Embed Size (px)
DESCRIPTION
There is an urgent need for effective, sustainable child obesity prevention strategies. Progress toward this goal requires strengthening current approaches to add a component that addresses pregnancy onward. Altering early-life systems that promote intergenerational transmission of obesity holds promise for interrupting the continuing cycle of the obesity epidemic. A 2011 Institute of Medicine (IOM) report emphasizes the need for interventions early in life to prevent obesity. A 2010 IOM report called for addressing gaps in existing obesity research evidence by using a systems perspective, simultaneously addressing interacting obesity promoting factors in multiple sectors and at multiple societal levels. A review of evidence from basic science, prevention, and systems research supports an approach that (1) begins at the earliest stages of development, and (2) uses a systems framework to simultaneously implement health behavior and environmental changes in communities.
Citation preview

195
childhood obesityJune 2012 | Volume 8, Number 3© Mary Ann liebert, inc.doi: 10.1089/chi.2012.0004
review
Introduction
Over the past several generations, societal changes have led to the obesity epidemic, with attendant health and economic consequences demanding
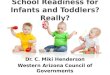
new scientific approaches, policy, and actions.1 Obesity is a complex problem involving contributing factors at mul-tiple levels of social organization, including the family (and its lifestyle habits), community structures and ser-vices (that provide or impede access to healthy food and safe activity), and broad societal forces (and related poli-cies, public understanding, and funding).2 There is grow-ing evidence that risk for childhood obesity is already present during gestation and even before pregnancy via maternal weight and epigenetic influences from the prior generation.3–8 Figure 1 provides a schematic view of the developmental and intergenerational effects of obesity, identifying six elements in an ongoing cycle of obesity risk and transmission. High-risk adolescent girls become
high-risk mothers who have high-risk infants, who in turn become high-risk children and adolescents, and the cycle continues. This information suggests that interrupting the effects of “obesogenic systems”9 early in life holds prom-ise.
In the United States, obesity now affects over 10% of preschool children; an additional 10% are overweight.10 Among low-income children, rates are even higher, with 14% being obese.11–13 Obese preschoolers are likely to be obese later in childhood14 and suffer obesity-related co-morbidities. Adverse effects of obesity appear as early as 3 years old, with obese children exhibiting inflamma-tory biomarkers linked to risk for later heart disease.15 The potential for childhood obesity to be precociously “locked in,”16 along with the persistence of obesity from early childhood to adolescence and adulthood,3,17 support the need for interventions to begin early in the life cycle. The resulting burden—poor health, health disparities, and related costs—is likely to continue to accumulate for
1Department of Pediatrics, University of California, San Diego, La Jolla, CA. 2Department of Health Promotion and Social and Behavioral Health, University of Nebraska Medical Center, Omaha, NE. 3Department of Biostatistics and Epidemiology, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA. 4Center on Social Dynamics and Policy, The Brookings Institution, Washington, DC. 5Departments of Pediatrics and Preventive Medicine, Northwestern University, Chicago, IL.
AbstractThere is an urgent need for effective, sustainable child obesity prevention strategies. Progress toward this goal requires strength-
ening current approaches to add a component that addresses pregnancy onward. Altering early-life systems that promote intergen-erational transmission of obesity holds promise for interrupting the continuing cycle of the obesity epidemic. A 2011 Institute of Medicine (IOM) report emphasizes the need for interventions early in life to prevent obesity. A 2010 IOM report called for address-ing gaps in existing obesity research evidence by using a systems perspective, simultaneously addressing interacting obesity pro-moting factors in multiple sectors and at multiple societal levels. A review of evidence from basic science, prevention, and systems research supports an approach that (1) begins at the earliest stages of development, and (2) uses a systems framework to simultane-ously implement health behavior and environmental changes in communities.
Next steps in obesity Prevention: Altering early life systems to support healthy Parents, infants, and toddlers
Philip R. Nader, M.D.,1 Terry T.-K. Huang, Ph.D., M.P.H.,2 Sheila Gahagan, M.D., M.P.H.,1 Shiriki Kumanyika, Ph.D., M.P.H.,3 Ross A. Hammond, Ph.D.,4
and Katherine Kaufer Christoffel, M.D., M.P.H.5
CHI 8.3 Jun 12 v1.indd 195 5/9/12 11:56 AM

decades18 unless we implement sustainable prevention measures earlier in the life cycle.
MethodsThe co-authors, a multidisciplinary group of senior
investigators, conducted a series of discussions on our understanding of the strengths and weaknesses of cur-rent approaches to the prevention of childhood obesity. A targeted literature review was conducted using PubMed, beginning with the search terms "obesity," "prevention," and "intervention." The search was narrowed to include publications related to pregnant women, infants, children, and adolescents. We began with review articles and used the bibliographies to identify primary studies. We then identified studies that cited those studies to insure the most current literature review. This review process was extensive beginning with 1438 references. We used the U.S. Preventive Services Task Force system to rank evi-dence and to rank order studies to include in our review. Results of the review were used to support the need for and refine a broader early life cycle approach to the pre-vention of childhood obesity.
