Embed Size (px)
DESCRIPTION
A Brief presentation about Occupational Therapy management for Post polio syndrome (PPS)
Citation preview

Post Polio Syndrome
(PPS)
Phinoj K AbrahamIInd MOTh Student
All India Institute of Physical Medicine & Rehabilitation, (AIIPM&R) Mumbai

2
Outline
Acute Paralytic Polio Stages
Post Polio Syndrome (PPS) Definition Epidemiology Causes Risk factors Path physiology Clinical Features Management Prognosis

3
Virus [ Burnhilde, Lansing & Leon]
Contaminated water / food
Affinity for motor (muscle) nerves
Kills / Injures motor nerves
Results in weakness / paralysis
Acute Paralytic Polio

4
Stages
There are four recognized stages:
Acute Paralysis and/or weakness Recovery and Rehabilitation Neurological Stability Post Polio Syndrome / Sequelae

5
Post-Polio Syndrome (PPS)
A Neurological condition
New symptoms many years after acute
polio - typically 30-50 yrs.
New symptoms appear after a period of
neurological stability
Major sxs- New weakness, loss of function,
intense fatigue, pain in muscles / joints

6
Halstead and Dalakas (1985) Definition Confirmed history of polio Partial or fairly complete neurological and
functional recovery after the acute episode. Period of at least 15 years with neurological and
functional stability Two or more of the following health problems
occurring after the stable period: Extensive fatigue Muscle and or joint pain New weakness in muscles previously affected or
unaffected New muscle atrophy Functional loss Cold intolerance
No other medical explanation foundHalstead LS. 1991

7
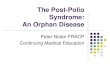
Epidemiology of PPS The frequency of PPS ranges between
15%-80%,
Natural history data from post-polio clinic in Houston, Texas. A = birth; B = onset of polio; C = maximum recovery; D = onset of new health problems; E = time of evaluation; F = death. (Halstead, L. S. and Rossi, C. D 1987)

8
Theorized Causes of PPS
The pathological changes that cause the symptoms of PPS are not well understood
There are four different theories on the cause of PPS:
Disintegration of overused motor units
Reactivation of Polio virus
Immune system dysfunction
Neural loss due to ageing

9
Causes of PPS Accelerated natural ageing Falling nerve to muscle motor unit ratio Inflammation and active immune response Co-morbidity:
Orthopaedic problems Radiculopathy and entrapment neuropathy Respiratory failure General medical problems
PPS is more likely with Increasing age; The more severe the initial weakness was The more time that elapses after the attack
of polio

10
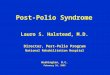
Possible Causes of Late Complications of Polio
Halstead, L. S 1988

11
Risk Factors for PPS
Higher age at onset of poliomyelitis The association with other diseases may
indicate that a chronic physical stress, particularly in already weak motor units, can contribute to the development of signs and symptoms of PPS
Poor Socio-economic conditions (Ragonese P et al)
Individuals who had polio exhibit "Type A" behavior and experience chronic stress (Richard L. Bruno et al)

12
Pathophysiology
Theories: Remaining healthy
motor neurons can no longer maintain new sprouts
Decompensation / chronic denervation and reinervation process.
Denervation exceeds reinervation
Dalakas, M. C., et al 1985

13
Theories (contd.)
Motor neuronal loss due to reactivation of a persistent latent virus.
Infection of the polio survivor’s motor neuron by a different enterovirus
Loss of strength associated with aging, in already weakened muscles
Dalakas, M. C., et al 1985

14
Main Clinical Features of PPSCommon Fatigue New Weakness Decreased
endurance Muscle & joint pain Loss of function
Gait disturbance Climbing Stairs Dressing (Activities that
require repetitive muscular contraction)
Less common Muscle atrophy Respiratory
problems Swallowing
problems Cold intolerance Sleep apnoea
Julie K Silver, Anne C Gawne 2004

15
Fatigue Post Polio Fatigue
Central (evolved from CNS)▪ Difficulty regarding cognition, concentration, memory
attention, maintaining wakefulness (because of the affectation of RAS, Basal Ganglia etc..)
Peripheral (evolving from the peripheral nerves i.e., the motor unit.)▪ Muscle weakness
According to Schanke and Stanghelle (2001), physical, peripheral fatigue was greater problem for the patients than mental, central Fatigue

