Embed Size (px)
DESCRIPTION
Presentation from the International Congress of the Royal College of Psychiatrists 24-27 June 2014, London
Citation preview

People with dementia in the acute
hospital:
Experiences and outcomes
Dr Liz Sampson
Senior Clinical Lecturer, Marie Curie Palliative Care Research Unit
Division of Psychiatry, University College London
Consultant in Liaison Psychiatry, North Middlesex University Hospital

A response to report-itis !

A case from the Ombudsman
“A former architect who had Parkinson’s dementia was taken
to x in Surrey after suffering paranoia and
hallucinations. The 72 year-old was given an antipsychotic
drug that left him like “a zombie, a ragdoll” and robbed him of
his dignity according to his wife. Doctors did not notice he
had developed pneumonia and he died within weeks. His
wife said their failings had “fast-tracked my husband to his
death” and the Ombudsman found he had been over-sedated
and nursing records fell short of standards”

Prevalence of Dementia (DSM IV)
Men:
70-79 16.4% (9.4-23.3)
80-89 40.4% (30.6-50.2)
90+ 48.8% (33.6-64.1)
Women:
70-79 29.6% (21.3-37.9)
80-89 52.9% (45.4-60.5)
90+ 75.0% (65.1-84.9)
Sampson et al. 2009

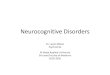
How common is dementia in the acute
hospital ?
Mukadam and Sampson 2011, Sampson et al 2009
DSM IV Dementia
Prevalence (95% CI) Study Year
Margiotta (330) 2006 26.1 (19.1 to 33.1)
Laurila (219) 2004 40.2 (33.7 to 46.7)
Zekry (349) 2008 43.3 (38.1 to 48.5)
0 20 40 60
Prevalence (%)
Sampson (617) 2009 42.4 (38.5 to 46.3)

BePaiD Study
• Estimate the prevalence and types of BPSD
• Impact of BPSD on the person with dementia,
– antipsychotic drugs, length of hospital stay, risk of adverse events, dying
• Prevalence of pain
– how well this is detected and managed by hospital staff
• The relationship between BPSD and Pain

Sample and setting
• >70 admitted to the Medical Acute Admissions Unit
• Cohort study (250 people with dementia)
• Recruiting at 2 London Hospitals (4 months at each)

Study Measures
Baseline
• Confusion Assessment Measure (CAM)
• Mini-Mental State Examination (MMSE)
• DSM IV Criteria Dementia
• Functional Assessment Staging Scale (FAST)
• Charlson Co-Morbidity Index (CCI)
Repeated measures (baseline and every 4 ± days)
• Behave-AD
• Cohen Mansfield Agitation Inventory (CMAI)
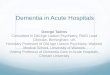
• PAINAD
• Do you have pain?
• Faces Pain Scale
On discharge or death
• Casenote review (ACOVE, economics, medications, AEs etc)

INDICATOR SCORE = 0 SCORE = 1 SCORE = 2 TOTAL
SCORE
Breathing Normal
breathing
Occasional laboured
breathing; Short
period of
hyperventilation
Noisy laboured
breathing. Long period
of hyperventilation.
Cheyne-Stokes
respiration
Negative vocalisations None Occasional
moan/groan. Low
level, speech with a
negative or
disapproving quality
Repeated troubled
calling out. Loud
moaning or groaning.
Crying.
Facial expression Smiling or
inexpressive
Sad, frightened,
frown
Facial grimace
Body language Relaxed Tense, distressed,
pacing, fidgeting
Rigid, fists clenched.
Knees pulled up.
Striking out. Pulling or
pushing away
Consolability No need to
console
Distracted by voice
or touch
Unable to console,
distract or reassure
TOTAL: (Max 10)
PAINAD


