Embed Size (px)
DESCRIPTION
Citation preview

PAIN & ADDICTION
Presented by:Stacy Seikel, MD
Board Certified Addiction MedicineBoard Certified Anesthesiology

DISCLAIMERDISCLAIMERStacy Seikel, MDStacy Seikel, MD
Medical Director, The Center for Drug-Free Living, Inc., Orlando, FL, Orlando, FL
Member: ASAM, FSAM, AMA, FMA, OCMS Officer/ Board Position: FSAM/OCMS Board Certified, Addiction Medicine,
Anesthesiology Medical Review Officer (MRO) Speakers Bureau: Reckitt Benckiser, Forrest,
Alkermes Some slides borrowed from Reckitt Benckiser,
Sanford Silverman, MD, Berndt Wollschlaeger, MD

OBJECTIVES
Discuss Pain and Addiction as co-morbid disease states
Discuss Epidemiology of Prescription Drug Abuse
Discuss methadone and buprenorphine and their roles in pain and addiction medicine

Pain and Addiction as Disease States

PAIN
DEFINITION: an unpleasant sensory &
emotional experience associated with actual
tissue damage or described in terms of such
damage.

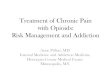
Analgesia and the Pain Pathway
Adapted from Gottschalk A, Smith DS. Am Fam Physician. 2001;63:1979-84.
Descending modulation
Dorsal horn
Ascendingsignalsinput
Spinothalamic tract
Dorsal root ganglion
Peripheral nerve
Peripheral nociceptors
Pain
Trauma
Local anestheticsOpioids 2 agonists
Opioids 2 agonists Centrally acting analgesicsCOX-2–specific inhibitorsTraditional NSAIDs
Local anestheticsAEDs
Local anesthetics CorticosteroidsTraditional NSAIDsCox-2–specific inhibitorsSubstance P inhibitorsOpioidsBaclofenClonidine
Adapted from Gottschalk A, Smith DS. Am Fam Physician. 2001;63:1979-84.Adapted from Gottschalk A, Smith DS. Am Fam Physician. 2001;63:1979-84.Adapted from Gottschalk A, Smith DS. Am Fam Physician. 2001;63:1979-84.Adapted from Gottschalk A, Smith DS. Am Fam Physician. 2001;63:1979-84.

Opioid Dependence (DSM-IV) – AKA Addiction
(3 or more within one year)
Tolerance Withdrawal Larger amounts/longer period than intended Inability to/persistent desire to cut down or control Increased amount of time spent in activities necessary to
obtain opioids Social, occupational and recreational activities given up
or reduced Opioid use is continued despite adverse consequences

Addiction
… a primary, chronic, neurobiological disease, with genetic, psychosocial, and environmental factors influencing the development and manifestations. It is characterized by behaviors that include one or more of the following:
Impaired control over drug use Compulsive use Continued use despite harm Craving (ASAM, 2001)

Cami, J. et al. N Engl J Med 2003;349:975-986
Neural Reward Circuits Important in the Reinforcing Effects of Drugs of Abuse

What Addiction Isn’t:Physical Dependence
Pharmacologic effect characteristic of opioids
Withdrawal or abstinence syndrome manifest on abrupt discontinuation of medication or administration of antagonist
Assumed to be present with regular opioid use for days-to-weeks
Becomes a problem if:Opioids not tapered when pain resolvesOpioids are inappropriately withheld

What Addiction Isn’t:Tolerance
Pharmacologic effect characteristic of opioids Need to increase dose to achieve the same effect or
diminished effect from same dose Tolerance to various opioid effects occurs at
differential rates Tolerance to non-analgesic effects often beneficial to
patients (sedation, respiratory depression) Analgesic tolerance is rarely the dominant factor in
the need for opioid Patients requiring dose escalation most often have a
change in pain stimulus (disease progression, infection, etc.)
(Foley, 1991)

Addiction
Compulsive Use Loss of control Continued use despite adverse
consequences

“Pseudo-Addiction”
Pattern of drug seeking behavior of pain patients receiving inadequate pain management that can be mistaken for addictionCravings and aberrant behaviorConcerns about availability“Clock-watching”Unsanctioned dose escalation
Resolves with reestablishing analgesia
Weissman, DE, Haddox, JD. Opioid pseudo addiction-an latrogenic syndrome. Pain 1989, 36-363.

