Embed Size (px)
DESCRIPTION
Neurological examination lecture http://www.asktheneurologist.com/Study-Neurology.html
Citation preview

Neurological Neurological examinationexamination
Submitted to Submitted to AskTheNeurologist.ComAskTheNeurologist.Com
in 2008in 2008http://www.asktheneurologist.com/Study-Neurology.htmlhttp://www.asktheneurologist.com/Study-Neurology.html

3 questions of neurological 3 questions of neurological diagnosisdiagnosis1)1) Is there a lesion ?Is there a lesion ?
- Presence of neurological abnormality- Presence of neurological abnormality2)2) Where is the lesion ?Where is the lesion ?
- Location of problem- Location of problem- Requires knowledge of neuroanatomy- Requires knowledge of neuroanatomy
3)3) What is the lesion ?What is the lesion ?

Why perform the Why perform the neurological examinationneurological examination1.1. Detect the presence of neurological Detect the presence of neurological
abnormalityabnormality2.2. Localise the abnormality within the Localise the abnormality within the
nervous system ( may later be nervous system ( may later be confirmed by investigations)confirmed by investigations)

Systematic approach to Systematic approach to weakness e.g. bilateral leg weakness e.g. bilateral leg weaknessweakness• MuscleMuscle• NMJNMJ• NerveNerve• Nerve rootsNerve roots• Spinal cord Spinal cord • BrainstemBrainstem• CerebrumCerebrum

Basic PlanBasic Plan• General examination ( vital signs etc)General examination ( vital signs etc)• Conscious stateConscious state• CognitionCognition• Meningeal signsMeningeal signs• Cranial nervesCranial nerves• MotorMotor• SensorySensory• CerebellumCerebellum• ExtrapyramidalExtrapyramidal

DON’T DO EVERYTHING!DON’T DO EVERYTHING!• Screening tests vs detailed testingScreening tests vs detailed testing• Problem orientated approachProblem orientated approach
– Screen all systemsScreen all systems– Concentrate on systems relevant to Concentrate on systems relevant to
complaintcomplaint– Formal cognitive testing may be skipped Formal cognitive testing may be skipped
if patient is cognitively intact during if patient is cognitively intact during history and problem seems unrelatedhistory and problem seems unrelated•E.g. foot-dropE.g. foot-drop

Conscious stateConscious stateGlasgow coma scaleGlasgow coma scale
•EyesEyes /4/4•VerbalVerbal /5/5•MotorMotor /6/6
Normal = 15Normal = 15Created to reflect measure of global brain functionCreated to reflect measure of global brain functionLimited value in neurological patientsLimited value in neurological patients
- Many processes selectively affect components - Many processes selectively affect components aboveabove
- e.g. aphasia in a fully “ conscious” patient- e.g. aphasia in a fully “ conscious” patient
Therefore best to record functions individuallyTherefore best to record functions individually

CognitionCognition• MMSE MMSE
– Score out of 30Score out of 30– Broad screening test of cognitive function Broad screening test of cognitive function
including attention, memory, languageincluding attention, memory, language– Good for diagnosing / monitoring certain Good for diagnosing / monitoring certain
types of dementia especially A.D.types of dementia especially A.D.– Other types of dementia / cognitive Other types of dementia / cognitive
problems require different testsproblems require different tests

Cognition 2Cognition 2• “ “ Frontal functions”Frontal functions”
– Attention & concentration ( digit span ) Attention & concentration ( digit span ) – Abstraction ( explain proverb )Abstraction ( explain proverb )– Judgment Judgment
• child lost in street..what would you do?child lost in street..what would you do?– Planning Planning
•How to plan a holidayHow to plan a holiday•Draw a clockDraw a clock

Cognition 3Cognition 3• Frontal release signsFrontal release signs
– Glabellar tapGlabellar tap– PoutingPouting– RootingRooting– SuckingSucking– GraspGrasp– Palmomental Palmomental

