Embed Size (px)
DESCRIPTION
Focusing on the fetus as the patient, this new edition also brings together a new team of editors whose perspectives on tissue engineering & molecular biology will bring this well into the 21st century To purchase this book please visit www.asia.elsevierhealth.com
Citation preview

- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
CHAPTER 120
Bladder and CloacalExstrophyLynn L. Woo, John C. Thomas, and John W. Brock III
The authors would like to acknowledge Romano T. DeMarcoand James A. O’Neill, Jr. for their previous contributions tothis chapter.
Bladder Exstrophy
Bladder exstrophy is a rare midline defect and exists as part ofa larger spectrum of abdominal-pelvic fusion abnormalities,known collectively as the exstrophy-epispadias complex(EEC). Presentation of EEC can range from isolated glanularepispadias to cloacal exstrophy, in which several other organsystems may be affected. In the case of bladder exstrophy, theopen bladder can be seen everting through a lower abdominalwall defect. This is accompanied by epispadias, a widened pu-bic diastasis, and an anus that is anteriorly displaced. Over thepast 2 decades, continued improvements in the methods offunctional bladder closure have dramatically increased recon-structive success rates; however, achieving the ultimate goalsof adequate bladder capacity, urinary continence, and a goodcosmetic outcome remain challenging.
HISTORICAL PERSPECTIVES
The earliest account of bladder exstrophy can be found on As-syrian tablets, dating back to 2000 BC. Von Grafenberg first de-scribed the medical condition in 1597, and Mowat is creditedwith providing a complete description of bladder exstrophy in1748. It was not until 1780, however, that Chaussier firstcoined the term “exstrophie.”1 Early management of bladderexstrophy included the application of an external urinary re-ceptacle to the surface of the exposed bladder,2 ureterosigmoi-dostomy,3 transplantation of the bladder trigone into therectum,4 and coverage of the exposed bladder with lateral skinflaps.5 These methods were fraught with continued urinaryincontinence and/or urosepsis. Contributions by Coffey,Nesbitt, Leadbetter, and Clarke improved the technique ofureterosigmoidostomy; however, associated morbidities in-cluded infection, electrolyte abnormalities, and malignancy.6
Complete urinary diversion into the colon or alternate conduitwas preferentially used to provide continence and minimizeinfection, but the problems of anatomic reconstruction andsexual function persisted.
Paralleling efforts to develop improved methods of urinarydiversion were attempts at successful bladder closure. Trende-lenburg described bilateral sacroiliac osteotomies and the ap-plication of a pelvic sling to support bladder and abdominalwall closure in 1892.7 The first case of successful closureand continence in a female patient with bladder exstrophywas not reported until 1942 by Young.8 Michon subsequentlyreported successful reconstruction in a male patient 6 yearslater.9 Despite these accounts of functional closure, a 1970 re-view of 329 cases by Marshall and Muecke concluded thatonly 19% of patients undergoing total reconstruction hadfair-to-satisfactory results.10 These unfavorable outcomeswere reported by others, spurring efforts to improve methodsof surgical repair.11,12
EPIDEMIOLOGY
The incidence of bladder exstrophy is estimated at between 1in 10,000 and 1 in 50,000 live births13 with a higher male-to-female ratio of between 2.3:1 and 4:1.14 Familial recur-rence is approximately 1 in 100.15 On the basis of a surveyof 2500 indexed cases, familiar occurrence was found to be1 in 275.14 Multiple reports of bladder exstrophy amongidentical twins have demonstrated variability in involvementof one or both twins. Subsequent siblings and the offspringof individuals with bladder exstrophy may be at increased riskof being affected.14,15 However, no clear pattern of inheritancehas been characterized and no specific genetic or environmen-tal factor that predisposes to bladder exstrophy has yet beenidentified.
EMBRYOLOGY
The underlying embryologic defect shared by bladder exstro-phy and other variants of the EEC is due to abnormal devel-opment of the cloacal membrane, a bilaminar structurecomposed of endoderm and ectoderm that overlies the cloacalcavity at the caudal end of the germinal disk.16 In normal
1515

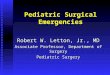
development, lateral ingrowth of mesoderm occurs betweenthe two layers of the cloacal membrane during the fourthand fifth weeks of gestation. This results in formation of thelower abdominal wall and pelvis. Subsequent caudal growthof the urorectal septum results in its fusion with the cloacalmembrane, thus fully separating the cloaca into the bladderanteriorly and the rectum posteriorly (Fig. 120-1). The pairedgenital tubercles, which will give rise to the phallus, migratemedially to fuse in the midline. Normal perforation of the clo-acal membrane occurs after fusion with the urorectal septum,at approximately the sixth week, resulting in formation ofseparate urogenital and anal openings.17
Migratory failure of the lateral mesodermal folds and ab-normal overdevelopment of the cloacal membrane have bothbeen proposed as potential causes of the prevention of normalmesodermal ingrowth to the cloacal membrane.16,18 The lackof adequate mesodermal reinforcement is thought to result inpremature rupture of the cloacal membrane, the timing ofwhich determines the extent of the abdominal wall defectand degree/severity of urogenital tract involvement.19 Ruptureof the cloacal membrane after fusion with the urorectal sep-tum results in bladder exstrophy, whereas rupture before fu-sion gives rise to the more severe presentation of cloacalexstrophy (see later discussion).
CLINICAL PRESENTATION
In general infants with bladder exstrophy are born full term,without coexisting anatomic anomalies. At birth, an evertedposterior bladder plate of varying size is seen in the midlineof the lower abdomen. The mucosa of the exposed bladderin the newborn is typically smooth and pink. The umbilicalcord exits from the superior-most border of the bladder plate,and a small umbilical hernia may be present (Fig. 120-2). Inaddition, there is significant widening of the pubic symphysisand the anus is anteriorly displaced. The levator ani complexis also divergent, leading to an inherent weakness in the pelvicfloor and a tendency toward rectal prolapse and varying de-grees of fecal incontinence. Associated inguinal hernias arecommon and have been reported in 82% of boys and 10%of girls.20 The upper urinary tract is usually normal, thoughrenal anomalies including ectopic, horseshoe, hypoplastic,dysplastic kidneys, and megaureters may be observed.21 Vesi-coureteral reflux occurs in the vast majority of children afterbladder closure, secondary to an exaggerated lateral courseof the ureters within the pelvis and lack of adequate
submucosal tunnel in the bladder wall.22 With continued ex-posure and chronic inflammation, the exstrophied bladderbecomes thickened and polypoid (Fig. 120-3). Long-termexposure may eventually result in a fibrotic, rigid bladderplate that is ultimately unsuitable for closure.
GENITAL DEFECTS—MALE
In the male infant, the open and everted urethral plate can beseen joining the exposed bladder. The penis is characteristi-cally short with a flattened, everted glans. The prepuce is lo-cated on the penile ventrum (Fig. 120-4). The ejaculatoryducts are typically normal and exit at the exposed verumon-tanum in the posterior urethra. The base of the penis and scro-tum are widely separated, with lateral displacement of thecorporal bodies and neurovascular bundles. Historically itwas believed that the individual corpora were of normal cal-iber and appeared shortened because of their attachment tothe widened pubic diastasis and associated dorsal chordee.
A B C
Mesonephricduct
Mesonephricduct
Allantois
Ureteric budUrorectalseptumUrorectal
septum
Hindgut
Cloacalmembrane
Primitiveurogenital
sinus
Anorectalcanal
Bladder
Ureter
Perinealbody
Phallus
FIGURE 120-1 Division of the cloaca in the urogenital sinus and rectum.A,At the end of the fifth week.B,At 7weeks.C,At 8weeks. (Modified from SadlerTW: Langman’s Medical Embryology, 8th ed. Philadelphia, Lippincott Williams and Wilkins, 2000, p 316.)
FIGURE 120-2 Typical findings of classic bladder exstrophy in a new-born male. The bladder plate is small, and a small hernia is evident at itssuperior border. The penis is foreshortened, with widely splayed corporalbodies and glanular separation. The urethral plate is short and located onthe anterior surface of the split phallus.
1516 PART VIII GENITOURINARY DISORDERS