What is the Risk of Addictionand Aberrant Behavior?
Boston collaborative Drug Surveillance Project: Porter and Jick, 1980. NEJM. 4 cases of addiction in 11,882 patients with no prior
history of abuse who received opioids during inpatient hospitalization.
Dunbar and Katz, 1996, JPSM. 20 patients with both chronic: pain and substance abuse
problems on chronic opioid therapy Nine out of 20 abused medication Of the 11 who did not abuse the medications, all were
active in recovery programs with good family support

Spectrum of Risk of Addiction or Aberrant Behavior
<1 %
~ 45%
LOWShort-termExposure toOpioids in
Non-addictsPorter and Jick
HIGHLong-term
Exposure toOpioids inAddicts,
Dunbar and Kafz
Where is your patient ?

Differential Diagnosis of Aberrant Drug-Taking Attitudes and Behavior
Addiction Pseudo-addiction (inadequate analgesia) Other psychiatric diagnosis
EncephalopathyBorderline personality disorderDepressionAnxiety
Criminal Intent(Passik & Portenoy 1996)

Aberrant Drug-taking Behaviors:
The Model
Probably more predictive Selling prescription drugs Prescription forgery Stealing or borrowing
another patient’s drugs Injecting oral formulation Obtaining prescription drugs
from non-medical sources Concurrent abuse of related
illicit drugs Multiple unsanctioned dose
escalations Recurrent prescription losses
Probably less predictive Aggressive complaining about
need for higher doses Drug hoarding during periods
of reduced symptoms Requesting specific drugs Acquisition of similar drugs Unsanctioned dose escalation
1-2 times Unapproved use of the drug to
treat another symptom Reporting psychic effects not
intended by the clinician
Passik and Portency, 1998

Opioid Addiction
Opioid addiction is a chronic, progressive, relapsing medical condition
Profound neurobiologic changes accompany the transition from opioid use to opioid addiction
Pharmacologic treatments are effective in normalizing the neurobiologic status, decreasing illicit opioid use, medical and social complications

AddictionPain
• High risk
• Costs
• Prescription abuse
• Morbidity & Mortality
The Nexus Of Pain And Addiction Is A Major Contributor To Current Epidemic

Epidemiology:Pain, Prescription Opioid Abuse

PAIN FACTS
Pain costs $150 billion annually 65 Million Americans suffer painful
disability 90% of all diseases noticed due to pain Untreated pain results in
unemployment Untreated pain associated with alcohol
and medication abuse 90% of patients in US pain clinics are
taking opioid analgesics

Factors Responsible For Increased Demand In
Managing Chronic Pain Pharmaceutical companies marketing Numerous organizations providing guidelines Patient advocacy groups Enactment of Patient’s bill of rights in many
states Unproven regulations by JCAHO misunderstood
by media and public Perceived patient’s right to pain relief Increased availability to internet “Pill Mills” High street value of prescription drugs Perceived legitimacy and safety prescription
drugs (pharm parties)

Prescription Opioid Abuse
Has always existed Recent explosive increase parallels that
of demand for pain management Paradigm shift in 1990’s to aggressively
treat pain Pain is the 5th vital sign Epidemic is the byproduct of compassion
and fundamental lack of understanding of complex nature of pain and nexus of chemical dependency (addiction)

Drug Diversion
Doctor shopping Internet sales Drug theft Improper prescribing Sharing amongst family and friends Diversion and abuse of methadone

Birnbaum HG et al. Clin J Pain. 2006;22:667-676.
Prescription Opioid Abuse Is a Significant
and Costly Public Health Problem
Health Care30%
Workplace53%
Criminal Justice17%
$4.6 billion
$1.4 billion
$2.6 billion
Total cost of prescription opioid abuse in the United States was $8.6 billion in 2001 and continues to grow.

