Embed Size (px)
DESCRIPTION
DR. VIPUL SHARMA, MEMBER, DELHI COUNCIL OF PHYSIOTHERAPIST. REG NO. PR 2649.
Citation preview

OSTEOARTHRITIS(OA)
It is a degenerative joint disease. The aetiology is multifactorial still not understood but commonly it
is thought to be wear and tear of joints as one ages. Two types :
PRIMARY OA: This occurs in a joint. It occurs in old age, mainly in weight bearing joints(knee and hip).
SECONDARY OA: congenital mal development of a joint, irregularity of joint surfaces, mal alignment, obesity and

excessive weight.
CLINICAL FEATURES
The disease occurs in elderly people, mostly in the major joints of the lower limb, frequently bilaterally.
Pain Swelling Crepitus Stiffness Muscle spasm Capsular contracture Incongruity of the joint surface contribute to it.
On examination ,
Tenderness on the joint line. Crepitus on moving the joint. Irregular and enlarged looking joint due to formation of peripheral
osteophytes.

Deformity – varus of the knee Effusion Terminal limitation of joint movement. Subluxation detected on ligament testing. Wasting of quadriceps femoris muscle.
INVESTIGATIONS
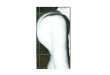
Radiological examination:
Figure: x-rays of the knee , AP and Lateral views, showing osteoarthritis of knee.
Narrowing of the joint space. Subchondral sclerosis: dense bone under the articular surface. Subchondral cysts. Osteophyte formation. Loose bodies. Deformity of the joints.

TREATMENT
METHODS OF TREATMENT
DRUGS: Analgesics are used. VISCOSUPPLEMENTATION: Sodium hylarunon has been
introduced. It is injected in the joint 3-5 times over weekly interval. It is supposed to improve cartilage function.
SUPPORTIVE THERAPY: i. Weight reduction.
ii. Avoidance of stress and strain.iii. Local heat provides relief of pain and stiffness.iv. Exercises for building up the muscles controlling the joint
help in providing stability to the joint.v. The local application of counter irritants.
SURGICAL TREATMENTi. Osteotomy.
ii. Joint replacement.iii. Joint debridement.iv. Arthroscopic procedures.

KNEE REPLACEMENTDue to rise in knee joint osteoarthritis, there is a rise in cases of knee replacement surgeries. The knee replacement is also known as knee arthroplasty. It is of two types:
Partial Knee Replacement. Total Knee Replacement(TKR).

During knee joint replacement surgery, damaged cartilage and bone are removed from the knee joint. Man-made (artificial) pieces, called prostheses, are then placed in the knee.
These pieces may be placed in up to three surfaces in the knee joint:
Lower end of the thigh bone. This bone is called the femur. The replacement part is usually made of metal.
Upper end of the shin bone--the large bone in your lower leg. This bone is called the tibia. The replacement part is usually made from metal and a strong plastic.
Back side of your kneecap. Your kneecap is called the patella. The replacement part is usually made from a strong plastic.
You will not feel any pain during the surgery because you will have one of these two types of anesthesia:
General anesthesia . This means you will be asleep and unable to feel pain.
Regional (spinal or epidural) anesthesia. Medicine is put into your back to make you numb below your waist. You will also get medicine to make you sleepy. And you may get medicine that will

make you forget about the procedure, even though you are not fully asleep.
After you receive anesthesia, your surgeon will make a cut over your knee to open it up. This cut is often 8 to 10 inches long. Then your surgeon will:
Move your kneecap (patella) out of the way, then cut the ends of your thigh bone and shin (lower leg) bone to fit the replacement part.
Cut the underside of your kneecap to prepare it for the new pieces that will be attached there.
Fasten the two parts of the prosthesis to your bones. One part will be attached to the end of your thigh bone and the other part will be attached to your shin bone.
Attach both parts to the underside of your kneecap. A special bone cement is used to attach these parts.
Repair your muscles and tendons around the new joint and close the surgical cut.
The surgery usually takes around 2 hours.
Usually, artificial knees have both metal and plastic parts. Some surgeons now use different materials, including metal on metal, ceramic on ceramic, or ceramic on plastic.



ROLE OF PHYSIOTHERAPYPhysiotherapist plays an equally important role as the surgeon performing the surgery. This is due to the fact that surgeon replaces a knee joint but the soft tissues i.e. ligaments, muscles, and myofacia requires a tissue-level engineering to gain a pain free , fully functional knee joint, which will be done by the physiotherapist after the surgery.

