Embed Size (px)
DESCRIPTION
Citation preview

CNS Infection
2011-2012Dr.Ali O. Saadoon
Neurosurgeon

Brain Death

Brain abscess
• 8% of all intracranial space-occupying lesions • %2 (most industrialized nations)

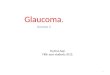
Axial computerised tomography scan with contrast of apatient with frontal sinusitis and epilepsy, showing a hypodense area ofcerebritis in the left frontal region.
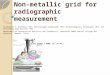
Axial computerised tomography scan with contrast ofthe same patient , but 2 weeks later. A ring-enhancinglesion has developed, typical of a pyogenic abscess.

The microorganism may reach the brain by different mechanisms:
• Direct spread from a contiguous site of infection (infected sinus)
• Hematogenous spread from remote reservoir of infection( RT-LT cardiac shunts)
• Direct inoculation from penetrating trauma or during neurosurgical procedures.
• In 20% of patients, no cause can be identified

The responsible microorganism
• Otitis media : anaerobic streptococci, Haemophilus and Gram-negative anaerobic
• Sinusitis: streptococcus milleri and staphylococcus • Traumatic: staphylococcus • Hematogenous spread : various organism are
involved

Clinical features
• features of raised intracranial pressure • Seizure• meningeal irritation • focal signs • rapid progression • Systemic features of infection are frequently
absent

Investigation
• leucocytosis, raised ESR, and C-reactive protein ( may initially be normal)
• CT and MRI: may show ring enhancing mass lesion (differ with the stage of the abscess)

Axial computerised tomography scan with contrast of apatient with frontal sinusitis and epilepsy, showing a hypodense area ofcerebritis in the left frontal region.
Axial computerised tomography scan with contrast ofthe same patient , but 2 weeks later. A ring-enhancinglesion has developed, typical of a pyogenic abscess.

Treatment
• identify the bacterial organism• IV antibiotics, 6-8 wks• Steroid ?• surgery A. drain or B. excision • Treat the cause• Anticonvulsant therapy

Surgical treatment
A. Needle aspiration : may be performed under local anesthesia if necessary, may be the only surgical treatment required but some time must be followed with excision, recommended with multiple or deep lesion, or with thin walled
B. Surgical excision: abscess is removed as any well-encapsulated tumor; the length of time on antibiotics can be shortened.

• before aspiration • After aspiration

subdural empyemas
• uncommon • sinusitis or mastoiditis • these patients are systemically unwell • with rapidly progressive neurological signs • a depressed level of consciousness and
hemiparesis • Epilepsy


Treatment
as for an intracranial abscess, complications include refractory status epilepticus and cortical venous sinus thrombosis

Posttraumatic meningitis
• Occurs in 1-20% of patients with moderate to severe head injuries
• 75% of cases have basal skull fracture and 58% had CSF rhinorrhea.

Treatment
• Conservative treatment: antibiotics are used according to the culture and sensitivity tests. There is high rate of infection with organisms indigenous to the nasal cavity
• surgical treatment : repair of the dural tear .

Osteomyelitis of the skull
• The skull is very resistant to osteomyelitis, • hematogenous infection is rare.• usually due to infected air sinus, penetrating
trauma or from scalp abscess

Treatment
• Antibiotics alone are rarely curative.• Treatment is usually surgical• debridement of infected skull (craniectomy) .• and 6-12 weeks of antibiotics. • if no sings of infection a cranioplasty may be
performed after 6 months. Post-operative.

Spine infection
1. vertebral osteomyelitis(spondylitis)a. pyogenicb. nonpyogenic e.g. tuberculous spondylitis 2. epidural abscess3. discitis a. spontaneousb. post-operative

Spinal tuberculosis Pott's disease
More commone in third world countries. Is usually symptomatic for many months and affect more than one level.the most common levels involved are the lower thoracic and upper lumbar levels.
Has a predilection for vertebral body, sparing the posterior elements. Psoas abscess is common .
Definitive diagnosis required a biopsy (may be done percutaneously) to identify the acid fast bacilli. Good results may be obtained with either medical treatment or surgery.
Surgery is needed when definite cord compression is documented or for complication such as abscess or sinus formation.



Hydatid Cyst disease
• Caused by encysted larvae of the dog tapeworm Echinococcus granulosa
• CNS involvement occurs in only 3%• Primary cysts are usually solitary, secondary cysts
(e.g. from embolization from cardiac cysts that rupture or from iatrogenic rupture of cerebral cysts) are usually multiple.
• Presentation : ↑ ICP ,seizures , or focal deficit.• Treatment : surgical removal of intact cyst.







Cardiac death:Heartbeat and breathing stop
Brain Death ?

Brain death
• Brain death defined as total and irreversible loss of function of the cerebral hemispheres and the brainstem.
• The patient may continue to have some spinal reflex activity, which dose not rule out the patient brain death.
• If ventilation and circulation are maintained artificially, the heart, kidneys, and liver may continue to function for some hours or days, but after brainstem death has occurred usually the cardiac arrest will follow within 2 weeks.

Diagnosis of brain death
• The reversible causes of coma should be excluded a. like hypothermia (brain-stem reflexes disappear when the core
temperature drops below 28°C), b. The effects of many sedative and anesthetic agents can closely mimic
brain death shock c. Guillain–Barré syndromed. locked-in syndrome(the destruction of the base of the pons. The condition
is most often caused by an acute embolus to the basilar artery. The patient cannot move the limbs, expression, or swallow, but the upper rostral mesencephalic structures involved in voluntary blinking and vertical eye movements remain intact)
• A committee should perform the testes. The findings

The findings• no motor response to deep central pain• fixed pupils : absent light reflex• absent corneal reflex• absent oculocephalic reflex(doll's eyes)• absent oculovestibular reflex (cold water calorics) • no cough and gag reflex• no motor responses within the cranial nerve distribution can be elicited
by adequate stimulation of any somatic area. • no spontaneous respiration( disconnecting the patient from the
respirator to allow the Pco2 to rise to 60 mmHg)• EEG is not detect brainstem activity• brain arteriogram show total lack of cerebral blood flow• Transcranial Doppler ultrasonography.





Positron emission tomography (PET)

There is a clear difference between severe brain damage and brain death. The physician must understand this difference, because brain death means that life support is useless, and brain death is the principal requisite for the donation of organs for transplantation.
In adults, the chief causes of brain death are traumatic brain injury and subarachnoid hemorrhage.
In children, abuse is a more common cause than motor vehicle accidents or asphyxia.




Thanks.Questions ?