Annual Numbers of New Nonmedical Users of Pain Relievers, by Age at Initiation: 1965-2003, SAMHSA

Drug Mortality Rate, Source, and Misuse of Prescription Drugs: Data from the 2002,
2003, and 2004 National Surveys on Drug
Use and Health, SAMHSA

Increase in New Starts of Prescription
Opioid Abuse Among Teenagers
Adapted from Manchikanti L. Pain Physician. 2006;9:287-321.
700
600
500
400
300
200
100
0
Pe
rce
nt
Inc
rea
se
1992 2003
542%—Incidence of new starts of prescriptionopioid abuse among teenagers
150%—Prescriptions written for controlled substances
14%—US population
212%----Number of 12-17 year olds abusing CS
81%---Adults abusing controlled substances

Past Year Users of Selected Drugs (Prevalence), Including Nonmedical Users of Prescription Psychotherapeutic Drugs:
Annual Averages Based on 2002-2004 SAMHSA

Past Year Initiates (Incidence) of Illicit Drug Use, by Drug: Annual Averages
Based on 2002-2004 (12 or older, 2002-2004) SAMHSA

Annual number of new non-medical users of Oxycontin
0
100
200
300
400
500
600
700
800
1999 2000 2001 2002 2003 2004
Oxycontin use inthousands

Drug-Related Emergency Department Visits With
Nonmedical Use of Opioid Analgesics (DAWN)
Adapted from the Drug Abuse Warning Network. DHHS Publication No. 07-4256, 2007.
Total = 598,542 Narcotic analgesics alone = 160,363
MethadoneFentanyl
Hydrocodone
Morphine
51,225 (32%)
42,810 (26.7%)
15,183 (9.5%)
41,216 (25.7%)
9,160 (5.7%)
Oxycodone
• 1 out of 3 visits were from nonmedical use of opioid analgesics in 2005.• Of these, oxycodone and hydrocodone account for about 60%.

DAWN Comparison2004 V. 2005
020000400006000080000
100000120000140000160000180000
Num
ber
vis
its
20042005
Adapted from the Drug Abuse Warning Network. DHHS Publication No. 07-4256, 2007.

Role of Physicians in Prescription Drug Abuse
The 5 D’s Dated: doctors who have not kept up with standards of practice
Duped: doctors easily manipulated by addicts, perhaps of difficulty in confronting patients, pride
Disabled: doctors who are impaired by illness or chemical dependency
Dishonest: doctors who willfully prescribe and use their licenses to deal drugs
Denial: doctors who refuse to admit that they are wrong, “I know what I am doing”
Principles of Addiction Medicine, 3rd Ed, 2005

CASA (The National Center on Addiction and Substance Abuse at
Columbia University) 20050f 979 physicians
Lack of Awareness <20% received any medical school training in
identifying prescription drug diversion <40% received any training in medical school in
identifying prescription drug abuse and addiction Inadequate Risk Management 43% do not ask about prescription drug abuse as part of
patient history 33% do not request records from previous health care
providers for new patients Inadequate Treatment of Patients 74% have not prescribed a controlled substance due to
concern about patient abuse in the past year

OPIOID THERAPY FOR
CHRONIC PAIN ?