ResultsMost efforts to combat childhood obesity have focused
on school-aged children and adolescents. The latest
Cochrane review19 suggests that obesity prevention inter-ventions may produce the largest magnitude of effect early in life. Despite this optimistic evidence, how-ever, the epidemic of childhood obesity persists19 and the impact of fetal overnutrition as a risk for continuing adult obesity may continue to reinforce this vicious cycle at the population level in the United States.20,21 Two Institute of Medicine (IOM) reports emphasize both the need for interventions early in life22 and the use of a “systems per-spective”23 to fill in gaps in obesity research evidence that can more effectively guide policy. There is no currently available framework or strategy that has been proposed to translate these IOM recommendations into action. On the basis of the results of our review of evidence from basic science, prevention, and systems research, presented below, and applied to pregnancy and before and infancy through preschool, this article presents for discussion a strategy to interrupt the continued progression of the childhood obesity epidemic. The twin premises of the approach we propose are: (1) Intervention is necessary before, during, and after pregnancy, and for very young children, and (2) systems approaches are needed for sus-tainable prevention of childhood obesity and its conse-quences.
Pregnancy and BeforeParental overweight conveys a major risk for over-
weight in children, for which both parents’ long-term overweight or obesity is the strongest single predictor.24
nader et al.196
Figure 1. Developmental and intergenerational effects of obesity. Significant interstage events include: 1, Intrauterine programming; 2, breastfeeding, early food exposure, attachment stage; 3, early childhood growth, child care, habit formation; 4, brain maturation, self-management, puberty, health behavior change, increased salience of peer effects and school effects; 5, independence, increasing life stress; 6, preconceptual health, parental health status, prenatal care.
Reproductiveage Adolescence
Childhood
ToddlerhoodInfancy
Pregnancy
Inte
rgen
erat
iona
l im
pact
of
ris
ksC
arry over effects across developm
ental stages
1
6
5
2
3
4
CHI 8.3 Jun 12 v1.indd 196 5/9/12 11:56 AM

197childhood obesity June 2012
Maternal obesity before and during pregnancy disrupts glucose homeostasis, insulin sensitivity, amino acid syn-thesis, and fat metabolism, increasing risk for subsequent obesity and disease in the offspring.25,26 Furthermore, ges-tational weight gain is an independent risk factor for obe-sity in the child.27 Both high and low birth weights (linked to maternal obesity) are also associated with higher maternal and infant complications and the development of childhood obesity. Therefore, interventions in pregnancy and early life offer promise for decreasing obesity preva-lence, as both are sensitive periods in which rapid weight gain creates risk for obesity.28 Preventing preconception obesity and excessive pregnancy weight gain and avoid-ing postpartum weight retention are important strategies for reducing obesity prevalence in adult women.29 In Proj-ect Viva, walking and vigorous physical activity in mid-pregnancy were protective against excessive gestational weight gain.30 Individual counseling, self-monitoring of diet and activity, and education paired with motivational interviewing are effective strategies in limiting excessive weight gain. In addition, postpartum weight loss reduces the likelihood of high birth weight and risk for later obe-sity in the next child.31
Infancy to Preschool Rapid weight gain during infancy significantly increas-
es the risk of later obesity.32–35 Therefore, monitoring infant weight gain and attention to nutrition during the first 12 months is crucial. Breastfeeding is associated with a small but significant reduction in risk for obesity, and breastfeeding promotion interventions can be successful.36 Recent analyses from the Feeding Infants and Toddlers Study indicate that the diets of young children remain less than optimal, with too many “empty calorie” foods consumed by children, even in the first year.37,38 Pairing breastfeeding with healthful weaning foods is likely to promote healthy weight trajectories.39–43
Attention to nutrition, physical activity, and screen time are important strategies in early childhood, and parents are important influences on all three. A recent review of effectiveness of interventions aimed at reducing screen time found that while overall there was no evidence of impact on BMI, interventions among the preschool age group held promise.44 A primary care–based intervention directed to 2- to 6-year-old overweight and obese chil-dren did not impact BMI, but the authors suggested that broader approaches could be more effective than primary healthcare interventions alone.45 Nutrition and physical activity practices in nonparental child care sites impact 61% of U.S. children less than 6 years old.46 The IOM report on early childhood obesity prevention22 calls atten-tion to community environmental influences on childhood obesity. Individual-, family-, and center-based early child-hood obesity interventions have been effective, using a combination of nutrition education, guided physical activ-ity, limitation of television viewing, and/or remuneration for participation. Attention to environmental determinants
and adequate intervention and follow-up time increased the likelihood of effectiveness.47
In summary, current evidence supports increased emphasis in obesity prevention efforts on promoting: Optimal preconceptual weight, avoiding excessive ges-tational weight gain, returning toward a healthy postpar-tum weight, breastfeeding promotion, monitoring infant growth for rapid weight gain, promotion of healthy wean-ing foods, limiting screen time, and child care practices48 that promote healthy nutrition and physical activity in young children.
A Systems ApproachA systems approach is one that explicitly focuses on the
interconnections between different aspects of the environ-ment and between individuals and the environment. This is what distinguishes a systems approach from a tradition-al multilevel or multicomponent model. Multicomponent interventions are not the same as systems interventions. Adding systems approaches to whole community—mul-tilevel, multicomponent—interventions allows investiga-tors from the onset to determine the interactions among the systems and sectors that will be required to result in intervention sustainability (persistence of changes made and ongoing adoption of new ones), scalability (diffusion across settings), and reach (across population subgroups).49–52 This is a crucial addition that may well assure adequate strength of the interventions and lead to a wider population change that will impact the course of the epidemic. The concept of multilevel influences on human behavior is well established in public health research and practice as the “ecological model.”53 Socioecological models advocate for combining individual and environ-mental approaches, but do not address how the different levels influence each other and whether that makes a dif-ference in the overall outcomes. Socioecological models also do not inform what is the optimal mix and sequence of intervention strategies to bring about sustained popula-tion-wide impact. This is important given new evidence that adult weight gain and loss do not occur in a linear trajectory,54 suggesting that different combinations and/or sequences of interventions of varying modalities may be needed throughout the developmental pathway to bring about sustained population impact across the age span influenced by early life-cycle systems.
