Embed Size (px)
Citation preview

Personalizing Treatment Choice
International MS Physician Summit Prague, 22nd-23rd March 2014
Gavin Giovannoni
Barts and The London

Disclosures
Professor Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical trial design, trial steering committees and data and safety monitoring committees from: Abbvie, Bayer-Schering Healthcare, Biogen-Idec, Canbex, Eisai, Elan, Fiveprime, Genzyme, Genentech, GSK, GW Pharma, Ironwood, Merck-Serono, Novartis, Pfizer, Roche, Sanofi-Aventis, Synthon BV, Teva, UCB Pharma and Vertex Pharmaceuticals.
Regarding www.ms-res.org survey results in this presentation: please note that no personal identifiers were collected as part of these surveys and that by completing the surveys participants consented for their anonymous data to be analysed and presented by Professor Giovannoni.
Professor Giovannoni would like to acknowledge and thank Biogen-Idec, Genzyme and Novartis for making available data slides on natalizumab, alemtuzumab and fingolimod for this presentation. I would like to acknowledge Mark Hughes, from Infusion, who helped me prepare some of my slides. Please note that Professor Giovannoni’s attendance at the 2014 MS Physician Summit, in Prague, was sponsored by Biogen-Idec.

Therapeutic Ideal
Reliable
long-term efficacy
Maintaining
QOL
Maintaining
independence
Maintaining the
ability to work
No issue for
pregnancy/fertility
Maximum reduction
of MS disease activity
Maximum
tolerability
Maximum
safety
Ease of use
Minor impact on
everyday life
QOL=quality of life.

Moving from Compliance to Concordance Requires a Culture Change
Concordance model Compliance model
Prescriber decides
diagnosis and treatment
Prescriber’s task is to
explain and instruct
Patient’s task is to
comprehend
Successful outcome is
compliance
Prescriber and patient negotiate
diagnosis and treatment
Prescriber elicits, explains,
persuades, and accommodates
Patient explains, considers, and
accommodates
Successful outcome is a
negotiated agreement
Royal Pharmaceutical Society of Great Britain. From compliance to concordance: achieving shared goals in medicine taking. London, 1997.

Canada: Deciding on an MS Treatment
Available from: mssociety.ca/en/pdf/EYO-ENG-web-2012.pdf. Accessed 13 March 2014.

Canada: Deciding on an MS Treatment
Available from: mssociety.ca/en/pdf/EYO-ENG-web-2012.pdf. Accessed 13 March 2014.

UK: Deciding on an MS Treatment
www.msdecisions.org.uk. Accessed 26 February 2014.

UK: Deciding on an MS Treatment
www.msdecisions.org.uk. Accessed 26 February 2014.

Compliance Model
“Trust me.
I am the
doctor”

Where are you on the diffusion curve?
Giovannoni G et al. Lancet Neurol. 2006;5:887-894.

Patient FAQs Regarding the Impact of Therapy on Daily Life
• What is MS?
• Are you sure that I have MS?
• What type of MS do I have?
• What prognostic group do I fall into?
• What is the risk of not being treated with a DMT?
• Do I have active MS?
• Am I eligible for treatment with a DMT?
• Do you understand the difference between the treatment strategies of maintenance-and-escalation and induction therapy?
• Do you understand the concept of treat-2-target of no evident disease activity (NEDA)?
• What about pregnancy?
FAQ=frequently asked question; MS=multiple sclerosis; DMT= disease modifying therapy.

Question: What prognostic group do you fall into?
Good prognosis Poor prognosis
Young
Female sex
“Unifocal”onset
Isolated sensory symptom (optic
neuritis, sensory)
Full recovery from attack
Long interval to second relapse
No disability after 5 years
Normal MRI findings/low lesion load
No posterior fossa lesions
No brain atrophy
CSF negative for OCBs
Older age of onset
Male sex
“Multifocal“onset
Efferent system affected (motor, cerebellar,
bladder)
Partial or no recovery from a relapse
High relapse rate in the first 2 years
Disability after 5 years
Abnormal MRI findings with large lesion load
Posterior fossa lesions
Brain atrophy
CSF positive for OCBs
Genomic factors (eg, ApoE4)
MRI=magnetic resonance imaging; CSF=cerebrospinal fluid; OCB=oligoclonal bands; Apo=apolipoprotein.
Adapted from Miller D et al. Lancet Neurol. 2005:4;281-288.

