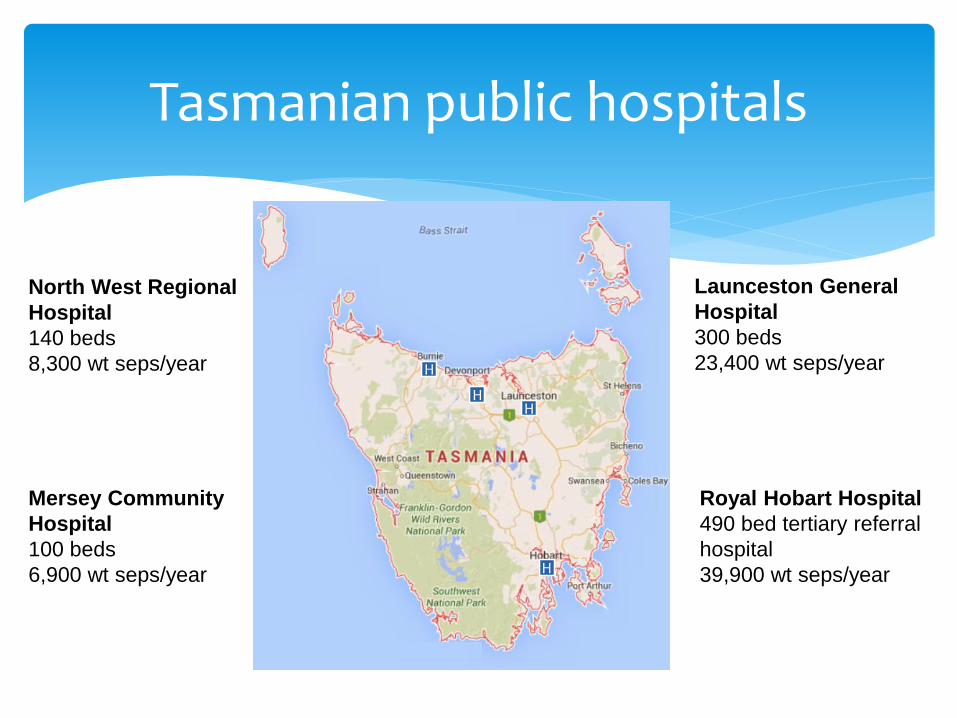
Tasmanian public hospitals
Launceston General
Hospital
300 beds
23,400 wt seps/year
Royal Hobart Hospital
490 bed tertiary referral
hospital
39,900 wt seps/year
North West Regional
Hospital
140 beds
8,300 wt seps/year
Mersey Community
Hospital
100 beds
6,900 wt seps/year
H
HH
H
Start in 2007 – now have substantial eMMfunctionality across the state
Modular expansion – discrete elements of functionality
State-wide implementations
Relatively low cost – no budget for large programs
Project-based funding approach
Tasmania's approach to eMM
Projects teams include both IT and clinical staff – recent projects have used pharmacists as clinical lead and trainers
Run old systems with the new for a time
Expanding to primary health sites
Local vendor (HealthCare Software – Clinical Suite)
Tasmania's approach to eMM
State-wide eMM functionality

Prior to admission
medication historyOutpatient
consultation summaries
Outpatient prescriptions
Discharge summaries &
procedure reports
Medication reconciliation at discharge
Medication counselling
sheets
Discharge prescriptions
Medication reconciliation
& meds management
plan
eCharts -Inpatient
prescribing & admin.