Other cognitive functionsOther cognitive functions• Neglect: Neglect:
– Failure to pay attention to area of spaceFailure to pay attention to area of space– Usually due to right parietal lesions Usually due to right parietal lesions
where neglect left-sided spacewhere neglect left-sided space• Praxis: Praxis:
– ability to perform learned actionability to perform learned action- e.g. dressing , combing hair- e.g. dressing , combing hair

Meningeal signsMeningeal signs• Neck stiffnessNeck stiffness• BrudzinskiBrudzinski• KernigKernig
– Most frequently found in patients with Most frequently found in patients with meningitis or SAHmeningitis or SAH

Cranial nerves (a)Cranial nerves (a)• I I - smell- smell• II II - Acuity ( Snellen chart)- Acuity ( Snellen chart)
- FundiFundi- Fields ( confrontation)Fields ( confrontation)- Pupil resting state and reaction to lightPupil resting state and reaction to light
- DirectDirect- ConsensualConsensual- Swinging flashlight testSwinging flashlight test
- Pupil reaction to accommodation Pupil reaction to accommodation

Cranial Nerves (b)Cranial Nerves (b)• III, IV, VIIII, IV, VI
– Ptosis?Ptosis?– Pupils (already examined)Pupils (already examined)– Movement ( H and X)Movement ( H and X)– Saccades and smooth pursuitSaccades and smooth pursuit– ? Diplopia? Diplopia– ? Nystagmus? Nystagmus

Cranial nerves (c) Cranial nerves (c) • VV
– Facial sensationFacial sensation– Muscles of masticationMuscles of mastication– Jaw jerkJaw jerk– Corneal reflex Corneal reflex
•Afferent = VAfferent = V•Efferent = VIIEfferent = VII

• VIIVII– Muscles of facial expressionMuscles of facial expression– Taste ant 2/3 tongueTaste ant 2/3 tongue– Tensor Tympani Tensor Tympani
Cranial nerves (d)Cranial nerves (d)

Cranial nerves (e)Cranial nerves (e)• VIIIVIII
– Nystagmus already notedNystagmus already noted– HearingHearing
• IX, XIX, X– Say ahh (X)Say ahh (X)– Gag reflex Gag reflex
•Afferent = IXAfferent = IX•Efferent = XEfferent = X

Cranial nerves (f)Cranial nerves (f)• XIXI
– sternocleidomastoid & trapeziussternocleidomastoid & trapezius
• XII ( tongue motor examination)XII ( tongue motor examination)– Observation ( atrophy, fasciculations)Observation ( atrophy, fasciculations)– Midline protrusion ( ? Deviation)Midline protrusion ( ? Deviation)– Power Power – Dexterity ( fast movement side-to-side)Dexterity ( fast movement side-to-side)

Upper motor neuron Upper motor neuron
• Cell body within motor cortex Cell body within motor cortex (prefrontal gyrus)(prefrontal gyrus)
• Axon terminates :Axon terminates :– Cranial nerve motor nucleus Cranial nerve motor nucleus
•““corticobulbar”corticobulbar”– Anterior horn of spinal cordAnterior horn of spinal cord
• “ “corticospinal”corticospinal”

Lower Motor NeuronLower Motor Neuron• Cell body of Cell body of
– Motor cranial nerve nucleusMotor cranial nerve nucleus– Anterior horn cellAnterior horn cell
• Axon terminatesAxon terminates– Motor end plate ( skeletal muscle)Motor end plate ( skeletal muscle)
•AKA Neuromuscular junction ( NMJ)AKA Neuromuscular junction ( NMJ)

Upper Motor Upper Motor NeuronNeuron
Lower Motor Lower Motor NeuronNeuron
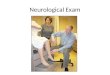
Inspection of Inspection of musclesmuscles
NormalNormal(disuse (disuse atrophy)atrophy)
AtrophyAtrophyFasciculatioFasciculationsns
ToneTone Increased Increased (unless acute)(unless acute)
DecreasedDecreased(or normal)(or normal)
Power (MRC Power (MRC scale) scale) 0-5 /5 0-5 /5
decreaseddecreased decreaseddecreased
Tendon ReflexesTendon Reflexes IncreasedIncreased(unless acute)(unless acute)
Decreased Decreased or Normalor Normal
Pathological Pathological reflexesreflexes
PresentPresent AbsentAbsent

