Embed Size (px)
DESCRIPTION
- Were you diagnosed with colon or rectal cancer before the age of 50? - Was anyone in your family diagnosed with colon cancer before the age of 50? - Was anyone in your family diagnosed with uterine (endometrial) cancer before the age of 50? - Are there cancers across several generations on one side of your family? If you answered YES to just one of these questions, it's time to talk turkey about Lynch syndrome. Lynch syndrome is an inherited genetic mutation, and having it increases your chance of getting colorectal cancer to 80%. Unfortunately, nearly every person living with Lynch syndrome is completely unaware of it. Lynch syndrome also puts you at higher risk for brain, breast, kidney, melanoma, ovarian, pancreas, small bowel, stomach, or uterine/endometrial cancers. Knowledge is power and will help your medical team act more aggressively with their screening measures. Brian Mansfield, a music critic for USA Today, didn't know he had Lynch syndrome until he was diagnosed with colorectal cancer earlier this year at the age of 48. After his diagnosis, he began talking with his family about their health history, "then the family tree lit up like a Christmas tree." Brian is chronicling his journey through a weekly USA Today online column, "My Semicolon Life." Join national patient advocacy group Fight Colorectal Cancer as we host Brian and his doctor, Dr. Bill Harb, a colorectal surgeon at Cumberland Surgical Associates, along with Associate Director of Human Genetics at Ohio State University Heather Hampel as they tell you more about Lynch syndrome and how to dig into the medical mystery that may be lurking within your family tree. With the holidays coming up, never has there been a more appropriate time to talk turkey...and Lynch syndrome. **Fight Colorectal Cancer thanks Can't Stomach Cancer, the Colon Club, Kidney Cancer Association, Myriad Genetics, and Ovarian Cancer National Alliance for their assistance with this webinar.**
Citation preview

Welcome! Talking Turkey
About Lynch SyndromePart of Fight Colorectal Cancer’s Monthly Patient Webinar Series
Our webinar will begin shortly
www.FightColorectalCancer.org877-427-2111

Fight Colorectal Cancer
1. Tonight’s speaker’s: Brian Mansfield, Dr. William Harb, and Heather Hampel
2. Archived webinars: Link.FightCRC.org/Webinars
3. Follow up survey to come via email. Get a free Blue Star of Hope pin when you tell us how we did tonight.
4. Ask a question in the panel on the right side of your screen
5. Or call the Fight Colorectal Cancer Answer Line at 877-427-2111
www.FightColorectalCancer.org877-427-2111

Fight Colorectal CancerUpcoming 2013 Webinar’s
Advancements in CRC SurgeryHighlights from GI ASCO
Highlights from ASCOManagement of Peripheral Neuropathy
Pathways and Targets: How these affect treatment optionsMolecular Testing and Tumor Tissue Testing
Register at www.FightColorectalCancer.org
1-877-427-2111

Fight Colorectal Cancer
Funding Research DirectlyLisa Dubow Fund
http://fightcolorectalcancer.org/research/lisa-fund

Fight Colorectal CancerDisclaimer
The information and services provided by Fight Colorectal Cancer are for general informational purposes only.
The information and services are not intended to be substitutes for professional medical advice, diagnosis, or treatment.
If you are ill, or suspect that you are ill, see a doctor immediately. In an emergency, call 911 or go to the nearest emergency room.
Fight Colorectal Cancer never recommends or endorses any specific physicians, products or treatments for any condition.
www.FightColorectalCancer.org877-427-2111

Fight Colorectal CancerResources
To learn more about Lynch Syndrome
http://fightcolorectalcancer.org/awareness/lynch_syndrome
5 Questions to Ask your Family at Thanksgiving
http://fightcolorectalcancer.org/images/posts/2012/10/5-Questions.pdf
Is Lynch Syndrome Lurking in your family worksheet
http://fightcolorectalcancer.org/images/posts/2012/10/Lynch-lurking.pdf

