Embed Size (px)
DESCRIPTION
Citation preview

Kenar D. Jhaveri, MDAssociate Prof of Medicine

Potential compartments of drug induced injury

Why is the Kidney Vulnerable to Chemotherapy?
• Patient Specific Factors• Kidney Specific Factors• Drug Specific Factors

Kidney Pathology 101
GlomeruliTubulesInterstitiumVasculature


Outline
Older agents known to be nephrotoxic
CisplatinumMethotrexateGemcitabineCalcineurin InhibitorsBisphosphanatesTyrosine Kinase Inhibitors Anti VEGF agents

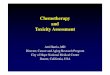
CASE 1• Mr. Fos is a 68 Y old male with un-resectable retroperitoneal seminoma
pre-treated with cisplatin 6 months ago with baseline SCr. of 1.3mg/dL and bland urine now presents with AKI after Drug X one dose of daily 2000mg/m2x3d and 2 doses 330mg/m2x2. Pt also received two concomitant doses of carboplatin (AUC of 7 daily for 3days). Post-treatment pt developed rising SCr; glucosuria, proteinuria, hypokalemia, metabolic acidosis and hypophosphatemia. Despite d/c of Drug X pt’s renal insufficiency progressed and he required dialysis 10 months after last dose of Drug X but remains NED from seminoma
• WHAT IS “DRUG X”?

H L
0.0
2.5
5.0
7.5
10.0
12.5
Jan 2009 Apr Jul Oct
Creatin ine
mg
/d
l
FERATOVIC, SABAN
Creatinine (mg/dl)
H L
0.0
2.5
5.0
7.5
10.0
12.5
Jan 2009 Apr Jul Oct
Creatin ine
mg
/d
l
FERATOVIC, SABAN
Creatinine (mg/dl)

IFOSFAMIDE NEPHROTOXICITY
Alkylating agent Proximal dysfunction-Fanconi Syndrome Most Data in children
– Tubulopathy-30% – Clinically significant Fanconi syndrome-5%
• Glucosuria with normal blood glucose levels• Hypophosphatemia, hypokalemia, metabolic acidosis,
hypouricemia, aminoaciduria AKI-usually resolves prior to next course Chronic renal disease
– Up to 50% suffer some degree of impairment– Average decline in GFR 35ml/min/1.73m2 (51Cr-EDTA)– Progressive even after IFOS stoppedSkinner R., et al. British Journal of Cancer (2000) 82(10): 1635-Skinner R., et al. British Journal of Cancer (2000) 82(10): 1635-16451645

IFOSFAMIDE NEPHROTOXICITY:RISK FACTORS
Cumulative dose >60-100gm/2 (*)
Age at treatment 3-5yrs (?)
Prior or concurrent treatment with cisplatin/carboplatin
H/o nephrectomy
Renal irradiation
Hydronephrosis
Jones D., et al. Pediatr Blood Cancer (2008); 51(6):724-731

LONG-TERM IFOSFAMIDE TOXICITY IN ADULTS Retrospective review 259 patient
▫Pts who received cisplatin were excluded
Decline in GFR correlated with ▫ Age (p<0.001)▫ Carboplatin exposure (p<0.001)
No Correlation with
▫ Ifosfamide dose-(?low overall dose)▫Aminoglycoside exposure▫Auto BMT
Mean GFR decline vs. ifosfamide dose quartiles
Latcha S., Flombaum CD. Personal communication, MSKCCLatcha S., Flombaum CD. Personal communication, MSKCC

