Embed Size (px)
Citation preview

Overview of micronutrient
deficiency disorders and
clinical signs
By: Darayus P.Gazder

All micronutrients are important for:
1) Growth,
2) Health,
3) Development.

BACKGROUND
Vitamins are organic substances thatare essential for several enzymaticfunctions in human metabolism
A compound is called vitamin when itcannot be synthesized in sufficientquantities by an organism, and must beobtained from the diet.

Functions
Acts as hormones (vitamin D)
Acts as antioxidant (vitamin E)
Acts as mediators of cell signallingand regulators of cell and tissuegrowth and differentiation(vitaminA)
Acts as precusors for enzymecofactor biomolecules(coenzymes)that help act as catalysts andsubstrates in metabolism

VITAMINS
Vitamins are classified accordingto solubility into fat soluble & watersoluble.
13 vitamins are known, 4 fatsoluble (KEDA) & 9 water soluble(C, Folate & the B group).

VITAMINS
Water soluble-dissolve easily inwater readily excreted from the body.
Fat soluble-absorbed through theintestinal tract with the help oflipids(fats).


VITAMIN A-Vitamin A is a
generic term for many related compounds.
Retinol (alcohol), Retinal (aldehyde) are often called preformed vitamin A.
Retinal can be converted
by the body to retinoic
acid which is known to
affect gene transcription.
Body can convert b-carotene
to retinol, thus called provitamin A.

FUNCTIONS•Immunity: important for activation of T lymphocyte, maturation of WBC & integrity of physiological barrier.
•Vision: integrity of eye & formation of rodopsin necessary for dark adaptation.
•Red blood cell production
•Regulation of gene expression: vital to cell differentiation & physiologic processes
• Growth & development

Animal Foods Plant Foods
Cod liver oil Sweet potato
Liver & kidney Carrots
Egg Spinach
Butter
Milk & cheese
RICH DIETARY SOURCES

Vitamin A deficiency
•Deficiency of vitamin A leads to:
1. Ocular change- Night blindness &
xerophthalmia
2. Extra ocular changes
Growth retardation
Acquired immune deficiency
Anemia

WHO CLASSIFICATION OF
XEROPTHALMIA
PRIMARY SIGNS SECONDARY SIGNS
X1A: Conjunctival
xerosis
X1B: Bitot’s spot
X2: Corneal xerosis
X3A: Corneal ulceration
X3 B: Keratomalacia
XN: Night blindness
XF: Fundal changes
XS: Corneal scarring

Xeropthalmia
Bitots spots (X1B) are foamy white areas on the white of the eye.
Corneal Xerosis(X2) Keratomalacia (X3)


INVESTIGATIONS:
Clinical evaluation(Skin, Eyes, Growth)
Serum retinol <20 mcg/dL;
Molar ratio of retinol:RBP(Retinol
binding protein) <0.7 is also diagnostic

Treatment
• Overall mortality is reduced by 23%
• Death from measles is reduced by 50%
• Death from diarrhea is reduced by 40%

TOXICITY- Children and adults ingesting
>50,000 IU/day for several month.
•Vitamin A in excess leads to:
•Dermatitis with xanthosis cutis
•Hepatosplenomegaly
•Fatigue, malaise, anorexia, vomiting
•Bone pain & increased risk of fracture
•Pseudotumor Cerebri
•Xray-hyperostosis of the shafts of long bones

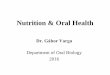
VITAMIN D
Vitamin D comprises a group of sterols; the
most important of which are cholecalciferol
(vitamin D3) & ergosterol (vitamin D2).
Humans & animal utilize only vitamin D3 &
they can produce it inside their bodies from
cholesterol.
Cholesterol is converted to 7-dehydro-
cholesterol (7DC), which is a precursor of
vitamin D3.

FUNCTIONS
•Calcium metabolism: vitamin D enhances Calcium absorption in the gut & renal tubules.
•Cell differentiation: particularly of collagen & skin epithelium
•Immunity: important for Cell Mediated Immunity & coordination of the immune response.

