Embed Size (px)
Citation preview

زدنى رب وقل
وقل رب زدنى اآلية علما طه (114 )سورة
Dr. Wesam MousaAssisstant Professor Anesthesia& Surgical ICU
Dammam Hospital of theUniversity04/15/23 1
Nitrous Oxide: the venerable old gentleman of the anaesthetic world

Nitrous oxide N=N=O Simple linear compound
Colorless, odorless, tasteless, and does not burn
Inert nature with minimal metabolism
Only anesthetic agent that is inorganic
04/15/23 3
Dark controversy still going on regarding N2O safety
Proponents say:
In view of the large number of patients exposed worldwide
every year for many years, good proof for its safety and
beneficial effects is accumulated.

04/15/23 4
Repellents say:
We have also, increasingly, seen wave after wave of scandals:
hypoxic events, neurological complications, foetal loss…
especially now as new, more glamorous pretenders to the
throne try to unseat it.

Proponents and repellents only agree for:
Prepared by Priestly in 1776
Anesthetic properties described by Davy in 1799
Used by Horace Wells- 1845

04/15/23 6
Nitrous oxide as seen by supporters:
Weak anesthetic, powerful analgesic (MAC 105%). It
reduces anesthetic and opioid requirements
intraoperatively and improve acute and chronic pain
outcomes postoperatively
Minimal effects on heart rate and blood pressure
But may cause myocardial depression in sick patients
Little effect on respiration
Low blood solubility (quick recovery)

Blood: gas partition co-efficient:
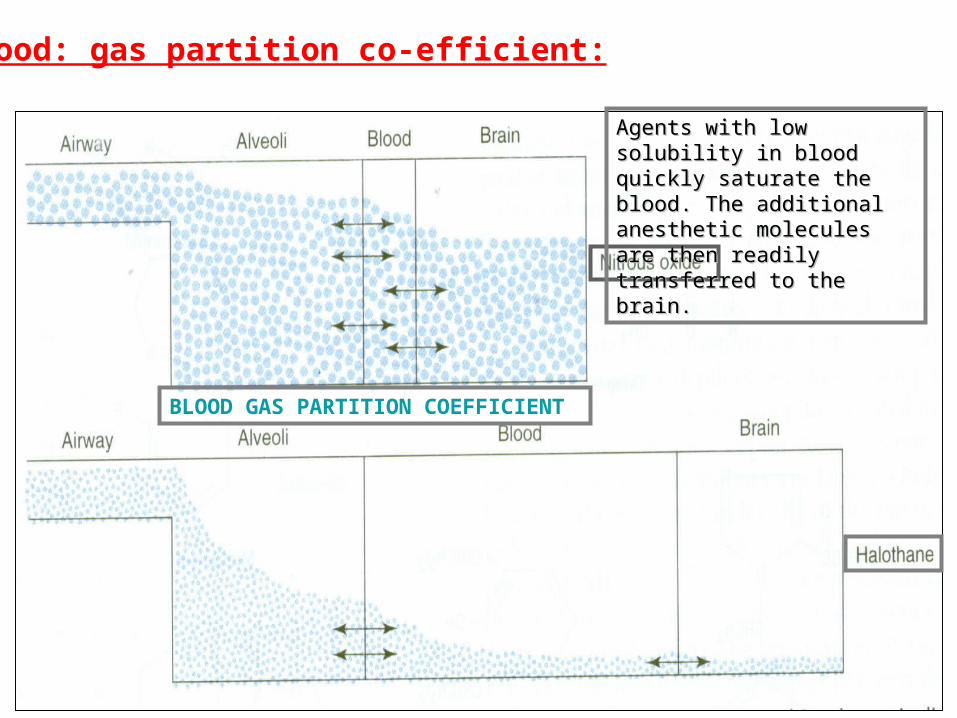
BLOOD GAS PARTITION COEFFICIENT
Agents with low solubility in Agents with low solubility in blood quickly saturate the blood quickly saturate the blood. The additional blood. The additional anesthetic molecules are anesthetic molecules are then readily transferred to then readily transferred to the brain.the brain.
Blood: gas partition co-efficient:

At beginning: second gas effect
At end: diffusion hypoxia
During maintenance: weak
Inhibits methionine synthetase, precursor to DNA synthesis Inhibits vitamin B-12 metabolism
Teratogenic
Nitrous oxide as seen by non-supporters:

OIL GAS PARTITION CO-EFFICIENT
The higher Oil: Gas Partition Co-efficient, the lower the MAC . E.g., Halothane
1.4 220
0.8

04/15/23 11
The point at which nitrous oxide is most hit is that it inhibits methionine synthetase, which increases plasma
homocysteine after surgery
In nonsurgical settings, it is well recognized that long-term increases of plasma levels of homocysteine are an
independent risk factor for coronary artery and cerebral vascular disease.