0
10
20
30
40
50
60
70
80
0 5 10 15 20
Pa
tie
nts
Co
nve
rtin
g t
o EDSS≥3.0(%)
Years
0 Lesions
1–3 Lesions
4–10 Lesions
>10 Lesions
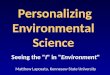
The data presented for years 5, 10, 14, and 20 were obtained from different publications based on the same longitudinal study.
The exact relationship between MRI findings and the clinical status of the patient is unknown. EDSS=Expanded Disability Status Scale.
Fisniku LK et al. Brain. 2008;131:808-817; Morrissey SP et al. Brain. 1993;116:135-146; O’Riordan JI et al. Brain. 1998;121:495-503;
Brex PA et al. N Engl J Med. 2002;346:158-164.
Baseline Number of Brain Lesions Predicts Progression to EDSS ≥3.0
Queen Square Study

Question: What prognostic group do you fall into?
Favourable
Indeterminate
Poor
time Aim of
treatment Giovannoni G. Barts & The London, UK, February 2014.

Question: What prognostic group do you fall into? Potential Consequences of the Disease

Question: Do You Have Active MS?
vs
1
2
3
Clinical
MRI
Biomarkers Giovannoni G. Barts & The London, UK, February 2014.

Treatment Selection
The individual MS patient: • MS prognosis • Life style and goals • Your goals for therapy
Individual MS patient’s measures: • Evidence of disease activity? • Tolerability/safety? • Adherence? • Drug or inhibitory markers?
Therapy: • Maintenance vs induction
• Moderate efficacy (1st-line) • Intermediate efficacy (2nd-line) • High-efficacy (3rd-line)
Monitoring: • Clinical
• Relapse • Disability progression • Risk profile for serious adverse events
• MRI • T2 & T1-Gd • Brain atrophy
• Biomarkers • NAbs • CSF neurofilament Gd=gadolinium; NAb=neutralising antibody.
Giovannoni G. Barts & The London, UK, February 2014.
Define the individual
MSpatient’sdisease
Treatment failure?
yes
no
Choose therapy
Monitoring
X Y Z

General Treatment Philosophy in 2008
Moderate
Efficacy
High
Efficacy
A
B
C
D
E
Giovannoni G. Barts & The London, UK, February 2014.

Increasing Choice: the Escalation Ladder
Moderate
Efficacy
Intermediate
Efficacy
High
Efficacy
Giovannoni G. Barts & The London, UK, February 2014.

A Conservative Alternative or, If Time=Brain, Is It Dangerous?
CO-CZ-0056b
N M
Y X Moderate
Efficacy
Intermediate
Efficacy
High
Efficacy
A
B
C
D
E
Giovannoni G. Barts & The London, UK, February 2014.

MS is an autoimmune
disease hypothesis
15−20 year
experiment
“T2T-NEDA & early”
Question: Do you understand the difference between the treatment strategies of maintenance, escalation and induction therapy?
What is your treatment philosophy? Maintenance-escalation vs induction
Survival
analysis
T2T=treat-to-target; NEDA=no evidence of disease activity.

Increasing Personalization: Matching Efficacy to Disease Activity
Moderate
Efficacy
Intermediate
Efficacy
High
Efficacy
Ongoing activity
but low concern
Ongoing activity
but high concern
Poor
(active disease)
Indeterminate
(active disease)
Favourable
(active disease)
Giovannoni G. Barts & The London, UK, February 2014.

An Aggressive Disease Requires a Strong Medicine
Moderate
Efficacy
Intermediate
Efficacy
High
Efficacy
Giovannoni G. Barts & The London, UK, February 2014.

Treat-to-Target: No Evidence of Disease Activity

Herd Immunity
Not immunised but
still healthy
Immunised and
healthy
Not immunised, sick
and contagious
http://en.wikipedia.org/wiki/Herd_immunity.
Accessed 7 March 2014.

A Hypothetical Population of Newly Diagnosed People with
CIS/MS
CIS=clinically isolated syndrome.

