Embed Size (px)
DESCRIPTION
Citation preview

Pathology of Epilepsy
Mark CohenDepartment of Pathology
University Hospitals Case Medical CenterJanuary 6th, 2009

'He was thinking, incidentally, that there was a moment or two in his epileptic condition almost before the fit itself (if it occurred in waking hours) when suddenly amid the sadness, spiritual darkness and depression, his brain seemed to catch fire at brief moments....His sensation of being alive and his awareness increased tenfold at those moments which flashed by like lightning. His mind and heart were flooded by a dazzling light. All his agitation, doubts and worries, seemed composed in a twinkling, culminating in a great calm, full of understanding...but these moments, these glimmerings were still but a premonition of that final second (never more than a second) with which the seizure itself began. That second was, of course, unbearable.'

Learning ObjectivesLearning Objectives
• Discuss the Blumcke classification of medial temporal lobe sclerosis, relating histopathologic features to surgical outcomes
• Discuss the Palmini classification of cortical dysplasia, relating histopathologic features to surgical outcomes
• Define “dual pathology” in temporal lobe epilepsy, and the relative contribution of hippocampal and neocortical lesions
• List two additional neuropathologic lesions which commonly present with epilepsy

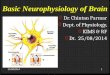
Pathology of TLEPathology of TLE
5%No Pathology
5%Dual Pathology
25%Focal lesions
65%Ammon’s Horn
Sclerosis
Blumcke I, Thom M, Wiestler OD. Ammon's horn sclerosis: a maldevelopmental disorder associated with temporal lobe
epilepsy. Brain Pathol. 2002 Apr;12(2):199-211



Wyler grading of HS (1992)Wyler grading of HS (1992)
��
>50% neuronal loss involving all hippocampal sectorsGrade 4
>50% neuronal loss CA1, CA3, and/or CA4; CA2 sparedGrade 3
10-50% neuronal loss in CA1, CA3, and/or CA4Grade 2
0-10% neuronal loss in CA1, CA3, and/or CA4Grade 1
AR Wyler, FC Dohan, JB Schweitzer, AD Berry A grading system for mesial temporal pathology (hippocampal sclerosis) from anterior temporal lobectomy - J Epilepsy, 1992



Blumcke I, et. Al. A new clinico-pathological classification system for mesial temporal sclerosis.
Acta Neuropathol (Berl). 2007 Mar;113(3):235-244.

Blumcke I, et. Al. A new clinico-pathological classification system for mesial temporal sclerosis.
Acta Neuropathol (Berl). 2007 Mar;113(3):235-244.


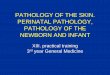
Blumke classification of MTSBlumke classification of MTS
CA1 preserved, moderate loss in other sectors (endfolium sclerosis)
o
MTS type 3 (5%)
M
Severe CA1 loss, mild loss in other sectors (CA1-sclerosis)
o
MTS type 2 (5%)
M
Severe neuronal loss involving all sectors (= Wyler grade 4)
(
MTS 1b (50%)
M
“Classic” – severe CA1 loss, moderate loss in other sectors MTS 1a (20%)
M
Neuronal cell loss within 1st SD compared to controlsNo MTS (20%)
N
A new clinico-pathological classification system for mesial temporal sclerosis.
Acta Neuropathol (Berl). 2007 Mar;113(3):235-244.

Blumcke type MTS
Age of initial precipitating injury
or first seizure (years)
Excellent outcome at 1 year post surgery (%)
Fair outcome at 1 year post surgery
(%)
No MTS 16 60 20
MTS type 1a 2 70 10
MTS type 1b 3 70 10
MTS type 2 6 70 10
MTS type 3 13 30 40

Generalized malformations of cortical developmentGeneralized malformations of cortical development
sporadicHME
SPPX2,sporadicPolymicrogyria
Filamin 1FLN 1PV nodular heterotopia
DoublecortinDCXLaminar heterotopia
PAF-acetylhydrolaseDoublecortinReelin
LIS1
DCX(XLIS)
D
RLN
LissencephaliesProteinGenesMalformation
Guerrini R, Dobyns WB, Barkovich AJ. Abnormal development of the human cerebral cortex: genetics, functional consequences and
treatment options. Trends Neurosci. 2008 Mar;31(3):154-62.