04/15/23 12
Pathophysiologically, hyperhomocysteinemia have been
found to:
cause endothelial dysfunction impair myocardial substrate
utilization enhance platelet aggregation

04/15/23 13
Cardiovascular events can plausibly be predicted to be
increased with acutely elevated homocystinemia; such increases
have been reported by Badner et al., in moderate-risk patients
having carotid endarterectomy
However, preoperative administration of folate and B
vitamins was shown to inhibit the nitrous oxide–induced increase in
homocysteine.

04/15/23 14
These data -in part- led to the conduct of the ENIGMA-I trial which was published in Anesthesiolog 2007. Entitled “Avoidance of Nitrous Oxide for Patients Undergoing Major Surgery”, this trial was taken by many to be the death knell for nitrous oxide: a view endorsed by the accompanying editorial
04/15/23 15

04/15/23 16
The primary endpoint was duration of hospital stay.
Secondary endpoints included duration of ICU stay, severe
PONV, pneumonia, pneumothorax, pulmonary embolism,
wound infection, myocardial infarction, venous
thromboembolism, stroke, awareness, and death within 30
days

04/15/23 17
This trial recruited 2050 patients, randomly assigning them
to either a nitrous oxide-free (80% oxygen, 20% nitrogen)
group or a nitrous oxide-based (70% nitrous oxide, 30%
oxygen) group.
All patients were scheduled to undergo major surgery of at
least 2 hours duration. It was presented as a pragmatic
study, with no attempt to control for possible confounding
variables and the anaesthetist had the option to cross over
from one group to the other

04/15/23 18
The results showed that there was no difference between the
two groups with regard to the primary endpoint, duration of
hospital stay. Analysis of the secondary endpoints,
however, appeared to show a lower rate of major
complications (wound infection, atelectasis, and
pneumonia) and severe PONV. No significant difference in
major adverse cardiac events or death was reported.

04/15/23 19

04/15/23 20
Harriet W. Hopf, M.D., Department of Anesthesiology, University of Utah wrote:
“This study is not the last word on nitrous oxide, but it is an important
one that is likely to have a major impact on clinical practice in
anesthesia. I personally stopped using nitrous oxide nearly a decade
ago because of previous trials demonstrating the importance of high
tissue oxygen in preventing wound complications. I am pleased to
have added justification for residents who challenge me to provide
evidence to support my clinical practice”

04/15/23 21

04/15/23 22
The validity of ENIGMA results, particularly with regard to the
secondary endpoints, has generated a flurry of controversy. The
opponents of nitrous oxide use have enthusiastically endorsed these
results as definitive evidence to abandon its use. This view is
inappropriate for a number of reasons:
K de Vasconcellos University of KWAZULU-NATAL

04/15/23 23
The chief reason is that the primary endpoint of the study showed no
difference between the two groups. Presumably this endpoint was chosen
as a composite endpoint to reflect any significant adverse postoperative
events, and was adequately powered to detect any significant differences.
The fact that it showed no difference can thus be taken, as one
correspondent to Anesthesiology put it, “as additional evidence of the
remarkable safety of nitrous oxide over the past 150 yr”
K de Vasconcellos University of KWAZULU-NATAL

04/15/23 24
In addition, results of the secondary endpoints must be viewed with
suspicion. As even the authors of ENIGMA noted “We undertook
multiple comparisons, which increases the chance of a type I error; the
secondary, exploratory, and subgroup analyses should be treated
cautiously.”
K de Vasconcellos University of KWAZULU-NATAL

