Embed Size (px)
Citation preview

Keep Smiling….!
“It will help you to grow up in greater happiness & Love for each other."
Mother Teresa1910-1997, Roman Catholic Missionary

Pathology of Pathology of Hypertension:Hypertension:
Dr. Venkatesh M. Shashidhar.Associate Professor & Head of Pathology

Introduction
• “Sustained increase in blood pressure”• Systolic >140, Diastolic > 90 mm of Hg*• Normal* < 130 <85 (120/80 +/- 10/5)• Mild + 20, Moderate +40 Severe +80• Malignant - > 210/120

Hypertension - Introduction• Silent Killer – painless – complications• dizziness, headache, and visual difficulties,• It is the leading risk factor – MI, DM, Stroke• Responsible for the majority of office visits, • Number one reason for drug prescription.• 25% of population, <35% aware…<5% ..! • Complications bring to diagnosis but late…• Chronic, end organ & vascular damage

Regulation of BP:
BP = Cardiac Output x Peripheral Resistance• Endocrine Factors
– Renin, Angiotensin, ANP, ADH, Aldosterone.• Neural Factors
– Sympathetic & Parasympathetic• Blood Volume
– Sodium, Mineralocorticoids, ANP• Cardiac Factors
– Heart rate & Contractility.

Etiologic Classification:• Essential (Primary) Hypertension (95%)
– Unknown etiology. Life style, genetic, …• Secondary Hypertension (5-10%)
– Renal – GN, RAS, Renin tumors– Endocrine – Cushing, OCP, Thyrotoxicosis
Myxdema, Pheochromocytoma, Acromegaly.– Vascular – Coarctation of Aorta, PAN, Aortic
insufficiency.– Neurogenic – Psychogenic, Intracranial
pressure, olyneuritis etc.

Etiology:
• Secondary - Known abnormal control.– Renal disorders – Renin-Angiotensin.
Sodium retention, ADH, Aldosterone.– Cushings, Pheochromocytoma,
• Essential - Etiology is multifactorial.– Increased peripheral resistance
(sympathetic tone)– stress, hormonal, neural.– Genetic, familial, life style.

Pathogenesis of Renovascular HTN:GFR
Renin by JGA
Angiotensin II
Vasoconstriction P. Resistance
Sodium RetentionBlood Volume
Aldosterone
Hypertension

Malignant Hypertension:
• Rapidly progressive end organ damage.• May complicate any type of HTN.• Artery necrosis with thrombosis.• Rapidly developing renal failure.• Hypertensive encephalopathy. • Left ventricular failure.• less time No hypertrophy …!

Morphology:• Large Blood Vessels – Macroangiopathy.
– Atherosclerosis and its complications.• Small Blood Vessels – Microangiopathy.
– Hyperplastic arteriolosclerosis. (thick arterioles)• Heart
– LVH, Hypertensive cardiomyopathy IHD, MI.• Kidney
– Benign nephrosclerosis.• Eyes:
– Hypertensive retinopathy• Brain:
– Haemorrhage, infarction, – splinter hemorrhages & Lacunar infarcts.

Pathogenesis of vascular changes.
•Arteriolosclerosis•Rupture•Aneurysm•Rupture.
Ischemia, Aneurysm, Rupture


Left Ventricular Hypertrophy:
Left Ventricular HypertrophyLeft Ventricular Hypertrophy

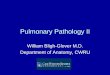
Hyperplastic Arteriolosclerosis:
Onion Skin ThickeningOnion Skin ThickeningOf arterioles.Of arterioles.
Narrow LumenNarrow Lumen

Nephrosclerosis in HPTN:
Artery Sclerosis
Artery Sclerosis
PCT hydropic deg.

Nephrosclerosis in HPTN:
Artery Sclerosis
Glom. Sclerosis
Artery Sclerosis
PCT hydropic deg.

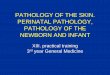
Necrotizing arteriole: Malignant HPTN
Fibrinoid NecrosisFibrinoid Necrosis
ThrombosisThrombosis

Subarachnoid Haemorrhage:
Cerebral Blood vessels
Special features:• Thin walled*• End arteries*• Cong. Aneurisms

Cerebral Infarction (Stroke) :HaemorrhagicHaemorrhagic
NecrosisNecrosis

Lacunar Infarct:• Chronic hypertension• Arteriolosclerosis of
deep penetrating arterioles of brain stem.
• Single or multiple cavitary infarcts – lacunes.
• Lenticular nucleus, thalamus
• Slit Haemorrhages.

Benign Nephrosclerosis:
Leathery Granularity Leathery Granularity due to minute scarringdue to minute scarring

Cerebral Infarction:

Renal Causes :
• Renal artery atherosclerosis • Polycystic Disease• Glomerulonephritis (A/C)• Renal artery stenosis• Renal vasculitis – SLE• Renin producing tumors.
Polycystic Kidney ->

Renal Artery stenosis - Atrophy
Leathery GranularityBenign Nephrosclerosis

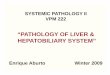
Normal Retina - Fundoscopy

Hypertensive Retinopathy:• Arteriosclerosis cause the arteriole light reflex to
become broad and dull – silver wire• Generalized or focal retinal arteriolar constriction
– pale.• Superficial flame-shaped hemorrhages.• Small white foci of retinal ischemia (cotton-wool
spots).• Yellow hard exudates, due to lipid deposition
deep in the retina.

Hypertensive Retinopathy:• Grade I – Thickening of
arterioles.• Grade II – Focal Arteriolar
spasms. Vein constriction. (AV nipping)
• Grade III – Hemorrhages (Flame shape), dot-blot and Cotton wool (ischemia) and hard waxy exudates (lipid deposition).
• Grade IV - Papilloedema

G Protien Polymorphisms in Metabolic Syndrome-X
• A common C825T polymorphism in the gene GNB3, which encodes the β3 subunit of heterotrimeric G proteins, was identified in cell lines from patients with hypertension. The 825T allele is associated with increased intracellular signal transduction. Many population-based and case-control studies in different ethnicities have investigated an association between this polymorphism and hypertension, obesity, and atherosclerosis. A critical assessment of published studies suggests that 825T allele carriers have an increased risk for hypertension combined with features of the metabolic syndrome, such as dyslipidemia, hypercholesterolemia, insulin resistance, and obesity. It is anticipated that this polymorphism will be used in clinical practice to better characterize hypertension and for individualized treatment regimens.

Conclusions:
• Persistent increased blood pressure..• 95% Essential, 5% secondary - Renovascular• Benign and Malignant types (>120 Diastolic)• Vessel damage & Arteriolosclerosis • Complicates - Atherosclerosis, Diabetes, IHD• Ischemia or Infarction in end organs.• Kidney, Brain, Heart & Eyes.• Complications: Nephrosclerosis, renal damage,
IHD, MI, Stroke & Retinopathy.

Self Assessment Questions:• Define essential, hypertension?• Briefly describe pathogenesis of renal damage in
hypertension.• Classify hypertension, briefly describe pathogenesis in
each?• Summarize common complications of hptn?• What is nephrosclerosis? Briefly describe its
pathogenesis?• What is meant by malignant hypertension? Briefly
describe clinical and pathological features?• What are lacunar infarcts? arteriolosclerosis?• How does hptn causes stroke? Damage heart?