Embed Size (px)
DESCRIPTION
Most deep fungal infections have their primary foci in the lungs, therefore those presenting with distant organs or skin involvement should be managed aggressively as untreated or severe disease can lead to severe scarring, disfigurement and even death.
Citation preview

GOOD AFTERNOO
N

Presented by: Dr.Prashant Munde
( MDS- I )Guided by :
Dr. Mrs. SHUBHANGI KHANDEKAR ( PROFESSOR & GUIDE )
Dr. Mrs. ALKA DIVE( PROFESSOR & H.O.D)
MYCOTIC INFECTIONS OF THE ORAL CAVITY
SEMINAR

INTRODUCTION• Mycotic infections are fungal infection of
animals, including humans.
• Mycotic infections are common and a variety of environmental and physiological conditions can contribute to the development of fungal diseases.
• Inhalation of fungal spores or localized colonization of the skin may initiate persistent infections; therefore, Mycotic infections often start in the lungs or on the skin.

The fungi that cause subcutaneous Mycotic infections normally reside in soil or on vegetation.
They enter the skin or subcutaneous tissue by traumatic inoculation with contaminated material.
In general, the lesions become granulomatous and expand slowly from the area of implantation to local lymph nodes.

Extension via the lymphatics draining the lesion is slow except in sporotrichosis.
Mycotic infections are usually confined to the subcutaneous tissues, but in rare cases they become systemic and produce life-threatening disease.

CAUSES
• People are at risk of fungal infections when they are taking strong antibiotics for a long period of time because antibiotics kill not only damaging bacteria, but healthy bacteria as well.
• This alters the balance of microorganisms in the mouth, vagina, intestines and other places in the body, and results in an overgrowth of fungus.

Individuals with weakened immune systems
• with HIV/AIDS, • under steroid treatments, and taking
chemotherapy.• with diabetes also tend to develop fungal
infections.
• Very young and very old people, also, are groups at risk.

PATHOGENESIS • The response to infection with many fungi
is the formation of granulomas.
• Granulomas are produced in the major systemic fungal diseases, e.g., coccidioidomycosis, histoplasmosis, and blastomycosis, as well as several others.
• The cell-mediated immune response is involved in granuloma formation.

• Activation of the cell-mediated immune system results in a delayed hypersensitivity skin test response to certain fungal antigens injected intradermally.
• Acute suppuration( pyogenic response ), characterized by the presence of neutrophils in the exudate, also occurs in certain fungal diseases such as aspergillosis and sporotrichosis.

• Intact skin is an effective host defense against certain fungi (e.g., Candida, dermatophytes), but if the skin is damaged, organisms can become established.
• The normal flora of the skin and mucous membranes suppress fungi.
• When the normal flora is inhibited, e.g., by antibiotics, overgrowth of fungi such as C. albicans can occur.

CANDIDIASIS(Candidosis,moniliasis,t
hrush)

CANDIDIASIS(Candidosis,moniliasis,thrush)
• The fungal infections of the oral mucosa most frequently occurred due to species of Candida, Candida albicans.
• Infections can be short-lived, superficial skin irritations to exaggerated , fatal systemic diseases.
• Candida is present as a commensal organism in the mouth of up to 40% of subjects with clinically normal mouths.

• The number of organisms in the saliva of the carrier increased with pregnancy, tobacco smoking and with wearing of dentures.
• Account for 80% of nosocomial fungal infections
• Candida is also present as a commensal organism in throat ,lung, bowel and vagina.
• The primary oral reservoir for the organism in carriers in the dorsum of the tongue .

• Isolation of the Candida from the mouth of an adult is not confirmatory evidence of infection and must be considered together with the clinical findings .
• The histological sections must show the hyphae but not spores alone to confirm the diagnosis.
• Budding cells of varying size that may form both elongate pseudohyphae and true hyphae.
• Forms off-white, pasty colony with a yeasty odor.

• Both general and local predisposing factors are important in the pathogenesis of oral Candida infections for example; debilitated patients , such as those receiving antibiotic, steroid or cytotoxic therapy are particularly susceptible to Candida infections, with local factors such as tobacco smoking ,trauma and xerostomia.