• Patient lists andworkflow and task management
• Importation of dispense details• Notes and messages to other care
providers (Drs, RNs, Allied Health) • Drug allergy recording and checking
• Drug interaction checking• Duplicate therapy checking• Clinic workflow management
• Dispensary workflow management andprescription tracking
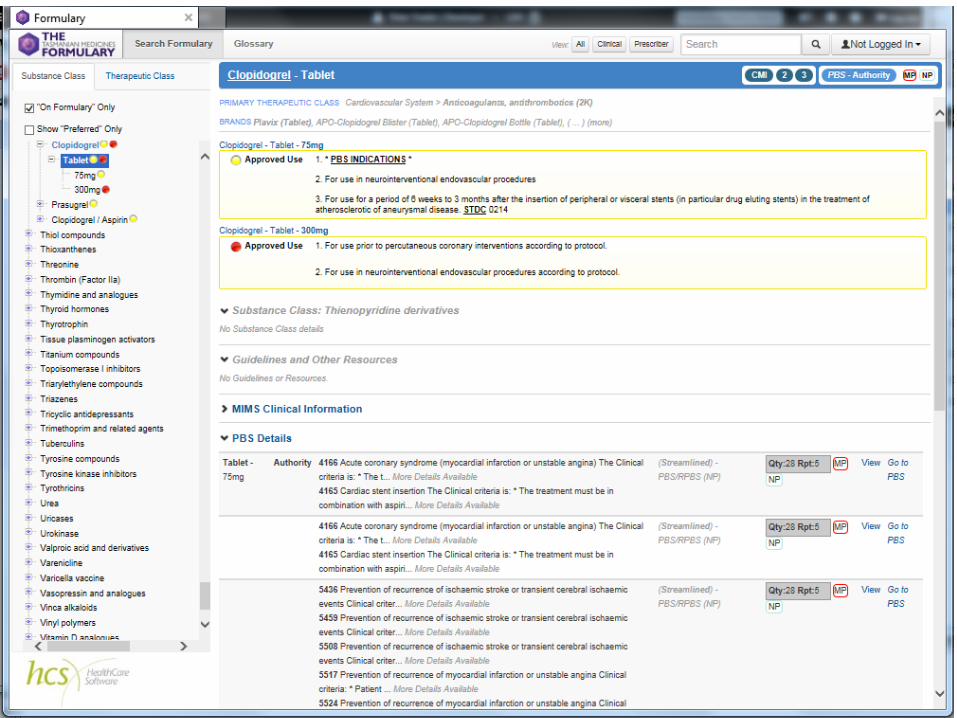
• Links to knowledge sources (e.g. PBS, Formulary, DORA, AMH)• Standard terminologies (AMT V3, SNOMED-CT)• Discharge and OP consultation summaries to GPs
and other nominated recipients• Discharge summaries to DMR & MyHR• Labs on discharge summaries to MyHR
• Visibility and management of MyHR consent• Prescribe and dispense messaging
to NPDR• NPDR viewing
Rx
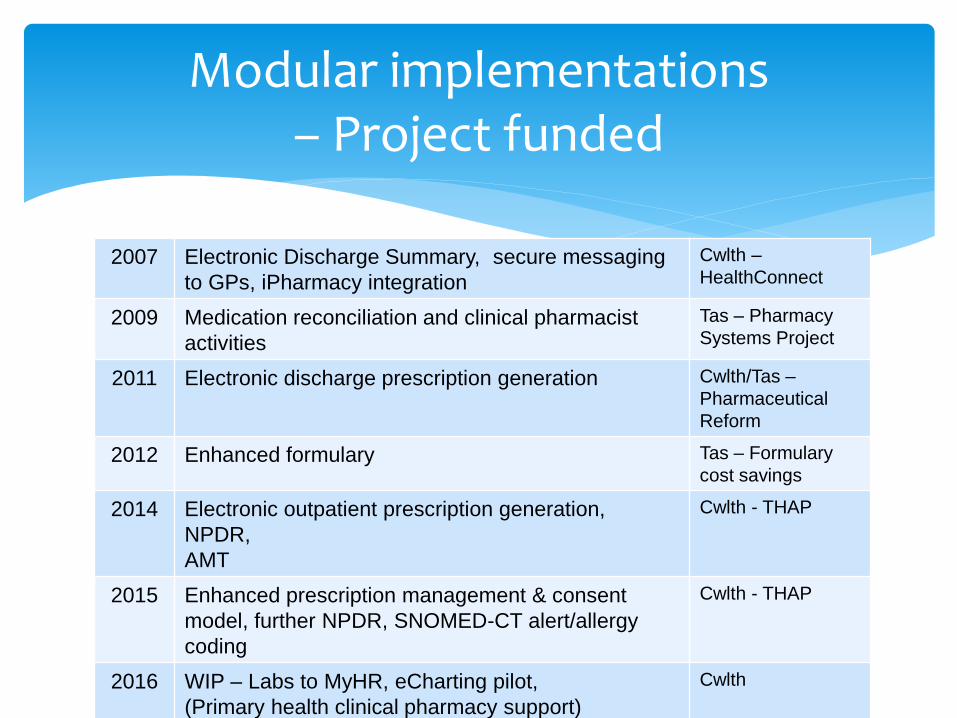
Modular implementations – Project funded
