Embed Size (px)
DESCRIPTION
Osteoarthritis - etiology and management simplified
Citation preview

Osteoarthritis
Dr. Angelo Smith M.DWHPL

Osteoarthritis (OA)• OA is the most common form
of arthritis and the most common joint disease
• Most of the people who have OA are older than age 45, and women are more commonly affected than men.
• OA most often occurs at the ends of the fingers, thumbs, neck, lower back, knees, and hips.

•The repair mechanisms of tissue absorption and synthesis get out of balance and result in osteophyte formation (bone spurs) and bone cysts

OA
OA is a disease of joints that affects all of the weight-bearing components of the joint:
•Articular cartilage•Menisci•Bone

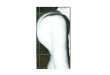
OA – Articular Cartilage
Articular cartilage is the main tissue affected OA results in:
•Increased tissue swelling•Change in color•Cartilage fibrillation•Cartilage erosion down to subchondral bone

OA – Articular Cartilage
A) Normal articular cartilage from 21-year old adult (3000X)B) Osteoarthritic cartilage (3000X)



Commonly AffectsCommonly Affects
– Hips– Knees– Feet– Spine– Hands (Interphalangeal joints)

Uncommonly Affected Joints
• Shoulder
• Wrist
• Elbow
• Metacarpophalangeal joint
• TMJ
• SI
• Ankle


OA
Nodal osteoarthritis Note bony enlargement of distal and proximal interphalangeal joints (Heberden's nodes and Bouchard's nodes, respectively).

Risk factors –Conditions that contribute to osteoarthritis

Age
• Age is the strongest risk factor for OA. Although OA can start in young
adulthood, if you are over 45 years old, you are at higher risk.
Female gender
• In general, arthritis occurs more frequently in women than in men. Before
age 45, OA occurs more frequently in men; after age 45, OA is more
common in women. OA of the hand is particularly common among women.
Joint alignment
• People with joints that move or fit together incorrectly, such as bow legs, a
dislocated hip, or double-jointedness, are more likely to develop OA in
those joints.
OA – Risk Factors

Hereditary gene defect
• A defect in one of the genes responsible for the cartilage component collagen can cause deterioration of cartilage.
Joint injury or overuse caused by physical labor or sports
• Traumatic injury (ex. Ligament or meniscal tears) to the knee or hip
increases your risk for developing OA in these joints. Joints that are
used repeatedly in certain jobs may be more likely to develop OA
because of injury or overuse.
Obesity
• Being overweight during midlife or the later years is among the
strongest risk factors for OA of the knee.

Pathogenesis of Osteoarthritis
An Interplay of Factors

• Family history of disease
• Increasing Age
• Being female
Risk factors you cannot change

• Overuse of the joint
• Major injury
• Overweight
• Muscle weakness
Risk factors you can change

Medical history
Physical exam
X-ray
Other tests
Diagnosing osteoarthritis

OA – Symptoms• OA usually occurs slowly -
It may be many years before the damage to the joint becomes noticeable
• Only a third of people whose X-rays show OA report pain or other symptoms:
– Steady or intermittent pain in a joint – Stiffness that tends to follow periods of inactivity, such as sleep
or sitting – Swelling or tenderness in one or more joints [not necessarily
occurring on both sides of the body at the same time] – Crunching feeling or sound of bone rubbing on bone (called
crepitus) when the joint is used

Two Major Types of OA
• Primary or Idiopathic
– Most common type
– Diagnosed when there is no known cause for the symptoms
• Secondary
– Diagnosed when there is an identifiable cause
• Trauma or Underlying joint disorder
• Each of these major types has subtypes


OA vs. Aging
Unlike aging, OA is progressive and a significantly more active process

Osteoarthritis with lateral osteophyte, loss of articular cartilage and some subchondral bony sclerosis- X-ray shows loss of joint space
OA – Overall Changes


Laboratory findings in OA
• THERE ARE NO DIAGNOSTIC LAB TESTS FOR OSTEOARTHRITIS
• OA is not a systemic disease, therefore:– ESR, Chem 7, CBC, and UA all WNL
• Synovial fluid• Mild leukocytosis (<2000 WBC/microliter)
• Can be used to exclude gout, CPPD, or septic arthritis if diagnosis is in doubt

Synovial fluid analysis• Severe, acute joint pain is an
uncommon manifestation of OA
• Clear fluidWBC <2000/mm3
• Normal viscosity

Differential Diagnosis
• Rheumatoid Arthritis
• Gout
• CPPD (Calcium pyrophosphate crystal deposition disease)
• Septic Joint
• Polymyalgia Rheumatica

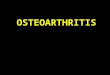
Asymmetrical joint space narrowing from loss of articular cartilage
The medial (inside) part of the knee is most commonly affected by osteoarthritis.
OA – Radiographic Diagnosis

OA – Radiographic Diagnosis•Asymmetrical joint space narrowing
•Periarticular sclerosis
•Osteophytes
•Sub-chrondral bone cysts


OA – Arthroscopic Diagnosis
Normal Articular Cartilage
Ostearthritic degenerated cartilage with exposed subchondral bone
Arthroscopy allows earlier diagnosis by demonstrating the more subtle cartilage changes that are not visible on x-ray

•OA is a condition which progresses slowly over a period of many years and cannot be cured•Treatment is directed at decreasing the symptoms of the condition, and slowing the progress of the condition
•Functional treatment goals:•Limit pain•Increase range of motion•Increase muscle strength
OA – Disease Management

Management/Treatment of OA
• Goals– Educate patient about disease and management– Improve function– Control pain– Alter disease process and its consequences