Factors predisposing to oral candidal infection.
*Local factors: • Mucosal traumas• Denture wearing• Tobacco smoking
*Age:• Extremes of age ;• neonates ,infants, old age
*Drugs:• Broad –spectrum antibiotics • Steroids, Local\ systemic.• Immunosuppressant

*Xerostomia
• Drugs, radiotherapy• Sjogren syndrome
*Systemic disease
• Iron deficiency• Megablastic anemia• Acute leukemia• Diabetes mellitus• H.I.V infection.• Immunodeficiency status

CLASSIFICATION OF ORAL CANDIDIOSIS
B- CHRONIC
*CHRONIC ATROPHIC CANDIDIOSIS (denture stomatitis)
*CHRONIC MUCOUTANOUS CANDIDIOSIS CHRONIC FAMILIAL CHRONIC LOCALISED CHRONIC DIFFUSED
*CHRONIC HYPERPLASTIC CANDDOSIS
(CANDIDAL LEUKOPLAKIA)
A-ACUTE
*ACUTE PSEDOMEMBRANEOUS ORAL CANDIDIOSIS (THRUSH)
*ACUTE ATROPHIC ORAL CANDIDIOSIS

ACUTE PSEDOMEMBRANEOUS
CANDIDOSIS(THRUSH)

ACUTE PSEDOMEMBRANEOUS CANDIDOSIS(THRUSH)
• Most common form of the candidosis
• Generally associated with local disturbance or systemic illness
• Thrush occurs in up to 5% of new born infants, which is probably associated with immature antimicrobial defences, also its seen in about 10% of elderly debilitated patient .

Acute Pseudomembranous Candidosis (Thrush)
• Pain or burning• Altered taste• Predisposing:
– Xerostomia,– Antibiotics – Decreased host
resistance

Acute Pseudomembranous Candidosis (Thrush)
presents clinically as a soft, thick white coating slightly elevated plaques.
The white plaques on the affected mucosa, which can be wiped awayto leave a red, or normal appearing mucosa .

The white plaques grossly resembling milk curds, consists of tangled mass of fungal hyphae with intermingled desquamatated epithelium,keratin fibrin, necrotic debris, leukocytes, and bacteria.

Lesions may occurs on any mucosal surface of the mouth and vary in size from small patches to confluent lesions covering a wide area.
Most frequently present on buccal mucosa & tongue but also seen on palate ,gingiva & floor of mouth. In severe cases entire oral cavity may be involved.

ACUTE ATROPHIC CANDIDIOSIS

ACUTE ATROPHIC (ERYTHEMATOUS) CANDIDIOSIS.
• Also known as ANTIBIOTIC SORE MOUTH• Seen most commonly on the dorsum of the
tongue in patients undergoing prolonged corticosteroid or antibiotic therapy.
• present as a red rather than white and often painful area of oral mucosa which resembles thrush without the overlying psedomembrane.

• Usually occurs as a sequelae to a course of broad spectrum antibiotics.
• Generalized pain, burning, erythema
• May occur at any site• Red and consisistently
painful
Comes under category of Erythematous Candidosis IncludesCentral paipllary atrophy of the tongue cheilocandidiasis

Central papillary atrophy of the tongue Median Rhomboid Glossitis
• Asymptomatic, symmetric , erythematous lesion on dorsal aspect of post. region of tongue, Just anterior to foramen cecum.
• Red depapillated smooth or fissured, due to loss of filiform papillae
• Strong association with chronic smoking
• Etiologic debate– Developmental or chronic
candidal infection

CHRONIC ATROPHIC CANDIDOSIS
( DENTURE STOMATITIS)

CHRONIC ATROPHIC CANDIDOSIS ( DENTURE STOMATITIS)
• This is common and usually symptomless condition found in about 50% of denture wearer ,more frequently in women than in man.
• Clinically there is chronic erythema and oedema of the mucosa directly covered by the denture.
• The palate is usually affected but it is very unusual to see lesions related to lower dentures.

CHRONIC ATROPHIC CANDIDOSIS (denture stomatitis)
– May be asymptomatic
– Candida colonize the denture surface
– Minimal or no candidal
invasion of mucosa
- Secondary infection by Candida in tissues modified by continual wearing of dentures Poor denture hygiene High carbohydrate diet

Clinically ,patterns of inflammations can be identified
1- Pin - point of erythema – localized inflammation.
2- Diffuse area of erythema –generalized inflammation.
3- Erythema associated with a granular or multinodular mucosal surface, chronic inflammatory papillary hyperplasia.