More recently, an MRI-based study by Silver and colleagues ofadult men with exstrophy and age-matched controls foundthat although the length of the posterior corporal bodieswas the same between groups, anterior corporal length inmen with exstrophy was nearly 50% shorter than that of con-trols.23 Therefore thepenis appears shortenednot only second-ary to corporal divergence, dorsal chordee, and abnormalcrural attachments to the corpora cavernosa but also becauseof an inherent deficiency of corporal tissue (Fig. 120-5). Thetestes may appear to be undescended, but in most cases theyare actually retractile and will eventually reside in the scrotumwithout the need for formal orchiopexy. Should it be required,orchiopexy is performed in conjunction with inguinal herniarepair.
GENITAL DEFECTS—FEMALE
The clitoris is bifid, with divergence of the mons pubis, labia,and clitoral halves (Fig. 120-6). The urethra and vagina areshortened, and the introitus is anteriorly displaced. The vag-inal orifice is often stenotic. The uterus and adnexa are typi-cally normal, though vaginal and uterine duplication havebeen reported.24,25 Uterine prolapse occurs commonly infemale patients, secondary to the inherent weakness in pelvicfloor support.
PELVIC DEFECTS
Some degree of widening of the pubic symphysis is present inall cases of bladder exstrophy and contributes to outward ro-tation and eversion of the pubic rami at their junctions withthe ischial and iliac bones (Fig. 120-7). Using computed to-mography (CT), Sponseller and colleagues further character-ized the pelvic anatomy of a large group of exstrophypatients, noting a significantly increased distance betweenthe triradiate cartilages (31%), external rotation of the anteriorpelvis (18%), and 30% shortening of the pubic rami.26 On thebasis of three-dimensional models generated by CT, Stec andcolleagues observed that among children with exstrophy, thelevator ani muscles were more posteriorly positioned and out-wardly rotated. Furthermore, the puborectal sling had a moreflattened configuration and supported twice the body cavityarea in exstrophy patients.27 As mentioned previously, thesepelvic floor defects predispose to pelvic organ and rectalprolapse in this patient population.
PRENATAL DIAGNOSIS
The use of prenatal ultrasound (US) and MRI has improvedthe antenatal diagnosis of bladder exstrophy, allowing for ap-propriate parental counseling and planning of postnatal man-agement. The prenatal diagnosis of bladder exstrophy may besuggested on US by failure to visualize the bladder in the pres-ence of normal kidneys and amniotic fluid.28–30 In a review ofprenatal US studies from 25 women who delivered infants
FIGURE 120-3 When the bladder has been exposed for at least 1 weekafter birth and the mucosa is subjected to continued exposure and inflam-mation, polypoid excrescences typically appear, as in this female infant.
6
1
3
4
5
7
2
FIGURE 120-4 Classic exstrophy in the male. The penis is pulled downward to expose the dorsal aspect, revealing the urethral plate leading to theexposed bladder. 1, umbilical cord; 2, bladder mucosa; 3, paraexstrophy tissues; 4, left ureteric orifice; 5, verumontanum; 6, urethral plate; 7, glans penis.
1517CHAPTER 120 BLADDER AND CLOACAL EXSTROPHY

with exstrophy, Gearhart and colleagues observed the follow-ing features: absent bladder (71%), lower abdominal bulge(47%) and anteriorly displaced scrotum with small phallusin male fetuses (57%), low-set umbilical cord (29%), andabnormal widening of the iliac crest (18%).31
SURGICAL RECONSTRUCTION
Surgical management of classic bladder exstrophy consists offunctional closure of the native bladder, closure of the epispa-dic urethra and genitalia, and creation of a continence mech-anism to allow for proper urine storage. Reconstruction may
be accomplished in a multi- or single-stage (complete) repair.Multiple contemporary approaches including the modernstaged reconstruction of exstrophy (MSRE) and completeprimary reconstruction of exstrophy (CPRE) along with War-saw,32 Erlangen,24 Mainz,33 and Kelly34 techniques have beenpublished; however, for the purposes of this review, only themajor principles of MRSE and CPRE are discussed.
1
2
3
4
7
7
88
6
6
9
5 5
10 10
112
9
A B
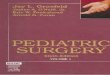
FIGURE 120-5 Penile configura-tion in classic bladder exstrophy.Normal male perineum (A) and withbladder exstrophy (B). Note the lossof the normal triangular shape ofthe perineum and widening of thepubic symphysis. In the setting ofexstrophy, the corpora cavernosaare widely separated and are intrin-sically shorter. 1, corpus caverno-sum of the penis; 2, glans penis;3, corpus spongiosum; 4, bul-bospongiosus muscle; 5, ischium;6, ischiopubic ramus; 7, pubis; 8,ischio-cavernosus muscle and crusof penis; 9, urogenital diaphragm;10, anus and external anal sphincter.
FIGURE 120-6 Typical appearance of classic bladder exstrophy in a fe-male. Note the widely divergent labia and anterior displacement of thevaginal introitus and anus.
FIGURE 120-7 Plain radiograph of a neonate with bladder exstrophydemonstrates the soft tissue mass effect of the exposed bladder, the widediastasis of the symphysis pubis, and the posterior rotation of theacetabula.
1518 PART VIII GENITOURINARY DISORDERS

