Embed Size (px)
Citation preview

Online Quiz
Pathology Lab V - AtherosclerosisPATHOLOGY LAB V-ATHEROSCLEROSIS -Arben Santo
CASE OUTLINE.Case Presentation: Veronica T.DefinitionDistribution of atherosclerotic lesionsEpidemiologyRisk factors of atherosclerosisConstitutional risk factors Modifiable risk factors Additional risk factorsClassification of atherosclerotic lesionsTransendothelial passage of atherogenic proteinsAtherosclerosis-prone areasType I lesion, fatty dotType II lesion, fatty streakType III lesion, preatheromaType IV lesion, atheromaType V lesion, fibrous plaqueType VI lesion, complicated plaqueMechanisms of thrombotic response to plaque rupturePathogenesis of atherosclerosisCharacterization of atherosclerotic lesions by clinical imagingAtherosclerosis of the carotid arteriesAtherosclerosis of the vertebral-basilar systemAtherosclerosis of the arteries of the lower extremityAtherosclerosis of the renal arteriesAtherosclerosis of the mesenteric arteriesCholesterol embolism OBJECTIVES. After completing this lab the student will be able to:1. Describe epidemiology of atherosclerosis 2. List risk factors3. Explain pathogenesis of the atherosclerotic process4. Discuss AHA classification of atherosclerotic lesions 5. Describe pathology of atherosclerosis: fatty dots and fatty streaks, atheroma, fibrotic plaque and complicated plaque6. Explain characterization of atherosclerotic lesions by clinical imaging7. Describe atherosclerotic disease of various vascular beds REFERENCES.1. Robbins and Cotran Pathologic Basis of Disease, 8th edition, 2010, p 496-5062. P. Libby. The vascular biology of atherosclerosis, in Braunwald’s Heart Disease, 7th edition, 2005, p 921-9383. P.M. Ridker, P.Libby, Risk Factors for Atherothrombotic disease, in Braunwald’s Heart Disease, 7th edition, 2005, p 939-9594. E. Falk, P.K. Shah, V. Fuster, Atherothrombosis and thrombosis-prone plaques, in Hurst’s The Heart, 11 th edition, 2004, p 1123-1153

CASE PRESENTATION: VERONICA T.A 68-year-old woman with peripheral vascular disease and hypertension was referred to our institution for aortic and femoral angiography to assess the possibility of peripheral arterial revascularization. Two months earlier, a renal artery angioplasty performed via the femoral artery was complicated by cholesterol embolization to both lower extremities, resulting in
gangrene of both feet. For this reason, a brachial arterial approach was planned. On physical examination, the patient’s blood pressure was 178/82 mm Hg in both arms. Carotid bruits were heard bilaterally, although no abdominal bruits were heard. The lower extremities were warm
with dry black gangrene involving nine of the 10 toes. No pulses were palpable below the femoral artery bilaterally. No aortic calcifications were seen on chest radiographs.
Transesophageal echocardiography was done before angiography to assess the extent of atherosclerosis within the thoracic aorta, and revealed extensive protruding atherosclerotic
plaques throughout the distal ascending aorta, aortic arch, and descending thoracic aorta. On the basis of the results of the transesophageal study, we thought that the risk of stroke or major
visceral embolism would be high if the aorta were approached from either brachial artery. The patient was therefore managed conservatively with prophylactic foot care and oral pentoxifylline,
400 mg three times a day.
Discussion.Cholesterol embolization is an uncommon but well-recognized complication after angiographic
procedures involving the aorta. Atheroemboli are usually thought to originate from atherosclerotic plaques within the lower abdominal aorta. As the thoracic aorta is less commonly
involved with atherosclerosis, one would expect that passing a catheter into the descending thoracic aorta from the brachial artery would be less likely to cause cholesterol embolization than
when the aorta is approached from the femoral artery. However, in patients with peripheral vascular disease in the Coronary Artery Surgery Study (CASS), catheterization from the brachial
approach resulted in embolism and death more often than catheterization from the femoral approach did. This may be because extensive atherosclerosis involving the ascending thoracic
aorta and arch is more common than previously thought. In a study of 97 cadaveric specimens of the ascending aorta in adults with clinical coronary artery disease, the prevalence of
atherosclerotic plaques greater than 8 mm in diameter was 38%. lntraoperative studies that usedechocardiography to image the ascending thoracic aorta have shown protruding atheromatous
plaque in up to 58% of patients undergoing coronary bypass surgery.
FEATURES OF ATHEROSCLEROSIS.
Atherosclerosis is the progressive accumulation of lipid, inflammatory cells, smooth muscle cells and connective tissue within tunica intima of arteries.
Atherosclerosis is a disease of large and medium-sized elastic and muscular arteries.