04/15/23 25
Other criticisms of ENIGMA include the choice of 80% O2/20% N2
as a control group. The question which has been raised frequently is
thus, is any difference between the groups due to a nitrous oxide effect
or an oxygen effect? Although academically interesting, I don’t think
it discredits the study. It simply means that if we believe there is a
difference between the groups, it could be due to avoidance of N2O or
due to use of a high inspired concentration of oxygen. It is useful to
know which of these it is, but, as a high FiO2 would be impossible to
achieve with the use of nitrous oxide, for our purposes, it makes little
practical difference.
K de Vasconcellos University of KWAZULU-NATAL
04/15/23 26
A more important factor is that the depth of anaesthesia between the
two groups was not equivalent. The median end-tidal agent
concentration in the nitrous oxide-free group was 0.87 MAC while in
the nitrous oxide group the total was 1.31 MAC. Monk, et al showed
that cumulative deep hypnotic time was an independent predictor of
postoperative mortality
K de Vasconcellos University of KWAZULU-NATAL

04/15/23 27
In addition, due to the pragmatic nature of the study other
confounding variables may not have been adequately
accounted/controlled for. As an example, the nitrous oxide-free group
received significantly more propofol. It’s not possible to say whether
this affected the PONV results, or any other outcomes.
K de Vasconcellos University of KWAZULU-NATAL
04/15/23 28
The authors of ENIGMA have also been accused of bias against N2O.
They appear to have highlighted the adverse secondary outcomes
over the neutral primary outcome. In addition, the study was not
blinded.
K de Vasconcellos University of KWAZULU-NATAL
04/15/23 29
It should also be highlighted that ENIGMA included only patients
undergoing major surgery predicted to last longer than 2 hours. This
represents only a proportion of surgical procedures, and a group of
patients at particular risk of adverse perioperative outcomes
K de Vasconcellos University of KWAZULU-NATAL
04/15/23 30
As a final word on ENIGMA, clinical practice should generally not be
altered on the basis of a single study. This is especially true when
based on secondary outcomes of doubtful validity.
K de Vasconcellos University of KWAZULU-NATAL

04/15/23 31
In response to these concerns regarding ENIGMA, ENIGMA II
commenced enrolment in 2007. This study aims to recruit 7000 patients
at risk of coronary artery disease, undergoing non-cardiac surgery, to test
the hypothesis that omitting N2O will reduce the incidence of death and
major adverse cardiac events. A key difference (vs. ENIGMA) is that the
control group will now use a 70% N2/ 30% O2 mix to avoid the possible
confounding effect of the high FiO2 in ENIGMA and we eagerly await
the results of this study.
K de Vasconcellos University of KWAZULU-NATAL

04/15/23 32

04/15/23 33
wow giving up nitrous in a practice is a profound effect
from a blog article

04/15/23 34
your original post on this matter a few months back caused me to give up nitrous after 28 years; your blog changed a practice 8 thousand miles away!(give or take a few) Thanks!

04/15/23 35
An incredible amount of additional data will be needed to 'out' nitrous oxide. Count on the pharmaceutical industry to lead the search for excuses to supplant N20 with a more expensive, proprietary "solution".

04/15/23 36
No single article, speech, research report or opinion should change a decades-long practice of safe, readily-available, reliable and cost-effective medicine (in any specialty).

04/15/23 37
Hmmm as mentioned in the previous post, this is another example of throwing out the known for the more expensive unknown. Correct me if I'm wrong but its more of a comparison of oxygen versus nitrous!!!
04/15/23 38

