Embed Size (px)
DESCRIPTION
Citation preview

Brain Injury & Vocational Implications
Greg Meyer, CBIS, LCSW

About Brain Injury
• Demographics
• Types and levels of brain injury (BI)
• Recovery and Common problems

Why is brain
injury called the
silent epidemic?
There are currently 5.3 million individuals—a little more than 2 percent of the U.S. population—living with a disability resulting from a traumatic brain injury.
When considering an individual’s family and circle(s) of support, brain injury touches the lives of approximately one in every 10 persons in the United States. The annual statistics of brain injury are staggering:
•1 million people are treated and released from hospital emergency departments
•230,000 people are hospitalized and survive
•80,000 Americans experience the new onset of long-term disability following hospitalization for traumatic brain injury (TBI)
•50,000 people die




Demographics• In every age group, TBI rates are higher for
males than for females. • Children aged 0 to 4 years, older adolescents
aged 15 to 19 years, and adults aged 65 years and older are most likely to sustain a TBI.
• About 75% of TBIs that occur each year are concussions or other forms of mild traumatic brain injury (MTBI).
• There was an increase in TBI-related emergency department visits (14.4%) and hospitalizations (19.5%) from 2002 to 2006.

Demographic Characteristics of the Population (NDSC study)
Average age = 39
Male (74%)
Minority population (33%)
High school education or less (64%)


Types of Brain Injury
• TBI– Open– Closed– Primary – Secondary
• Acquired

•A traumatic brain injury occurs when an outside force impacts the head hard enough to cause the brain to move within the skull or if the force causes the skull to break and directly hurts the brain.
Traumatic Brain Injury (TBI)

Closed Head Injury• Closed Head Injury: the result of a bow to the
head which causes the brain to move or shake within the skull. The sharp and hard internal surfaces of the skull can cut and bruise the brain.
• Movement or shaking can cause the brain to be damaged in many areas, not only at the point of the blow. For this reason, persons with closed head injuries can show a wide range of problems.
• Often called diffused injuries

Open Head Injury
• An open head injury is the result of a sharp object entering the brain through the skull, such as a bullet. In this type of injury, damage to the brain tissue is seen mostly in one area-the area of penetration
• These types of injuries are called focal injuries

Primary Injuries• Diffuse Axonal Injury- A Diffuse Axonal Injury can be caused by shaking or
strong rotation of the head, as with Shaken Baby Syndrome, or by rotational forces, such as with a car accident.Injury occurs because the unmoving brain lags behind the movement of the skull, causing brain structures to tear.
• Concussion-caused when the brain receives trauma from an impact or a sudden momentum or movement change. The blood vessels in the brain may stretch and cranial nerves may be damaged.
• Coup-Contrecoup Injury-This occurs when the force impacting the head is not only great enough to cause a contusion at the site of impact, but also is able to move the brain and cause it to slam into the opposite side of the skull, which causes the additional contusion
• Penetration Injury-Penetrating injury to the brain occurs from the impact of a bullet, knife or other sharp object that forces hair, skin, bone and fragments from the object into the brain.
• Contusion-A contusion is a bruise (bleeding) on the brain

Secondary Injuries• When a TBI occurs, other factors can affect the brain, called
secondary injuries. These can cause further problems in addition to the trauma
• Bleeding (hemorrhage)- when deep blood vessels in the brain are injured an bleed causing injury from loss of blood or pressure
• Blood clots (hematomas)- clots can form when there is bleeding. Clots can create pressure, which can lead to further damage
• Swelling (edema)- causes pressure which can damage the brain
• Lack of oxygen (anoxia)- because of bleeding in the brain or injury to other parts of the body, the flow of oxygen to the brain may be poor and cause damage.

An acquired brain injury is an injury to the brain, which is not hereditary, congenital, degenerative, or induced by birth trauma. An acquired brain injury is an injury to the brain that has occurred after birth.
Acquired Brain Injury

Causes of Acquired Brain Injury Airway obstruction
Near-drowning, throat swelling, choking, strangulation, crush injuries to the chest
Electrical shock or lightening strike
Trauma to the head and/or neck
Traumatic brain injury with or without skull fracture, blood loss from open wounds, artery impingement from forceful impact, shock
Vascular Disruption

Acquired BI Heart attack, stroke, arteriovenous malformation (AVM),
aneurysm, intracranial surgery
Infectious disease, intracranial tumors, metabolic disorders
Meningitis, certain venereal diseases, AIDS, insect-carried diseases, brain tumors, hypo/hyperglycemia, hepatic encephalopathy, uremic encephalopathy, seizure disorders
Toxic exposure
Illegal drug use, alcohol abuse, lead, carbon monoxide poisoning, toxic chemicals, chemotherapy (not all the time).