Atherosclerosis manifests itself focally, by lesions called plaques. Atherosclerotic plaques, atheromas, fibrotic plaques or complicated plaques are terms denoting diverse
stages of plaque development.
A plaque is composed by a core of lipid (cholesterol and cholesterol esters) covered by a firm, white fibrous cap made of collagen fibers and smooth muscle cells.
The plaque size varies from less than 1 mm to 1.5 cm. Atherosclerotic lesions are focal and sparsely distributed along the vessels length. With
the disease progression they become numerous and larger in size. The growth of an atherosclerotic plaque is a slow dynamic process that usually occurs
over several decades.

Atherosclerotic plaques lead to serious complications:o In medium-sized arteries plaques may narrow and obstruct the lumen of the vessel,
compromise the blood flow to distal organs and cause ischemic injury.o In large arteries plaques may encroach on the subjacent media and weaken the
affected vessel wall, causing aneurysms that may rupture.
DISTRIBUTION OF ATHEROSCLEROTIC LESIONS.Which are the arteries involved in atherosclerotic process? Atherosclerotic plaques develop
primarily in: Large elastic arteries: aorta, carotid, iliac and femoral arteries
Medium-sized muscular arteries: coronary, vertebral, mesenteric, popliteal arteries, arteries of the circle of Willis.
Atherosclerosis has a predilection for some arteries but not for all the arteries. Example: pulmonary arteries and brachial arteries are not involved in atherosclerosis
PREVALNCE OF ATHEROSCLEROSIS
Atherosclerosis if the major cause of death in developed countries. The major complications of atherosclerosis including ischemic heart disease, stroke, gangrene of the extremities, account for
more than half of the annual mortality in the USA.
At the beginning of the 20th century atherosclerotic disease accounted for less than 10% of all deaths. The incidence of atherosclerosis-related diseases in the USA rose from early 20th century

to a peak in 1963 when deaths from coronary heart disease only accounted for 50% of the overall mortality.
Between 1963 and 2000 there was a 50% decrease in the death rate from coronary heart disease and 70% decrease in death rate from stroke.
Atherosclerosis is much less prevalent in Central and South America, Africa, and parts of Asia.
The mortality rate for ischemic heart disease in the United States is among the highest in the world and is approximately five times higher than that in Japan. Nevertheless, ischemic heart
disease has been increasing in Japan and is now the second leading cause of death there. Moreover, Japanese immigrants who adopt American life styles and dietary customs acquire the
same predisposition to atherosclerosis as the indigenous population.
RISK FACTORS OF ATHEROSCLEROSIS.The causes of atherosclerosis are unknown. A number of large epidemiological studies in North America and Europe have identified numerous risk factors for the development and progression of atherosclerosis. The most important epidemiological studies include the Framingham Heart
Study and Atherosclerosis Risk in Communities Study.
A risk factor is a variable associated with an increased risk of disease. Risk factor is an epidemiological term. Risk factor is a factor associated with doubling in the incidence of clinical complications of atherosclerosis such as ischemic heart disease. A risk factor is not yet a proven etiologic factor; risk factors are correlational and not necessarily causal, because correlation does not imply causation. Some risk factors are constitutional (therefore less controllable): age, male
gender, family history and genetic abnormalities. Other risk factors (such as hyperlipidemia, hypertension, cigarette smoking) are acquired or related to behaviors that are potentially
amenable to intervention.
For a risk factor to be convincingly proven that is an etiological factor, it has to fulfill Sir Austin Bradford Hill’s (1964) criteria of causality. Sir Austin Bradford Hill was a British medical
statistician (1897-1991). Some of these criteria are presented here:

