Embed Size (px)
DESCRIPTION
Pediatric eye and vision
Citation preview

1

2
Pediatric Eye And VisionExamination
شکرالله شفائی کارشناس ارشد اپتومتری

3
Pediatric population can be divided into three subcategories: (Press LJ, Moore BD.1993)
■ Infants and toddlers (birth to 2 years, 11 months)
■ Preschool children (3 years to 5 years, 11 months)
■ School-age children (6 to 18 years).

4

5
Patient AgeAsymptomatic/ At-risk
Patient Age risk-freeAt-risk
Birth to 24 months
At 6 months of ageAt 6 months of age or as recommended
2 to 5 yrs.At 3 years of ageAt 3 years of age
or as recommended
6 to 18 yrs.Before first grade
and every 2 years
thereafter
Annually or as
recommended
Recommended Eye Examination Frequency for the Pediatric Patient (OPTOMETRIC CLINICAL PRACTICE GUIDELINE ; Mitchell M. Scheiman, 2002)

6
A. Examination of Infants and Toddlers
1 .General Considerations - time of examination; morning visit
- types of examination; objective - fast but exact; age appropriate
2 .Early Detection and Prevention3 .Examination Sequence
a. Patient History
■Nature of the presenting problem, including chief complaint ■Visual and ocular history
■General health history, including prenatal, perinatal, and postnatal history and review of systems
■Family eye and medical histories ■Developmental history of the child.

7
b. Visual Acuity
Assessment of visual acuity for infants and toddlers may include these procedures:
•Gross estimate of visual function at near •Fixation maintenance & preference tests
-10 prism diopter (PD) lens
•OKN •Preferential looking visual acuity test
•VEP

8
pincer grasp to pick up cake decoration ( or raisin).
Candy beads at 40 cm = 20/285 ( Frenkel & Evans, 1980)

9
lights on lights turned down.
Note marked retraction of the upper lids. indicating some visual function.

10
Fixation maintenance test
■To test central & steady fixation
■Shine a light at uncovered eye
■Estimate the position of the light reflexes (or angle Kappa); displaced +0.5 mm nasally
■Any deviation = eccentric fixation

11
Fixation preference test
■can be judged when obvious strabismus is present ■cover and uncover the fixing eye to force fixation to the
nonpreferred eye ■ observe the fixation pattern
- good vision in case of alternate fixation

12
Teller cards
-pack of 16 cards
-from 38.0 to 0.32 cycles/cm
-test dist. 38 cm for infants , 55 cm for toddlers

13
Spatial frequency paddles
-calibrated for a specific distance( 1 m)
-4 paddles and 6 different sp. fr. -hold the gray over one of sp. fr .
-separate the paddles and notice the fixation

14
Preferential looking tests of visionKeeler/Teller cards for infants

15

16
Normal levels of visionPreferential looking tests (Mayer et al, 1995)
1 month 24/400 – 20/1600
4 month 20/100 – 20/400
12 month 20/80 – 20/300

17
Vertical optokinetic nystagmus testing using an OKNdrum. If a vertical nystagmus can be elicited, vision is 20/400 or better.

18
vestibular-ocular reflex, which stimulates the semicircular canals, causing the eyes to deviate in the direction of rotation.

19
The early decreased visual acuity in the infant is due to:
1 -foveal cone immaturities; small and stumpy - at 4 years, the length of an adult cone
- at 3.5 – 4 years, adult level of cone density
2 -cortical immaturities
3 -incomplete myelination of the optic pathways

20
Cardiff acuity cards for toddlers; vanishing optotype
■in children from 1 to 3 years of age■ 11 sets of cards are available ; 20/400 to 20/20
■ test dis. 0.5 m and 1.0 m
■ present one set of cards and notice the fixation
■ better done binocularly first( Adoh and Woodhouse,1994)

21
Cardiff acuity test (Monocular; Adoh & Woodhouse 1994)
12-18 months(20/50-20/120) +0.4 to +0.8 L.MAR
18 -24 months( 20/25- 20/100)+0.1 to +0.7 L.MAR
24-30 months( 20/25-20/60) +0.1 to +0.5 L.MAR
30-36 months(20/20-20/40)+0.0 to +0.3 LMAR

22
c. Refraction
Traditional subjective procedures , ineffective with infants or toddlers because of short attention span and poor fixation. (Ciner EB, 1990)
The two most commonly used procedures are:
■Cycloplegic retinoscopy
■ Near retinoscopy

23
Take several precautions: (Gray L. 1979)
• Select the cycloplegic agent carefully (e.g., an increased response to drugs in fair-skinned children with blue eyes and more frequent or stronger dosages in darkly pigmented children ).
• Avoid overdosage (e.g., children with Down syndrome, cerebral palsy, trisomy 13 and 18, and other central nervous system disorders in whom there may be an increased reaction to cycloplegic agents, 1% tropicamide may be used).
• Be aware of biologic variations in children (e.g., low weight infants may require a modified dosage).