ANGULAR CHEILITIS• Multifactorial disease of
infectious origin
• Fungal or bacterial or combined– Candida or Staph
aureus or Streptoccocci
• Mainly in denture wearers– 30% of patient with
denture stomatitis have anguar cheilitis

Clinically characterized by soreness, erythema ,Cracks, crusts, pain and fissuring at the corners of mouth.– Loss of vertical dimension – Deep folds of skin at angles
of mouth– Nutritional deficienciesIron ,folic acid , B12

CHRONIC HYPERPLASTIC CANDIDOSIS
(candidal leukoplakia)

CHRONIC HYPERPLASTIC CANDIDOSIS. (candidal leukoplakia)
• Commonly referred to as candidal leukoplakia, presents clinically as a persistent firm, adherent white plaques on the oral mucosa which is indistinguishable from leukoplakia.
• They cannot be removed by scraping but fragments may be detached and identification of hyphae in smears of such material assists in diagnosis.

Chronic Hyperplastic Candidosis (Candidal Leukoplakia)
• The lesions present as dense ,opaque white patches of irregular thickness with a rough or nodular surface.
• Most frequent location:
• Lips , tongue, buccal mucosa at commissures

• It is considered to be a premalignant lesion and epithelial dysplasia is seen in about 50% of cases.
• It is not been conclusively shown whether chronic hyperplastic candidosis is primarily leukoplakia with a secondary candidal infection or whether its primarily a chronic candidal infection which in time leads to epithelial hyperplasia and acanthosis.

• According to Cawson and Binnie , there is a definite relationship between chronic candidiasis and oral epidermoid carcinoma basing on this , chronic candidiosis itself is a cause of leukoplakia and thus must be regarded as having possible premalignant potential.
• Roed -peterson and his associates have reported a high incidence of candida organisms and occurance of cytological epithelial atypia in the biopsied lesions of leukoplakia.

CHRONIC MUCOCUTANOUS
CANDIDOSIS

• This is a group of disorders characterized by persistent superficial candidal infections of the skin, scalp, nails & mucous membranes
• Oral mucosa involved in most cases• similar to chronic hyperplastic candidiasis and occur in same intraoral locations.
CHRONIC MUCOCUTANOUS CANDIDOSIS

• Oral manifestations occur in numerous forms of candidiasis and these have been categorised and modified by Lehner, and includes the -
o CHRONIC LOCALISED MUCOCUTANEOUS CANDIDIASIS
o CHRONIC DIFFUSE MUCOCUTANEOUS CANDIDIASIS
o CANDIDASIS ENDOCRINOPATHY SYNDROME

FEATURES SUBGROUP Severe form occuring in early life, no genetic transmission,Widespread skin involvement and granulomatous and horny masses on scalp, nail and face.
CHRONIC LOCALISED
MUCOCUTANEOUS CANDIDIASIS
Least common form, of late onset Severe skin and oral lesions raised crusty sheets involving groin,limbs, face , scalp, shoulder, nails, and mouth.
CHRONIC DIFFUSE MUCOCUTANEOUS
CANDIDIASIS
Genetically transmitted (AR) Mild\moderate oral and skin lesions Hypoparathyrodism,Addison's disease ,D.M or ovarian insufficiency.
CANDIDASIS ENDOCRINOPATHY
SYNDROME
CHRONIC MUCOCUTANOUS CANDIDOSIS

DEEP FUNGAL INFECTIONS

ETIOLOGY AND PATHOGENESIS
Deep fungal infections are characterized by primary involvement of the lungs. Infections may disseminate from this focus to involve other organs. Oral infections typically follow implantation of infected sputum in oral mucos or may also follow hematogenous spread of fungus from another site such as the lung.

Oral manifestation of deep fungal infections
• Oral lesions are relatively uncommon presenting most frequently as non-specific ulceration or as nodular granulomatous lesion.