Management/Treatment of OA
• No known cure for OA
• HOWEVER– Impaired muscle function– Reduced fitness
• Affect pain and dysfunction
• Are amenable to therapeutic exercise

Management/Treatment of OA
• Pharmacologic– Acetaminophen
– NSAIDS• Cox-2 specific
inhibitors
• With PPI or misoprostol
– Nonacetylated salicylate
– Tramadol
– Opioids
• Topical– Capsaicin
– Methylsalicylate
– NSAIDS
• Intra-articular– Corticosteroids
– Hyaluronic acid

Treatment/Management of OA
• Pharmacologic– Herbal therapy
• Avocado soybean unsaponifiables (ASU’s) with promising results in 2 studies on:
– Functional index, pain, NSAID use, and global evaluation
• Reumalex (willow bark preparation) inconclusive
• Tipi tea inconclusive

Management/Treatment of OA
• Possible structure/disease modifying stuff– Glucosamine– Diacerein– Cytokine inhibitors– Cartilage repair– Bisphosphonates– Degradative enzyme inhibitors
• Tetracyclines, metalloproteinase inhibitors

Treatment/Management of OA
• Pharmacologic– Glucosamine 20 studies with >2500 patients
• If only high quality studies evaluated:– No benefit over placebo on pain
• If all studies included:– Pain may improve by as much as 13 points
• 2 RCT’s using Rotta preparation:– Demonstrated slowing of radiological progression of OA
over a 3 year period

Treatment/Management of OA
• Pharmacologic– Diacerein
• Pain improved 5 points compared to placebo
• Over 3 years,– Slowed progress of OA in the hip compared to placebo
– Did not slow progress of OA in the knee
• Diarrhea is most common side effect– 42 out of 100 had diarrhea in the first 2 weeks
– 18 discontinued because of side effects (13 in placebo)

• I recommend in ALL patients with knee and hip OA– GS 1500 mg/ CS 800 mg
• 3 month trial, evaluate efficacy; continue if helping
• Consider indefinite use even if no pain relief for joint space preservation
Glucosamine/Chondroitin--My Take

Management/Treatment of OA
• Non-pharmacologic– Patient education
– Self-management programs
– Weight loss
– PT/OT
– ROM exercises
– Muscle strengthening
• Non-pharmacologic– Assistive devices
– Patellar taping
– Appropriate footwear
– Lateral-wedged insoles
– Bracing
– Joint protection and energy conservation

Summary• Non-pharmacologic therapy is important in the
prevention and treatment of OA
• The best studied and most effective non-pharmacologic therapy is EXERCISE
• Exercise helps control weight, increase strength, improve and maintain function and decrease pain
• Traditional belief - patients concerned that joint use will “wear out” a damaged joint that is already “worn out” - NOT true for moderate intensity exercises

OA – Arthroscopic Treatment•In addition to being the most accurate way of determining how advanced the osteoarthritis is:•Arthroscopy also allows the surgeon to debride the knee joint
•Debridement essentially consists of cleaning out the joint of all debris and loose fragments. During the debridment any loose fragments of cartilage are removed and the knee is washed with a saline solution. •The areas of the knee joint which are badly worn may be roughened with a burr to promote the growth of new cartilage - a fibrocartilage material that is similar scar tissue. •Debridement of the knee using the arthroscope is not 100% successful. If successful, it usually affords temporary relief of symptoms for somewhere between 6 months - 2 years.
•Arthroscopy also allows access for surgical treatment of articular cartilage: graft-transplantation, micro-fracture techniques, sub-chondral drilling

OA – Non-operative Treatments
•Pain medications•Physical therapy•Walking aids•Shock absorption•Re-alignment through orthotics•Limit strain to affected areas

•Osteoarthritis usually affects the inside half (medial compartment) of the knee more often than the outside (lateral compartment).
•This can lead to the lower extremity becoming slightly bowlegged, or in medical terms, a genu varum deformity
Proximal Tibial Osteotomy

Proximal Tibial Osteotomy
•The result is that the weight bearing line of the lower extremity moves more medially (towards the medial compartment of the knee).
•The end result is that there is more pressure on the medial joint surfaces, which leads to more pain and faster degeneration.
•In some cases, re-aligning the angles in the lower extremity can result in shifting the weight-bearing line to the lateral compartment of the knee. This, presumably, places the majority of the weight-bearing force into a healthier compartment. The result is to reduce the pain and delay the progression of the degeneration of the medial compartment.

Proximal Tibial Osteotomy•In the procedure to realign the angles, a wedge of bone is removed from the lateral side of the upper tibia.
•A staple or plate and screws are used to hold the bone in place until it heals.
•This converts the extremity from being bow-legged to knock-kneed.
•The Proximal Tibial Osteotomy buys some time before ultimately needing to perform a total knee replacement. The operation probably lasts for 5-7 years if successful.

The ultimate solution for osteoarthritis of the knee is to replace the joint surfaces with an artificial knee joint:•Usually only considered in people over the age of 60•Artificial knee joints last about 12 years in an elderly population
•Not recommended in younger patients because:•The younger the patient, the more likely the artificial joint will fail•Replacing the knee the second and third time is much harder and much less likely to succeed.•Younger patients are more active and place more stress on the artificial joint, that can lead to loosening and failure earlier•Younger patients are also more likely to outlive their artificial joint, and will almost surely require a revision at some point down the road.
•Younger patients sometimes require the surgery (simply because no other acceptable solution is available to treat their condition)
Total Knee Replacement

•The ends of the femur, tibia, and patella are shaped to accept the artificial surfaces. •The end result is that all moving surfaces of the knee are metal against plastic
Total Knee Replacement