Embed Size (px)
Citation preview
Patients with Permanently Implant Radioactive Sources Requiring Unrelated Surgery
Risk Assessment
Regulatory and Local Policies
Pre-Surgery Risk
Reduction
Surgery / Intervention
Post-Surgery Risk
Reduction
Best Practices
Policy Changes
PS Basran WA Beckham
P Baxter
Download the poster (PDF) http://goo.gl/6xSmzd Download the long abstract (PDF) http://goo.gl/IpKESV View the Prezi http://goo.gl/Z1GvFq
See the multimedia enriched poster in Prezi
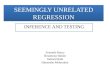
The Problem Permanent implant of sealed radioactive sources is an effective technique for treating cancer. There may be instances where these patients must undergo unrelated surgical procedures when the radioactive material remains active enough to pose risks. This work explores these risks, discusses strategies to mitigate those risks, and describes a case study for a permanent I-125 prostate brachytherapy implant patient who developed adenocarcinoma of the lower sigmoid and required surgery 6 months after brachytherapy. The tumor volume extended to the recto-sigmoid junction. Surgery involved laparotomy and removal of rectal and sigmoid volumes along with reconstruction. The patient was implanted with 85 I-125 seeds.
Is it really a problem? If a patient has a surgical procedure that may involve interrogation of the implanted region, then there should be an assessment of the risk of radiation contamination and the risk of compromising the brachytherapy treatment itself. Specific considerations include: the location of the surgery is near implant; and, the surgical intervention could result in dislodging of radioisotopes such that the treatment may be compromised or that there is an increased risk of exposure to staff; and, the radioisotope has not decayed to background levels; and, the surgery cannot be postponed.
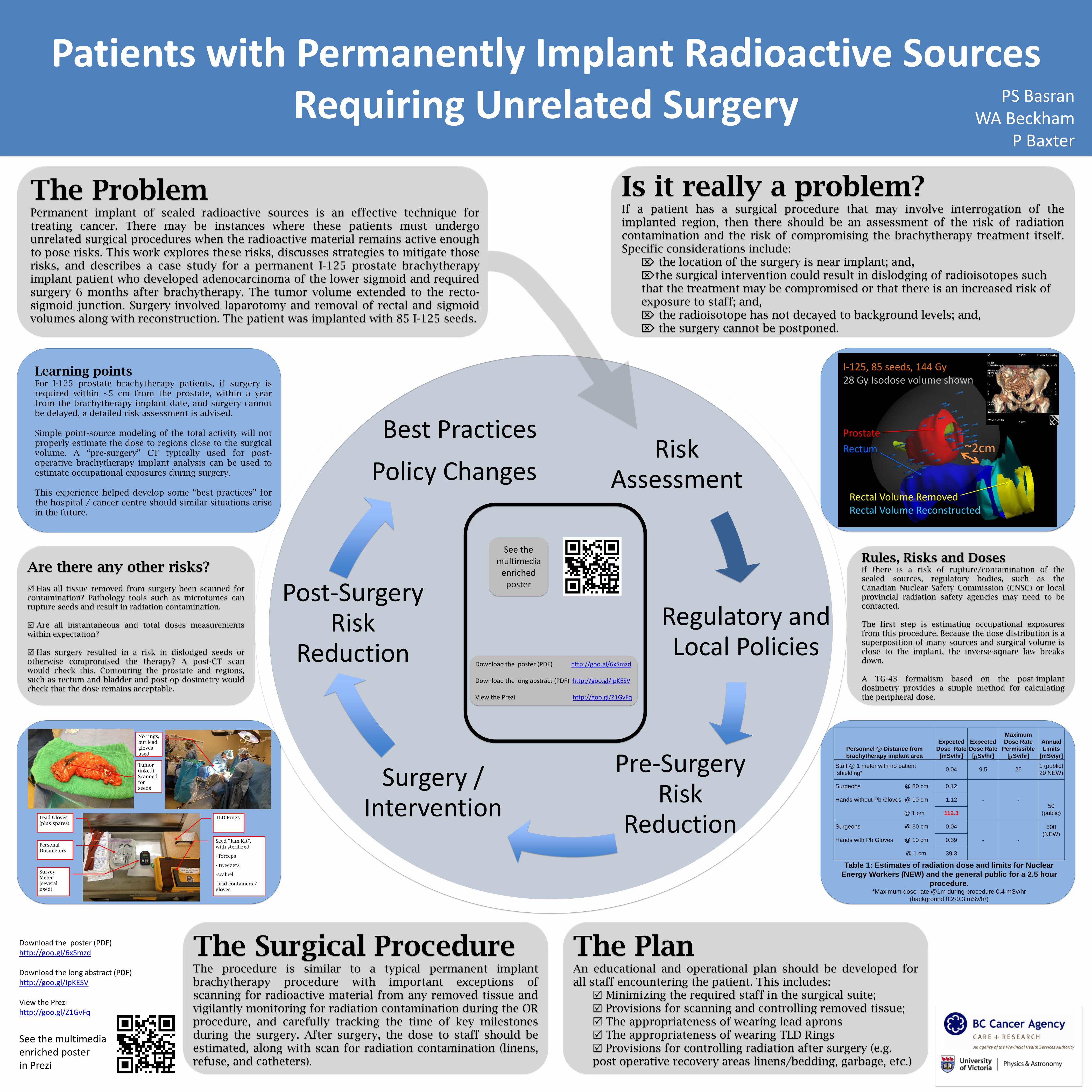
Rules, Risks and Doses If there is a risk of rupture/contamination of the sealed sources, regulatory bodies, such as the Canadian Nuclear Safety Commission (CNSC) or local provincial radiation safety agencies may need to be contacted. The first step is estimating occupational exposures from this procedure. Because the dose distribution is a superposition of many sources and surgical volume is close to the implant, the inverse-square law breaks down. A TG-43 formalism based on the post-implant dosimetry provides a simple method for calculating the peripheral dose.