A. North american blastomycosis(gilchrist’s disease)
B. South american blastomycosis (paracoccidioidomycosis)
C. Histoplasmosis ( darling’s disease)
D. Coccidioidomycosis: (san joaquin valley fever)
E. Cryptococcosis
F. PhycomycosisG. Sporotrichosis

North American Blastomycosis
(Gilchrist’s disease)

North American Blastomycosis(Gilchrist’s disease)
• Blastomyces dermatitidis- causes blastomycosis
• Free-living species distributed in soil of a large section of the north U.S.
• Inhaled 10-100 conidia convert to yeasts and multiply in lungs.
• Affects mainly lungs and nearly 50% of those infected show cough and fever or no symptom.
• It may spread to other parts of the body, skin is involved in 20% to 40% of cases.

Cutaneous features
Skin lesions are common on the face, neck and the extremities as the infection spreads from the lungs to other parts of the body.
Lesions begin as papules, pustules or as subcutaneous nodule. Within weeks to months, the lesions develop into ulcers and form crusty sores.

Clinically, the chronic, non healing oral ulcers may resemble those of epidermoid carcinoms and cervicofacial actinomycosis.
Over a period of months to years, lesions grow larger and heal to form raised wart-like scars.
Lesions may cover much of the face causing severe disfigurement.

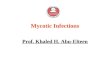
Figure 2-25 Blastomycosis showing granuloma (macrophages) with a central abscess.
The basic inflammatory response in a deep fungal infection is granulomatous.
In the presence of these microorganisms, macrophages and multinucleated giant cells dominate the histologic picture . Peculiar to blastomycosis is pseudoepitheliomatous hyperplasia, associated with superficial infections in which ulceration has not yet occurred.

Histologic freatures:- Inflammed connective tissue shows giant cells and macrophages and typical round budding organisms with doubly refractile capsule measuring between 5 to 15 microns in diameter.

TREATMENT• Those suffering from mild symptoms
require no treatment as symptoms are usually self-limiting and the infection clears spontaneously
• When other organs or skin are involved, sponteneous resolution does not occur
• Itraconazole – oral• Amphotericin B – intravenous

South American Blastomycosis
(Paracoccidioidomycosis)

South American Blastomycosis (Paracoccidioidomycosis)
• Paracoccidioides brasiliensis
• Distributed in Central and South America • Lung infection occurs through inhalation or
inoculation of spores.• Systemic lesions are similar to those of
North American Blastomycosis

• The organisms enter the body through periodontal tissues and subsequently reach the regional lymph nodes, producing lymphadenopathy,
• Papillary lesions & Widespread ulcerations of the oral cavity

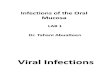
The difference between north and South American Blastomycosis is in size of micro organisms.
South American Blastomycosis 10 to 60 microns in diameter North American Blastomycosis 5 to 15 microns in diameter.
South American Blastomycosis North American Blastomycosis

Diagnosis and Treatment• Presumptive diagnosis made if budding
yeast cells and pseudohyphae are found.
• Growth on selective, differential media differentiates Candida species
• Topical antifungals for superficial infections, amphotericin B and fluconazole for systemics

HISTOPLASMOSIS ( Darling’s Disease)
Ohio Valley Fever

HISTOPLASMOSIS ( Darling’s Disease) Ohio Valley Fever
Caused by Histoplasma capsulatum , worldwide in distribution, although it is endemic in the northestern United States.
The organism multiplies in soil enriched with the droppings of birds and bats and the spores remain viable for years.
Infection is by inhalation of infected dust containing spores of fungus excreta of birds , such as pigeons, starlings and blackbirds.

HISTOPLASMOSIS- PATHOLOGY
• The parasite in its yeast phase multiplies in the monocytes and macrophages and produces areas of necrosis where parasites may abound.
• From these foci the blood stream may be invaded producing metastatic lesions in the liver, spleen and lymph nodes.
• Pulmonary histoplasmosis may produce changes similar to those of tuberculosis.

The ulcerated areas are covered by nonspecific grey membrane and are indurated.
They appear as nodular ,ulcerative , or vegetative lesions on the buccal mucosa, gingiva , tongue, palate , or lips.
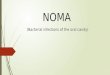
Figure 2-23 Histoplasmosis-caused chronic ulcers.

Histoplasmosis
Figure 2-24 Histoplasmosis showing macrophages with cytoplasmic microorganisms.