2007 Electronic Discharge Summary, secure messaging
to GPs, iPharmacy integration
Cwlth –
HealthConnect
2009 Medication reconciliation and clinical pharmacist
activities
Tas – Pharmacy
Systems Project
2011 Electronic discharge prescription generation Cwlth/Tas –
Pharmaceutical
Reform
2012 Enhanced formulary Tas – Formulary
cost savings
2014 Electronic outpatient prescription generation,
NPDR,
AMT
Cwlth - THAP
2015 Enhanced prescription management & consent
model, further NPDR, SNOMED-CT alert/allergy
coding
Cwlth - THAP
2016 WIP – Labs to MyHR, eCharting pilot,
(Primary health clinical pharmacy support)
Cwlth
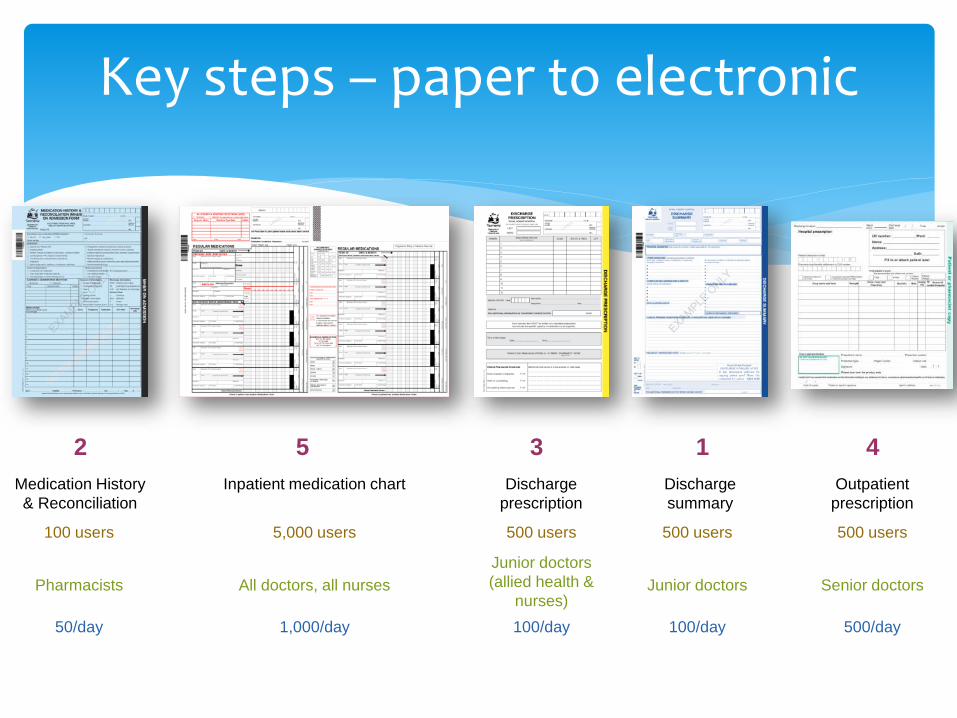
Medication History
& Reconciliation
Inpatient medication chart Discharge
prescription
Discharge
summary
Outpatient
prescription
12 3 45
100 users 5,000 users 500 users 500 users 500 users
Pharmacists All doctors, all nurses