INITIAL MANAGEMENT
At birth, the umbilical cord should be ligated with a silk sutureto avoid irritation of the bladder surface from the traditionalplastic clip. The exposed bladdermucosa should bemoistenedwith saline and protected with a nonadherent sheet of plasticwrap (e.g., Saran Wrap). A complete physical examination isperformed to rule out associated anomalies and to assess thesize of the bladder plate and extent of the genital defect.Renal US may be obtained to exclude hydronephrosis and/orother upper tract abnormalities. Prophylactic antibioticsshould be administered.
MODERN STAGED RECONSTRUCTIONOF BLADDER EXSTROPHY
A three-stage approach for the treatment of bladder exstrophywas first pioneered by Jeffs and Cendron in the 1970s,35,36
and continued improvements in technique have contributedto increased success of the procedure.37–39 Stage 1 is per-formed at birth to protect the upper urinary tracts and assistlater continent reconstruction. It consists of early closure ofthe bladder, posterior urethra, and abdominal wall with orwithout osteotomy. The primary objective of functional clo-sure is to convert the bladder exstrophy into a complete epis-padias.40 Stage 2 is performed in later infancy and involvesrepair of the epispadias, with the goal of optimizing genitalfunction and appearance, as well as increasing outlet resis-tance to promote bladder growth. Stage 3 is undertaken beforeschool age and consists of bladder neck repair for continenceand ureteral reimplantation for vesicoureteral reflux.
Primary functional closure is generally undertaken in theneonatal period, which offers several potential advantages.The pliability of the pelvic ring, in infants younger than72 hours old, may obviate the need for osteotomy; earlyclosure prevents further exposure and scarring of the bladderplate; there is theoretically less opportunity for bacterialcolonization of the plate with decreased risk of postoperativeinfection. Alternatively, delayed closure in combination withpelvic osteotomy may be performed, allowing for patientgrowth and a period of time out of the hospital beforereconstruction.
Stage 1: Functional Closure
At the time of surgery, the patient should be prepped widelyincluding the entire body anteriorly and posteriorly below thenipple line so that intraoperative turning is easier. Cardiopul-monary monitoring and adequate intravenous access are crit-ical. Intraoperative and postoperative analgesia may beafforded by means of an epidural catheter. The most commontechnique of functional closure is based on descriptions byJeffs and colleagues36,41,42 and Duckett and Caldamone.43
Figure 120-8 depicts the initial incisional template for bladderclosure in the female infant, and Figure 120-9 details the com-plete sequence of stage 1 closure in the male. Traction suturesare placed into the glans penis, and ureteral catheters are se-cured in each ureteral orifice. An incision is made around theperiphery of the exstrophic bladder plate, and a plane of dis-section is established between the rectus fascia and bladder.The umbilical cord is excised, and umbilicoplasty may be per-formed during or after the initial procedure. Dissection is con-tinued toward the pubis, and the incision is then extended
distally to the verumontanum on both sides of the prostaticurethra, leaving a wide strip of bladder neck and urethralplate.
A major objective of primary closure in the male patient isto place the bladder and prostate deep within the pelvis toachieve a more normal anatomic position.44,45 In some boys,this maneuver results in inadequate length of the urethralplate for subsequent penile reconstruction. Duckett thereforeproposed transection of the urethral plate, distal to the veru-montanum, with the development of lateral paraexstrophicskin flaps, which could be then rotated medially to bridgethe gap between the transected edges of the urethra.46 Al-though this technique allows for better mobilization of thebladder, Gearhart and colleagues41,47 reported a 40% compli-cation rate associated with the use of paraexstrophy flaps. Ure-thral stricture is the most common complication and may besecondary to local tissue ischemia. The routine use of suchflaps appears to be decreasing, though their application re-mains a viable option when a short urethral plate prohibitsadequate bladder mobilization.48
If the urethral plate is left intact, it should be mobilized tothe level of the prostate to create as much urethral length aspossible. Following complete mobilization of the bladder,the corpora cavernosa are dissected off the inferior pubic ramibilaterally, taking care to preserve the neurovascular bundlesand avoid penile devascularization. This maneuver aids in pe-nile lengthening, primarily through release of dorsal chor-dee.23 After placement of a Malecot suprapubic tube andexteriorization of the ureteral catheters, the bladder is closedanteriorly in the midline and the urethra tubularized over a10- to 12-Fr sound. The first-stage repair thus results in anisolated penopubic epispadias, which is generally incontinent.
Closure of the pelvic ring is required to assist in abdominalwall closure. Pubic approximation without ancillary osteot-omy may be possible in the immediate newborn period, whenthe bones are still malleable; however, osteotomy is generallyrequired after 3 days of age. Although multiple techniques are
FIGURE 120-8 Typical findings of classic bladder exstrophy in a femaleand the incision template used for repair.
1519CHAPTER 120 BLADDER AND CLOACAL EXSTROPHY