Hypothetical Long-term Outcomes Under the Current Treatment Paradigm
Giovannoni G. Barts & The London, UK, February 2014.

Hypothetical Long-term Outcomes Under the T2T-NEDA Paradigm
Giovannoni G. Barts & The London, UK, February 2014.

Question: What about pregnancy?
14. How do you treat hyperemesis gravidarum during pregnancy?
15. Should I continue taking my other drugs for my MS symptoms during
pregnancy?
16. What is the best treatment strategy for my MS? Should I go onto a DMT and
get my MS under control before starting a family or should I start my family
first?
17. What is the best treatment strategy for my MS to maximise my chances of
having a family and keeping my MS under control?
18. How will having neutralizing anti-IFN beta antibodies affect my baby?
19. Can I have in vitro fertilization? Will the drugs that are used to induce
ovulation affect my MS?
20. What dose of vitamin D do you advise during pregnancy?
21. Are oral contraceptives safer for my MS? Which contraceptive do you
recommend?
1. Does MS affect my fertility?
2. Will pregnancy affect the course of my MS?
3. Will I be able to breast feed after delivery?
4. How long before I fall pregnant must I stop my DMT?
5. If I fall pregnant on a DMT will this affect the baby?
6. Can I breast feed on my DMT?
7. Will I be able to be a good parent if I become disabled from my MS?
8. If I become disabled or unemployed as a result of MS will I be able to support
my children?
9. What is the risk of my children getting MS?
10. Can I do anything to prevent them from getting MS?
11. Am I more likely to need an assisted delivery because I have MS?
12. Will I be able to have a normal vaginal delivery?
13. Will I be able to have an epidural during labour?

Considerations for Women of Childbearing Potential
Interferon β • In monkeys, increased rate of abortion. No malformations in
surviving animals
• Initiation of treatment is contraindicated during pregnancy
Glatiramer acetate
• Animal studies are insufficient with respect to effects on pregnancy;
embryonal/foetal development, parturition, and postnatal
development
• Contraindicated during pregnancy
Natalizumab
• Studies in guinea pigs and monkeys showed no evidence of
teratogenic effects or effects on growth of offspring
• Should not be used during pregnancy unless the clinical condition of
the woman requires treatment with natalizumab
Fingolimod
• Animal studies have shown reproductive toxicity, including foetal loss
and teratogenicity
• While on treatment, women should not become pregnant; if
pregnancy occurs, discontinuation of fingolimod is recommended
Animal studies, Clinical recommendations
Data from summary of product of characteristics (SmPC) for each therapy.

Considerations for Women of Child-bearing Potential
Teriflunomide
• Embryotoxic and teratogenic in rats and rabbits at doses in the
human therapeutic range
• Contraindicated in pregnancy
• Patient advised to contact physician if pregnancy is suspected;
institution of accelerated elimination may decrease risk to foetus
Alemtuzumab
• Dosing mice for 5 days during gestation resulted in significant
increases in dead or resorbed conceptuses and reduction in viable
foetuses
• Placental transfer and potential pharmacologic activity observed
• Contraception advised during treatment and for 4 months following
• Should be administered during pregnancy only if the potential benefit
justifies the potential risk to the foetus
• Thyroid disease poses special risks in women who are pregnant
(potential miscarriage, foetal effects such as mental retardation and
dwarfism,transientneonatalGraves’disease)
Dimethyl fumarate • No malformations have been observed at any dose in rats or rabbits
• Should be used during pregnancy only if clearly needed and if the
potential benefit justifies the potential risk to the foetus
Animal studies, Clinical recommendations
Data from summary of product of characteristics (SmPC) for each therapy.

Key Takeaways
• There is a large gap between the therapeutic ideal and reality
• How are you going to close this gap?
• By practicing the concordance model?
• By being ready to answer your patients questions?
• We need to find balance between therapeutic objectives and patient needs (benefit-risk
assessment)
• What are your therapeutic objectives?
• Patient and physician perception of burden of therapy may differ
• Treatment philosophies vary widely
• Principal patient considerations impacting on treatment choice and adherence are
• Pregnancy
• Route of administration
• Dosing frequency
• Cognitive level
• Depression
• Belief in medicine/concept of disease (patient vs doctor)
• Understanding that effectiveness varies between individuals