Fight Colorectal Cancer
Lynch Syndrome
Patient
PhysicianGenetics Counselor

Fight Colorectal Cancer
Brian Mansfield

Fight Colorectal CancerTo learn more about Brian’s Story:
Downloadable PDF -
http://fightcolorectalcancer.org/images/posts/2012/10/Lynch-article-FINAL.pdf
www.FightColorectalCancer.org877-427-2111

Fight Colorectal CancerDr. William Harb

Talking Turkey about Lynch Syndrome
Dr. William J. Harb, M.D., FASCRSColorectal Surgeon
Nashville, TN

48 year old male presents with a change in his bowel habits
Referred by his internist to a gastroenterologistUndergoes colonoscopyFamily history?
Maternal great-grandfather had colon cancerMaternal uncle with colon cancerQuestionable ovarian cancer in paternal
grandmother and aunt


What next?

A visit to the colorectal surgeonWhat do we talk about?
Review of colonoscopyReview of CT scanDiscussion of colon anatomyDiscussion of family history


Genetic testingWhy? Age under 50Family history
Often unreliable as in Brian’s case – many physicians would think that maternal great-grandfather and uncle not related closely enough
Ovarian cancer often neglected in family history

Brian had genetic testing prior to surgeryIt actually changed what operation he had!



He needs colonoscopy every yearNot every 5 years or 3 yearsNeed to check his stomach Family members need genetic testing
Referral to genetic counselor

SummaryLynch syndrome is not rare
But if you don’t look for it then it won’t be foundWe need the help of patients to discuss this with
their family and their doctorsWe can prevent colon cancer with genetic testing
And we can prevent people like Brian from having to go thru this ordeal
Please talk to your doctors and your family – the holidays are a great time of year to talk about medical history

Fight Colorectal CancerHeather Hampel

Talking Turkey about Lynch syndrome
Heather Hampel, MS, CGC

25
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Causes of Hereditary Susceptibility to CRC
Adapted from Burt RW et al. Prevention and Early Detection of CRC, 1996
Sporadic (65%–85%)
Familial (10%–30%)
Lynch syndrome (3%)
Familial adenomatous polyposis (FAP) (1%)
Rare CRC syndromes
(<0.1%)

26
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Lynch Syndrome
MLH1
MSH2MSH6
PMS2

27
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Sporadic Inherited
• Later age at onset (60s or 70s)• Little or no family history of cancer• Single or unilateral tumors
•Early age at onset (<50)•Multiple generations with cancer•Clustering of certain cancers (i.e. breast/ovarian)
Normal gene
Somatic mutation
Somatic mutation
Germline mutation
Somatic mutation

28
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Carrier Parent Non-carrier Parent
Aa aa
Aa Aa aa aa
Carrier Carrier Non-carrier Non-carrier
Autosomal Dominant Inheritance
1/2 1/2

29
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Clinical Features of Lynch syndrome
Early but variable age at CRC diagnosis (~45 years)
Tumor site in proximal colon predominates
Extracolonic cancers: endometrium, ovary, stomach, urinary tract, small bowel, bile ducts, sebaceous skin tumors

30
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Lynch Syndrome Cancer Risks (to 70)Cancer MLH1& MSH2 MSH6 PMS2
♂ Colon cancer 56% - 85% 22% 20%
♀ Colon cancer 48% - 85% 10% 15%
Endometrial cancer 35% - 64% 26% 15%
♂ Other LS cancers 19.3% 3% 6%
♀ Other LS cancers 5% 11% 6%

31
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Surveillance Options for Patients with Lynch syndrome
Lindor NM, et al. JAMA 2006;296(12):1507-1517.
InterventionColonoscopy
Transvaginal ultrasound
Endometrial aspirate
RecommendationBegin at age 20–25,
repeat every 1–2 years
Annually, starting at age 25–35
MalignancyColorectal cancer
Endometrial cancer

32
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Surveillance Reduces Risk of Colorectal Cancer in Lynch syndrome Families
Jarvinen HJ et al. Gastro 108:1405, 1995
Years of follow-up
% of subjects
with CRC
30
20
10
4.5%
11.9%
0 3 6 9
SurveillanceNo surveillance
0

33
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Prophylactic Surgery Options for Patients with Lynch syndrome
Options include subtotal colectomy, hysterectomy, and oophorectomy
Surgery does not eliminate cancer risk Recent data that hysterectomy with BSO
eliminates the risk of endometrial and ovarian cancer in LS patients
Schmeler KM, et al. NEJM 2006;354:261-269.

