Embed Size (px)
Citation preview

Pediatric Pediatric VideostroboscopyVideostroboscopy
ENT Department. Hospital de Niños “J.M de los Ríos”.Caracas- Venezuela
Dr. M.Adriana Pérez, Dr. Victoria Tenías, Dr. Jacqueline Alvarado, Dr. Ligia Acosta, Dr. Yanet bastidas, Dr. Marisol Díaz

Well known use of videostroboscopy Minor Structural Alterations of larynx (Paulo Pontes
Brasil 1994): Laryngeal Asymmetry Posterior fusion incomplete Glottic disproportion Alteration of focal fold cover
Chronic Dysphonia Congenital origin?
BackgroundBackground

Design a protocol for performing videostroboscopy in children
Point out usefulness of previous training for children below 8 years old
Precise incidence of minor structural alterations of larynx in pediatric population
ObjectivesObjectives

Prospective and descriptive study Aug 2008 - Aug 2009 165 Dysphonic patients 33 patients (+24m) Between 4 and 18 years old / 21 M – 12 F Exclusion criteria.:
Cranial and facial dimorphism Puberphonia Laryngeal Papillomatosis Vocal fold paresis Laryngeal previous surgery
Methods IMethods I

History of Dysphonia
Methods IIMethods II

History of Dysphonia
Methods IIMethods II

Transnasal Flexible Fibroptic evaluation
Methods IIMethods II
Aritenoids mobility
Vocal fold
Lesions

Videostroboscopic assessment: Mother training/child training: minimal 2 weeks Gag reflex: metoclorpamide if needed
Methods IIMethods II

Methods IIMethods II

ResultsResults Distribution of Minimal Structural Alterations in
patients with dysphonia
N= 165

ResultsResults
N= 33
Distribution by age of patients with minimal structural alterations

ResultsResults Distribution of minimal structural alterations
types

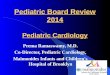
ResultsResults Number of failed intents by age

-All patients trained.-21% (7) needed “ a second chance”-9% (3) needed a “ third chance”-Ages 7 to 10 more affected-More frequent lesion: sulcus vocalis-All (33 pts) had Minimal Structural Alterations.
ConclusioConclusionsns

- Videostroboscopy can be done in pediatric patients-Minimal structural alterations could have a congenital origin-Voice therapy can be follow up in children's-Management of dysphonic patients could be done more accurately in pediatric patients
ConclusioConclusionsns

THANK YOU