Type of cortical dysplasia
Age at onset of seizures (years)
Age at surgery (years)
Hemispheric (with hemimegalencephaly)
0.1 1
Hemispheric (without hemimegalencephaly)
0.8 3.5
Multilobar 0.7 4.5
Lobar 1.2 5
Focal 1.7 7.5
Cepeda C, et. Al. Epileptogenesis in pediatric cortical dysplasia: the dysmature cerebral developmental hypothesis.
Epilepsy Behav. 2006 Sep;9(2):219-35

MCD pathology by MRI typeMCD pathology by MRI type
00153055Immature neurons
8035452045Balloon cells
10253555100Layer I neurons
1025806580PMG
7040703590Cytomegalic neurons
100909010090Dysmorphic neurons
100100100100100WM neurons
FocalLobarMultilobarHemi CDHMEPath (%)

Palmini classification
Mild Malformations of Mild Malformations of Cortical DevelopmentCortical DevelopmentType I: Ectopic neurons Type I: Ectopic neurons in/near Layer 1in/near Layer 1
Type 2: Neuronal Type 2: Neuronal heterotopia outside Layer 1heterotopia outside Layer 1
Focal Cortical Focal Cortical DysplasiasDysplasias
Type IA: Dyslamination +/- Type IA: Dyslamination +/- mild MCDmild MCD
Type IB: IA + giant or Type IB: IA + giant or immature neuronsimmature neurons
Type IIA: Dysmorphic Type IIA: Dysmorphic neurons neurons sanssans balloon cells balloon cells
Type IIB: Dysmorphic Type IIB: Dysmorphic neurons neurons avecavec balloon cells balloon cells
Palmini A, Najm I, Avanzini G, Babb T, Guerrini R, Foldvary-Schaefer N, Jackson G, Luders HO, Prayson R, Spreafico R, Vinters HV. Terminology and classification of the
cortical dysplasias. Neurology. 2004 Mar 23;62(6 Suppl 3):S2-8





• •

Dual Pathology: HS + FCDDual Pathology: HS + FCD
• 12 male patients12 male patients– Age of onset 10 years (<1 – 29)Age of onset 10 years (<1 – 29)
AA
– Age at invasive EEG 30 years (6 – 50)Age at invasive EEG 30 years (6 – 50)
AA
• 113 seizures + interictal data from 113 seizures + interictal data from depth electrodes in HC & subdural depth electrodes in HC & subdural electrodes over temporal neocortexelectrodes over temporal neocortex
• 40% of seizures from AHC, 35% from 40% of seizures from AHC, 35% from TN, and 25% from bothTN, and 25% from both
Fauser S, Schulze-Bonhage A. Epileptogenicity of cortical dysplasia in temporal lobe dual pathology: an electrophysiological study with invasive recordings.
Brain. 2006 Jan;129(Pt 1):82-95




Pathologic diagnosis % of cases
Cortical dysplasia (including Tuberous Sclerosis)
20
Vascular malformations (including Sturge-Weber disease)
20
Glioneuronal tumors 20
Other gliomas 10
Gliosis 30
52 patients with occipital lobe epilepsy
Binder DK, Von Lehe M, Kral T, Bien CG, Urbach H, Schramm J, Clusmann H.Surgical treatment of occipital lobe epilepsy.
J Neurosurg. 2008 Jul;109(1):57-69.



Rasmussen syndromeRasmussen syndrome
• 45 patients (27F, 18M)45 patients (27F, 18M)
44
• Age at onset: 7 +/- 3 yearsAge at onset: 7 +/- 3 years• Age at hemispherectomy: 9.5 +/- 4 yearsAge at hemispherectomy: 9.5 +/- 4 years• Duration of symptoms: 0.5 – 14 yearsDuration of symptoms: 0.5 – 14 years
Pardo CA, Vining EP, Guo L, Skolasky RL, Carson BS, Freeman JM. The pathology of Rasmussen syndrome: stages of cortical involvement and
neuropathological studies in 45 hemispherectomies. Epilepsia. 2004 May;45(5):516-26.


RS: Pathologic stagingRS: Pathologic staging
Pan-laminar cavitation &/or gliosis4
Pan-laminar degeneration & gliosis3
Pan-laminar inflammation & gliosis2
Mild focal inflammation1
Normal cortex0

Learning ObjectivesLearning Objectives
• Discuss the Blumcke classification of medial temporal lobe sclerosis, relating histopathologic features to surgical outcomes
• Discuss the Palmini classification of cortical dysplasia, relating histopathologic features to surgical outcomes
• Define “dual pathology” in temporal lobe epilepsy, and the relative contribution of hippocampal and neocortical lesions
• List two additional neuropathologic lesions which commonly present with epilepsy

" For several instants I experience a " For several instants I experience a happiness that is impossible in an ordinary happiness that is impossible in an ordinary state, and of which other people have no state, and of which other people have no conception. I feel full harmony in myself conception. I feel full harmony in myself and in the whole world, and the feeling is and in the whole world, and the feeling is so strong and sweet that for a few seconds so strong and sweet that for a few seconds of such bliss one could give up ten years of such bliss one could give up ten years of life, perhaps all of life.of life, perhaps all of life.
I felt that heaven descended to earth and I felt that heaven descended to earth and swallowed me. I really attained god and swallowed me. I really attained god and was imbued with him. All of you healthy was imbued with him. All of you healthy people don't even suspect what happiness people don't even suspect what happiness is , that happiness that we epileptics is , that happiness that we epileptics experience for a second before an attack."experience for a second before an attack."