Statistical validity (there has to be a valid statistical association between the risk factor and the disease);
Temporality (the risk factor must precede the disease); Plausibility (i.e. biological credibility); there should be an existing biologic mechanistic
model to explain the association; Biological gradient (i.e. dose-response); the association is more likely to be causal if its
strength increases as exposure level increases; Experimental evidence (well designed and conducted experimental studies provide
strong evidence for or against causation).Only hyperlipidemia fulfills Sir Austin Bradford Hill’s criteria of causality.
Risk factors have a multiplicative effect; two risk factors increase the risk approximately
fourfold. When three risk factors are present (e.g., hyperlipidemia, hypertension, and smoking), the rate of myocardial infarction is increased seven times.
CONSTITUTIONAL RISK FACTORS (AGE, GENDER, AND GENETICS).
1. Age. Age is a dominant influence. Although atherosclerosis is typically progressive, it usually does not become clinically manifest until middle age or later. Between ages 40 and 60, the
incidence of myocardial infarction increases fivefold. Death rates from ischemic heart disease rise with each decade even into advanced age.
2. Gender. Other factors being equal, premenopausal women are relatively protected against atherosclerosis and its consequences compared to age-matched men. Thus, myocardial infarction
and other complications of atherosclerosis are uncommon in premenopausal women in the absence of risk factors such as diabetes, hyperlipidemia, or severe hypertension. After
menopause, however, the incidence of atherosclerosis-related diseases increases and at older ages actually exceeds that of men. Although a favorable influence of estrogen has long been proposed to explain the protective effect, some clinical trials have failed to demonstrate any
utility of hormonal therapy for vascular disease prevention.3. Genetics. Family history is the most significant independent risk factor for atherosclerosis. Many Mendelian disorders associated with atherosclerosis have been characterized (such as familial hypercholesterolemia). Nevertheless, these genetic diseases account for only a small
percentage of cases. The well-established familial predisposition to atherosclerosis and ischemic heart disease is usually multifactorial, relating to inheritance of various genetic polymorphisms,
and familial clustering of other established risk factors, such as hypertension or diabetes.
MODIFIABLE RISK FACTORS.1. Hyperlipidemia. Hyperlipidemia is a major risk factor for atherosclerosis. Common
lipoprotein abnormalities that predispose to atherosclerosis include (a) increased LDL cholesterol levels, and (b) decreased HDL cholesterol levels. Epidemiologic analyses demonstrate a
significant correlation between the severity of atherosclerosis and the levels of total plasma cholesterol or LDL. The dominant lipids in atheromatous plaques are cholesterol and cholesterol esters. Genetic defects in lipoprotein uptake and metabolism that cause hyperlipoproteinemia are associated with accelerated atherosclerosis. Lowering serum cholesterol by diet or drugs slows
the rate of progression of atherosclerosis, causes regression of some plaques, and reduces the risk of cardiovascular events.

2. Hypertension. Hypertension is another major risk factor for atherosclerosis; both systolic and diastolic levels are important. On its own, hypertension increases the risk of ischemic heart
disease by approximately 60%. 3. Cigarette smoking. Cigarette smoking is a well-established risk factor in men and probably
accounts for the increasing incidence and severity of atherosclerosis in women. Prolonged smoking of one pack of cigarettes (or more) daily, doubles the death rate from ischemic heart
disease. Smoking cessation reduces the risk substantially. 4. Diabetes mellitus. Diabetes mellitus induces hypercholesterolemia and markedly increases the risk of atherosclerosis. Other factors being equal, the incidence of myocardial infarction is
twice as high in diabetics as in nondiabetics. There is also an increased risk of strokes and a 100-fold increased risk of atherosclerosis-induced gangrene of the lower extremities.
ADDITIONAL RISK FACTORS.
Approximately 20% of all cardiovascular events occur in the absence of hypertension, hyperlipidemia, smoking, or diabetes. Clearly, other factors contribute to risk; the assessment of
some of these has entered clinical practice.1. C-Reactive Protein (CRP). CRP is an acute phase reactant mainly produced by hepatocytes.
It is a marker for systemic inflammation, and has been linked to increased risk of myocardial infarction, ischemic stroke peripheral arterial disease and sudden cardiac death. This finding
suggests that systemic inflammation may contribute to atherogenesis.2. Hyperhomocysteinemia. Clinical and epidemiologic studies show a strong relationship between total serum homocysteine levels and coronary artery disease, peripheral vascular
disease, stroke, and venous thrombosis. Homocystinuria, due to rare inborn errors of metabolism, results in elevated circulating homocysteine (>100 micromol/L) and premature vascular disease. Patients with homocystinuria are characterized by extensive atheroma formation at young age.
Almost 25% of patients die as a result of thrombotic complications before the age of 30.3. Lipoprotein (a). Lipoprotein (a) is an altered form of LDL that contains the apolipoprotein B-
100 portion of LDL linked to apolipoprotein A. Lipoprotein (a) levels are associated with coronary and cerebrovascular disease risk, independent of total cholesterol or LDL levels.
4. Other factors. Factors associated with a less pronounced and/or difficult-to-quantitate risk include lack of exercise; competitive, stressful life style ("type A" personality); and obesity (which is often associated with hypertension, diabetes, hypertriglyceridemia, and decreased
HDL).
CLASSIFICATION OF ATHEROSCLEROTIC LESIONS.

The American Heart Association classification divides atherosclerotic lesions into 6 types that are stages or gradations that reflect the natural history of the disease. Note that the atherosclerotic
lesions are divided into “initial lesions” or “innocent precursors” and “advanced lesions”.The initial lesions (innocent precursors):
Type I -----Fatty dot Type II-----Fatty streak
Type III-----Intermediate lesionThe advanced lesions Type IV----Atheroma
Type V---Fibrous plaque (“The time bomb”) Type VI---Complicated plaque (“The killer”)
EARLIEST STAGES OF ATHEROSCLEROSIS.