Sources of Vitamin D
Sunlight is the most important
source
Fish liver oil
Fish & sea food (herring & salmon)
Eggs
Plants do not contain vitamin D3
Human milk deficient in vit. D,
contains only 30-40 IU per liter mostly
from 25(OH)D3

Vitamin D deficiency
•Deficiency of vitamin D leads to:
Rickets in small children.
Osteomalacia

RICKETSLack of adequate mineralisation of growing bone
CLINICAL FEATURES

RICKETS
Sign and symptoms-
•Skeletal deformity-bowed legs(genu varum) in toddlers, knock knees (genu valgum) in older children, craniotabes (soft skull), spinal and pelvic deformities, growth disturbances, costochondral swelling(rickety rosary), harrisons groove, greenstick fractures, bone pain and tenderness, muscle weakness and dental problems.

INVESTIGATIONS
Radiologic changes-loss of normal zone of provisional calcification adjacent to metaphysis.
Widening of the growth plate.
Splaying and cupping of metaphysis.
Generalized reduction in bone density.
Low circulating levels of 25(OH)D3.
Elevated serum alkaline phosphate.
Calcium level may be normal or low
Phosphate level usually are unchanged or low.

Metaphyseal
cupping and
fraying in the
distal radius
and ulna in
rickets

TREATMENT
AAP: 400IU/day for all breastfed infants, beginning in
1st 2months of life and continue until infant is receiving
>500ml/day of vitamin of formula or vitamin D fortified
milk
Rickets: 1600-5000IU of VitD3 per day
Stross therapy:


TOXICITY•Hypervitaminosis D – infants-2,000-3,000 IU/day,
adults-10,000 IU/day for several months.
causes hypercalcemia,hyperphosphatemia,
hypertension which manifest as:
Nausea & vomiting
Excessive thirst & polyuria
Severe itching
Joint & muscle pains
Azotemia, nephrolithiasis, ectopic calcification.
Disorientation & coma.

Vitamin K
It is a cofactor of the enzyme that catalyzes one
step in the formation of prothrombin.
Needed for the generation of several clotting
factors in the liver.
Source- green leafy vegetables.
Deficiency-coagulation defect due to
hypoprothrombinemia and deficiency of factor VII
resulting in hemorrhagic disease of the newborn.
1mg IM –newborn.
In severe deficiency-2.5 to 5 mg/day parenterally.

Vitamin C - Ascorbic Acid
Humans are among the few species that cannot synthesize vitamin C and must obtain it from food
Manufacture of collagen
Helps support and protect blood vessels, bones, joints, organs and muscles
Protective barrier against infection and disease
Promotes healing of wounds, fractures and bruises
Sources
Citrus fruits, strawberries, kiwifruit, blackcurrants, papaya, and vegetables

Scurvy – Signs & Symptoms
Small blood vessels fragile
Gums reddened and bleed easily
Teeth loose
Joint pains
Scorbutic rosary: Costochondral junction is more angular
and has a sharper step-off
Dry scaly skin
Lower wound-healing, increased susceptibility to
infections, and defects in bone development in
children
Legs assume a “frog like position”(Hips and knees
are semiflexed with the feet rotated outwards)

Diagnosis
History+Clinical Features
Xray appearance of long bones:
1. Ground glass appearance of bones
2. Cortex is reduced to “Pencil Point” thinness
3. There is white line of Fraenkel (An irregular but
thickened white line at metaphysis representing
the zone of well calcified cartilage
Low levels of Vitamin C

Treatment
Prevented by a diet of Vitamin C
Daily therapeutic dose of Vitamin C is 100-200mg
or more.
Daily requirement is 45-60mg/day in children

Thiamin – Vitamin B1
What it does in the body
energy production and carbohydrate and fatty
acid metabolism
vital for normal development, growth,
reproduction, healthy skin and hair, blood
production and immune function
Deficiency due to diets of polished rice

Beri Beri- Signs & Symptoms
Develop within 12 weeks
Dry Beriberi peripheral neuropathy
Difficulty walking and paralysis of the legs
Reduced knee jerk and other tendon reflexes, foot
and wrist drop
Progressive, severe weakness and wasting of
muscles
Wet Beriberi cardiopathy
Edema of legs, trunk and face
Congestive heart failure (cause of death)