Case 2Mr. Kohl Farabean is a 48 year old with AML who presented to the hospital with fever and headaches for one week. His neutropenic fever was treated with intravenous vancomycin, cefepime and voriconazole and oral acyclovir. There was no prior kidney disease and on admission the serum creatinine was 1.15 mg/dL with good urine output. On hospital day 9 re-induction therapy with “Drug Z” 30 mg/m2 intravenous(IV) daily days 1 to 5 (his first exposure to this drug) and “Drug Y “(he had previously been treated with this agent) 2 g/m2 IV daily days 1 to 5 two hours after “Drug Z” was initiated. On hospital day 11, AKI was detected with rise in serum creatinine from 0.97 mg/dL prior to initiation of chemotherapy on day 9 to 2.14 mg/dL on day 11. Urine output decreased and he became anuric on day 11. There was no laboratory evidence of tumor lysis syndrome. Later on hospital day 11 the serum creatinine increased to 3.56 mg/dL. Hemodialysis was started on hospital day 12 due to worsening azotemia and anuria.

Clofarabine induced renal disease
• Drug Z = clofarabine• Drug Y = cytarabine
Jhaveri KD, Chidella S, Allen S, Fishbane S. Clofarabine induced kidney disease. J Onco Pharm Pract 2013 in press

Literature review
Type study % patients with renal insult
Renal injury grade Other
Case report – 1 patient 1 Proteinuria, Aki No biopsy ( reversible)
Phase trials( AML)-112 adults patients
36% rise in creatinine Grade 3( 6%) No biopsy
Phase trials(AML)- 106 adults patients
14-16% Grade 4 No biopsy
FAERS database ( our review)
29 patients reported No grade reported No biopsy
Kintzel PE, Visser JA, Campbell AD. Clofarabine-associated acute kidney injury and proteinuria. Pharmacotherapy. 2011 Sep;31(9):923. Kantarjian H et al;. J Clin Oncol. 2010 Feb 1;28(4):549-55Burnett AK et al. J Clin Oncol, 2010 May 10;28(14):2389-95http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Surveillance/AdverseDrugEffects/default.htm accessed January 23, 2013

Mechanism?
• No biopsies till date• Tubular vs. glomerular vs. endothelial damage• Clofarabine inhibits DNA synthesis and is also a ribonucleotide reductase (RNR) inhibitor • RNR is an enzyme that catalyzes the formation of deoxyribonucleotides from ribonucleotides
which in turn facilitates DNA synthesis. • Depleting RNR could result in kidney injury??• Powell et al studied a knockout model of mice with no functional RNR. The animals died early
at 6 weeks of age. Interestingly, there was progressive podocyte damage and significant foot process effacement. In the few mice that survived beyond 9 weeks, collapsing glomerulopathy with widespread avascular glomeruli was noted
Powell DR et a;l. Rapid development of glomerular injury and renal failure in mice lacking p53R2. Pediatr Nephrol. 2005
Mar;20(3):432-40.

Case 3Mr. Kia Prol is a 68-year-old man with IgG κ-type refractory multiple myeloma presented to the hospital with fever and acute-on-chronic kidney disease (creatinine 3.65 mg/dL, baseline 1.6 mg/dL). He had been switched to carfilzomib and steroids 1 month prior to presentation because his disease had failed to respond to bortezomib and thalidomide, and had received 1 cycle of carfilzomib and dexamethasone 9 days prior to presentation. During the hospital course, his creatinine peaked at 4.59 mg/dL
Prior to administration of carfilzomib, his free κ:λ ratio was 78. His renal function worsened as the κ:λ ratio decreased to 16.8. His serum calcium was in the range of 8.5 to 9.0 mg/dL. His uric acid was normal. Urinalysis revealed a urine pH of 6, specific gravity of 1.009, mild glucosuria, small amount of blood, 75 mg/dL of protein, 2 to 5 white blood cells per high power field, and 0 to 2 red blood cells per by high power field. No granular, red blood cell, or white blood cell casts were noted. His proteinuria was unchanged, at 1.6 g per 24 hours.