16
Muscle Pain
Extremely prevalent in PPS
Deep aching pain
Myofascial pain syndrome / Fibromyalgia
Small number of patients have muscle tenderness on palpation
Julie K Silver, Anne C Gawne 2004

17
Differential Diagnosis Weakness and Functional Loss.
focal neurological disease such as a radiculopathy, focal compressive neuropathy, or spinal cord lesion and medical causes of neuropathy such as diabetes, thyroid disease, uremia, alcohol, toxins, and, uncommonly, hereditary neuromuscular disease.
Fatigue. anemia, chronic infections, collagen disorders,
thyroid disease, diabetes, cancer, depression . Pain.
osteoarthritis, bursitis, tendinitis, and myofascial pain polymyalgia rheumatica, fibromyalgia, polymyositis, and rheumatoid arthritis

18
Management
Medical management Evaluation
Confirmation of previous Paralytic Polio Exclusion of other causes of new symptoms
Medications No well-proven pharmacologic treatment for this
▪ Pyridostigmine – fatigue (effectiveness ?)▪ Amantadine (Anti viral agent) effectiveness ?▪ High dose Prednisone (no significant improvement in
M Strength, however a trend to an increse in isometric strength)
Other symptomatic management

19
Management cont..
Rehabilitative Interdisciplinary team
assessment▪ Physician, OT, PT,
SLP,P&O, SW, Respiratory Therapist
Goal setting Treat ment Planning &
intervention▪ Management of
Weakness▪ Management of Fatigue▪ Management of Pain
For the assessment of Fatigue

20
Occupational Therapy
OT interventions are tasks or activities that promote health and improve occupational performance .
Role of OT in PPS Exercise program that involves the U/E Prevention of overuse injuries Treatment of any existing arm problems Education about the principles of energy
conservation

21
Occupational therapy cont…
Interventions are Orthoses for the U/E (e.g. splints ) Assistive technology Modifications at home and work Lifestyle modification Exercise program Discharge and follow-up
MOYERS P et al .AJOT 53:251-289,1999

22
Management of Fatigue
Energy conservation techniques
Life style changes
Regular rest periods or naps during the day
Pacing (rest periods during activity)
Improvement of sleep ( e. g relaxation
techniques)
Avoidance of excessive fatigue

23
Management of pain
Most effective treatments for pain include: Heat Massage Gentle exercise Education Stretching Orthoses and Walking aids Re-education of Movement

24
Prognosis
Post-polio syndrome is not life-threatening unless there is severe pulmonary involvement or a swallowing disorder.
The symptoms are manageable and with proper measures quality of life can remain good.

25
Reference 1. Halstead LS. 1991. Assessment and differential diagnosis for
post-polio syndrome. Orthopedics. 14(11):1209.2. Halstead, L. S. and Rossi, C. D., Post-polio syndrome: clinical
experience with 132 consecutive outpatients, in Research and Clinical Aspects of the Late Effects of Poliomyelitis, Halstead, L. S. and Weichers, D. O., Eds., March of Dimes Birth Defects Foundation, 23(4), White Plains, NY, 1987, 13-26.
3. Halstead, L. S., Late complications of poliomyelitis, in Rehabilitation Medicine, Goodgold, J., Ed., CV. Mosby, Washington, D.C., 1988, 328-340.
4. Dalakas, M. C., Sever, J. L., Fletcher, M., Madden, D. L., Papadopoulos, N., Shekarchi, I., and Albrecht, P., Neuromuscular symptoms in patients with old poliomyelitis: clinical, virological and immunological studies, in Late Effects of Poliomyelitis, Halstead, L. S. and Weichers, D. O., Eds., Symposia Foundation, Miami, FL, 1985, 73-90.
5. Julie K Silver, Anne C Gawne 2004 Post Polio Syndrome p 5

26
Reference
Ragonese P, Fierro B, Salemi G, Randisi G, Buffa D, D'Amelio M, Aloisio A, Savettieri G. Prevalence and risk factors of post-polio syndrome in a cohort of polio survivors. J Neurol Sci. 2005 Sep 15;236(1-2):31-5.
Stress and "Type A" Behavior as Precipitants of Post-Polio Sequelae: The Felician/Columbia Survey Richard L. Bruno, PhD, and Nancy M. Frick, MDiv, LhD

27
THANK YOU…