Sensory SystemSensory System• ModalitiesModalities
– PainPain– TemperatureTemperature
– VibrationVibration– ProprioceptionProprioception
Spinothalamic
Post. columns

Sensory examination IISensory examination II• Problem orientated approachProblem orientated approach
– Left vs RightLeft vs Right– Spinal sensory levelSpinal sensory level– Radicular / dermatomalRadicular / dermatomal– Nerve distributionNerve distribution– Distal vs ProximalDistal vs Proximal

Which method would you Which method would you concentrate on?concentrate on?1.1. Sudden onset of dysphasia and Sudden onset of dysphasia and
right sided weaknessright sided weakness2.2. Numbness and paraesthesia in feet Numbness and paraesthesia in feet
with absent ankle jerkswith absent ankle jerks3.3. Acute bilateral leg weakness with Acute bilateral leg weakness with
loss of sphincter controlloss of sphincter control4.4. Drop footDrop foot

Symptoms and signs of Symptoms and signs of cerebellar disease cerebellar disease (VANISH’D)(VANISH’D)• VertigoVertigo• Ataxia - usually falls towards lesionAtaxia - usually falls towards lesion• Nystagmus – increased with gaze towards Nystagmus – increased with gaze towards
lesionlesion• Intention TremorIntention Tremor• Scanning speechScanning speech• HypotoniaHypotonia• Dysdiadochokinesia + DysmetriaDysdiadochokinesia + Dysmetria

Stability and GaitStability and Gait• Check ability to stand straight with eyes openCheck ability to stand straight with eyes open• Check ability to stand straight with eyes Check ability to stand straight with eyes
closedclosed– If significantly worse than with eyes open = If significantly worse than with eyes open =
positive Romberg signpositive Romberg sign– Usually signifies defect in pathways involved in Usually signifies defect in pathways involved in
proprioceptionproprioception– May signify vestibular diseaseMay signify vestibular disease
• Check gaitCheck gait

Extrapyramidal “ TRAP”Extrapyramidal “ TRAP”• Tremor ( rest, pill-rolling)Tremor ( rest, pill-rolling)• Rigidity ( lead-pipe, cog-wheel)Rigidity ( lead-pipe, cog-wheel)• Akinesia / bradykinesiaAkinesia / bradykinesia• Postural instabilityPostural instability

Normal examinationNormal examination
• Patient fully conscious, orientated in Patient fully conscious, orientated in time and place with no meningeal signstime and place with no meningeal signs
• PEARLA, Fundi intact, ( acuity and visual PEARLA, Fundi intact, ( acuity and visual fields intact)fields intact)
• Eye movements normalEye movements normal• Facial sensation normalFacial sensation normal• Face symmetricalFace symmetrical• (Hearing normal)(Hearing normal)• Palate / uvula rises symmetricallyPalate / uvula rises symmetrically• Gag preserved bilaterallyGag preserved bilaterally• Tongue centralTongue central

Normal examination 2Normal examination 2• No atrophy / fasciculations No atrophy / fasciculations
– (muscle inspection)(muscle inspection)• Tone preservedTone preserved• Power 5/5 in all 4 limbsPower 5/5 in all 4 limbs• Reflexes symmetricalReflexes symmetrical• No pyramidal signsNo pyramidal signs

Normal examination 3Normal examination 3• Sensation preservedSensation preserved• No cerebellar signsNo cerebellar signs• Romberg negativeRomberg negative• Gait normalGait normal

How to presentHow to present• Keep to orderKeep to order• Mention all abnormalitiesMention all abnormalities• Include “ core” points ( just described)Include “ core” points ( just described)• Mention all “ important negative points”Mention all “ important negative points”
– Leg weakness… “no sensory level”Leg weakness… “no sensory level”– History of MS with optic neuritis… “ no RAPD”History of MS with optic neuritis… “ no RAPD”– Complains of difficulty chewingComplains of difficulty chewing
•Mention power of masticatory musclesMention power of masticatory muscles