When to go for the knee replacement?The foremost indication to undergo a knee replacement surgery is the pain that is immense and disabling i.e. it is affecting the day to day activities. This pain along with severe arthritic changes evident on radiographs requires a planned knee replacement surgery. But before undergoing knee replacement, the following conservative treatment can be considered:
NSAIDs Physiotherapy treatment for atleast one month. Lifestyle modification and ambulatory aids, for example, cane,
leaving cross-legged sitting, use of western commode etc. Early surgical intervention- steroid injection, arthroscopic
debridement etc as per the consultant surgeon advice.
OUTCOMES: KNEE REPLACEMENTAfter an initial period of extensive physiotherapy and rehabilitation (say about 2-3 months), a person can expect a pain free knees, a normal pattern of walking that also allows the patient to ascend or descend the stairs ( although stair climbing should be restricted after total knee replacement). Along with this, the person will be able to do all activities of daily living. Cross- legged sitting is generally not advisable (some implants offer that opportunity also).

Post – operatively knee flexion range of 90 degrees should be attained for normal activities of daily living. But 105 degrees to 110 degrees of knee flexion range is required.
REHABILITATION PROCEDURE: KNEE REPLACEMENTEARLY GOALS OF PHYSIOTHERAPY
Following the knee replacement surgery, there must be rapid mobilization of the patient to avoid the complications of bed rest i.e. DVT (Deep vein thrombosis), pulmonary embolism, pressure ulcers, bed sores.
O-90 degrees of knee ROM in the first two weeks of arthroplasty ( except mention by surgeon). Along with this , complete extension should be achieved in the operation room following surgery. And rehabilitation procedures should take care to maintain that range.
Rapid return of quadriceps strength. And knee musculature strengthening.
Learning safe transfers and ambulation. Independent walking with an assisted device.
NOTE: In case of complex knee arthroplasty involving osteotomies or other procedures simultaneously, the patient may be non weight bearing for a longer duration.

PRE OPERATIVE PHYSIOTHERAPY
Pre – operative physiotherapy plays a very important role in successful outcome of TKR. 2-5 pre –operative physiotherapy sessionsn should be undertaken before going for arthroplasty. Benefits of pre- operative physiotherapy includes:
This will help patient to learn all the exercises that they needs to do following surgery. Learning of execises will be somewhat difficult after the surgery due to pin, knee stiffness.
Learn to walk with the walker, ascending and descending of stairs with stick and other transfers.
Making the patient aware of the overall procedure and initial pain after the surgery that may stay for a few weeks. In many cases, when pre- operative PT sessions have not considered.
Learn to use cold packs. Avoid placing a pillow below the knee while resting, avoid putting
excessive load on the replaced knee by trying to walk without walker, unless it is advised.
Post operative physiotherapyThis phase of post- operative PT is generally covered in hospitals and thus no elaborations are required here. Main points include:
Maintaining complete extension range. Minimizing the effects of bed boundation by early
ambulation.

Minimizing edema in lower limb especially at ankles and knees.
Minimizing inflammation at knees by use of cold packs. Gait training and stair ascending/ descending.
EARLY WEEKS(2ND TO 8TH WEEK)
This is the most challenging rehabilitation period for the PT following knee replacement surgery. This is the phase that decides the outcomes of the surgery. In this phase, physiotherapy should be continued at home under the guidance of a well qualified physiotherapist.
MAJOR GOAL INCLUDE:
Increasing the flexion range to 90 to 120 degrees depending upon the requirements, ability of the client and other post surgical factors.
Keeping the post surgical pain to the minimal level. Helping the client learn the use of western style toilet seat. Rapid increase in strength of quadriceps, hamstrings and
gluteal muscles( hip musculature) Normal scar mobility.

PHYSICAL THERAPY AND EXERCISES
Following your surgery, you will have many weeks of physical therapy (PT) to
help ease your operated knee back into activity. PT is an integral part of your
recovery and is very important in determining the outcome of your surgery.
We have a list of commonly used exercises, but your surgeon and physical
therapist will prescribe a specific set of exercises that is best for your unique case.
These exercises are important to your overall recovery – preventing blood
clots, improving circulation, improving flexibility and knee movement and
strengthening muscles. While they may feel uncomfortable at first, they will
become easier with time and help you return to normal activity.

Ankle Pumps Quad Sets Short Arc Quads (Terminal Knee Extension) Heel Slides (Hip & Knee Flexion) Long Arc Quad (Knee Extension & Flexion) Straight Leg Raises
a

b c
d
e

Dr. Vipul Sharma, Reg.No. PR 2649
B.P.T., CMT ( ORTHO AND SPORTS), MIAFT, MDCPT, BYT.
CONSULTANT PHYSIOTHERAPISTMEMBER, DELHI COUNCIL OF PHYSIOTHERAPIST, GOVERNMENT OF NCT OF DELHI.Ex- Physio , Tejasvini Multispeciality Hospital, Orthopaedics and Trauma Centre, Mangalore.Visiting Consultant Physio, Yenepoya Hospital, Mangalore.Physio, Arya Physiotherapy Centre, New Delhi.
Contact: +91 9999989492