A B C D
E F G H
I J K
FIGURE 120-9 Sequence of repair of bladder exstrophy in a male. A, Completion of the dissection around the periphery of the bladder and the urethralplate. B, Inversion of the bladder plate and approximation of the corpora as a first stage in epispadias repair. Also note the inferior paraexstrophy incisions.C, Further closure of the skin over the corpora and their partial freeing from the pubis.D, Placement of a suprapubic drainage tube. E, Further closure of theskin inferiorly, with approximation to the urethral plate. Creation of the paraexstrophy flaps is now evident. F, The urethral plate is prepared for tubular-ization over a catheter. G, The urethral plate is now tubularized, and ureteral catheters are placed bilaterally and brought out on each side of the bladder.The bladder is also in the process of being tubularized. H, Completion of tubularization of the bladder and urethra, and location of the various drainagetubes. I, After two-layer closure of the bladder and urethral plate, the bladder is reduced into the pelvis and fixed with sutures. J, Sutures are placed toencourage approximation of the pubic halves. K, Drainage tubes are brought out superiorly, and fascia, subcutaneous tissue, and skin are approximated.Approximation of the pubis helps protect the bladder closure and the abdominal wall closure.
1520 PART VIII GENITOURINARY DISORDERS

described, combined bilateral anterior innominate and verti-cal iliac osteotomy is most frequently used to assist symphy-seal approximation and medial rotation of the pelvic bones.49
Fixator pins are then placed into the iliac wings and lowerosteotomized segments. Our group generally used bilateralanterior iliac osteotomies (Fig. 120-10). Closure of the pelvicring is performed using a large-sized, monofilament suture,taking care to place the knot anteriorly to avoid erosion intothe soft tissue below. The newly closed bladder and urethracan now be covered by reapproximation of the rectus fasciaand skin, with externalization of tubes and drains. Externalfixators are applied to the pins to hold the pelvis in the correctconfiguration. Lower extremity traction is applied to keep thelegs still and prevent destabilization of the pelvis (Fig. 120-11).The external fixator remains in place for 4 to 6 weeks aftersurgery, allowing for callus formation at the osteotomy sites.As an alternative to external fixation, immobilization may alsobe accomplished through the application of a spica cast, whichenvelops the hips and lower extremities. The cast remains inplace for 4 to 6 weeks.
The technique for initial closure in a female patient is sim-ilar to that described previously. The traction suture is initiallyplaced anterior to the vagina, which is fully mobilized, as theneourethra is tubularized. The vagina is then repositioned tocreate a more caudal angle of entry.
Postoperatively, the patient is maintained on antibiotic pro-phylaxis. Parenteral nutrition may be used initially in order toavoid abdominal distension. Close attention must be given topatient positioning and fixator pin sites to minimize the risk ofskin ulceration and nerve injury.
Stage 2: Epispadias Repair
The second stage of repair is generally undertaken between6 and 12 months of age. It centers on reconstruction of thephallus, with repair of epispadias and urethroplasty. Thismay further optimize bladder capacity, through an increasein outlet resistance.50 Although many techniques have beenused, the method described by Cantwell and later modifiedby Ransley has been shown effective in accomplishing urethralrelocation to the penile ventrum, correction of chordee, and a
B
A
FIGURE 120-10 A, If the pubiscannot be approximated in a new-born or if the procedure is under-taken later, when the pelvis is lessflexible, pelvic osteotomy is re-quired. The location of an anterior il-iac osteotomy is shown. B, Externalfixator pins are used to hold thepelvis, and the pubic halves arebrought together in the midline.
1521CHAPTER 120 BLADDER AND CLOACAL EXSTROPHY

low fistula rate (Fig. 120-12).51,52 This technique involves fullmobilization of the corpora and dorsal urethral plate, which isdissected free and tubularized. Correction of dorsal chordee isachieved by incising each corpora transversely, creatingdiamond-shaped defects and anastomosing their dorsal me-dial aspects over the tubularized urethra. A ventral meatotomyis then performed at the tip of the glans to produce a moreanatomically normal meatal position.53 Other describedmodifications of the Cantwell-Ransley technique include fulldetachment of the urethral plate from the corporal bodies,leaving only the distal-most 1 cm of urethra attached to theglans tip. The urethra is then tubularized, the corpora are
incised transversely at the point of maximumdorsal curvature,and the corporocavernostomy defects sutured together, thuscovering neourethra. This maneuver places the urethra ven-trally between the corporal bodies, causes downward deflec-tion of the penis, and also provides extra length. If chordee iscorrectable by simple corporal rotation, bilateral corporo-tomies are not required. The glansplasty is completed intwo layers, resulting in a ventrally placed neourethra.54 Fur-ther modifications to the technique of epispadias repair in-clude the use of full penile disassembly described byMitchell and Bagli (Fig. 120-13).55
Stage 3: Bladder Neck Reconstructionand Ureteroneocystostomy
The final stage of exstrophy repair involves the construction ofa urinary continence mechanism and is generally undertakenaround 4 years of age.56 During this interval, the patient ismonitored periodically with renal US to evaluate the adequacyof upper tract drainage. Bladder capacity is also assessed be-fore bladder neck surgery. Jeffs and colleagues57 reported thata bladder capacity of greater than 60 mL typically allows foradequate functional storage capacity without the need forconcomitant bladder augmentation, although others havereported median capacities of greater than 85 mL to be morepredictive of achieving continence.58 Regardless, it is generallyagreed that continence is highly dependent on the size of theoriginal bladder plate, successful initial bladder closure, andan adequate preoperative bladder capacity.
The Young-Dees-Leadbetter technique of bladder neck re-pair remains the most common approach to bladder neckreconstruction (Fig. 120-14). After opening the bladder, theureters are first mobilized and reimplanted into a more ceph-alad position by either cross-trigonal or cephalotrigonal ure-teroneocystotomy.22,59 This procedure not only correctsvesicoureteral reflux, which occurs in virtually all cases ofclosed bladder exstrophy, but also allows for creation of pos-terior bladder plate flaps for the bladder neck reconstruction.A recent report by Braga and colleagues also describes
FIGURE 120-11 An infant in Bryant’s traction. The patient must remainimmobilized for 4 to 6 weeks postoperatively.
A B C
FIGURE 120-12 Steps in the Cantwell-Ransley epispadias repair. A, The urethral plate is dissected from the corpora and is tubularized, taking care topreserve the lateral blood supply of the urethra and the neurovascular bundles. B, Corporotomies are created at the midphallus, and the urethra is trans-posed to the ventral surface. C, The corpora cavernosa are rotated medially and reapproximated at the corporotomy sites, pulling the corporal bodiesinward and providing coverage of the neourethra. This procedure permits further urethral lengthening, approximation of the corpora with preservationof the blood supply, and full coverage of the urethra.
1522 PART VIII GENITOURINARY DISORDERS