Guidelines and Prescribing Principles for
Opioid Therapy

PAIN MANAGEMENT ≠
OPIOID DISPENSING

Universal Precautions in Pain Medicine
1. Diagnosis with appropriate differential2. Psychological assessment including risk of
addictive disorders3. Informed consent (verbal v. written/signed)4. Treatment agreement
(verballv.written/signed)5. Pre/Post Intervention Assessment of Pain
Level and Function
Heit, Gourlay, Pain Medicine; 6,2005. Universal Precautions in Pain Medicine:A Rational Approach to the Treatment of Chronic Pain

Universal Precautions in Pain Medicine (cont’d)
6. Appropriate trial of opioid therapy +/- adjunctive medication
7. Reassessment of pain score and level of function
8. Regularly assess the “Four A’s” of pain medicine : Analgesia, Activity, Adverse reactions, Aberrant behavior
9. Periodically review pain diagnosis and co-morbid conditions, including addictive disorders
10. Documentation

Assessment Benefit-Risk: New Paradigms in Chronic Pain
Treatment
GOODPRACTICE
• Goal of therapyis pain relief and improved function
•Predictable pharmacokinetics• Evaluate interaction with alcohol
• Long vs short acting• Level of difficulty to alter delivery system• Street value
Efficacy
Abuse PotentialSafety

Establish Treatment Goals
Set realistic patient expectations for analgesia and functionality Smart goals
Realistic pain control Improved functionality and productivity Improved quality of life
Concomitant physical therapy to improve treatment outcomes Commit the patient to routine evaluation of treatment outcomes
Pain relief Physical and psychosocial function
Commit the patient to monitoring and routine follow-up
Adapted from Trescot AM et al. Pain Physician. 2006;9:1-40.
X“High” (Euphoria) Pain Control

Return Periodically and Review Outcomes
Adapted from Trescot AM et al. Pain Physician. 2006;9:1-40.
Stable doses• Analgesia: decreased pain level (pain score) and increased level of function in postintervention reassessment • No evidence or suspicion of abuse• No unmanageable side effects• Improved activity and quality of life
Success—continue therapy
Despite dose escalation or switching to other opioids• Inadequate analgesia• Inadequate improvement in function• Intolerable side effects• Abuse• Noncompliance
Failure—discontinue therapy
Review comorbidities and pain diagnosis periodically

PAIN MANAGEMENT =
RATIONAL POLYPHARMACY
Ongoing PT, Psych, interventional mgt.

Buprenorphine and Methadone use in pain and addiction medicine.

Substance Abuse
Nearly 1/3 of the US population hasused illicit drugs and an estimated 6-15% have a substance use disorder or some type.
Substance Abuse and Mental Health Administration, 2007

Problem• Pain and Addiction CAN coexist• SO DOES Pain and Depression (reduced hedonic tone)• Addiction in General Population (6-15%)• Varies with the drug, gender, economic status, race Addiction in Chronic Pain Population• Probably increased (at least 15%)• We use the same terms, with different meaning• Lack of precision in definitions aroundabuse/dependency/addiction
Pain and AddictionPain and Addiction

Addiction - a side effect of opiate analgesic therapy?
Published rates of abuse and/or addiction in chronic pain populations are < 10%*
Suggests that known risk factors for abuse or addiction in the general population would be good predictors for problematic prescription opioid use
History of early substance use Personal/family history of substance abuse Co-morbid psychiatric disorders
Fishbain, 1992, 1996

Correlates of analgesic abuse in chronic pain patients
with a history of addiction
Absence of family support Lack of 12-step involvement Recent history of polysubstance
abuse (not alcohol abuse alone) Previous history of chronic opioid
therapy Failure in improvement of pain
symptoms(Dunbar & Katz, 1996)

Little evidence to suggest that a patient with CNMP who is responsive to opioid therapy is at increased risk for patterns of “problematic” prescription opioid use
An individual with chronic pain AND untreated addictive disease WILL NOT get better with opioid prescription
Pain and Chemical Dependency (Addiction)
Risk of addiction?
Compton, P; ASAM 2005