Evolving systems methods49 offer tools to anticipate and leverage complex interactions, feedbacks, and conse-quences in planning interventions. For example, aligning priorities in disparate sectors (e.g., early child care sys-tems, public schools, health agencies, and primary care providers) will lead to new interactions between sectors. These interinstitutional alignments can be defined by sys-tems interactions and can estimate the synergistic effects of coordinating separate sector interventions. Systems methods can also identify key mechanisms at work that affect the evaluation of interventions. Complex interac-
CHI 8.3 Jun 12 v1.indd 197 5/9/12 11:56 AM

nader et al.198
tion effects, nonlinearities, and dynamic feedback can be difficult to capture in traditional statistical approaches and randomized controlled trial interventions and designs. Systems modeling can provide a valuable complement to conventional research methods.50,55 Systems tools can also help us anticipate unintended consequences when other-wise well-intended interventions are implemented.49,50
Although there is broad agreement that obesity is deter-mined by factors at multiple levels of social organization and across sectors—from the food industry to transporta-tion policy—public health and healthcare systems have been somewhat slow to embrace a systems approach to prevention. However, whole community interventions to prevent obesity in the United States and elsewhere are documented and continue to be evaluated.56–61 Many of these interventions focus on changing social norms via community health promotion (nutrition education and media), school and community mobilization, leadership by political officials, business participation, and attempts to remove individual-level barriers to healthy eating and physical activity. Examples include the multicomponent
projects Shape Up Somerville62 (a city-wide campaign to increase daily physical activity and healthy eating in Somerville, MA) and “Together Let’s Prevent Childhood Obesity”63 (EPODE, in numerous cities and towns in Europe). These interventions have resulted in less weight gain in older children and adolescents. Whole community systems approaches aimed much earlier in the life cycle remain to be tested.
A Systems Framework To Prevent Obesity by Targeting Early Life
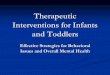
To provide a framework to guide the implementation of a systems approach targeting early life, Figure 2 illustrates how policies and practices at the local, state, and national level directly and indirectly affect community-level physi-cal and social environments, the economic environment, healthcare systems, and family and individual health behaviors. These systems influence health behaviors and environments that impact both adults and children simul-
Figure 2. A community systems framework of early intervention of childhood obesity with feedbacks between individuals and the environment. Systems pathways: 1. Policies related to urban planning, housing, transportation, parks and recreation, food availability, access, financing and marketing, and edu-cation. 2. Policies on media and information, housing segregation, industry practices, labor, individual incentives (tax, insurance). 3. Policies on healthcare infrastructure, financing, delivery mode. 4. Interplay between social and physical environment. 5. Social and physical environments enable and/or constrain family and individual behavior. Individuals can also shape their environment. 6. Preventive and treatment services to families and individuals. 7. Healthcare providers’ behaviors and practices, policies, and as advocates for social and environmental changes to promote healthy lifestyles. 8. Individual empowerment and community mobilization to effect policy change.
CHI 8.3 Jun 12 v1.indd 198 5/9/12 11:56 AM

199childhood obesity June 2012
taneously, principally in the family setting, but also within community institutions, such as child care and schools for children, work site and neighborhoods for adults, and healthcare systems for both children and adults.64 Systems interaction pathways (1–8, see Fig. 2) are identified, giv-ing a template for designing interventions that specifically enhance pathways that promote healthy behaviors, and dis-rupt pathways that perpetuate obesity, requiring program-ming impacting both adults and children.
System pathways impact behaviors that ultimately determine weight status. As illustrated in Figure 2, for mothers and young children, these eating and activity behaviors are nested within family and cultural beliefs, customs and habit, and adult behaviors and role model-ing related to child feeding and physical activity. Parental choices for their own and their children’s behaviors are influenced by the relative costs involved for parents. Interventions that deal with relative cost issues to families may yield faster change than those related to family cul-tural norms and attitudes. Supports in physical environ-ments (e.g., settings where children and young families spend time, neighborhood characteristics) and social environments (e.g., social relationships, social norms, and cultural influences) are shown as key factors that enable or constrain family and individual behavior. Because the physical environment can shape the social and cultural environment over time, and the social and cultural envi-ronment can perpetuate the status quo in the physical environment, both need to be addressed simultaneously to disrupt the lockstep cycle that prevents progress and change. Physical and social environments are influ-
enced by local, state, and national policies and can also be changed through advocacy by individuals, families, and institutions. Advocacy and policy go hand in hand. Examples of physical environments include lack of access to fresh vegetables and fruits in certain neighborhoods (“food deserts”), or lack of safe places to walk, exercise, or ride bikes. Healthcare and community systems provide obesity prevention and treatment services to individuals and families and are also influenced by local, state, and national policies. Direct advocacy by primary care health practitioners and others who work within community health systems is an important pathway to change physi-cal and social environments in communities.