successful bilateral ureteral reimplantation at the time of pri-mary bladder closure.33
A strip of posterior bladder plate 2 cm � 4 cm is markedoff, and the triangles of bladder laterally are demucosalized.The strip of bladder is tubularized, and the triangles of de-nuded muscle are mobilized laterally to provide coverage ofthe neourethra. If prior urodynamic evaluation has demon-strated inadequate bladder capacity, augmentation cystoplastywith a bowel segment may be performed at this setting.
SINGLE-STAGE RECONSTRUCTION:COMPLETE PRIMARY REPAIROF EXSTROPHY
Recently, Mitchell and Grady minimized the number of re-quired operations by combining bladder closure with epispa-dias repair at birth in a technique known as complete primaryrepair.60 Major potential benefits of this approach include theearlier creation of bladder outlet resistance, theoretically lead-ing to normal cycling and improved bladder capacity andfunctionality as the patient grows. Major principles of CPREinclude total penile disassembly and division of the intersym-physeal band, which enables posterior positioning of the
bladder, bladder neck, and urethra. As described by Gradyand Mitchell,60 CPRE begins with intubation of each ureteralorifice with ureteral catheters. Traction sutures are placed intoeach hemiglans, the bladder plate is circumscribed, and dis-section is continued inferiorly along the ventral aspect ofthe penis. The urethral plate is mobilized off the penis, whichis fully disassembled into separate right and left corporal bod-ies and the spongiosum-containing urethra. The intersymphy-seal band is incised (Fig 120-15), which allows the bladderunit to be positioned deep within the pelvis. A suprapubictube is left in place, the ureteral catheters are externalized,and the bladder is closed. Similar to the staged approach, pel-vic osteotomymay be required for abdominal closure. The pu-bic symphysis is approximated using PDS sutures, and theabdominal wall is closed. The urethral plate is tubularizedand transposed to the penile ventrum, and the corporal bodiesare rotated medially and reapproximated (Fig. 120-16).Because of the new posterior positioning of the bladder unit,urethral length is often inadequate to reach the glans, anda hypospadiac meatus is left for future reconstruction(Fig. 120-17). Penile shaft coverage is achieved through theuse of ventral rotational penile skin flaps. Postoperatively,the patient remains immobilized as previously described inthe technique of staged closure. Additional procedures to cor-rect for residual hypospadias, vesicoureteral reflux, andincontinence may be required as the child grows.
URINARY DIVERSION
Urinary diversion, in the form of a bowel conduit or reservoir,may ultimately be required for patients with insufficient blad-der plate or after reconstructive efforts have been unsuccessfuland is discussed in Chapter 118.
OUTCOMES AND COMPLICATIONS
Themost devastating complication of bladder closure is dehis-cence. Major contributing factors include wound infection,abdominal distension, bladder prolapse, and loss of ureteraland/or suprapubic catheters within 6 days of closure.61 Uri-nary diversion, reclosure of the bladder as a urethral tubefor later augmentation, or delayed repair of the bladder maybe performed. If not performed in the initial setting, pelvicosteotomy is frequently necessary for successful reclosure.
Urinary incontinence remains a significant problem for upto 30% of bladder exstrophy patients. In the case of bladderneck incompetence, injectable bulking agents, bladder necksling or artificial urinary sphincter have all been applied. Blad-der neck reconstruction or formal closure of the bladder neck,with the creation of a catheterizable channel, can also be per-formed. In cases where incontinence is secondary to insuffi-cient bladder capacity, augmentation cystoplasty remains themost viable treatment option.
Following epispadias repair, the most common complica-tion is urethrocutaneous fistula, which ranges from 2% to26% in modern series.51,54,62
The incidence of adenocarcinoma of the bladder in adultswith bladder exstrophy has been estimated to be 250 times thatof the normal population and is likely due to chronic inflam-mation, infection, and metaplasia of an exposed bladderplate.63 A series by Woodhouse and colleagues, however, re-cently documented an 800-fold risk in the incidence of bladder
A
B
C D
FIGURE 120-13 Complete penile disassembly technique. A, The corpo-ral bodies and the hemiglans are separated. B, The urethra is tubularizedand moved ventrally. C, The corpora are reapproximated dorsally.D, Glansclosure is performed distally to complete the repair. (Modified fromMitchell ME, Bagli DK: Complete penile disassembly for epispadias repair:The Mitchell technique. J Urol 1996;155:300.)
1523CHAPTER 120 BLADDER AND CLOACAL EXSTROPHY

- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
malignancy among thosewith a history of bladder exstrophybyage 40.64 Thedevelopment of adenocarcinoma and transitionalcell carcinoma of the bladder is also a potential risk in thosepatients who have undergone augmentation cystoplasty.65,66
Fertility in patients with bladder exstrophy and epispadiaswas studied by Shapiro and colleagues,14 who surveyed 2500patients. Among these, 38 men had successfully fathered chil-dren and 131 women had given birth. Diminished fertilityrates amongmales may be secondary to retrograde ejaculation,though libido and erectile function appear to be normalaccording to a report by Woodhouse and colleagues.67 Femalepatients face a significant risk of uterine prolapse.
CONCLUSION
Contemporary reconstructive techniques for the repair ofbladder exstrophy have resulted in acceptable function andcosmesis for the majority of patients with classic bladderexstrophy. Overall continence rates range from 70% to 80%.
Bladder augmentation is preferred in patients without ade-quate bladder capacity, and bladder neck closure with creationof a continent catheterizable stoma may be performed whenother continence procedures have failed.
Cloacal Exstrophy
Cloacal exstrophy is a rare condition occurring in 1 of 200,000to 400,000 live births68 and comprises the most severe defor-mation along the EEC spectrum, which includes both epispa-dias and classic bladder exstrophy. Cloacal exstrophy is alsoreferred to as the OEIS complex (omphalocele, exstrophy, im-perforate anus, and spinal defect) when other malformationsof the urogenital, gastrointestinal, skeletal, and neurospinalaxis are present.
Although first described by Littre in 1709, historic survivalrates were dismal secondary to sepsis or fluid, electrolyte, andnutritional derangements from short gut syndrome or
Bladder
Suspensory sutures
Urethra
Lateral view
A
B
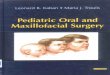
FIGURE 120-14 Young-Dees-Leadbetter procedure for bladderexstrophy repair. A, The ureters areappropriately reimplanted to avoidreflux. Triangular areas at the blad-der base are then denuded, andthe remaining muscle is tubularizedover a catheter. This serves tolengthen the urethra and providessufficient pressure to encouragethe development of improved blad-der capacity without causing ure-thral obstruction. B, The bladder isreclosed, and the bladder neck isfurther supported by sutures, whichsecure it to the pubis anteriorly.
1524 PART VIII GENITOURINARY DISORDERS