Transendothelial passage of atherogenic plasma proteins into the subendothelial space is the first event in the birth of an atherosclerotic plaque.
The key process that initiates atherosclerosis is the transudation oxidation of low-density lipoprotein (LDL), which occurs in the subendothelial space.
Oxidized LDL (oxLDL) has properties that render it a prime candidate for initiating and sustaining the pathological processes underlying atherosclerosis.
OxLDL induces up-regulation of adhesion molecules on endothelial cells (such as ICAM, and VCAM), promotes monocyte and T lymphocyte transmigration, and is
recognized by macrophage scavenger receptors. Activated monocytes, i.e. macrophages, take up oxLDL and become foam cells.
This process is accompanied by the release of cytokines. These first steps of this pathological process constitute an immuno-inflammatory
response: macrophages and T lymphocytes continue to be present throughout plaque development.
ATHEROSCLEROSIS-PRONE AREAS.
Lesions of atherosclerosis are located preferentially in three areas which are considered atherosclerosis-prone areas of blood vessels
Origin of branch points, Outer wall of bifurcations, Inner wall of curvatures

The low shear stress hypothesis explains this distribution of lesions: the hemodynamic shear stress is the frictional force acting on the endothelial surface as a result of blood flow. In the
atherosclerosis-prone areas hemodynamic shear stress on the vessel wall is significantly lower in magnitude and exhibit directional changes and flow separation (turbulences) features absent
from regions of the vascular tree generally spared from atherosclerosis.Direct measurements of these susceptible regions have revealed shear values of the order of ± 4
dyne/cm2 compared with greater than 12 dyne/cm2 in the atherosclerosis-resistant areas.
The carotid angiogram shows narrowing at the outer walls of the common carotid artery bifurcation in both the internal carotid artery and the external carotid artery. Computational fluid modeling of the velocity map of the bifurcation shows that lower velocities are seen at the outer lateral edges. Pathological lesions are absent from the flow-dividers and inner walls where shear
stress is higher.
Endothelial cells “sense” hemodynamic forces and respond differently to different flow patterns. Shear stress controls the endothelial phenotype. Physiologic high shear stress (> 15 dynes/cm2)
determines a quiescent, atheroresistant endothelial phenotype:

Decreases the basal rate of endothelial cell proliferation Increases prostacyclin and nitric oxide (both hinder platelet activation)
Attenuates smooth muscle cell proliferation Suppresses the production of adhesion molecules and chemokines
Endothelial cells become fusiform and aligned in the direction of the flowLow shear stress (0-4 dynes/cm2) determines a proliferative, proinflammatory and atherogenic
endothelial phenotype: Increases the basal rate of endothelial cell proliferation
Enhances production of adhesion molecules and chemokines Fails to stimulate endothelial NO synthase
Foster focal platelet adhesion Endothelial cells become polygonal, cobblestone-shaped
TYPE I LESION (FATTY DOT).
The precursors of advanced atherosclerotic lesions include 3 morphological lesions: Type I, II and III.
Type I lesion is the first microscopically detectable lipid deposit in the intima.Gross:
Rarely visible to the unaided eye or Small yellow dots on the intimal surface of arteries
Histologically: Small groups of macrophages containing lipid droplets (foam cells) in the intima
There is no identifiable extracellular lipid in the intima Lipid-laded macrophages are circulating monocytes which are recruited focally into the
intima. Accumulation of T lymphocytes in the intima but they are much less numerous than
macrophagesClinically: Fatty dots do not protrude into the lumen, they are asymptomatic.
Fatty dots are common in the aorta of infants and children. They can also be found in adults, particularly in those with little atherosclerosis or in locations of arteries that are atherosclerosis
resistant.

TYPE II LESION (FATTY STREAK).
Gross: Yellow-colored streaks or patches on the intimal surface of arteries
Size 1 mm wide and 10 mm or more long They stain red with Sudan III or Sudan IV when the whole aorta is incubated in the stain
solution.
Histologically:
Macrophages containing lipid droplets (foam cells) which consist of cholesterol esters, cholesterol and phospholipids.
Stratified in several adjacent layers rather than being present as only isolated small groups of few cells
T lymphocytes present but much less numerous than foam cells There is no identifiable extracellular lipid in the intima
Clinically: Fatty streaks do not protrude into the lumen, they are asymptomaticFatty dots and fatty streaks are present in the aorta of 50% of infants and in 100% of children
from 2 to15 years old.