Wrist & foot drop:
Dry Beri Beri
Edema:
Wet Beri Beri

Riboflavin Deficiency
Deficiency is rare and often occurs with other
B vitamin deficiencies
Several months for symptoms to occur
Burning, itching of eyes
Angular stomatitis
Cheilosis
Swelling and shallow ulcerations of lips
Glossitis

Riboflavin deficiency
Angular stomatitis Glossitis

Niacin – Vitamin B3
Essential for healthy skin, tongue, digestive
tract tissues, and RBC formation
Processing of grains removes most of their
niacin content so flour is enriched with the
vitamin

Pellagra – Signs & Symptoms
‘Three Ds’: diarrhea, dermatitis and dementia
Reddish skin rash on the face, hands and feet which becomes rough and dark when exposed to sunlight (pellagrous dermatosis)
acute: red, swollen with itching, cracking, burning, and exudate
chronic: dry, rough, thickened and scaly with brown pigmentation
dementia, tremors, irritability, anxiety, confusion and depression

Pellagra Dermatitis

Anemia
Iron deficiency is the most common cause of anemia and
most common preventable nutritional deficiency.

Causes:Nutritional
Mother anemic
Increased Fe
demands:(Preterm,IUGR,
Cyanotic heart disease)
Prolonged breastfeeding,
cow milk
Malabsorption
Poor weaning
Blood Loss
1. Neonates:
Fetomaternal transfusions
Twin to twin transfusions
Bleeding from umblical cord
Hemorrhagic disease of
Newborn
2. Children:
Hookworm infestation
Rectal polys
IBD

Anemia- Signs & Symptoms Symptoms
Tiredness/ Fatigue/ Headache/Breathlessness
Signs
Pallor: Pale conjunctivae, palms, tongue, lips, skin,
Spoon shaped nails.
Tachycardia, Systolic murmur
If Hb<3, check for
signs of CHF

Investigations:
CBC: 1) Hemoglobin <11.0 g/dL
MVC/ MCH/ MCHC are all decreased
Reticulocyte count: Normal or minimally elevated
Peripheral blood smear:
Microcytic hypochromic anemia
Serum Fe levels: Decreased
TIBC: Increased
Serum ferritin levels: Decreased

Normal Blood Film

MICROCYTES

HYPOCHROMIA

Anemia- Treatment
Dietary counseling: Infants fortified milk formula less than 1yr
of age
Dietary diversification
Foods that are rich in iron include:
Meat/ Fortified cereals/ Spinach/Lentils and beans
Iron supplements
Mild to moderate anemia: 3-6mg/kg/day of iron (3-5 months)
Severe anemia and cardiac decompensation: Start blood
transfusions, packed RBC’s: (2-3ml/kg)

Zinc Deficiency
Zinc essential for the function of many enzymes
and metabolic processes
Zinc deficiency is common in developing countries
with high mortality
Zinc commonly the most deficient nutrient in
complementary food mixtures fed to infants during
weaning
Zinc interventions are among those proposed to
help reduce child deaths globally by 63% (Lancet,
2003)

Zinc Deficiency- Signs & Symptoms
Skin lesions
Immune impairment
Diarrhea
Poor growth
Acrodermatitis enteropathica:
AR disorder (defect of Zn absorption)
Begins within 2-4 weeks of
weaning
Perioral/ Perianal dermatitis/
Failure to thrive

Zinc Deficiency- Assessment
No simple, quantitative biochemical test of zinc status
Serum Zinc• Can fluctuate as much as 20% in 24-hour period
• Levels decreased during acute infections
• Expensive
Hair zinc analysis

Zinc Deficiency- Treatment
Regular zinc supplements can greatly reduce common
infant morbidities in developing countries • Adjunct treatment of diarrhea
-10 mg/day for infants below 6 months,
-20mg/day of zinc for 10-14 days(>6months)
Zinc deficiency commonly coexists with other
micronutrient deficiencies including iron, making
single supplements inappropriate
Emperical trial of Zinc supplementation(1ug/kg/day)
is safe and reasonable