Embed Size (px)
Citation preview

PD Catheter DysfunctionBY
DR. AHMED MOSTAFA TAHA MOAHAMED
DaVita BuraydahPD Orientation Program




Not ALL Migrant PD Catheters are MALFUNCTIONING.BUTMany Malfunctioning PD Catheters are Migrating.
So If Catheter Migrated but Functions WELL , Just leave it.



We can use Fogarty Catheter or guide wire for the Malpositioned or occluded PD Catheter
Different Types of Fogarty catheters

PD Catheter Occlusion
Mucinous Fibrin normally present to lubricate the external part of bowels
in peristalsis
Some times it suspend and cause concretions lodging in the distal tip of
PD catheter or the side holes causing obstruction and malfunction .
When it is noticed by patient in tubes or bags , He/She can inject
anticoagulant .
The standard is using Heparin 500-1000 u / Liter PD dialysate ( about 1000
– 2000 u heparin in ordinary 2 L bag ).
Same Maneuver can be Prophylactically be done to patient with
cloudy effluent specially in peritonitis


USE Of tissue Plasminogen Activator in PD Catheter occlusion
The Gambro New Haven experience with administration of tPA
8 mgs in 10 ml (up to 10 mg/10 ml may be used) of sterile water injected into the catheter and allowed to dwell for 1 hour) in 29 cases of catheter obstruction in 18 patients is presented. Patency was restored in 24 instances with no adverse effects. In the 5 cases that did not respond, the primary cause of poor drain was catheter malposition in 2, constipation in 2, and adhesions in 1.
Nephrol Nurs J. 2004 Sep-Oct;31(5):534-7.

Case
A 71-year-old man with ESRD due to ADPKD on HD 8 Years , then Transplant , allograft failure 3 years later , initiate PD , Catheter is inserted , worked well for 3 weeks .
Then inflow was noted to be slow, with no outflow possible. Additionally, a significant amount
of fibrin was noted in the catheter. Conservative measures such as use of laxatives and
recurrent catheter flushes with heparinized saline were unsuccessful.
Abdominal radiography demonstrated that the tip of the PD catheter was appropriately
located in the mid-pelvis.
A decision was made to proceed to catheter manipulation under fluoroscopic guidance.
At the time of catheter manipulation, it appeared that the PD catheter was completely
encased in a fibrin sheath. Injected contrast was seen tracking retrograde along the catheter to the site of spillage in the lower left quadrant.
Perit Dial Int. 2012 Mar-Apr; 32(2): 218–220.

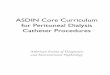
Before manipulation, the
peritoneal dialysis catheter
is positioned in the mid-
pelvis. Injected contrast is
seen tracking retrograde
along the catheter to the
site of spillage in the lower
left quadrant (white arrow).

A stiff guidewire was therefore used to manipulate the
catheter, displacing the catheter into the left paracolic
gutter, with its tip near the splenic flexure. The PD catheter
was intact, and in this new position, free injection and
aspiration of fluid from the catheter, with excellent inflow
and outflow, was attained. Interestingly, after the PD
catheter was repositioned, the fibrin sheath from the catheter’s initial position remained in the pelvis

the peritoneal dialysis
catheter is visualized in
its new position in the left
paracolic gutter (white
solid arrow). In the mid-
pelvis, a contrast-filled
fibrin sheath from the
initial PD catheter
placement is seen (white dashed arrow).

Fibrin Sheath


From Nolph and Gokal's Textbook of Peritoneal Dialysis


From Nolph and Gokal's Textbook of Peritoneal Dialysis

From Nolph and Gokal's Textbook of Peritoneal Dialysis

From Nolph and Gokal's Textbook of Peritoneal Dialysis