TYPE III LESION (PREATHEROMA).
Synonim: Intermediate lesionsType III lesion was identified around 1990. Gross and histology are very similar to fatty streaks. But, beside foam cells in several layers in intima, there are extracellular lipid droplets that lie on the intercellular matrix below the foam cell layer. A lipid core has not yet developed. The lipid
core is the characteristic component of the advanced atherosclerotic plaques (types IV, V and VI)
TYPE IV LESION (ATHEROMA).
Advanced atherosclerotic lesions include type IV, V and IV lesions. These lesions are considered advanced when accumulations of lipid, cells and matrix components are associated with
structural disorganization, repair, thickening of the intima, deformity of the arterial wall and lumen stenosis.
The lipid core is the most characteristic component of type IV lesion:

The lipid core is a massive, confluent, well-delineated accumulation of extracellular lipid Located in the deep intima Develops from two sources:
Continued insudation from plasma Following apoptotic death of macrophage foam cells
Between the lipid core and the endothelial surface the intima is still the intima of the preceding
stage of plaque development, i.e., contains ground substance but not increased amounts of collagen fibers. In the periphery there is evidence of neovascularization. Small blood vessels
proliferate and are surrounded with inflammatory cells (T lymphocytes)Gross:
Atheromas are elevated because of the thickening of intima They are pale yellow and have a smooth surface
They vary in size 0.3 to 15 mm When the cut surface of an atheroma is examined, a yellow grumous core of lipid stands
out.
TYPE V LESION (FIBROUS PLAQUE).

Synonim: Fibroatheroma Fibrous plaques are atheromas with a fibrous cap. The fibrous cap is a prominent new fibrous
collagen tissue which has formed between the lipid core and the endothelial surface. Gross:
Fibrous plaques are more elevated that atheromas They are white lesions and have a smooth surface
When the cut surface is examined, there is a yellow grumous core of lipid and a white fibrous cap of variable thickness
Histologically: Cap contains many smooth muscle cells rich in rough-surfaced endoplasmic reticulum
which manufacture collagen fibers as a reaction against the lipid core Capillaries at the margins of the lipid core are more numerous. They are present in the
fibrous cap as well. Lymphocytes and microhemorrhages are present around newly formed capillaries
The lipid core or fibrotic parts of the plaque may be calcified.

TYPE VI LESION, COMPLICATED PLAQUE.Type VI lesion is a type V lesion which has developed complications.
Complications of the atherosclerotic plaque are calcification, plaque rupture, cholesterol embolism and plaque hematoma.

Calcification occurs in areas of necrosis and elsewhere in the plaque. Calcification in the artery is thought to depend on mineral deposition and resorption, which are regulated by osteoblast-like
and osteoclast-like cells in the vessel wall.
Plaque rupture is the most fearsome complication. Plaque rupture can be superficial or deep. Rupture of the plaque surface: it is plaque erosion or a fissure that induces non-occlusive
thrombus formation. Rupture of the entire cap: it is a deep ulceration that exposes and releases lipids from the
lipid core and precipitates occlusive thrombosis. Plaque rupture often occurs at the shoulder of the plaque, suggesting that hemodynamic
shear stress weakens and tears the fibrous cap. If not repaired, endothelial loss leads to erosion of the plaque, weakening the fibrous cap and exposing the plaque to blood
constituents. Plaque rupture has been associated with (a) areas of inflammation, (b) large lipid core size, (c) thin fibrous cap (<65 micrometers).
Most plaques that rupture show less than 50% luminal stenosis.

Cholesterol embolism: the deeply ulcerated plaque discharges grumous debris into the lumen and this can result in embolization of cholesterol crystals.
Plaque hemorrhage is due to rupture of thin, newly formed capillaries of the fibrous cap or of the base of the plaque. Hemorrhage may produce a hematoma that expands the plaque and so
narrows the lumen further. Plaque hematoma can also be complicated with a subsequent rupture of the fibrous cap. The hemorrhage will be reabsorbed over time within the plaque, and leaving
telltale residual hemosiderin-laden macrophages.
MECHANISMS OF THROMBOTIC RESPONSE TO PLAQUE RUPTURE.Intact Endothelium.
When the endothelium is intact and healthy, a thrombus, of course, should not form. A number of factors keep a clot from forming under these circumstances.
Prostacyclin (prostaglandin I2) is synthesized by the intact endothelium and prevents platelet activation.
Collagen, tissue factor and VWF remain out of contact the blood due to the intact endothelium.