Junior doctors
(allied health &
nurses)Junior doctors Senior doctors
50/day 1,000/day 100/day 100/day 500/day
Key steps – paper to electronic

Alignment with investment priorities of CEOs (& DHHS and Cwlth)
Creating the value proposition for key users, esp. doctor (Med Rec benefits discharge prescribing then discharge summaries)
The vendor and product development
Determining priorities
Pros and cons of modular approach
Affordable
Work to clearly defined endpoints
Increasing user familiarity makes subsequent implementations easier
Always looking for $$ for the next stage
Projects targeted to funding objectives – not always local priority
Support requirements expand continuously
Duplicate systems for some time
Pros Cons

System overview
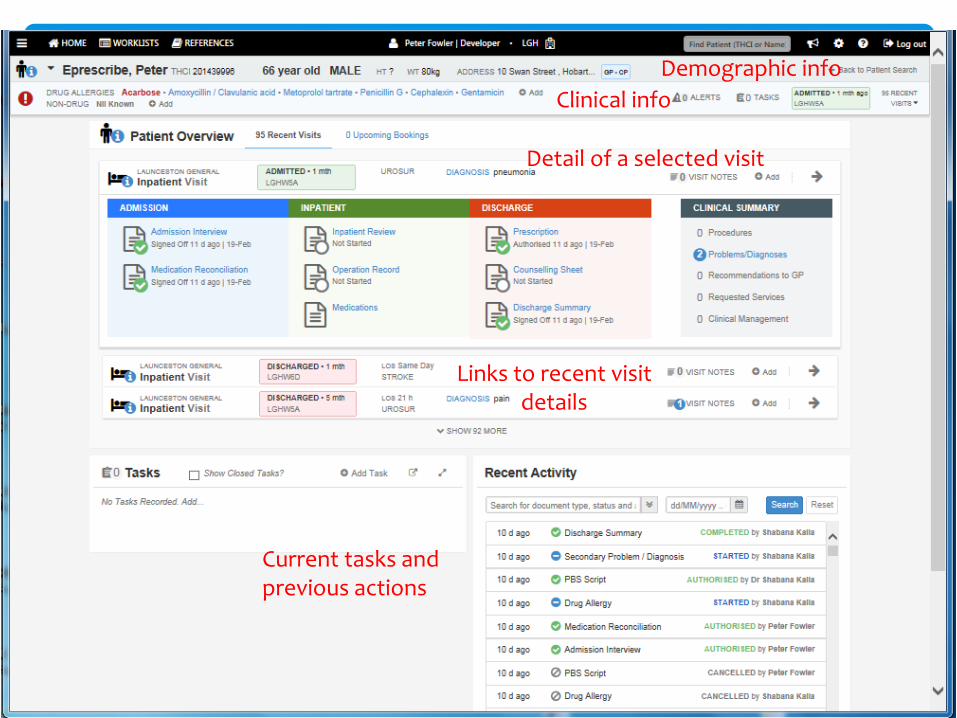
Demographic info
Clinical info