intestinal obstruction.69 The first successful repair wasreported in 1960 by Rickham, who recommended staged sur-geries for reconstruction.70 Advances in neonatal care and sur-gical technique have resulted in present-day survival rates thatexceed 90%, and principle goals of treatment are now directedtoward improving quality of life in these patients.68,71–75
EMBRYOLOGY AND GENETICS
The underlying defect in cloacal exstrophy is thought to be re-lated to abnormal development and premature rupture of thecloacal membrane, as described earlier in the bladder exstro-phy section. In the setting of cloacal exstrophy, it has been pos-tulated that membrane rupture occurs within the first 8 weeksof gestation. Confirmation of this theory is difficult, however,
given no embryologic stage similar to cloacal exstrophy existsin normal development.76 Disruption of the cloacal membrane,as the principle underlying abnormality, has been supported bysurgically induced exstrophy in animal models.19,77 The pre-vailing developmental theories are further clouded by severalrecent reports documenting rupture as late as 26 weeks.78,79
Rupture at 5 weeks gestation, as traditionally postulated, wouldcause anterior herniation of the bladder and small bowel, whichwould prevent normal midline fusion of the hindgut, bladderplate, genital tubercles, and mullerian ducts, thus resulting inthe typical anatomic presentation of two open bladder halvesseparated by a strip of exstrophied cecum, hemiphallic halveswith a widely separated pubic diastasis, an underdevelopedand blind-ending distal hindgut with imperforate anus, andan omphalocele of varying size (Fig. 120-18).
Bladder
Corpus spongiosum
Perinealmembrane
Incision throughperineal membrane
Plane of Cross sectionCorrection of Exstrophy
Cross section
Anus
Sup. Transverseperineal muscle
ProstateUrethra
Symphysis
FIGURE 120-15 Pelvic view ofmale exstrophy repair as described by Grady andMitchell. Aggressive dissection along each side of the urethra and divisionof the intersymphyseal band allow posterior positioning of the bladder in the pelvis. (Modified from Grady RW, Mitchell ME: Complete primary repair ofexstrophy. J Urol 1999;162:1416.)
BA
FIGURE 120-16 A, Closure of the urethral plate and bladder as a continuous unit. B, Placement of the urethra ventral to the corporal bodies by posi-tioning the bladder, bladder neck, and urethra posteriorly in the pelvis. (Modified from Grady RW, Mitchell ME: Complete primary repair of exstrophy. J Urol1999;162:1417.)
1525CHAPTER 120 BLADDER AND CLOACAL EXSTROPHY

No single environmental exposure or consistent genetic de-fect in the etiology of cloacal exstrophy has yet been identified.Thauvin-Robinet and colleagues recently identified an unbal-anced translocation between chromosomes 9q andYq, andotherstudies have implicated mutations in homeobox genes suchas HLXB9 and HOX, which are involved in the developmentof embryonic mesoderm.80–82 Although there have been multi-ple reports of cloacal exstrophy among members of the samefamily, these are generally anecdotal andhave involvedmultigen-erational relatives or nontwin siblings.83–85Multiple instances ofaffected monozygotic twins have been reported, however,which lends support to an underlying genetic cause.76,86–88
ASSOCIATED ANOMALIES
Unlike classic bladder exstrophy, cloacal exstrophy is typicallyassociatedwitha variety of other anatomicdefects (Table120-1).
GASTROINTESTINAL
Ileocecal exstrophy with an associated omphalocele, hindgutremnant, and imperforate anus is the most common clinicalpresentation.54 Omphaloceles are present in 88% to 100%of infants and generally contain portions of small boweland/or liver.54,89 Other findings include intestinal duplicationanomalies, gastroschisis, ectopic anus, colonic exstrophy, andmalrotation.90,91 Short gut syndrome may be a significantsource of morbidity among patients with cloacal exstrophyand is observed in 25% of cases.71 The risk of short gutsyndrome is markedly increased in patients subjected toileostomy placement as the initial intestinal diversion proce-dure.92,93 Furthermore, the phenomenon may occur evenin the presence of normal bowel length, implicating an inher-ent absorptive abnormality of the intestine.71,72,90
GENITOURINARY
Abnormalities of the upper urinary tract have been reported in41% to 66% of cases.72,89 Unilateral renal agenesis, pelvic kid-ney, and/or hydronephrosis were observed in up to 33% inDiamond’s 1990 series.89 Less commonly reported findingsinclude horseshoe kidney, fusion anomalies, and ureteral ab-normalities.72,89,90 Complete separation or even absence ofthe phallic/clitoral halves may be observed, and the scro-tum/labia are widely separated. Male infants frequently haveundescended testes with associated bilateral inguinal hernias,whereas failure of mullerian duct fusion in females results invarying degrees of uterine and vaginal duplication anomaliesin the majority of patients.72,89
FIGURE 120-17 At completion of complete primary closure, placementof the bladder and urethral units deeper within the pelvis along with ven-tral transposition of the urethramay result in a hypospadiac meatus, whichcan later be reconstructed with formal urethroplasty.
FIGURE 120-18 Typical presentation of cloacal exstrophy in a male in-fant. O, omphalocele; hB, hemibladder; Ce, exstrophied cecum; hP, hemi-phallus; hS, hemiscrotum; I, prolapsed ileal segment.
TABLE 120-1
Anomalies Associated with Cloacal Exstrophy
Gastrointestinal
Omphalocele
Imperforate anus, anal atresia/stenosis
Short gut syndrome
Intestinal malrotation
Intestinal duplication
Genitourinary
Unilateral renal agenesis
Pelvic kidney
Ureteral duplication
Hydronephrosis
Bilateral cryptorchidism, inguinal hernias
Uterine duplication
Vaginal duplication
Central Nervous System
Spinal dysraphism
Skeletal
Vertebral (absent, extra, hemi)
Club foot
Other lower limb (absence, shortening)
Hip subluxation
1526 PART VIII GENITOURINARY DISORDERS