The Plan An educational and operational plan should be developed for all staff encountering the patient. This includes:
Minimizing the required staff in the surgical suite; Provisions for scanning and controlling removed tissue; The appropriateness of wearing lead aprons The appropriateness of wearing TLD Rings Provisions for controlling radiation after surgery (e.g. post operative recovery areas linens/bedding, garbage, etc.)
The Surgical Procedure The procedure is similar to a typical permanent implant brachytherapy procedure with important exceptions of scanning for radioactive material from any removed tissue and vigilantly monitoring for radiation contamination during the OR procedure, and carefully tracking the time of key milestones during the surgery. After surgery, the dose to staff should be estimated, along with scan for radiation contamination (linens, refuse, and catheters).
Are there any other risks?
Has all tissue removed from surgery been scanned for contamination? Pathology tools such as microtomes can rupture seeds and result in radiation contamination.
Are all instantaneous and total doses measurements within expectation?
Has surgery resulted in a risk in dislodged seeds or otherwise compromised the therapy? A post-CT scan would check this. Contouring the prostate and regions, such as rectum and bladder and post-op dosimetry would check that the dose remains acceptable.
Personnel @ Distance from
brachytherapy implant area
Expected
Dose Rate
[mSv/hr]
Expected
Dose Rate
[mSv/hr]
Maximum
Dose Rate
Permissible
[mSv/hr]
Annual
Limits
[mSv/yr]
Staff @ 1 meter with no patient
shielding* 0.04 9.5 25
1 (public)
20 NEW)
Surgeons @ 30 cm 0.12
- - 50
(public)
500
(NEW)
Hands without Pb Gloves @ 10 cm 1.12
@ 1 cm 112.3
Surgeons @ 30 cm 0.04
- - Hands with Pb Gloves @ 10 cm 0.39
@ 1 cm 39.3
Table 1: Estimates of radiation dose and limits for Nuclear
Energy Workers (NEW) and the general public for a 2.5 hour
procedure. *Maximum dose rate @1m during procedure 0.4 mSv/hr
(background 0.2-0.3 mSv/hr)
Learning points For I-125 prostate brachytherapy patients, if surgery is required within ~5 cm from the prostate, within a year from the brachytherapy implant date, and surgery cannot be delayed, a detailed risk assessment is advised. Simple point-source modeling of the total activity will not properly estimate the dose to regions close to the surgical volume. A “pre-surgery” CT typically used for post-operative brachytherapy implant analysis can be used to estimate occupational exposures during surgery. This experience helped develop some “best practices” for the hospital / cancer centre should similar situations arise in the future.
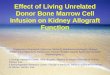
Lead Gloves (plus spares)
Personal Dosimeters
Survey Meter (several used)
TLD Rings
Seed “Jam Kit”, with sterilized
- forceps
- tweezers
-scalpel
-lead containers / gloves
No rings, but lead gloves used
Tumor (inked) Scanned for seeds
I-125, 85 seeds, 144 Gy 28 Gy Isodose volume shown Prostate
Rectum ~2cm
Rectal Volume Removed Rectal Volume Reconstructed
Download the poster (PDF) http://goo.gl/6xSmzd Download the long abstract (PDF) http://goo.gl/IpKESV View the Prezi http://goo.gl/Z1GvFq
See the multimedia
enriched poster