Complex systems-oriented inteventions65 are geared toward generating solutions to real-world situations that continually change. Such system issues become critical to intervention design, and effectiveness, with focused attention to contextual issues unique to each community. Because obesity prevalence among children and adults var-ies by geographic area, race/ethnicity, and socioeconomic status,66,67 “place-based” community and family interven-tions aiming to prevent excessive maternal weight gain during pregnancy and caloric balance in young mothers and children are proposed. Little is known about cost-effec-tiveness68 of obesity prevention strategies and the potential of systems approaches69 at this early stage.
Evidenced-based sustainable behavior change interven-tions70,71 that parallel policy and environmental change efforts are key components, with a common set of health behavior goals for the three target developmental stag-es—pregnancy, infancy, and toddler. The goals (shown in Table 1) are categorical rather than specific in recog-nition that prevailing guidelines will change over time. Table 2 gives examples of what this approach would look like to influence change through the pathways in Figure 2. For example, access to fresh foods could be enhanced via pathways 1 and 2 through policies promot-ing use of food stamps for fresh fruits and vegetables at farmer’s markets. The primary healthcare sector can implement the latest patient care protocols supporting healthy weight in mothers and young children and make available family-based health promotion behavior change classes (pathway 6). The health sector can also advocate (pathway 7) with government, schools, early child care groups, and birthing hospitals to adopt policies that cre-ate environments that support families to carry out the behavioral goals listed in Table 1. Table 3 summarizes examples of policy, professional action, and public edu-cation targets for early life systems change organized by developmental stage.
DiscussionBeginning obesity prevention in pregnancy has been
suggested before,26 but not with the supporting rationale and systems strategies proposed in this paper. Whole community interventions addressing both policy and
Table 1. Early Life Systems: Key Behavior Intervention TargetsPregnancy
• Engage in early prenatal, post-natal, and inter-conceptual care
• Achieve healthy gestational weight gain
• Post-partum return towards a healthy weight
• Prepare to breast feed
Infancy
• Initiate and maintain breast feeding
• Appropriate introduction of other beverages and foods
• Support for healthy sleep patterns
• Support for appropriate soothing, not always using food
• Support for motor development
• Avoid excessive weight gain in infancy
• Avoid screen time
Toddler Years
• Active play at least one hour per day, limitation of screen time
• Consumption of healthy foods, snacks, and un-sweetened beverages in appropriate portion sizes
• Healthy nutrition and activity standards in childcare settings
• Limit screen time
CHI 8.3 Jun 12 v1.indd 199 5/9/12 11:56 AM

nader et al.200
behavior change have led to leveling of the progression of overweight in targeted groups. Applying place-based early life systems–oriented health behavior change inter-ventions combined with simultaneously implemented
supportive environmental changes is the next logical step in obesity prevention efforts.
Combining simultaneous behavioral and environmental change marks a notable departure from existing single
Table 2. Pathways for Early Life SystemsSystems pathways framework (Figure 2) Examples of systems interactions
1. Policies related to urban planning, housing, transportation, parks and recreation, food availability, access, financing and marketing, and education
Increased access to safe places for physical activity using primary medical care “Rx for physical activity” honored by local recreation centers; joint use agreements between parks and recreation and schools.
2. Policies on media and information, housing (e.g., segregation), industry practices, labor, individual incentives (tax, insurance, etc.)
Policies on advertising to young children, WIC incentives for breastfeeding, lactation support for working mothers; day care food and activity policies and certification.
3. Policies on healthcare infrastructure, financing, delivery mode
Culturally relevant family behavior change programs, use of lay health outreach educators connecting primary care and community prevention; institution of baby-friendly practices in birthing institutions and prenatal care; community prevention campaigns, surveillance and monitoring of population health outcomes (BMI).
4. Interplay between social and physical environment Attempt to change social and physical environments through social networks and urban redevelopment to shift social norms and culture.
5. Social and physical environments that enable and/or constrain family and individual behavior; Individuals shaping their environment
Identify barriers and supports for families and provide tools to help them make small changes in their immediate environment.
6. Preventive and curative services to families and individuals Update pregnancy, postpartum, and pediatric clinical protocols to provide same age-appropriate health messages and services to interconceptual and pregnant women, and postnatal nutrition and activity goals.
7. Healthcare providers’ behaviors, policies, and practices, and as advocates for social and environmental changes to promote healthy lifestyles
Develop toolkits to equip providers with advocacy skills; provider training on latest IOM/ACOG policies and health system guidelines; support provider engagement with community agencies such as WIC, and child care providers.
8. Individual empowerment and community mobilization to effect policy change
Use grassroots advocacy and civic participation to promote policy change.
IOM, Institute of Medicine; ACOG, American Congress of Obstetricians and Gynecologists; WIC, Women, Infants and Children Program.