TFPI (tissue factor pathway inhibitor), which is released from the endothelium, binds to tissue factor and keeps it inactive.
Thrombomodulin binds thrombin and protein C, which activates protein C, which in turn inactives important clotting factors in the blood.
Heparan proteoglycan binds and activates anti-thrombin, which in turn inactivates thrombin. Platelet Plug Starts to Form.
A break in the endothelium allows platelets to contact collagen and the other factors that activate platelets.
Platelets begin adhering to one another and the subendothelial tissue via fibrinogen and Von Willebrand Factor receptors.
If the break is small, this platelet plug may be adequate to seal the break. Coagulation Reactions Begin at Surface of Platelet.
Coagulation reactions begin occurring more rapidly since tissue factor is exposed and the surface of activated platelets provides the environment for the activation of the cascade that ultimately
converts prothrombin to thrombin.The developing thrombus consists of interlaced fibrin fibrils, activated platelets and red and
white blood cells.
RESPONSE-TO-INJURY HYPOTHESISThe response-to-injury hypothesis reflects the contemporary view of atherogenesis. The
response-to-injury hypothesis views atherosclerosis as a chronic inflammatory and healing response of the arterial wall to endothelial injury. Lesion progression occurs through the
interaction of modified lipoproteins, monocyte-derived macrophages, and T lymphocytes with the normal cellular constituents of the arterial wall. According to this model, atherosclerosis is
produced by the following pathogenic events: Endothelial injury, which causes (among other things) increased vascular permeability,
leukocyte adhesion, and thrombosis Accumulation of lipoproteins (mainly LDL and its oxidized forms) in the vessel wall Monocyte adhesion to the endothelium, followed by migration into the intima and
transformation into macrophages and foam cells Platelet adhesion
Factor release from activated platelets, macrophages, and vascular wall cells, inducing smooth muscle cell recruitment, either from the media or from circulating precursors
Smooth muscle cell proliferation and ECM production Lipid accumulation both extracellularly and within cells (macrophages and smooth
muscle cells)
1. Endothelial cell injury. Endothelial cell injury is the cornerstone of the response-to-injury hypothesis. Endothelial loss
due to any kind of injury-induced experimentally by mechanical denudation, hemodynamic forces, immune complex deposition, irradiation, or chemicals-results in intimal thickening; in the
presence of high-lipid diets, typical atheromas ensue. However, early human lesions begin at sites of morphologically intact endothelium. Thus, endothelial dysfunction underlies human

atherosclerosis; in this setting, dysfunctional endothelial cells show increased endothelial permeability, enhanced leukocyte adhesion, and altered gene expression.
The specific pathways and factors contributing to endothelial cell dysfunction in early atherosclerosis are not completely understood; etiologic culprits include hypertension,
hyperlipidemia, toxins from cigarette smoke, homocysteine, and even infectious agents. Inflammatory cytokines (e.g., tumor necrosis factor) can also stimulate pro-atherogenic patterns
of endothelial cell gene expression. However, the two most important causes of endothelial dysfunction are hemodynamic disturbances and hypercholesterolemia.
2. Hemodynamic disturbances.
The importance of hemodynamic turbulence in atherogenesis is illustrated by the observation that plaques tend to occur at ostia of exiting vessels, branch points, and along the posterior wall
of the abdominal aorta, where there are disturbed flow patterns. In vitro studies further demonstrate that nonturbulent laminar flow in the normal vasculature leads to the induction of endothelial genes whose products (e.g., the antioxidant superoxide dismutase) protect against atherosclerosis. Such "athero-protective" genes could explain the nonrandom localization of
early atherosclerotic lesions.
3. Lipids.Chronic hyperlipidemia, particularly hypercholesterolemia, can directly impair endothelial cell
function by increasing local oxygen free radical production; oxygen free radicals injure vascular wall tissues and accelerate nitric oxide decay, reducing its vasodilator activity. Dysfunctional endothelial cells manifest increased permeability: lipoproteins accumulate within the intima.
These lipids are oxidized through the action of oxygen free radicals locally generated by macrophages or endothelial cells. Oxidized LDL is ingested by macrophages through a
scavenger receptor, distinct from the LDL receptor, and accumulates in phagocytes, which are then called foam cells. In addition, oxidized LDL stimulates the release of growth factors, cytokines, and chemokines by endothelial cells and macrophages that increase monocyte
recruitment into lesions. Finally, oxidized LDL is cytotoxic to endothelial cells and smooth muscle cells and can induce endothelial cell dysfunction. Oxidized LDL is the most important
molecule in atherogenesis.
4. Inflammation.Inflammatory cells and pathways contribute to the initiation, progression, and complications of
atherosclerotic lesions. Although normal vessels do not bind inflammatory cells, early in atherogenesis, dysfunctional arterial endothelial cells express adhesion molecules that encourage
leukocyte adhesion; vascular cell adhesion molecule 1 (VCAM-1), in particular, binds monocytes and T cells. After these cells adhere to the endothelium, they migrate into the intima
under the influence of locally produced chemokines. Monocytes transform into macrophages and avidly engulf lipoproteins including oxidized LDL.
Monocyte recruitment and differentiation into macrophages (and ultimately into foam cells) is
theoretically protective, because these cells remove potentially harmful lipid particles. However, the oxidized LDL augments macrophage activation and cytokine production (e.g., TNF). This
further increases leukocyte adhesion and production of chemokines (e.g., monocyte chemotactic