The rationale for opioid therapy

Analgesic Choices for Chronic Pain: Opioids
Treat moderate to severe pain No ceiling effect No major organ dysfunction Generally manageable side effects

Incidence of Adverse Events of Opioids
No evidence of major organ dysfunction Constipation is most persistent side effect Evidence suggests development of
tolerance to sedative and cognitive effects

PHARMACOTHERAPYWEAK OPIOID ANALGESICS
codeine
hydrocodone (Vicoden)
oxycodone (Percocet)
propoxyphene (Darvocet)
tramadol (Ultram, Ultracet)

PHARMACOTHERAPYSTRONG OPIOIDS
Agonists Morphine Oxycodone Methadone Meperidine Hydromorphone Fentanyl Sufentanil
Mixed agonists -antagonists
Pentazocine Nalbuphine Butorphanol
Partial agonist Buprenorphine

Federal laws governing addiction treatment

Methadone and Pain
Methadone may be prescribed for the treatment of pain in any patient
This includes pain patients without addiction and pain patients with a history of addiction

Methadone and Pain
Methadone has been used as an effective analgesic agent for decades. New information about NMDA receptor antagonist actions, combined with its relatively low cost, has generated increasing interest for use in pain management.
The use of methadone as a treatment for addiction has complicated efforts to appropriately position the drug for analgesic therapy. For example, some physicians erroneously believe that a special license is required to prescribe methadone as an analgesic agent. This concern is particularly strong when the patient is receiving MMT and the use of methadone is being considered for pain.

Methadone for Addiction
In order to use Methadone for Opioid Addiction Therapy (OAT), one must obtain a special federal license and be affiliated with an opioid addiction treatment program (“methadone clinic”)

Opioid Therapy for the Addicted Patient – Choices
Short acting opioids (NOT!!!!) Sustained release opioids? Methadone Buprenorphine

Methadone for pain and addiction
Potent mu agonist Useful for addiction and pain Need federal license for addiction only
management Composed 50/50 racemic L and D isomer L isomer mu agonist D isomer inactive but NMDA antagonist Long T1/2, good oral bioavailability Analgesic T1/2 4-8 hours

Methadone Conversion Ratios
Patients with prior morphine experience require a greater reduction in the estimated methadone dose than relatively morphine-naive patients.
It is not known whether this variability in the estimated dose ratio between morphine and methadone is unidirectional or should also be considered when switching from methadone to morphine.
Indelicato RA, Portnoy RK (2002);

Buprenorphine and Pain

Buprenorphine: What is it?
Buprenorphine joined methadone, LAAM, and naltrexone as the fourth medication for treating opiate addiction
May be used off label for pain May be particularly effective in
patients with pain and addiction

Buprenorphine: Why is it needed?
Federal law prohibits physicians from prescribing methadone (or other DEA Schedule II medications) for maintenance therapy or opiate addiction* EXCEPT in a federally licensed opiate treatment program (OTP) (this includes methadone maintenance).
* There is a difference between detoxification and tapering a non addicted patient off opiates once pain is resolved.

Legislation: DATA 2000
Permits qualified physicians to obtain a waiver to treat opioid addiction with Schedule III, IV, and V opioid medications (or combinations of such medications) Medications must be approved by the FDA
for that indication Medications may be prescribed or dispensed

Legislation: DATA 2000
Medications Approved by FDA 10/8/02 for use in the treatment of Opioid Addiction are: Subutex® CIII 2mg, 8mg sublingual tablet
Buprenorphine Suboxone® CIII 2/.5mg, 8/2mg sublingual tablet
Buprenorphine and Naloxone (4:1 ratio)
No other opioid agonist or partial agonist medications have been approved
Methadone is Schedule II Buprenorphine is Schedule III

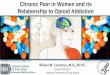
Pharmacology: Partial Opioid Agonists
Bind to and activates opiate mu receptor
Increasing dose does not produce as great an effect as does increasing the dose of a full agonist (less of a maximal effect is possible)
“Ceiling effect” on respiratory depression
Example: buprenorphine