Table 3. Strategies for Policy, Professional Behavior, and Public Education Supporting Individual and Family Health Behavior Changes for Pregnancy, Infancy, and Toddlers
In addition to policies and built environments supporting safety, walkability, access to healthy foods and water, and active transportation
Pregnancy Infancy Toddler
PO
LIC
Y • Baby-friendly policies in prenatal care and birthing institutions
• Work site and service site lactation support policies
• Day care food and activity policies and certification
• Creation of children’s zones to encourage healthy behaviors
PR
OF
ES
SIO
NA
L
• Incorporate most recent IOM/ACOG guidelines in prenatal/interconceptual care
• Consistent health recommendations regarding breastfeeding and infant nutrition from prenatal and postnatal health providers
• Monitor infant growth with appropriate infant nutrition recommendations
• Provider encouragement and reinforcement of family activity behavior and home environment change, parenting, sleeping and infant soothing techniques other than feeding
• Provider advocacy for work site lactation support
• Day care and health provider encouragement and reinforcement of family health behavior changes in food and snack choices, sweetened foods and beverages, portion size, and screen time
• Provider encouragement of daily activity/play time
• Provider advocacy for healthy day care environments
ED
UC
AT
ION
• Community support systems for timely prenatal care and breastfeeding preparation
• Community support for and awareness of maintaining a healthy maternal weight before, during, and after pregnancy
• Same current health messages from all infant care providers
• WIC support and incentives to continue breastfeeding
• Community systems support ability of families with infants to achieve a healthy home environment
• Day care encouragement and modeling of changes in food and snack choices, sweetened foods and beverages, portion size, and screen time
• Family and community resource centers reinforce same targeted health behaviors
IOM, Institute of Medicine; ACOG, American Congress of Obstetricians and Gynecologists; WIC, Women, Infants and Children Program.
CHI 8.3 Jun 12 v1.indd 200 5/9/12 11:56 AM

201childhood obesity June 2012
modality approaches (behavior change only or environ-mental change only). Whitaker72 noted that traditional research methods, such as the randomized trial, are lim-ited in addressing the complex factors involved in child-hood obesity. The approach presented here uses systems methods that take into account attitudes and norms in a defined community, as well as the challenges imposed by broader societal values and physical, social, and institu-tional barriers to change. The public message would be to promote well-being as opposed to avoiding poor health outcomes. For example, providing the best chances for a healthy life for an expected offspring is likely to be more valued by the average person than linking motivation for behavior changes to a distant goal of avoiding extra weight because of increased risks for chronic disease later in life.
To see if building early life systems–oriented solutions to obesity works, we propose a series of community-driven, coordinated, place-based interventions that are rigorously evaluated. Sites with experience in cross-sector collaboration, with strong research methodologists and community leadership and partnerships, would be selected through a competitive mechanism with national oversight from a major public health research institu-tion. For example, selection of 8–10 specific communi-ties reflecting diverse populations would implement and evaluate interventions tailored to the unique strengths and constraints of participating local communities. The evalu-ation would combine the strengths of community-based participatory research with the rigor of the randomized clinical trial. The interventions would be standardized, but intentionally variable with regard to delivery meth-ods, cultural tailoring, and real-world problem solving. Comparisons could be done with cluster randomization, or simulated through multiple baselines, or interrupted time series analyses in a single population. Iterations in several communities add validity to overall conclu-sions of effectiveness. Standardized outcome measures and analytical methods will be employed. Design and oversight responsibilities are shared by research method-ologists and community leaders. This method has been suggested as a “multisite translational community trial” to test the real-world community efficacy of complex health promotion interventions.73
The series of interventions would be evaluated by the outcomes of healthier weight for childbearing women and their infants and young children. Follow-up should con-tinue long enough to track adult and child weights, and to document the sustainability, costs, and any demographic changes over time.
Is it feasible to implement and evaluate this added emphasis to current obesity prevention efforts? Feasibil-ity is linked to prioritization of financial resources, which potentially contrasts the values of remaining with the sta-tus quo intervention and research methods, compared to the costs of testing a broader paradigm and methods. Both need to be referenced to the estimated costs of a continu-
ing obesity epidemic. Currently, obesity-related diseases account for 10% of U.S. medical spending, or an estimat-ed $147 billion/year. Estimates of medical costs associat-ed with treatment of obesity related diseases are projected to increase by $48 to $66 billion/year in the United States by 2030.74 The National Institutes of Health (NIH) spent $971 million in fiscal 2010 on obesity research. In 2010, the CDC awarded $372.8 million to 44 communities for “Communities Putting Prevention to Work” (CPPW) grants to improve nutrition and physical activity, reduce obesity, and prevent smoking. An additional $100 mil-lion has been allocated for “Community Transformation Grants” to prevent chronic diseases and health disparities. Funds for testing this approach could conceivably come from prioritizing existing and planned funding streams directed toward reducing the economic and health bur-dens of a continuing obesity epidemic. Using a systems approach might eventually result in cost savings because of cost-efficiencies gained through coordination of exist-ing policy and behavior change interventions and the avoidance of redundancies, as well as rapid identification and remedy of costly unintended consequences.75
One of the first multilevel, multicomponent, school-based interventions to simultaneously address both policy and behavioral interventions was the Child and Adolescent Trial for Cardiovascular Health/Coordinated Approach to Child Health (CATCH) study. At that time (1987–1996), multicomponent interventions were novel to researchers. Today, there is substantial experience with policy (e.g., baby-friendly and lactation support policies) and health behavior intervention research (e.g., limiting excessive gestational weight gain and early childhood interventions). What remains to be done is to implement and evaluate policy change and health behavior change at the same time in the same place, using systems-based methods that include the interactions among individuals and environments. The current experience of U.S. com-munities that have already implemented environmental changes, such as those participating in CDC’s CPPW and Community Transformation Grants, provides a pool of communities that could be ready to implement and test this combined approach applied to the systems impacting early life.