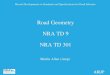
Functions of the Brain: Frontal, Temporal, Parietal, Occipital, Brain Stem
The brain is divided into main functional sections, called lobes. These sections or brain lobes are called the Frontal Lobe, Temporal Lobe, Parietal Lobe, Occipital Lobe, The Cerebellum, and the Brain Stem. Each has a specific function, as described below.


Cerebral Hemispheres
Left: verbal functions including language, thought, memory involving words
Right: Nonverbal functions such as recognizing differences in visual patters, reading maps, music, expression and understanding emotions

Levels of Brain Injury
Mild
Moderate
Severe

Mild BI
Loss of consciousness is very brief, usually a few seconds or minutes
Loss of consciousness does not have to occur—the person may be dazed or confused
Testing or scans of the brain may appear normal
A mild traumatic brain injury is diagnosed only when there is a change in the mental status at the time of injury—the person is dazed, confused, or loses consciousness. The change in mental status indicates that the person’s brain functioning has been altered, this is called a concussion

Moderate BI
A loss of consciousness lasts from a few minutes to a few hours
Confusion lasts from days to weeks
Physical, cognitive, and/or behavioral impairments last for months or are permanent.
Persons with moderate traumatic brain injury generally can make a good recovery with treatment or successfully learn to compensate for their deficits.

Severe BI• Severe brain injury occurs when a prolonged unconscious state
or coma lasts days, weeks, or months. Severe brain injury is further categorized into subgroups with separate features:
• Coma• Vegetative State -Arousal is present, but the ability to interact with the
environment is not. Eye opening can be spontaneous or in response to stimulation.General responses to pain exist, such as increased heart rate, increased respiration, posturing, or sweatingSleep-wakes cycles, respiratory functions, and digestive functions return
• Persistent Vegetative State • Minimally Responsive State-demonstrate: Primitive reflexes,Inconsistent
ability to follow simple commands, and an awareness of environmental stimulation
• Akinetic Mutism- neurobehavioral condition that results when the dopaminergic pathways in the brain are damaged.
• Locked-in Syndrome

Factors that Affect Recovery
• Age at the time of injury• Area and amount of injury• Time since the injury happened• Skills and behavior before injury• Motivation for recovery• Substance use and/or abuse• Past brain injury or concussion• Adequate supports/family involvement

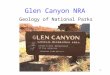
Neurorecovery Process1. Neuronal cell reactivation (24hr to 120 days)
2. Neuroplasticity (varies by area)
3. Adaptation (lifetime)
TIME
Sym
pto
m S
everit
y
Symptom Severity



Common Problems after TBI
• Cognitive
• Perceptual
• Physical
• Behavioral/emotional
• Psychiatric

Cognitive Problems
• Short term memory• Judgment• Concentration• Processing new information• Distraction• Sequencing• Sensory overload• Language abilities• Fatigue

Executive Functions
• Gain insight into strengths and limitations• Goal setting• Planning and organizing• Initiating tasks• Self-control or self-inhibiting behavior• Monitoring and evaluating performance• Problem solving• Transferring newly acquired skills to alternate
settings and situations

Executive Functions (cognitive)• Impact person’s ability to initiate, plan,
organize and complete everyday and higher level, work related tasks
• Hinder the person’s ability to follow-through with suggestions, to use compensatory strategies, and to inhibit impulses to act inappropriately

Perceptual Problems
• Vision• Hearing• Smell/taste• Touch• Time• Space orientation• Balance• Increased pain sensitivity

Physical Problems
• Impaired motor skills• Endurance/fatigue• Speech• Chronic pain/headaches• Photosensitivity• Hemiplegia (total paralyisis) or hemiparesis
(weakness) • Seizures• Impaired balance and coordination

Behavioral/Emotional Problems• Irritability • Impatience• Impulse control• Stress• Reading social cues• Initiation• Self-awareness• Mood swings • Personality changes

Psychiatric Problems
• Depression
• Anxiety
• PTSD
• Substance abuse

Employment after a BI
• 28% employed 1 yr post injury, 63% employed at injury

Injury Severity (Persons with more severe injuries are more likely to be unemployed)
Duration of Coma
Length of Hospitalization
Scores on Functional Independence Scales at Rehabilitation Admission and Discharge
Performance on Neuropsychologic Tests
History of Alcohol Abuse
Amount of Education (The more education the better the vocational outcome)
Age (Persons above age 45 are less likely to return to work following a TBI)
Predictor Factors for Returning to Work (Sander, Kreutzer, Rosenthal et al., 1996)