04/15/23 39
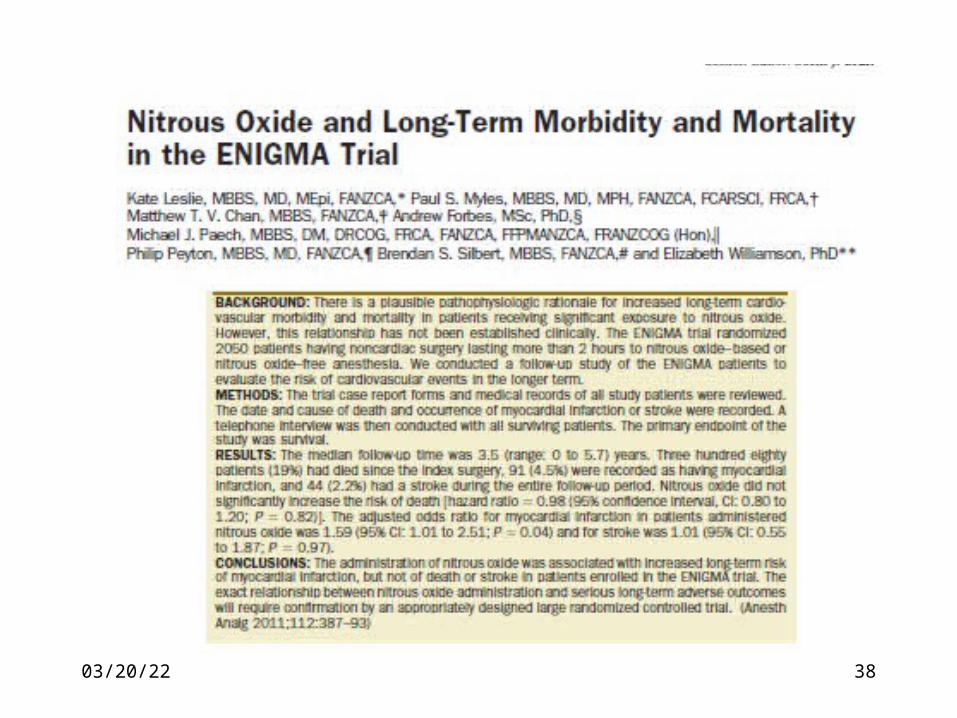
Leslie et al. have published the longer-term results of the original ENIGMA-I trial. They
found that patients exposed to nitrous oxide had an increased incidence of
myocardial infarction, in a mean follow-up period of 3.5 years after a nitrous oxide–
based general anesthetic with no difference in mortality

04/15/23 40

04/15/23 41
The results provided by Leslie et al.15 are a valuable addition to our
knowledge about the effects of intraoperative nitrous oxide. The
article is undoubtedly intriguing; however, it still does not answer
several important safety aspects. There is clearly a need for more
information on this subject. We hope that the ENIGMA-II trial, a
prospective study of intermediate- or high-risk patients randomized to
the use of nitrous oxide that is currently enrolling patients, will help
provide some additional answers.

04/15/23 42

04/15/23 43

04/15/23 44
BACKGROUND: In this post hoc subanalysis of the
Perioperative Ischemic Evaluation (POISE)trial,
we sought to determine whether nitrous oxide
was associated with the primary composite
outcome of
cardiovascular death,
nonfatal myocardial infarction
nonfatal cardiac arrest within 30 days of
randomization.

04/15/23 45
METHODS:
The POISE trial of perioperative β-blockade was
undertaken in 8351 patients. Nitrous oxide anesthesia
was defined as the coadministration of nitrous oxide in
patients receiving general anesthesia, with or without
additional neuraxial blockade or peripheral nerve
blockade. Logistic regression, with inverse probability
weighting using estimated propensity scores, was used to
determine the association of nitrous oxide with the
primary outcome, MI, stroke, death, and clinically
significant hypotension.

04/15/23 46
RESULTS: Nitrous oxide was administered to 1489 (29%) of the 5133
patients included in this analysis. Nitrous oxide had no significant effect
on the risk of the primary outcome, death or clinically significant
hypotension
04/15/23 47
CONCLUSIONS:
nitrous oxide was not associated with an increased risk of adverse
outcomes in the POISE trial patients.
This analysis was limited by the observational nature of the data and the
lack of information on the concentration and duration of nitrous oxide
administration. Further randomized controlled trial evidence is required.
(Anesth Analg 2013;116:1034–40)

04/15/23 48

04/15/23 49
In this issue of the journal, Turan et al. report for the first time that
noncardiac surgery patients receiving general anesthesia with nitrous
oxide (N2O) experience 33% decreased odds of 30-day mortality,
17% decreased odds of in-hospital morbidity and mortality, and 41%
decreased odds of pulmonary morbidity compared with patients
anesthetized without N2O.