ConclusionThe approach proposed in this paper—to focus a new
effort on evaluating multiple place-based (defined com-munity) systems-oriented interventions designed around pregnancy, resulting in a healthy weight for women and their offspring—is intended to launch a discussion among private and public health practitioners and investigators, leaders in maternal and child health, policy makers, gov-ernment agencies, and private foundations on the merits of adding this approach to obesity prevention efforts. Federal and private agency initiatives reflect a growing momentum to alter the systems that feed the continuation
CHI 8.3 Jun 12 v1.indd 201 5/9/12 11:56 AM

nader et al.202
of the obesity epidemic. We believe this is the next logical step in obesity prevention, built upon the tools and expe-rience gained over the last 30 years and that the nation could be prepared to take on this challenge.
AcknowledgmentsThe authors gratefully acknowledge: Natalia Veronique
Lotz, medical student, Eastern Virginia Medical School, and Matthew Cappiello, medical student, University of Cali-fornia, San Diego School of Medicine, for their assistance with literature review for this paper. We also appreciate the careful manuscript preparation and review by Christine Williams, M.P.H., and Estela Blanco, M.P.H., M.A. In addi-tion, thanks to Melinda Bender, R.N., Ph.D., and Yvette La Coursiere, M.D., M.P.H., Assistant Clinical Professor, Department of Obstetrics and Gynecology, Reproductive Medicine, University of California, San Diego, for their suggestions of literature pertaining to intervention with preschool Latino children and relevant studies and policies related to maternal overweight before and during pregnancy.
Author Disclosure Statement No competing financial interests exist for Drs. Nader, Huang, Gaha-gan, Kumanyika, Hammond. Northwestern University receives salary support from CDC/ CPPW for Dr. Kaufer Christoffel.
References 1. Gortmaker SL, Swinburn BA, Levy D, et al. Changing the future of
obesity: Science, policy, and action. Lancet 2011;378:838–847.2. Brown T, Kelly S, Summerbell C. Prevention of obesity: A review
of interventions. Obes Rev 2007;8(Suppl 1):127–130.3. Whitaker RC, Wright JA, Pepe MS, et al. Predicting obesity in
young adulthood from childhood and parental obesity. N Engl J Med 1997;337:869–873.
4. Seckl JR. Physiologic programming of the fetus. Clin Perinatol 1998;25:939–962, vii.
5. Rogers I. The influence of birthweight and intrauterine environ-ment on adiposity and fat distribution in later life. Int J Obes Relat Metab Disord 2003;27:755–777.
6. Oken E, Gillman MW. Fetal origins of obesity. Obes Res 2003;11:496–506.
7. Moschonis G, Grammatikaki E, Manios Y. Perinatal predictors of overweight at infancy and preschool childhood: The GENESIS study. Int J Obes 2007;32:39–47.
8. Nelson SM, Matthews P, Poston L. Maternal metabolism and obe-sity: Modifiable determinants of pregnancy outcome. Hum Reprod Update 2010;16:255–275.
9. Swinburn B, Egger G, Raza F. Dissecting obesogenic environ-ments: the development and application of a framework for identi-fying and prioritizing environmental interventions for obesity. Prev Med 1999;29:563–570.
10. Ogden CL, Carroll MD, Curtin LR, et al. Prevalence of high body mass index in US children and adolescents, 2007–2008. JAMA 2010;303:242–249.
11. Freedman DS, Ogden CL, Flegal KM, et al. Childhood overweight and family income. MedGenMed. 2007;9:26.
12. Mason M, Meleedy-Rey P, Christoffel KK, et al. Prevalence of overweight and risk of overweight among 3- to 5-year-old Chicago children, 2002-2003. J Sch Health 2006;76:104–110.
13. Obesity prevalence among low-income, preschool-aged chil-dren—United States, 1998–2008. MMWR Morb Mortal Wkly Rep 2009;58:769–773.
14. Nader PR, O’Brien M, Houts R, et al. Identifying risk for obesity in early childhood. Pediatrics 2006;118:e594–e601.
15. Skinner AC, Steiner MJ, Henderson FW, et al. Multiple markers of inflammation and weight status: Cross-sectional analyses through-out childhood. Pediatrics 2010;125:e801–e809.
16. Gillman MW. Early infancy as a critical period for development of obesity and related conditions. Nestle Nutr Workshop Ser Pediatr Program 2010;65:13–20; discussion 20–14.
17. Freedman DS, Khan LK, Serdula MK, et al. The relation of child-hood BMI to adult adiposity: The Bogalusa Heart Study. Pediatrics 2005;115:22–27.
18. Wang Y, Beydoun MA, Liang L, et al. Will all Americans become overweight or obese? Estimating the progression and cost of the US obesity epidemic. Obesity (Silver Spring) 2008;16:2323–2330.
19. Waters E, de Silva-Sanigorski A, Hall BJ, et al. Interventions for preventing obesity in children. Cochrane Database Syst Rev 2011;12:CD001871.
20. Flegal KM, Carroll MD, Ogden CL, et al. Prevalence and trends in obesity among US adults, 1999–2008. JAMA 2010;303:235–241.
21. Levi J, Segal L, St. Laurent R, et al. F as in Fat: How Obesity Threatens America’s Future. Trust for America’s Health: Robert Wood Johnson Foundation: Washington, DC, 2011.