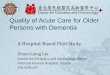
Total
(1612)
Screened, does not meet study
criteria (1320)
Screened, met study criteria
(292)
Patient had capacity
(63)
Personal Consultee
(215)
Professional Consultee
(14)
Assent form not returned
(23)
Not suitable
(1)
Total Participating Professional
Consultee (13)
Assented, not eligible
(4)
Total Participating
Personal Consultee
(188)
Total Participating with capacity
(29)
Consented, not eligible
(34)
Total Participants in study (230)
MMSE >24/AMTS>7 634 Discharged before seen 145 Does not consent 58 Too ill to take part 60 Missed the 72 hour window 78 Not Care of the Elderly 95 Limited English 124 Does not fit DSM Criteria 103 Consistent CAM POS 8 Planned admission 5 Deceased 10

Cohort characteristics
• Mean age 87 years , 66% female
• 76% white British
• 11% delirium on admission
• 30% no previous diagnosis
49%
7%
13%
31% House
Sheltered
Residential Home
Nursing Home
33%
27%
25%
15%
2-5 (functional deficit, difficulties with some ADLs)
6a-c (help putting on clothes, toiletting or bathing)
6d-e (double incontinence)
7a-f (speaks 5-6 words, can no longer walk, sit up smile or hold up head)


Management of BPSD
• 12% started on neuroleptics
• “treatment gap”
– 22.6% mittens or cotsides
– 15% increased supervision
– 6% family assistance
– 1% music, massage

Outcomes associated with BPSD
• BPSD at baseline are not associated with increased length of stay
• BPSD during admission are not associated with increased costs of
care
• BPSD during admission are associated with:
– Lower scores on the ACOVE indicators
– Increased adverse events
– Increased mortality

Pain
Self reported
• 49% of people with dementia in our study were unable to complete the
FACES pain tool
• 21% said ‘Yes’ they had pain in last 24 hours
Observed pain
• Pain during rest-28%
• Pain during activity-65%
• Persistent pain during admission 36%

Management of pain
• Of those who experienced pain at any time during admission, at
movement or at rest only 65% were prescribed an analgesic
• Preliminary analysis suggests that pain medications were only given to
30% of those who were in pain
• Non-pharmacological techniques were NEVER used

The association between pain and BPSD
p=0.003/0.005
p=0.02
p=0.04 p=0.01
Generalised estimating equations GEE- adjusted for age gender, delirium, severity, Charlson score,
reason for admission

Dying with dementia in the acute hospital
• 30 (13%) died during their admission
• Mean age 87 years
• 37% admitted from nursing homes
• 23% had delirium at admission (vs. 9% who were discharged)
• 70% of deaths were “expected”
• 67% were placed on LCP

Symptoms at death
Pain
• 27% died with pressure sores (grades 1-4)
• 50% of patients were noted by clinicians to be in pain in the last 48
hours of life
• Mean PAINAD of 2.69 compared to 1.49 for those who were
discharged
BPSD
• 50% of patients were noted by clinicians to be experiencing agitation
at the last 48 hours of life
? LCP

Pain and discomfort
BPSD
Staff
disengagement
Loss of personhood
Loss of person centered care

Its not all bad…
“That my aunt was treated for her infection and was sent back to the care
home in a much better condition”
“I'm glad she was recognised as someone who wanders off and therefore
placed in a specialised unit, so that she was safe”
“Having a care package arranged when leaving hospital”
“Being able to visit out of hours, staff were ok. Diamorphine in the end”

Conclusions
• BPSD are common, they may lead to
– Poorer quality care
– Increased adverse events
• Management of BPSD is still very basic and requires specialist support
• Commonly used pain tools may not be suitable for this population
• Pain appears to drive some BPSD
• Dying is recognised but poorly managed
• Some carers described good experiences

Acknowledgments
• Alzheimer’s Society
– Barbara Di Vita
– Sylvia Wallach
– Lynn Whittaker
• Health Services for Older People
• Dr Sophie Edwards and Dr Dan Lee
• Project team
– Nicola White
– Kathryn Lord
– Sharon Scott
@PainandDementia