34
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
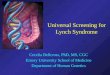
The Family History is Key to Diagnosing Lynch syndrome
CRCdx 45
OvarianCa, dx 64
CRCdx 50s
CRCdx 61
CRCdx 75
CRCdx 48
CRCdx 52
EndometrialCa, dx 59
CRCdx 42
45

35
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Amsterdam Criteria II
3 or more relatives with verified HNPCC-associated cancers* in family
One case a first-degree relative of the other two Two or more generations One CRC by age 50 FAP excluded
Vasen HFA et al. Gastroenterology 116:1453, 1999
*HNPCC associated cancers: CRC, endometrial, small bowel, ureter, renal pelvis

36
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Genetic Features of Lynch Syndrome
Genes belong to DNA mismatch repair (MMR) family
Mutations in MMR genes lead to microsatellite instability
MMR proteins are missing in the tumor tissue making immunohistochemical staining useful

37
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Microsatellite Instability (MSI)
Repetitive DNA sequences 1- 4 nucleotides (microsatellites) normally found genome Mono: TCGAGG AAAAAAAA GGAGCT Di: TCGAGG CACACACACACA GGAG
With MMR failure, variability in repeats 90% of HNPCC tumors are MSI+ 10%–15% of sporadic CRCs are MSI+

38
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
MSI testing on Genotyper

39
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Immunohistochemistry
Identify MMR proteins
Normally present If protein is absent,
gene is not being expressed (mutation or methylation)
Helps direct gene testing by predicting likely involved gene
If abnormal IHC (absent), MSI+
MSH2MLH1
MSH6PMS2

40
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
When to Suspect Hereditary Cancer Syndrome
Cancer in 2 or more close relatives (on same side of family)
Early age at diagnosisMultiple primary tumorsBilateral or multiple rare cancersConstellation of tumors consistent with specific cancer syndrome (eg, breast and ovary)Evidence of autosomal dominant transmission

41
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
When Should Genetic Testing Be Considered?
Significant family cancer history Reasonable likelihood of carrying an altered cancer susceptibility gene Ideally, test affected person first Results will influence medical management Patient wants information (empowerment)

42
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
GINA
Prevents health insurers from denying coverage, adjusting premiums, or otherwise discriminating on the basis of genetic information. Group and self-insured policies
Insurers may not request that an individual undergo a genetic test.
Employers cannot use genetic information to make hiring, firing, compensation, or promotion decisions.
Sharply limits a health insurer's or employer's right to request, require, or purchase someone's genetic information.

43
The Ohio State University Comprehensive Cancer Center –
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Resources Heather Hampel
614-293-7240 [email protected]
Family HealthLink https://familyhealthlink.osumc.edu Free, on-line tool that assesses
family history of cancer and cardiovascular disease
Find a Genetic Counselor www.nsgc.org www.cancer.gov/cancertopics/gene
tics/directory/results

Fight Colorectal Cancer
Lynch Syndrome
Patient
PhysicianGenetics Counselor

Fight Colorectal Cancer
www.FightColorectalCancer.org877-427-2111

Fight Colorectal CancerResources
To learn more about Lynch Syndrome
http://fightcolorectalcancer.org/awareness/lynch_syndrome
5 Questions to Ask your Family at Thanksgiving
http://fightcolorectalcancer.org/images/posts/2012/10/5-Questions.pdf
Is Lynch Syndrome Lurking in your family worksheet
http://fightcolorectalcancer.org/images/posts/2012/10/Lynch-lurking.pdf

Fight Colorectal CancerCONTACT US
Fight Colorectal Cancer1414 Prince Street, Suite 204
Alexandria, VA 22314(703) 548-1225
Toll-Free Answer Line: 1-877-427-2111www.FightColorectalCancer.org
Email us: [email protected]