22. Birch L, Burns A (eds), Early Childhood Obesity Prevention Poli-cies. Institute of Medicine Committee on Obesity Prevention Poli-cies for Young Children. National Academies Press: Washington, DC, 2011.
23. Kumanyika SK, Parker L, Sim LJ (eds), Bridging the Evidence Gap in Obesity Prevention. A Framework to Inform Decision Mak-ing. Institute of Medicine, National Academies Press: Washington, DC, 2010.
24. Jaaskelainen A, Pussinen J, Nuutinen O, et al. Intergenera-tional transmission of overweight among Finnish adolescents and their parents: A 16-year follow-up study. Int J Obes (Lond) 2011;35:1289–1294.
25. Barker DJ. In utero programming of chronic disease. Clin Sci (Lond) 1998;95:115–128.
26. Wojcicki JM, Heyman MB. Let’s Move—Childhood obesity prevention from pregnancy and infancy onward. N Engl J Med 2010;362:1457–1459.
27. Oken E, Rifas-Shiman SL, Field AE, et al. Maternal gestational weight gain and offspring weight in adolescence. Obstet Gynecol 2008;112:999–1006.
28. Dietz WH. Critical periods in childhood for the development of obesity. Am J Clin Nutr 1994;59:955–959.
29. Asbee SM, Jenkins TR, Butler JR, et al. Preventing excessive weight gain during pregnancy through dietary and lifestyle counsel-ing: A randomized controlled trial. Obstet Gynecol 2009;113:305–312.
30. Olson CM, Strawderman MS, Reed RG. Efficacy of an intervention to prevent excessive gestational weight gain. Am J Obstet Gynecol 2004;191:530–536.
31. Getahun D, Ananth CV, Peltier MR, et al. Changes in prepreg-nancy body mass index between the first and second pregnancies and risk of large-for-gestational-age birth. Am J Obstet Gynecol 2007;196:530 e531–e538.
CHI 8.3 Jun 12 v1.indd 202 5/9/12 11:56 AM

203childhood obesity June 2012
32. Taveras EM, Rifas-Shiman SL, Sherry B, et al. Crossing growth percentiles in infancy and risk of obesity in childhood. Arch Pedi-atr Adolesc Med 2011;165:993–998.
33. Chomtho S, Wells JC, Williams JE, et al. Infant growth and later body composition: Evidence from the 4-component model. Am J Clin Nutr 2008;87:1776–1784.
34. Botton J, Heude B, Maccario J, et al. Postnatal weight and height growth velocities at different ages between birth and 5 y and body composition in adolescent boys and girls. Am J Clin Nutr 2008;87:1760–1768.
35. Ekelund U, Ong K, Linne Y, et al. Upward weight percentile crossing in infancy and early childhood independently predicts fat mass in young adults: The Stockholm Weight Development Study (SWEDES). Am J Clin Nutr 2006;83:324–330.
36. Dyson L, McCormack F, Renfrew MJ. Interventions for promoting the initiation of breastfeeding. Cochrane Database of Systematic Reviews 2005. Art. no. CD001688.
37. May AL, Dietz WH. The Feeding Infants and Toddlers Study 2008: Opportunities to assess parental, cultural, and environmental influ-ences on dietary behaviors and obesity prevention among young children. J Am Diet Assoc 2010;110:S11–S15.
38. Briefel R, Ziegler P, Novak T, et al. Feeding Infants and Toddlers Study: Characteristics and usual nutrient intake of Hispanic and non-Hispanic infants and toddlers. J Am Diet Assoc 2006;106:S84–S95.
39. Esposito L, Fisher JO, Mennella JA, et al. Developmental perspec-tives on nutrition and obesity from gestation to adolescence. Prev Chronic Dis 2009;6:A94.
40. Owen CG, Martin RM, Whincup PH, et al. The effect of breast-feeding on mean body mass index throughout life: A quantitative review of published and unpublished observational evidence. Am J Clin Nutr 2005;82:1298–1307.
41. Owen CG, Martin RM, Whincup PH, et al. Effect of infant feeding on the risk of obesity across the life course: A quantitative review of published evidence. Pediatrics 2005;115:1367–1377.
42. Arenz S, Ruckerl R, Koletzko B, et al. Breast-feeding and child-hood obesity—A systematic review. Int J Obes Relat Metab Disord 2004;28:1247–1256.
43. Harder T, Bergmann R, Kallischnigg G, et al. Duration of breast-feeding and risk of overweight: A meta-analysis. Am J Epidemiol 2005;162:397–403.
44. Wahi G, Parkin PC, Beyene J, et al. Effectiveness of interventions aimed at reducing screen time in children: A systematic review and meta-analysis of randomized controlled trials. Arch Pediatr Adolesc Med 2011;165:979–986.
45. Taveras EM, Gortmaker SL, Hohman KH, et al. Randomized con-trolled trial to improve primary care to prevent and manage child-hood obesity: The High Five for Kids Study. Arch Pediatr Adolesc Med 2011;165:714–22 epub.
46. America’s children—key national indicators of well-being, 2009—family and social environment. Childstats.gov 2009. Available at www.childstats.gov/americaschildren/famsoc3.asp#19/. Last accessed April 16, 2012.
47. Bluford D, Sherry B, Scanlon K. Interventions to prevent or treat obesity in preschool children: A review of evaluated programs. Obesity (Silver Spring) 2007;15:1356–1372.