HISTOPLASMOSIS- MANAGEMENT
• Only symptomatic acute pulmonary histoplasmosis, chronic histoplasmosis and acute disseminated histoplasmosis require therapy.
• Itraconazole or ketoconazole are indicated for moderate disease. Severe infection is treated with intravenous amphotericin B to a total dose of 1.5 g followed by itraconazole.

Coccidioidomycosis San Joaquin
Valley Fever

Coccidioidomycosis: San Joaquin Valley Fever
• Coccidioides immitis - causes coccidioidomycosis
• Distinctive morphology – blocklike arthroconidia in the free-living stage and spherules containing endospores in the lungs.
• Lives in alkaline soils in semiarid, hot climates and is endemic to southwestern U.S.

• Arthrospores inhaled from dust, creates spherules and nodules in the lungs.
• A skin eruption resembling erythema multiforme occasionally appears concomitantly with coccidioidomycosis infection
• Amphotericin B treatment

Cryptococcosis

CRYPTOCOCCOSIS
• Cryptococcus neoformans causes cryptococcosis.
• A widespread encapsulated yeast that inhabits soil around pigeon roosts
• Common infection of AIDS, cancer or diabetes patients.

• Infection of lungs leads to cough, fever, and lung nodules
• Dissemination to meninges and brain can cause severe neurological disturbance and death.

Diagnosis and Treatment• Negative stain demonstrating
encapsulated budding yeast• Biochemical tests, serological
testing• Systemic infection requires
amphotericin B and fluconazole.

PHYCOMYCOSIS/ ZYCOMYCOSIS

• Phycomycosis, also known as mucormycosis, fungal infections caused by the genera Mucor and Rhizopus.
• Organisms in this family of fungi, which normally are found in bread mold or
decaying fruit and vegetables, are opportunistic, infecting humans when systemic health is compromised.
PHYCOMYCOSIS/ ZYCOMYCOSIS

• In the head and neck, lesions are most likely to occur in the nasal cavity, paranasal sinuses, and oropharynx. Pain and swelling precede ulceration.
• Tissue necrosis result in perforation of palate. Extension into the orbit or brain is a common complication.
• The fungus has a predilection for arterial wall invasion, which may lead to infarction.

PHYCOMYCOSIS/ ZycomycosisMicroscopically, an acute and chronic inflammatory infiltrate is seen in response to the fungus . The organism is usually readily identified in hematoxylin and eosin-stained sections in areas of tissue necrosis. Characteristic necrotic vessel walls containing thrombi and fungi may be evident.Microscopically, the fungus consists of large, pale-staining, nonseptate hyphae that tend to branch at obtuse angles.
Round or ovoid sporangia are also frequently seen in tissue sections.

SPOROTRICHOSIS

SPOROTRICHOSISCaused by Sporothrix schenckii lives as a
saprophyte on plants in many areas of the world.
In which portal of entry is not entirely understood.
Reported to occur after-
Exposure to animalsAccidental injury to thorns of plantsLab. or clinical inoculation of hospital
workers

Etiology and Pathogenesis
Subcutaneous Fungal Infections affect primarily subcutaneous tissues results from inoculation of the skin or mucosa by contaminated soil or thorny plants.
After an incubation period of several weeks, subcutaneous nodules, which frequently become ulcerated, develop.
Systemic involvement is rare but may occur in individuals with suppressed immune responses.

Clinical Manifestations Involve skin, subcutaneous tissue,oral, nasal and
pharangeal mucosa.
Skin lesions appear as red papule often described as “Sporotrichotic chancres “forms at the site of inoculation.
Oral lesions are described as nonspecific ulcerations healing by soft pliable scars.
Over the next several weeks, similar nodules form along proximal lymphatic channels.
The nodules intermittently discharge small amounts of pus and ulceration may occur.

SPOROTRICHOSIS-Diagnosis
• Culture of pus, joint fluid, sputum, or a skin biopsy specimen is preferred.
• In skin lesions, the organisms are hard to find because of small size of fungus 3-5 microns.
• It can be cultered on SDA

LABORATORY DIAGNOSIS

LABORATORY DIAGNOSIS
• There are four approaches to the laboratory diagnosis of fungal diseases:
(1)DIRECT MICROSCOPIC EXAMINATION,
(2) CULTURE OF THE ORGANISM,
(3) DNA PROBE TESTS, AND
(4) SEROLOGIC TESTS.