24
Cyclopentolate hydrochloride , the cycloplegic agent of choice
One drop , twice, 5 minutes apart, in each eye , - 0.5% for children from birth to 1 year
- 1% for older children. (Amos JF, 2001)
Spray administration of the drug , a viable alternative. (Amos JF,
2001) )1 (The child has less of an avoidance response
)2 (A single application can achieve both cycloplegia and pupillary dilation )3 (a mixture of 0.5% cyclopentolate, 0.5% tropicamide, and 2.5% phenylephrine is used.
Retinoscopy may be performed 20-30 minutes after instillation. (Bartlett JD, 1993 )

25
Near retinoscopy
May have some clinical value in the following situations:
• When frequent followup is necessary
• When the child is extremely anxious about instillation of cycloplegic agents
• When the child has had or is at risk for an adverse reaction to cyclopentolate or tropicamide.

26
■ Near retinoscopy , an alternative to cycloplegic refraction in children and infants (Mohindra 1977) .
■A dim retinoscope light is used as a fixation target and seen in complete darkness and perform retinoscopy using a lens rack or individual trial case lenses .
■Working at 50 cm, -1.25 DS rather than the standard -2.00 DS is added to the final retinoscopy result .(Mohindra 1977).
■The test is comparable to cycloplegic retinoscopy (e.g. Saunders & Westall1992).
■Add - 0.75 DS for infants (2 years) ; -1.00 DS for children (over 2 years) rather than the original 1.25 DS. (Saunders & Westall (1992)

27
REFLEX SCANING To get a quick idea of the prescription in both eyes,
)Lynne Speedwell, 2007(
-hold a pair of +2.00DS trial lenses in front of the child’s eyes in a
darkened room.
-With the child fixing on the retinoscope light at 50 cm,
quickly move the retinoscope horizontally and then vertically
across both eyes.

28
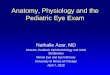
Refractive Error
Green line – cycloplegic refraction on infants (0-6mths)
Blue line – non-cycloplegic refraction on infants (0-6mths)
Red line – Refraction in older children
-6 -4 -2 0 2 4 6 8
0
10
20
30
40
50
60
70
80
Fre
qu
en
cy
(%
)
Spherical Equivalent (Dioptres) Adapted from Gwiazda et al 1993

29
d. Binocular Vision and Ocular Motility
•Observation
•Hirschberg test
•Krimsky test
•Brückner test
•Cover test

30

31
1 -General observation
■size of head
■ IPD
■ nose bridge
■ lid asymmetries
■ pupil or orbit position
■ epicanthal folds
lid asymmetries

32
2 -Hirschberg test
■ fixate your penlight at 50 cm
■ +0.5 mm ( nasal displacement of reflex)
■ note any asymmetric displacement
■ 1mm = 22 pd( Eskridge et al, 1988)

33
)A (The light reflection in the deviated right eye is temporal to the pupillary
center .
)B (Using a prism, the Krimsky test measures the amplitude of the esotropia by centering the light reflection in the right pupil.
3 -Krimsky test

34
4 -Brückner test
■ fixate an ophthalmoscope light at one meter
■ illuminate both eyes at the same time
■observe the relative whiteness & brightness of each pupillary reflex
■strabismus in case of whiter & brighter reflex
■it can help in the diagnosis of small angle strabismus (Miller et al. 1995)

35
5 -Cover test
-Targets; brightly colored with sound & fine detail -Use your thumb to avoid
distraction -For distance, moving targets

36
Binocular vision testing
■ intermittent esotropia should stop by the age of two months ■ exotropia by six months (Sondhi et al, 1988).
There are three types of prism test that are useful on young
children:
1 -The 20Δ base out prism test
2 -A 20Δ base in lens
3 -A 10Δ base down

37
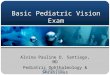
1 -The 20Δ base OUT prism test
■Assesses motor fusion and gross binocular function , not ideal for amblyopia assessment.
■The child fixes a toy and a 20Δ base OUT lens is placed in front of one eye.
■Both eyes should move in the direction of the prism apex and then the eye not being covered by the prism should be seen to
refixate to the centre .
■If no refixation movement is seen with one eye, it is likely that there is only weak fusion, suggesting one eye has poorer vision.

38
The 20 Δ base out test. A- fixation toy is used as a target and corrective eye B - movements are observed in response to a 20 diopters base out prism challenge.
A B

39
2 .A 20Δ base IN lens
■will assess fixation preference and will therefore demonstrate amblyopia.
■The prism is held in front of first one eye then the other, whilst the child fixes a light .
■The eye underneath the prism should move outwards (in the direction of the prism apex).
■If the eye under the prism is amblyopic, it will not move when the prism is placed in front of it .