CENTRAL NERVOUS SYSTEM
Some form of spinal dysraphism including tethered cord,myelomeningocele, or lipomyelomeningocele is present innearly all patients, with recent reports ranging from 64% to100%.74,84,91,94 Neurologic impairment is variable and mayaffect bladder function, urinary continence, lower extremitymovement, and erectile function. Detailed postmortem micro-dissection studies have demonstrated both aberrant origin andvascular supply of the pelvic autonomic nerves,95 and thesenerves are at additional risk of iatrogenic injury during oper-ative repair. Other reported abnormalities include periventri-cular leukomalacia, hydrocephalus, hypoplastic cerebellum,and Chiari malformation.84
SKELETAL
Abnormalities of the spine, pelvis, and limbs have all been ob-served in the setting of cloacal exstrophy. Spinal anomalies, ex-cluding myelodysplasia, have been reported in 22% to 60%and consist mainly of absent or extra vertebrae, scoliosis,and kyphosis.90,96,97 The pelvic deformity is similar to thatof classic bladder exstrophy but typically more severe with sig-nificant widening of the pubic diastasis, external angling of theposterior and anterior segments, and external rotation and ab-duction of the iliac wings.70 A review by Jain and Weaverfound a 17% to 26% incidence of associated lower limb abnor-malities.98 Certain limbmalformations like club foot and equi-novarus deformities can be seen in association withmyelomeningocele, which often accompanies cloacal exstro-phy; however, a variety of true limb malformations includinghypoplasia, absence, split foot, and ectopic or additional digitshave also been observed.98
PRENATAL DIAGNOSIS
Early prenatal diagnosis allows time for thorough parentalcounseling and allows for consideration of pregnancy termi-nation. Prenatal diagnosis was first reported by Meizner andBar-Ziv in 1985,99 and since then, several authors have pro-posed criteria for the prenatal diagnosis of cloacal exstrophy.Principle findings include failure to visualize the urinarybladder along with a large midline anterior abdominal walldefect and/or lumbosacral myelomeningocele.87,100–102 Theprolapsed ileal segment, which may appear as an “elephanttrunk–like” mass on US, has also been reported as a path-ognomic finding.103 From a review of 22 cases, Austin andcolleagues102 developed a list of major and minor criteriafor prenatal US diagnosis on the basis of the frequency withwhich abnormalities were observed. Major criteria were thoseseen in greater than 50% of cases and included nonvisualiza-tion of the bladder (91%); a large, midline, infraumbilicalanterior abdominal wall defect or cystic anterior abdominalwall structure (82%); omphalocele (77%); and myelomenin-gocele (68%). Minor criteria were observed in less than 50%and consisted of lower extremity defects (23%), renal anom-alies (23%), ascites (41%), widened pubic arches (18%), nar-row thorax (9%), hydrocephalus (9%), and single umbilicalartery (9%).102
SURGICAL REPAIR
Immediate Postnatal Management
After delivery and stabilization of the newborn, exposed or-gans and mucosal surfaces including the omphalocele, blad-der, intestine, and myelomeningocele should be protectedby enclosing the infant’s lower torso in a bowel bag or by firstmoistening surfaces with saline and covering with sterile plas-tic wrapping.90 Urologic examination should attempt to notegenetic sex and size of hemibladder plates. Baseline renalfunction, electrolyte, and hematologic status should be deter-mined. Karyotyping can be performed if gender has not beenpreviously determined or is not obvious on examination. Ini-tial imaging should include plain films of the chest and spinealong with head, abdominal, renal, and spinal US. In the ab-sence of obvious spinal dysraphism, magnetic resonance im-aging (MRI) may be advisable for detection of occult lesions.Consultation should also be made to general surgery, neuro-surgery, and orthopedics for operative planning. Once the ini-tial evaluation has been completed, discussion may be hadwith the parents regarding gender assignment, surgical recon-struction, potential functional deficits, and overall expectedquality of life.
Principles of Repair
The surgical management of cloacal exstrophy is typically un-dertaken in the newborn period (48 to 72 hours) as a com-bined effort between pediatric surgery and urology. In thesetting of associated spinal dysraphism, neurosurgical consul-tation and closure should be undertaken as soon as the infantis medically stable. Early operation minimizes bacterial colo-nization of exposed viscera and may decrease the need for pel-vic osteotomy.68,104 The traditional approach of staged repairhas been thoroughly described by Gearhart and Jeffs.40,94
Complete primary repair has also been reported by Howelland colleagues,68 Zderic and colleagues,105 Hendren,106
and most recently by Mitchell and Plaire.75 It is generallyagreed that an individualized approach toward reconstruc-tion, whether in a single-staged or multistaged procedure, re-sults in the best long-term outcomes.107 The main goals ofreconstruction include secure abdominal wall and bladderclosure, preservation of renal function, prevention of shortgut syndrome, creation of functionally and cosmetically ac-ceptable genitalia, and attainment of urinary and fecalcontinence.73,94
Although various operative algorithms have been published,all approaches begin with initial separation of the interveningcecal plate from the two bladder halves, closure of the ompha-locele, and hindgut preservation (Fig. 120-19).68,71,72,75,107
In the past, the bowel was initially diverted through the creationof loop or end-ileostomies, and the hindgut segment was uni-formly discarded. This practice has since fallen out of favor inorder to maximize the absorptive capabilities of the intestinaltract.72,74 Currently, after tubularization of the exstrophied ce-cum, it is recommended that the hindgut segment be broughtout as an end-colostomy.92 In the rare instance when the hind-gut remnant is not used, it may be left as a mucous fistula foruse in future urologic or vaginal reconstruction.90
The omphalocele is reduced to assist abdominal wall clo-sure; however, in cases of large omphaloceles, complete initialreduction may not be possible. In this setting, a silo device
1527CHAPTER 120 BLADDER AND CLOACAL EXSTROPHY