-10 -9 -8 -7 -6 -5 -40
10
20
30
40
50
60
70
80
90
100
Intrinsic Activity
Log Dose of Opioid
Full Agonist(Morphine)
Partial Agonist(Buprenorphine)
Antagonist (Naloxone)
Intrinsic Activity: Full Agonist (Morphine), Partial Agonist
(Buprenorphine), Antagonist (Naloxone)

Onset of action: 30 – 60 minutes (after S/L administration)
Peak effects: 1 – 4 hours
Half-life ~24 to 36 hours or longer
Analgesic half life 4-8 hrs
Duration of Action

Buprenorphine/Naloxone Combination (Suboxone®)
Addition of naloxone to buprenorphine to decrease abuse potential of tablets
If taken as medically directed (dissolve under tongue), predominant buprenorphine effect
If opioid dependent person dissolves tablet and injects, predominant naloxone effect (and precipitated withdrawal)

Safety Overview Highly safe medication (acute and chronic
dosing) Primary side effects: like other mu agonist
opioids (e.g., nausea, constipation), but may be less severe
No evidence of significant disruption in cognitive or psychomotor performance with buprenorphine maintenance (or with methadone maintenance)
No evidence of organ damage with chronic dosing with buprenorphine or methadone

Safety
Low risk of clinically significant problems No reports of respiratory depression in clinical
trials comparing buprenorphine to methadone Pre-clinical studies suggest high doses of
buprenorphine should not produce respiratory depression or other significant problems
Overdose of buprenorphine combined with other drugs may cause problems (reviewed below)
Less QT prolongation than methadone

Safety
Reports of deaths when buprenorphine injected along with non-medical doses of benzodiazepines Reported from France, where
buprenorphine-only tablets available: appears patients dissolve and inject tablets
Probably possible for this to occur with other sedatives as well
Probably occurs when buprenorphine taken SL with oral benzodiazepines

Acute Pain Management for Patients on Suboxone
Ensure some form of maintenance therapy is continued (bup or methadone)
Maintenance WILL NOT treat acute pain
Try non-opioid analgesics first

Acute Pain Management
Mild – moderate pain, i.e. dental extraction:Mild – moderate pain, i.e. dental extraction: Continue buprenorphine maintenanceContinue buprenorphine maintenance Use short acting opioids (effect may be blocked)Use short acting opioids (effect may be blocked)
Moderate – Severe pain i.e. hip replacementModerate – Severe pain i.e. hip replacement Discontinue buprenorphine (may “bridge with Discontinue buprenorphine (may “bridge with
tramadol tramadol or 3 days of opiates)or 3 days of opiates)
Treat pain with opioidsTreat pain with opioids Reinduction with buprenorphineReinduction with buprenorphine

Buprenorphine and Chronic Pain
Is an effective opioid analgesic 30X Is an effective opioid analgesic 30X more potent than morphinemore potent than morphine
Ceiling effect on analgesiaCeiling effect on analgesia Analgesic t1/2 is shorter than actual Analgesic t1/2 is shorter than actual
(serum) t1/2 hence requires BID-TID (serum) t1/2 hence requires BID-TID dosingdosing
In US only parental (buprenex) is FDA In US only parental (buprenex) is FDA approved for painapproved for pain

Can One Use Suboxone ® or Subutex ® for Analgesia?
The buprenorphine products Suboxone ® and Subutex ® are the twoSchedule III narcotic medications currently approved for the treatmentof opioid dependence under the federal Drug Addiction Treatment Act of 2000 (DATA).
The off-label use of the sublingual formulations of buprenorphine (Suboxone,Subutex) for the treatment of acute or chronic pain is not prohibited under DEA requirements.
One does not need a wavier from CSAT but a valid license to prescribe schedule III controlled substances.

Thank You.