04/15/23 50
No amply powered investigations have previously concluded that N2O
anesthesia reduces all-cause mortality or respiratory complications. The
pulmonary N-methyl-daspartate receptor antagonist explanation for
reduced lung injury with N2O proposed by Turan et al. is an assumption
at present, in the absence of targeted experiments using N2O at the
bench and in the clinic to test this hypothesis. Nor can we suggest
another mechanism that could explain such “wonder-working” effects.
04/15/23 51
04/15/23 52
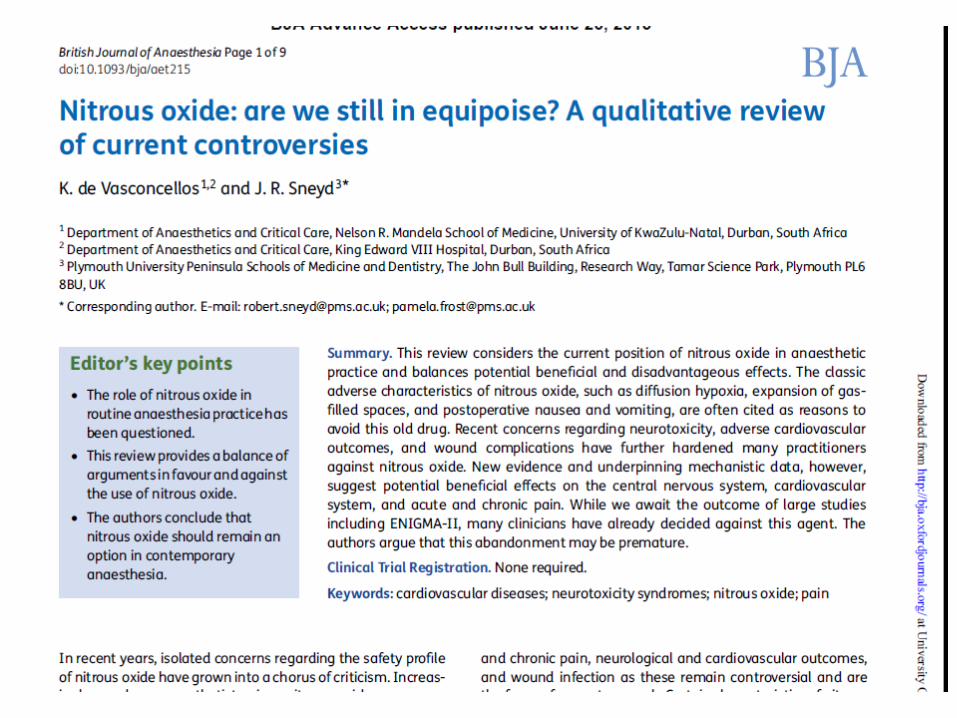
This review considers the current position of nitrous oxide in anaestheticpractice and balances potential beneficial and disadvantageous effects. The classic adverse characteristics of nitrous oxide, such as diffusion hypoxia, expansion of gas filled spaces, and postoperative nausea and vomiting, are often cited as reasons to avoid this old drug. Recent concerns regarding neurotoxicity, adverse cardiovascular outcomes, and wound complications have further hardened many practitioners against nitrous oxide.
New evidence and underpinning mechanistic data, however, suggest potential beneficial effects on the central nervous system, cardiovascular system, and acute and chronic pain. While we await the outcome of large studies including ENIGMA-II, many clinicians have already decided against this agent.
The authors argue that this abandonment may be premature.

04/15/23 53
Conclusion
Nitrous oxide should remain an option in contemporary anaesthesia. There are potential advantages in pain control and prevention, reduction of awareness with recall, and use in neurologically and cardiovascularly ‘at risk’ patients. With respect to its side-effect profile, recent data suggest that nitrous oxide is safe (and possibly beneficial) in an unselected heterogenouspatient population.

04/15/23 54
So, let’s suspend our general bias against nitrous oxide and grant it the place it deserves in anaesthetic practice. We might even find that this faithful old anaesthetic dog has some exciting new tricks to show us.

04/15/23 55
Nitrous oxide is a unique drug with many positive attributes and deserves an important place in anaesthetic practice. Although modern anaesthesia would not collapse with the removal of nitrous oxide, or any other anaesthetic agent, it would be much poorer for its absence.
K de Vasconcellos University of KWAZULU-NATAL

04/15/23 56
NITROUS OXIDE Who will have the last laugh?