Detail of a selected visit
Links to recent visit details
Current tasks and previous actions

Detail of a current visit
Hover-over
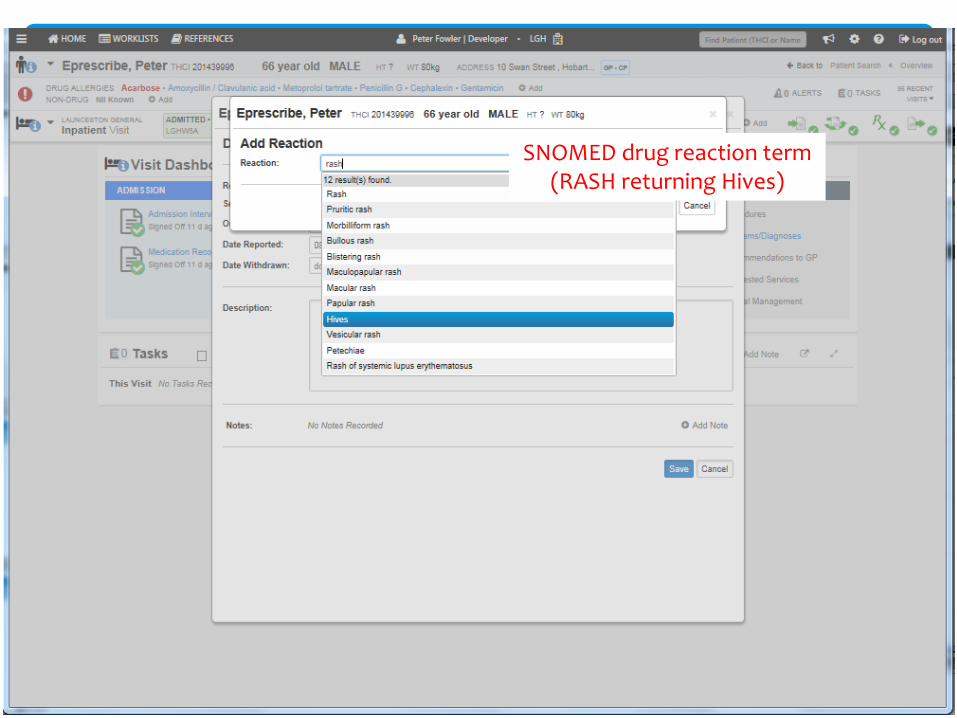
SNOMED drug reaction term(RASH returning Hives)
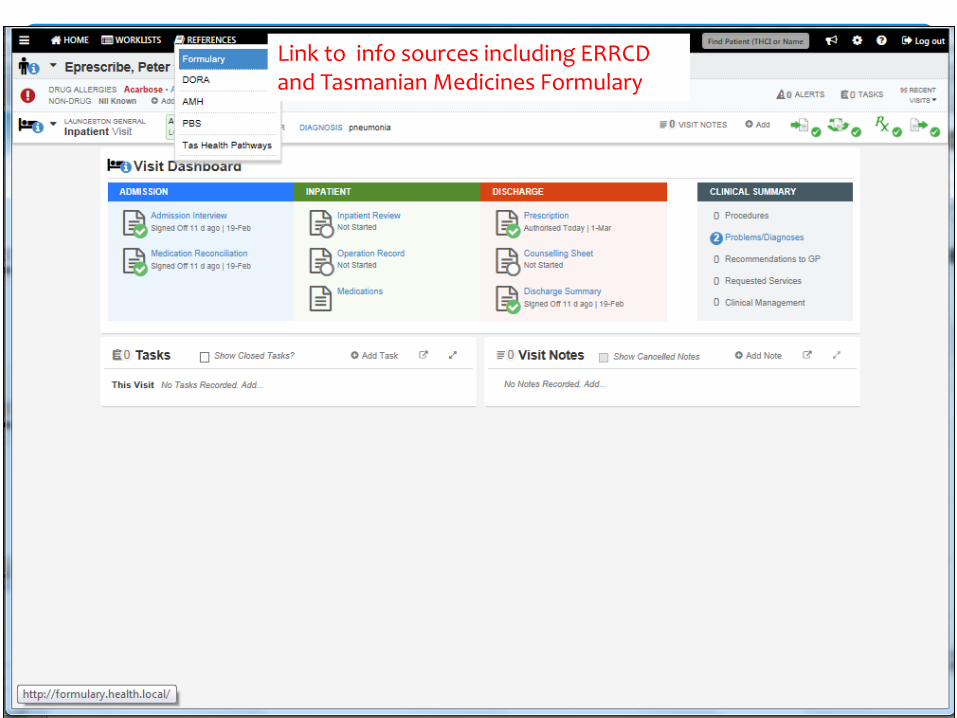
Link to info sources including ERRCD and Tasmanian Medicines Formulary
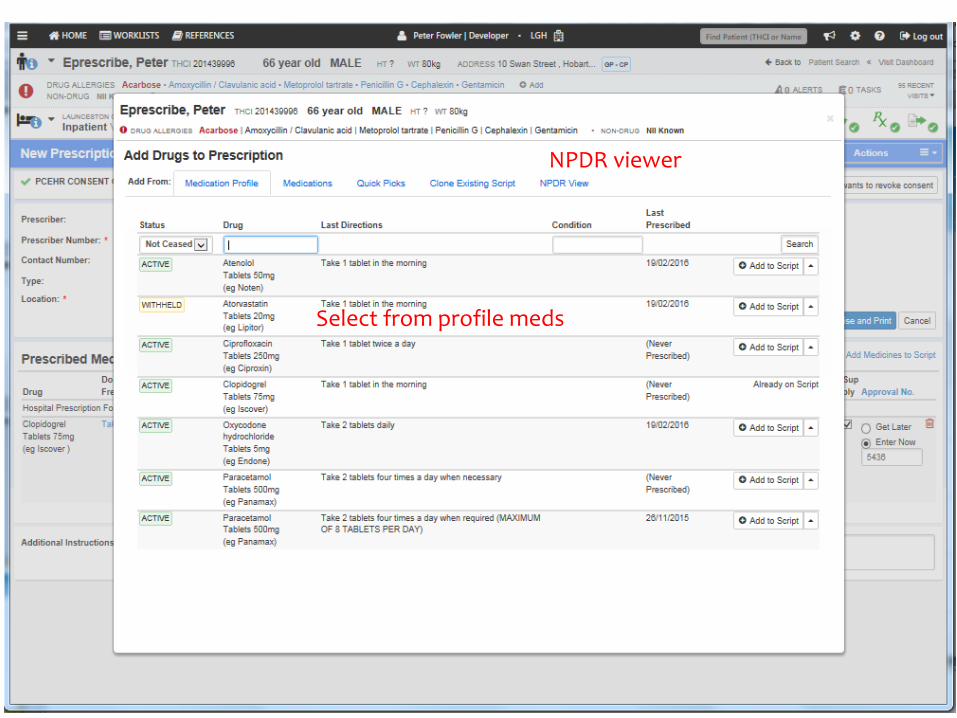
Select from profile meds
NPDR viewer
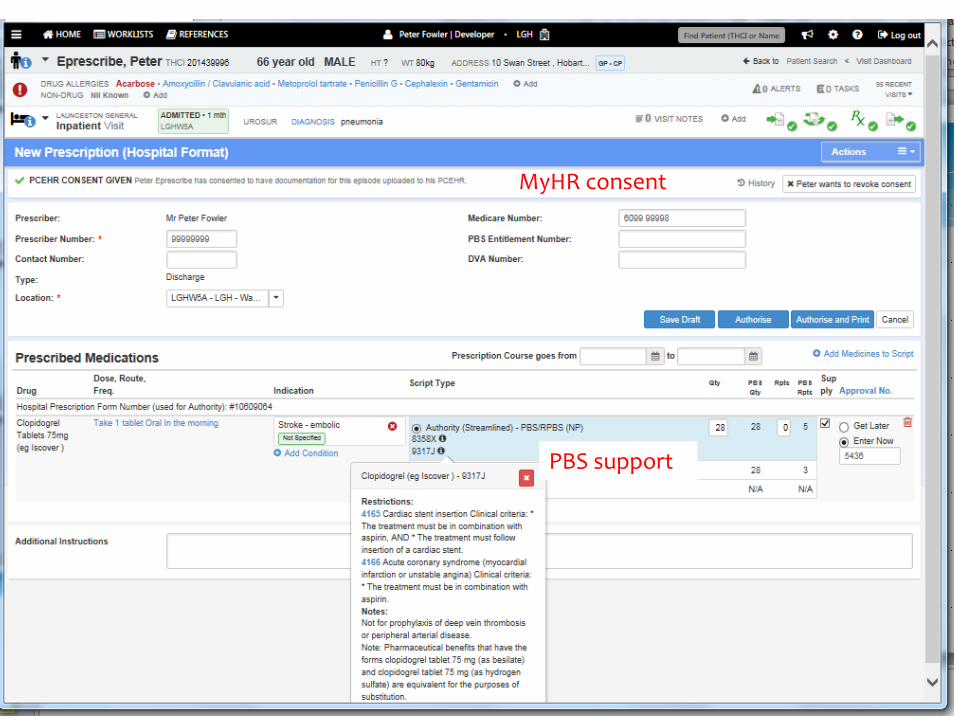
MyHR consent
PBS support
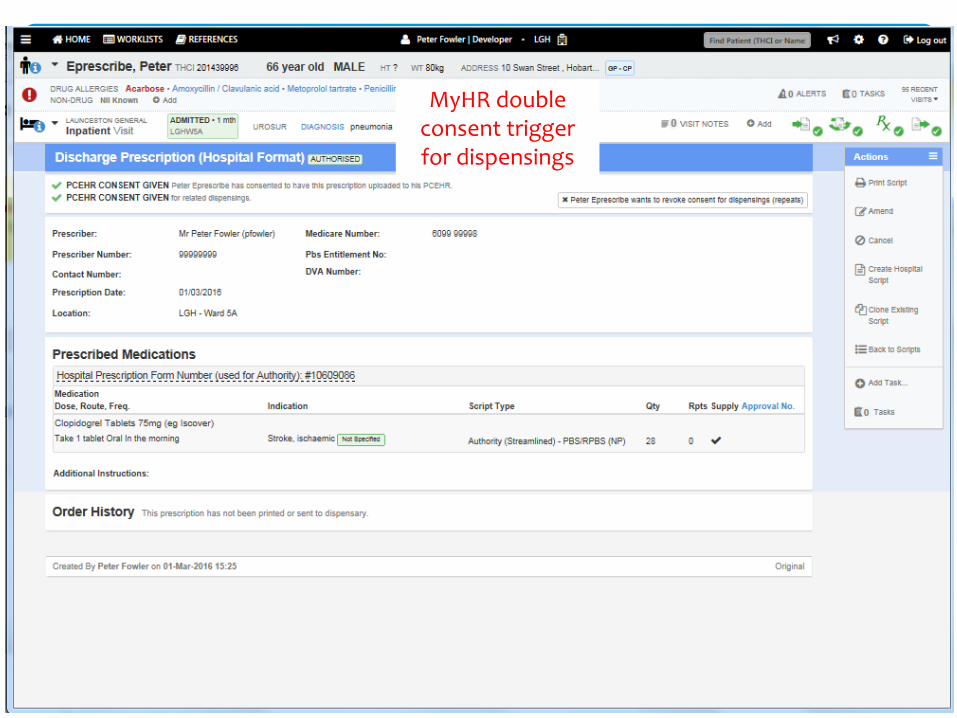
MyHR double consent trigger for dispensings
MyHR integration:
Discharge summaries
Prescriptions and matched dispensings to NPDR
Robust consent model
Standard terminology
SNOMED-CT – Drug reaction terms
AMT v2 – AMT v3
Outcomes and key achievements
HCS-CS derives product file from MIMS
Pack size, PBS and TGA information