Initial phase 2 trials: Increased serum creatinine was the most frequently reported renal adverse event , affecting 25% of the 266 patients in this study.
Acute kidney injury was reported in 13 patients (5%), 9 of whom experienced serious grade 3 acute renal failure. Chronic renal failure was reported in 10 patients (3.8%), with 3 of these events considered severe and 2 resulting in discontinuation of carfilzomib.
Siegel DS et al, Blood 2012

But does it really exist?-counter evidence
• Badros et al- the pharmacokinetics and safety of carfilzomib among MM patients in predefined cohorts identified by various degrees of renal function . The researchers studied 50 patients who had disease progression after 2 or more prior lines of therapy, and observed no differences between patients with and without normal renal function in carfilzomib clearance and exposure.
•Harvey et al - analysis of renal dysfunction in 526 patients treated with single-agent carfilzomib in 4 phase 2 trials. The analysis showed that overall, 87% of patients did not have worsening renal function during treatment. Of the patients who experienced worsening of renal function, 46% experienced transient worsening of a median duration of 1.4 weeks, and 54% experienced non transient worsening. A total of 8 of the 37 patients with non transient worsening discontinued carfilzomib treatment owing to an adverse event related to renal dysfunction
Badros AZ et al. Leukemia 2013Harvey D et al. Haematologica 2012

Pre renal insult?
Personal communication, Dr R. Niesvizky and Dr.R Wanchoo

Case 4Mr. Rapa Moin is a 76 year old was admitted for acute renal failure. He had a history of hypertensive chronic kidney disease (basal serum creatinine level 2.27 mg/dl). A mantle cell lymphoma diagnosed on February 2009 was treated by chemotherapy (rituximab , adriamycin, bortezomib, and dexamethazone, six cycles) replaced by rituximab, dexamethasone, oxaliplatin, and citarabin in August 2010.Temsirolimus as maintenance therapy was introduced in January 2011. The serum creatinine level was 2.78 mg/dl) and rises to 4.61 mg/dl 1 month later. On admission, after 5 weeks of temsirolimus, his blood pressure was 180/90 mmHg. Laboratory studies revealed a serum creatinine level of 5.5 mg/dl, blood urea of 34 mmol/l, a hemoglobin of 8.6 g/dl and platelets count of 27.000/mm3. Urinalysis revealed a daily protein excretion of 3 g and red 20 red cell per high-power field. Haptoglobin was low. Renal sonography finding was normal. Immunological tests were negative. The patient required iterative hemodialysis.
• Kidney biopsy showed?

Huh?

mTOR inhibitors and renal toxicities
• Proteinuria and TMA( you know this) from Renal transplantation literature• Sirolimus and everolimus have been reported to cause FSGS, collapsing FSGS and
TMA and other proteinuric diseases.• New reports of these agents causing ATN
• mTOR activity is low or absent in the normal kidney, but increased markedly after ischemic injury. Additionally, inhibition of mTOR delays renal recovery and repair. This begs the question of whether mTOR inhibition is the true cause of the renal dysfunction or this is an indirect effect, in not allowing renal tissue repair in response to nephrotoxic stress.
Izzadine H et al. Acute tubular necrosis associated with mTOR inhibitor therapy: a real entity biopsy-proven. Ann Oncol 2013

Case 5• Mr. Don Rubinson is a 44-year-old white male diagnosed in September
2010 with peripheral T-cell lymphoma, His renal function was normal. He received two cycles of standard cyclophosphamide/daunomycin/vincristine/prednisone (standard CHOP chemotherapy).
• Approximately 11 weeks after starting therapy, Creatinine was 3.6 mg/dL (319 µmol/L Antinuclear (ANA), hepatitis C and human immunodeficiency virus (HIV) antibodies, and hepatitis B surface antigen (HbsAgHBsAg) were negative. 24-hour hr urine collection contained 10g of protein with 1+ blood. A renal biopsy was performed.

Anthracyclines and kidney diseases
Mohammed N et al. Am J Kidney Dis 2013

Glomerular lesions caused by chemotherapy
Jhaveri KD , Shah HH et al. Glomerular Diseases seen with cancer and chemotherapy, Kidney Int 2013.

Watch out kidney, chemo is here!