Assessment, Plan Development, and Strategies
• Neuropsychological testing• Community-Based situational
assessments• Recommendations for
accommodations, modifications and compensatory strategies
• Team meetings with VR, client, and treatment team

Examples of Compensatory strategies
Cognitive Challenge Possible Intervention
Orientation Keep a calendar for appointment, to-do lists, checklist, phone #’s etc.
Attention/Concentration Ask for clarification and step by step instructions when necessary. Present new information slowly
Visual Perceptual Process
Provide orientation to written documents or screens/fields on a computer screen
Organization Follow established, set process, organized checklist or schedule for completing certain tasks. Do one thing at a time.
Memory Use a tape recorder to remember information provided in presentations or meetings. Take notes. Summarize information. Organize notes.
Problem-Solving Depending on the task, use a decision table or chart to solve recurring problems
Self-monitoring Keep a schedule or checklist of work tasks necessary to
complete. Check-off completed items.

Examples of Environmental Modifications or AccommodationsCognitive Challenge Possible Intervention
Orientation Organize work materials or set up in a consistent manner. Keep a calendar with schedule and daily tasks
Attention/Concentration Minimize distractions through noise control or visual barriers
Visual Perception Process Use high contrast materials to complete certain tasks
Organization Use graphics, checklists or charts to outline essential job functions. Keep files
Memory Use a planner pad/appointment book to track meetings, goals and “to do” lists
Problem-Solving Identify staff as resource people to help solve certain problems (natural supports). Plan and structure each day.
Self-monitoring Keep a checklist of tasks that need to be completed daily

More compensatory strategies
• Fatigue: regular rest breaks with a focus on energy conservation vs reaction to fatigue; gradual increase in work hours
• Memory: have co-workers or supervisor email list of tasks vs random conversations that occur in the hallway
• Noise: earplugs or noise canceling headsets• Organization: take 10 minutes at the
beginning of each day to organize desk and to do list for the day


Elks Rehab HospitalBrain Injury Programs
Inpatient
• CARF accredited (Commission on Accreditation of Rehabilitation Facilities)
• Patients have a need and can tolerate at least 5-7 days a week, 3 hours a day of therapy which can include PT, OT, Speech, Rec.
• Program is directed by a physiatrist.
• Nursing staff, dietician, and social services part of treatment team.
• Contact: Katie Anderson LCSWBrain Injury Program Director489-4558
Outpatient
• Provided at Elks Rehab Hospital
• CARF accredited (Commission on Accreditation of Rehabilitation Facilities)
• Comprehensive neurological rehabilitation designed to meet the individual needs of children, adolescents, and adults as well as their families.
• Interdisciplinary treatment team staffs patients weekly and consists of PT, OT, Speech, Recreational, Social Worker, Neuropsychologist, and Physiatrist. All of which are nationally Certified Brain Injury Specialists (CBIS).
• Individualized treatment plans focused on reintegration of patients back to their homes, school, or work.
• Contact: Kristi Pardue M.S. CCC-SLP CBISOutpatient Neurological Program Manager489-4785

Outpatient Brain Injury Program
• Specialized interdisciplinary treatment approach for patients who have experienced a neurological injury (including brain injury, stroke, tumor resection, etc.) that affects their functioning.
• Patients and families work with a designated team of rehabilitation specialists who exclusively treat the neurological population.
• Each patient has a formal plan to either return to work, school or their home/community.

What does each team member do to help patients return to work?• Physiatrist – medical doctor specializing in rehabilitation.
Addresses medical issues including medications required in transitioning a person back to work. Guides team in a return to work plan.
• Neuropsychologist – completes comprehensive testing to assess memory, attention, problem solving, speed of processing, and the effect of fatigue on cognitive functioning. Guides team in return to work plan and how neurocognitive difficulties may impact return to work.
• Social Work – completes Track assessment, provides education, updates on progress, links to appropriate services, coordinates meetings with involved agencies, follows up with employers/employee while at work, provides supportive counseling

What does each team member do to help patients return to work?
• Speech Therapy – addresses communication and cognition skills (memory, attention, organization, problem solving, and compensatory strategies) necessary to enable the patient to successfully transition to the work environment.
• Occupational Therapy- addresses cognition, vision, gross and fine motor skills, endurance and strength for work environment as well as a work site evaluation.
• Physical Therapy- addresses the specific mobility activities limiting the patient’s ability to access and function in the work environment. Safety, movement and weight restrictions are also assessed.
• Recreational Therapy – provide opportunities for work trials and re-entry, work conditioning and stress management to encourage a successful adjustment back into work.