protein 1), creating a stimulus for recruitment of additional mononuclear inflammatory cells. Activated macrophages also produce reactive oxygen species that aggravate LDL oxidation and
elaborate growth factors that drive smooth muscle cell proliferation.
T lymphocytes recruited to the intima interact with the macrophages and can generate a chronic inflammatory state. It is not clear whether the T cells are responding to specific antigens (e.g.,
bacterial or viral antigens, heat-shock proteins, or modified arterial wall constituents and lipoproteins) or are nonspecifically activated by the local inflammatory milieu. Nevertheless, activated T cells in the growing intimal lesions elaborate inflammatory cytokines, (e.g., IFN-
gamma), which can stimulate macrophages as well as endothelial cells and smooth muscle cells.As a consequence of the chronic inflammatory state, activated leukocytes and vascular wall cells
release growth factors that promote smooth muscle cell proliferation and ECM synthesis.
5. Infection.Although there is tantalizing evidence that infections may drive the local inflammatory process that underlies atherosclerosis, this hypothesis has yet to be conclusively proven. Herpesvirus,
cytomegalovirus, and Chlamydia pneumoniae have all been detected in atherosclerotic plaques but not in normal arteries, and seroepidemiologic studies find increased antibody titers to C.
pneumoniae in patients with more severe atherosclerosis. Of course, some of these observations are confounded by the fact that C. pneumoniae bronchitis is also associated with smoking, a well-established atherosclerosis risk factor. Moreover, infections with these organisms are
exceedingly common (as is atherosclerosis), so that distinguishing coincidence from causality is difficult. Nevertheless, it is certainly possible that such organisms could infect sites of early atheroma formation; their foreign antigens could potentiate atherogenesis by driving local immune responses, or infectious agents could contribute to the local prothrombotic state.
6. Smooth muscle proliferation.
Intimal smooth muscle cell proliferation and ECM deposition convert a fatty streak, the earliest lesion, into a mature atheroma and contribute to the progressive growth of atherosclerotic
lesions. Several growth factors are implicated in smooth muscle cell proliferation and ECM synthesis, including PDGF (released by locally adherent platelets, as well as macrophages,
endothelial cells, and smooth muscle cells), FGF, and TGF-alpha. The recruited smooth muscle cells synthesize ECM (notably collagen) that stabilizes atherosclerotic plaques. However,
activated inflammatory cells in atheromas can cause intimal smooth muscle cell apoptosis, and also increase ECM catabolism resulting in unstable plaques.
1. Angiography.
Lesion types I, II and III are not detected by angiography Lesion types IV and V are detected as a stenosis with smooth borders
Lesions type VI: Plaque rupture with superimposed partially occluding thrombus are detected as a narrowing with irregular borders.
Lesions type IV: Plaque rupture with superimposed occlusive thrombus is an intraluminal defect on angiography

Severity of stenosis is estimated by expressing angiographic stenotic diameter as a percentage of the adjacent normal diameter. Percent diameter stenosis is clinically useful as a measure of
obstruction to blood flow. Coronary blood flow begins to decrease with stenosis grater than 50% and decreases rapidly when it exceeds 70%. Example: the stenotic segment is 2 mm in diameter,
the adjacent normal artery is 4 mm in diameter, and angiographer estimates a stenosis 50%The pathologist sees the cross section of the coronary artery in autopsy and estimates the
percentage of cross sectional area occupied by plaque. Same example: pathologist sees that the remaining luminal diameter is 2 mm but this would translate into a 75% cross sectional area
narrowing.

2. Intravascular ultrasound.Angiography does not show the vascular wall and therefore is insensitive for characterization of
the types of lesions presentIntravascular ultrasound is a more sensitive method for characterization of lesion composition:
It can detect the lipid core, the fibrous cap and calcificationsBut it is not feasible to examine the entire arterial tree
Only selected portions of the artery of interest can be examined
ATHEROSCLEROSIS OF THE CAROTID ARTERIES.
Atherosclerotic lesions involve the origin of internal carotid arteries Internal carotid arteries supply the majority of both cerebral hemispheres except the occipital and medial temporal lobes which are supplied by the vertebral-basilar system It is also called the “anterior circulation” of
the brain 75% of strokes occur in the anterior circulation
Embolization is considered the most common mechanism causing the ischemic strokes from atherosclerotic lesions in the internal carotid system
Clinical manifestations: Transient ischemic attacks
Cerebral infarction in the anterior circulation
ATHEROSCLEROSIS OF THE VERTEBRAL-BASILAR SYSTEM.There are three main vessels in this system: two vertebral arteries and one basilar artery. They
supply the brain stem, cerebellum and the occipital lobe. It is also called the “posterior circulation” of the brain
Atherosclerotic lesions most frequently involve the initial segment of the vertebral artery and the proximal portion of the basilar artery just after joining of the two vertebral arteries.
Approximately 25% of strokes occur in the vertebral-basilar system