• Direct microscopic examination of clinical specimens such as sputum, lung biopsy material, and skin scrapings depends on finding characteristic asexual spores, hyphae, or yeasts in the light microscope.
• The specimen is either treated with 10% KOH to dissolve tissue material, leaving the alkali-resistant fungi intact, or stained with special fungal stains.
DIRECT MICROSCOPIC EXAMINATION

Some examples of diagnostically important findings made by direct examination are
(1) spherules of C. immitis and (2)wide capsule of Cryptococcus neoformans
seen in India ink preparations of spinal fluid.
Calcofluor white is a fluorescent dye that binds to fungal cell walls and is useful in the identification of fungi in tissue specimens.
Methenamine-silver stain is also useful in the microscopic diagnosis of fungi in tissue.

Smear preperation



PAS stain

PAS stain modified for fungi

• Fungi are frequently cultured on Sabouraud's agar, which facilitates the appearance of the slow-growing fungi by inhibiting the growth of bacteria in the specimen.
Inhibition of bacterial growth is due to :• low pH of the medium• chloramphenicol• cycloheximide. • The appearance of the mycelium and the
nature of the asexual spores are frequently sufficient to identify the organism.
SABOURAUD'S AGAR

DNA TECHNIQUES• Tests involving DNA probes can identify colonies
growing in culture at an earlier stage of growth than can tests based on visual detection of the colonies.
• As a result, the diagnosis can be made more rapidly.
• At present, DNA probe tests are available for1. Coccidioides, 2. Histoplasma, 3. Blastomyces, 4. Cryptococcus.

• A significant rise in the antibody titer must be observed to confirm a diagnosis.
• The complement fixation test is most frequently used in suspected cases of coccidioidomycosis, histoplasmosis, and blastomycosis.
• In cryptococcal meningitis, the presence of the polysaccharide capsular antigens of C. neoformans in the spinal fluid can be detected by the latex agglutination test.
SEROLOGY

ANTIFUNGAL THERAPY

ANTIFUNGAL THERAPY• The most effective antifungal drugs,
amphotericin B and the various azoles, exploit the presence of ergosterol in fungal cell membranes that is not found in bacterial or human cell membranes.
• Amphotericin B disrupts fungal cell membranes at the site of ergosterol and azole drugs inhibit the synthesis of ergosterol, which is an essential component of fungal membranes.
• Another antifungal drug, caspofungin (Cancidas), inhibits the synthesis of -glucan, which is found in fungal cell walls but not in bacterial cell walls. Human cells do not have a cell wall.

TREATMENT MODELATIES• Look for underlying cause and
treat it• If antibiotics or corticosteroids are
the cause, reduce the dose or change the treatment
• Intermittent or prolonged topical antifungal may be necessary when the underlying cause is unavoidable
• Denture cleansing is necessary

ANTIFUNGAL AGENTS• Amphotericin B is an effective
treatment for all forms of oral fungal infection
• Other agents that are less cytotoxic may also be effective
• Azoles are considered better but expensive
• Newer azoles may be required in invasive or resistant infections

Antifungal agents..• Flucytosine Active against
Candida and Cryptococcus species• Fluconazole has been active
against oral candidosis in HIV disease
• Nystatin is oftenly used for Candidosis

COMPLICATIONS• Drug resistance• Drug interactions and adverse
effects• Structural defects or loss of
function (eg, resulting from fungal destruction of the maxilla, orbit, and/or cranial base)

PROGNOSIS
• Most fungal infections in healthy individuals are self-limiting and have a good prognosis
• If a deep fungal oral lesion develops, the lesion likely represents a potentially serious underlying infection
• Although most deep fungal infections respond
to aggressive antifungal therapy, infections can be fatal

CONCLUSION • Most deep fungal infections have
their primary foci in the lungs, therefore those presenting with distant organs or skin involvement should be managed aggressively as untreated or severe disease can lead to severe scarring, disfigurement and even death

REFFERENCERegezi: Oral Pathology: Clinical
Pathologic Correlations, 5th ed.Shafer’s Textbook of oral
pathology, 5 th edition.Color Atlas of Clinical Oral
Pathology, 2nd Edition

THANK YOU!