may be used or the omphalocele may be allowed to re-epithelialize, converting it to a ventral hernia, which may berepaired at a later time (Fig. 120-20).94
The hemibladders are dissected and then reapproximatedin the midline. In infants with few other associated malforma-tions and who are medically stable, complete closure of the ab-dominal wall, bladder, and phallic halves may be undertaken atthis point in a single-stage procedure with or without pelvicosteotomy. If this is not possible at the initial setting, the twobladder halves can first be joined in the midline, recapitulatingthe appearance of classic bladder exstrophy, which can then berepaired in a staged fashion as described in the previous section.
Genital reconstruction consists of bringing the phallichalves together to create an appearance congruent with theassigned gender. In the male infant with cloacal exstrophy,the phallic halves are characteristically diminutive, widelyseparated, and asymmetric. Historically, genetically male in-fants were routinely assigned to female gender at the time ofinitial closure, undergoing orchiectomy and feminizing geni-toplasty.108 Recent data regarding gender identity outcomes ingender-reassigned cloacal exstrophy patients has suggested an
inherent preference toward male behaviors and sexual identi-ties in these patients.75,105,109 It remains a topic of continuedstudy and debate. Gender reassignment has since been largelyabandoned in the current management of cloacal exstrophy,though functional and aesthetic phallic reconstruction re-mains challenging. Vaginal reconstruction is necessary in fe-males and in gender-reassigned males and is accomplishedthrough the use of bowel or skin grafts.
Gastrointestinal reconstruction, in the form of a pull-through procedure, may be performed in select patients, sometime after initial diversion and abdominal closure. The deci-sion is based on the potential for fecal continence and maybe influenced by colonic length, ability to form solid stool,and the presence of anal stenosis versus imperforate anus.
Like those with classic bladder exstrophy, these patientswill also require the creation of antireflux and urinary conti-nence mechanisms. The presence of myelodysplasia in thesepatients usually necessitates augmentation cystoplasty witha bowel segment and intermittent catheterization in order toachieve continence. Continence procedures include creationof a neourethra, construction of a catheterizable abdominalstoma with concomitant bladder augmentation, and/or blad-der neck closure, the selection of which is influenced by thepresence of short gut syndrome, manual dexterity, degree ofmobility, and patient motivation.94
POSTOPERATIVE CONSIDERATIONS
Given the high incidence of short gut syndrome, fluid and nu-tritional status must be carefully monitored and the initial useof total parenteral nutrition (TPN) is advocated.110 The keys topostoperative success are similar to those for repair of classicbladder exstrophy. Patients are immobilized in some type oftraction device. In the setting of pelvic osteotomy, an externalfixator is left for 4 to 6 weeks postoperatively. Broad-spectrumantibiotics are administered to minimize risk of wound in-fection and urosepsis. In contrast to patients with classicbladder exstrophy, the presence of associated myelodysplasiain cloacal exstrophy generally precludes use of an epiduralcatheter. Pain control in cloacal exstrophy patients can bechallenging, and the involvement of the pediatric pain serviceis recommended. Finally, the importance of limiting abdomi-nal distension to ensure successful abdominal closure and
CA B
Ileum
Colon
FIGURE 120-19 Repair of cloacal exstrophy.A and B, The bowel and bladdermucosa are separated, and the ileocecal junction is tubularized and broughtout as an end-colostomy. The bladder halves are turned in, as in a complete exstrophy repair, with approximation of the pubic rami. C, Alternatively, thebladder halves are approximated in the midline and left open for staged repair if tubularization is not possible. The omphalocele is also closed.
FIGURE 120-20 If initial closure of the omphalocele is not possible, itmay be allowed to epithelialize, converting the omphalocele to a ventralhernia, which can be repaired at a later time.
1528 PART VIII GENITOURINARY DISORDERS

adequate drainage of both ureteral and bladder catheterscannot be understated.61,111,112 Following repair, close mon-itoring of the upper tracts by US is mandatory to observe foradequate renal growth and to detect evidence of obstructionor VUR, which has been reported in 50% to 60% of cloacalexstrophy patients after staged or complete primaryrepair.60,107
CONCLUSION
For the past 20 years, survival among patients with cloacalexstrophy has exceeded 90%.68,72,74,105 Death is typically re-lated to complications related to extreme prematurity, renalagenesis, or other complex malformations that are incompat-ible with life. It is interesting to note that cardiovascular anom-alies are rarely observed in the setting of cloacal exstrophy. Thevarious complications related to the management of patientswith cloacal exstrophy are similar to those of patients withclassic bladder exstrophy, as described in the previous section.Compared with those with classic exstrophy, however, cloacalexstrophy patients face additional challenges of achievingbowel and bladder continence secondary to the need for analreconstruction and the associated defect of spinal dysraphism.It must be stressed that multiple operations are the rule, andthese patients will likely face significant medical, psychologic,and social challenges throughout their lives. Advancements in
medical and surgical management continue to improve func-tional and quality of life outcomes in these patients, but it isimportant that these individuals remain under the care of amultidisciplinary team of providers who can offer medicalcare, psychologic support, and lifelong follow-up.
The complete reference list is available online at www.expertconsult.com.
SUGGESTED READINGS
Ebert AK, Reutter H, Ludwig M, Rosch WH. The exstrophy-epispadias com-plex. Orphanet J Rare Dis 2009;4:23.
Gearhart JP, Mathews R. The Exstrophy-Epispadias Complex: Research Con-cepts and Clinical Applications. New York: Kluwer Academic Publishers;1999.
Hernandez DJ, Purves T, Gearhart JP. Complications of surgical reconstructionof the exstrophy-epispadias complex. J Pediatr Urol 2008;4:460–466.
Husmann DA. Surgery insight: Advantages and pitfalls of surgical techniquesfor the correction of bladder exstrophy. Nat Clin Pract Urol 2006;3:95–100.
Ludwig M, Ching B, Reutter H, Boyadjiev SA. Bladder exstrophy-epispadiascomplex. Birth Defects Res A Clin Mol Teratol 2009;85:509–522.
Woodhouse CR, North AC, Gearhart JP. Standing the test of time: Long-termoutcome of reconstruction of the exstrophy bladder. World J Urol 2006;24:244–249.
Woo LL, Thomas JC, Brock JW. Cloacal exstrophy: A comprehensive review ofan uncommon problem. J Pediatr Urol 2009 Oct; (Epub ahead of print).
1529CHAPTER 120 BLADDER AND CLOACAL EXSTROPHY