AMT coding to TPP level
Medicines linked: iPharmacy HCS-CS MIMS AMT
Simplified NPDR integration: one system (HCS-CS) for prescribe and dispense details and consent status
AMT V3

Outcomes
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre reform 6/11 11/11 5/13 5/14 5/15
All sites - Transfer of patient information to GP – High risk patients
All inpatient admission meds histories and med reconciliations are recorded electronically
Approx. 40% of outpatient and almost all discharge prescriptions are generated electronically
Electronically generated prescriptions are dispensed 33% faster than hand-written prescriptions
NPDR integration – prescriptions and dispensings
Incorporation of standard terminologies (AMT V3 & SNOMED-CT)
Outcomes
Pathology results in discharge summaries to MyHR(different pathology systems in south, north and northwest – state-wide implementation), first go-live March 2016
Pilot of eCharting and administration
Next Steps – work in progress
Challenges and risks:
Gradual implementation leads to increasing support requirements – not provided by project-funded model
Finding funding for the next stage
Who owns the system? (a shared vision)
Inpatient charting (key component) not clinically tested / validated.
Lessons learned
Modular approach has enabled Tasmania to incrementally invest in eMM capability – with advantage and disadvantage
Vendor has developed eMM capability aligned with PBS, NEHTA and local requirements
MyHR / NPDR integration achieved including AMT v3 through MIMS
SNOMED-CT for drug reaction terms
Tasmania has made significant progress towards paperless, closed-loop medication management
Conclusion






