Embolic phenomena are much less frequent than in the carotid system The atherosclerotic/thrombotic occlusion is the most common mechanism causing
ischemic stroke in the posterior circulationClinical manifestations:
Transient ischemic attacks (vertebral-basilar insufficiency) Brain infarctions in the posterior circulation
ATHEROSCLEROSIS OF THE ARTERIES OF THE LOWER EXTREMITY.
Atherosclerotic lesions most frequently involve the common iliac arteries, superficial iliac arteries, common femoral arteries, superficial femoral arteries, profunda femoris arteries,
popliteal arteries, and anterior or posterior tibialis arteries.Clinical manifestations:
Intermittent claudication: pain and muscle fatigue which occurs during exercise and is relieved by rest
Ulcers of the foot Gangrene of the foot or leg
Physical examination: Decreased or absent distal pulses
Bruits over narrowed artery Hair loss
Shiny skin and thickened nails
ATHEROSCLEROSIS OF THE RENAL ARTERIES.Atherosclerotic lesions involve the renal artery ostium and are associated usually with partial
occlusions which produce chronic renal ischemia: Local or global atrophy of the kidney, more pronounced in the tubular tissue.
Renal infarctionsClinical manifestations
Renovascular hypertension which is difficult to control Unexplained renal insufficiency
ATHEROSCLEROSIS OF THE MESENTERIC ARTERIES.
Atherosclerotic lesions involve the celiac artery, superior mesenteric artery and inferior mesenteric artery.
Results in decreased blood supply to the small and/or large bowel, bowel ischemia or infarctionClinical manifestations:
1) Chronic mesenteric ischemia Diffuse atherosclerosis of mesenteric arteries
Histologically no necrosis but only atrophy of the tips of intestinal villi Postprandial pain starting 20-30 minutes after the last meal that may last up to 60-90
minutes (intestinal angina) Patients develop food fear and experience subsequent weight loss and malnourishment
2) Acute mesenteric ischemia: Acute thrombosis of mesenteric arteries
Most often involves the superior mesenteric artery Hemorrhagic infarction followed by gangrene is the common pathologic result

Pain, severe and diffuse, abdominal distension, rectal bleeding, sepsis and septic shock
CHOLESTEROL EMBOLISM.Synonim: atheroembolization
Definition: Occlusion by cholesterol crystals of small arteries and arterioles. Cutaneous manifestations are the most common physical finding. Results from embolization of the lower
half of the body from severe atherosclerosis of the abdominal aortaThe most common symptoms are:
Livedo reticularis Lower extremity pain Good peripheral pulses
Other signs: Acrocyanosis (blue toe syndrome)
Gangrene confined to toes
1.
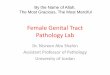
A 4 year-old girl died from complications of complications of lobar pneumonia. The gross appearance of the aorta incubated with an alcoholic solution of Sudan IV at autopsy is shown. Histologic examination of the dark red-stained spots of this aortic specimen is most likely to
show which of the following features?

A core of lipid debris covered by a fibrotic cap
Lipid-filled foam cells
A core of lipid debris filled with fresh hemorrhage.
Lipid-filled foam cells and free extracellular lipid.
Collection of foam cells, necrotic areas and calcification
2.
A 66-year-old man died from complications of liver cancer. A single atherosclerotic plaque with 65% stenosis of the lumen stenotic lesion was found in the proximal segment of the right
coronary artery. The histologic image of the right coronary artery cross section at the stenotic point is shown. Which of the following pathologic changes are evident?
Thrombosis and calcification
Atherosclerosis and thrombosis
Aneurysm and canalization
Vasculitis
Atherosclerosis and calcification
3.
A 68-year-old man, who had not seen a physician for about 25 years, presented with chest pain associated with nausea and profuse sweating. He had a 20-pack-year cigarette-smoking history. An acute inferior myocardial infarction was diagnosed by electrocardiography. The patient was
treated with reteplase (thrombolytic drug, a recombinant form of human tissue plasminogen activator) followed by a heparin infusion. At admission, his creatinine level was 2 mg/dL

(reference range 0.7-1.4). He was unaware of any prior kidney disease. The only medication he was taking was aspirin for occasional arthralgias. His kidney function deteriorated throughout her hospital stay. On hospital day 8, his creatinine level was 3.2 mg/dL when he underwent a
cardiac catheterization. A renal ultrasound showed an atrophic left kidney. All laboratory investigations for inflammatory or immune-mediated kidney diseases came back negative. A
renal biopsy was performed and its histopathological appearance is shown. What is the appropriate diagnosis?
Kawasaki disease
Giant cell arteritis
Polyarteritis nodosa
Cholesterol embolism
Buerger disease