40
A B
A 20Δ base IN lens test

41
3 .10Δ base DOWN
-In front of each eye in turn
-The upward vertical movement is easy for the observer to see.

42
e. Ocular Health Assessment and Systemic Health Screening
An evaluation of ocular health may include:
•Evaluation of the ocular anterior segment and adnexa
•Evaluation of the ocular posterior segment
•Assessment of pupillary responses
•Visual field screening (confrontation).

43
Testing visual fields in a young child. Begin by attractingthe child’s attention
straight ahead (top) .
Then move an object in from the side. A head movement to the side of the target (bottom) indicatesintact peripheral field.

44
B. Examination of Preschool Children

45
b. Visual Acuity •Lea Symbols chart
•Broken Wheel acuity cards
•HOTV test.
•Allen chart

46
The LH or Lea Cards
■make use of a logMAR scoring system and produce accurate results
■available in linear and single optotype formats and use shapes instead of letters
■at a dist. of 10 ft to 20 ft
Lea optotypes
A Lea symbol presented in a 'crowded box'

47
Broken Wheel acuity cards
-best for testing 3 year olds( McDonald and Chaudry, 1989)
-a set of 7 matched pairs of cards -20/20 to 20/100, held at 10 ft.
-should point to the car with broken wheels -if the child gets 4 of 4, go to the smaller sets

48
Kay picture cards
Having vision checked using the crowded 3 meter LogMAR

49
HOTV test
-for children , 21/2 to 5 yrs. of age. -no verbal response
-just point to the appropriate letter -at a dist. of 3 m.

50
The Allen Preschool Vision Test
ALLEN CARDS -7 optotypes for 2.5 to 5 yrs. of age
-20/30 , 20/40 ,20/50,20/70 ,20/100 ,20/200 -ask the child to call off the name of the pictures he see

51
Expected levels of vision
Age Vision
Neonate 6/300
1 month 6/200 – 6/90
3 months 6/60 – 6/36
6 months 6/60 – 6/36
9 months 6/36 – 6/24
1 year 6/24 – 6/12
2 years 6/12 – 6/9
3 years 6/9 – 6/6

52
c. Refraction
•Static retinoscopy
•Cycloplegic retinoscopy.

53
Cyclopentolate (1%) is the cycloplegic agent of choice. Two drops should be instilled, one at a time, 5 minutes apart, in each eye.
(Bartlett JD , 2001)
The use of a spray bottle to administer the drug is also effective for this age group.
Retinoscopy may be performed with a lens rack or loose lenses 20-30 minutes after instillation.(Bartlett JD, 1993)

54
d. Binocular Vision, Accommodation and Ocular Motility
•Cover test •Positive and negative fusional vergences (prism
bar/step vergence testing) •Near point of convergence (NPC)
•Stereopsis (Lang stereotest , Frisby tests) •Monocular estimation method (MEM) retinoscopy
•Versions.

55
e. Ocular Health Assessment and Systemic Health Screening
•Evaluation of the ocular anterior segment and adnexa
•Evaluation of the ocular posterior segment
•Color vision testing
•Assessment of pupillary responses
•Visual field screening (confrontation).

56
C. Examination of School-Age Children

57
b. Visual Acuity
LogMAR chart

58
c. Refraction
•Static (distance) retinoscopy
•Cycloplegic retinoscopy
•Subjective refraction.

59
d. Binocular Vision, Accommodation ,and Ocular Motility
•Cover test •Near point of convergence (NPC)
•Positive and negative fusional vergences, AC/A •Accommodative amplitude and facility,NRA,NPA •Monocular estimation method (MEM) retinoscopy
•Stereopsis (random dot stereopsis test) •Versions
- assessment of stability of fixation - saccadic function ,
- pursuit function
BV equipment

60
Cover-uncover test

61
Alternate cover test

62
The near point of convergence (NPC) is performed with a 6/9 target on a fixation stick
NPC assessment
Fusional reserves assessment

63
The negative/positive relative accommodation)NVA/PRA (is done in the phoropter with a 6/9 target
at 40cm

64Measuring the fusional reserves with a prism bar

65
The monocular/binocular accommodative flippers (MAF/BAF) is performed with ±2D flippers and a 6/9 target on a fixation stick held at 40cm

66
e. Ocular Health Assessment and Systemic Health Screening
•Evaluation of the ocular anterior segment and adnexa
•Evaluation of the ocular posterior segment •Measurement of intraocular pressure
•Color vision testing •Assessment of pupillary responses
•Visual field screening (confrontation).

67
Peripheral visual field assessment by confrontation

68
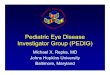
Finger mimicking visual fields. The child is asked to show the same number of fingers as the examiner. These should be displayed quickly to avoid fixation artifact.

69
Thank you