48. Story M, Kaphingst KM, French S. The role of child care settings in obesity prevention. Future Child 2006;16:143–168.
49. Huang TT, Drewnosksi A, Kumanyika S, et al. A systems-oriented multilevel framework for addressing obesity in the 21st century. Prev Chronic Dis 2009;6:A82.
50. Hammond RA. Complex systems modeling for obesity research. Prev Chronic Dis 2009;6:A97.
51. Mabry PL, Marcus SE, Clark PI, et al. Systems science: A revolution in public health policy research. Am J Public Health 2010;100:1161–1163.
52. Levy DT, Mabry PL, Wang YC, et al. Simulation models of obe-sity: A review of the literature and implications for research and policy. Obes Rev 2011;12:378–394.
53. McLeroy KR, Bibeau D, Steckler A, et al. An ecological perspec-tive on health promotion programs. Health Educ Q 1988;15:351–377.
54. Hall KD, Sacks G, Chandramohan D, et al. Quantification of the effect of energy imbalance on bodyweight. Lancet 2011;378:826–837.
55. Glass TA, McAtee MJ. Behavioral science at the crossroads in pub-lic health: Extending horizons, envisioning the future. Soc Sci Med 2006;62:1650–1671.
56. Gooze RA, Hughes CC, Finkelstein DM, et al. Reaching staff, par-ents, and community partners to prevent childhood obesity in Head Start, 2008. Prev Chronic Dis 2008;7:A54.
57. Gleeson B, Sipe NG. Creating child friendly cities: Reinstating kids in the city. Routledge: New York, 2006.
58. Advancing the Movement at: Communities Uniting for a Healthy and Prosperous 3rd American Century. Available at www.advancingthemovement.org/Default.aspx/. Last accessed April 16, 2012.
59. Chomitz VR, McGowan RJ, Wendel JM, et al. Healthy Liv-ing Cambridge Kids: A community-based participatory effort to promote healthy weight and fitness. Obesity (Silver Spring) 2010;18(Suppl 1):S45–S53.
60. de Silva-Sanigorski AM, Bell AC, Kremer P, et al. Reducing obesity in early childhood: Results from Romp & Chomp, an Australian community-wide intervention program. Am J Clin Nutr 2010;91:831–840.
61. de Silva-Sanigorski A, Prosser L, Carpenter L, et al. Evaluation of the childhood obesity prevention program Kids— ‘Go for your life’. BMC Public Health 2010;10:288.
62. Economos CD, Hyatt RR, Goldberg JP, et al. A community inter-vention reduces BMI z-score in children: Shape Up Somerville first year results. Obesity (Silver Spring) 2007;15:1325–1336.
63. Fussenegger D, Pietrobelli A, Widhalm K. Childhood obesity: political developments in Europe and related perspectives for future action on prevention. Obes Rev 2008;9:76–82.
64. Katz DL. Advancing the health of families: Who’s the BAWSS? Childhood Obes 2011;7:73–75.
65. Huang T, Grimm B, Hammond R. A systems-based typological framework for understanding the sustainability, scalability, and reach of childhood obesity interventions. Children's Health Care 2011;40:253–266.
66. Bethell C, Simpson L, Stumbo S, et al. National, state, and local disparities in childhood obesity. Health Aff 2010;29:347–356.
67. Cossrow N, Falkner B. Race/ethnic issues in obesity and obesity-related comorbidities. J Clin Endocrinol Metab 2004;89:2590–2594.
68. Carter R, Moodie M. The cost-effectiveness of obesity prevention. In: Crawford D, Jeffery, RW (ed), Obesity prevention and public health. Oxford University Press: Oxford, New York: 2005:xiii, pp 338.
69. Cawley J. The cost-effectiveness of programs to prevent or reduce obesity: The state of the literature and a future research agenda. Arch Pediatr Adolesc Med 2007;161:611–614.
70. Nader PR, Stone EJ, Lytle LA, et al. Three-year maintenance of improved diet and physical activity: The CATCH cohort Child and Adolescent Trial for Cardiovascular Health. Arch Pediatr Adolesc Med 1999;153:695–704.
CHI 8.3 Jun 12 v1.indd 203 5/9/12 11:56 AM

71. Nader PR, Sallis JF, Patterson TL, et al. A family approach to cardiovascular risk reduction: Results from the San Diego Family Health Project. Health Educ Q 1989;16:229–244.
72. Whitaker RC. The childhood obesity epidemic: Lessons for pre-venting socially determined health conditions. Arch Pediatr Ado-lesc Med 2011;165:973–975.
73. Katz DL, Murimi M, Gonzalez A, et al. From controlled trial to community adoption: The multisite translational community trial. Am J Public Health 2011;101:e17–e27.
74. Wang YC, McPherson K, Marsh T, et al. Health and economic bur-den of the projected obesity trends in the USA and the UK. Lancet 2011;378:815–825.
75. Clancy TR, Effken JA, Pesut D. Applications of complex systems theory in nursing education, research, and practice. Nursing Out-look 2008;56:248–256.e243.
Address correspondence to:Philip R. Nader, M.D.
Professor Emeritus of PediatricsDepartment of Pediatrics
University of California, San Diego9500 Gilman Drive, MC 0927
La Jolla, CA 92093-0927E-mail: [email protected]
nader et al.204
CHI 8.3 Jun 12 v1.indd 204 5/9/12 11:56 AM