Embed Size (px)
DESCRIPTION
Proof version: Bishop, D., & Rutter, M. (2008). Neurodevelopmental disorders: conceptual approaches. In M. Rutter, D. Bishop, D. Pine, S. Scott, J. Stevenson, E. Taylor & A. Thapar (Eds.), Rutter's Child and Adolescent Psychiatry (pp. 32-41). Oxford: Blackwell.
Citation preview

32
From the beginnings of psychiatric classifications, there havebeen attempts to establish broad overarching groups (seechapter 2). Thus, for many years, mental disorders tended tobe put into the two broad categories of “organic” and “func-tional” disorders. The rationale was that, with respect to causation, the disorders within each group had more in com-mon with other disorders in the same group than with thosein the alternative group. The implication was that it might be useful for research into causal processes to determine com-monalities within these broad groups, rather than to assumethat each diagnostic category would have a unique cause notshared by all other conditions.
One such broad grouping was the notion of “minimalbrain dysfunction” (MBD) which was popular in the 1960sand 1970s (Wender, 1971). The concept has been discredited(Rutter, 1982) and is no longer in general use. The crucial flawswere that particular behaviors could not be used to infer brainpathology, and that organic brain dysfunction did not lead to a homogeneous psychopathologic pattern. In addition, itseemed to presuppose that all types of brain dysfunctionwould have similar consequences. It is clear that is not so. Theproblem with this broad grouping is that it arose from a theoretical notion for which there was no good empirical sup-port. The question that we consider in this chapter is whetherthe concept of neurodevelopmental disorders fares any betteras a guide to the future. Our focus here is on conceptual issuesin the characterization and classification of disorders, ratherthan on aspects of clinical management, which are dealt within the chapters on individual disorders.
What Do We Mean byNeurodevelopmental Disorders?
Over the last two decades or so, there has been increasing use of this concept. However, there are at least four ratherdifferent ways in which the term has been used. The narrowestconcept is provided by the second axis of the ICD-10 classifica-tion (World Health Organization, 1996), dealing with SpecificDisorders of Psychological Development. They were placed on
a separate axis because they differed from the general run ofpsychopathologic conditions in three key respects:1 An onset that is invariably during infancy or childhood;2 An impairment or delay in the development of functions that are strongly related to biologic maturation of the centralnervous system; and3 A steady course that does not involve the remissions and relapses that tend to be characteristic of many mental disorders.The overall description of this group of disorders noted thatthere is impairment in some aspect of mental development,but the impairment tends to lessen as the children grow older;despite this, deficits tend to continue into adult life; most of the conditions are more common in males than females; and a family history of similar or related disorders is com-mon, suggesting that genetic factors have an important role in the etiology. The subclassification within this axis com-prised disorders involving language development, scholasticskills or motor function. DSM-IV (American PsychiatricAssociation, 2000) has a broadly comparable subclassifica-tion but the disorders are not placed on a separate axis andthe overall conceptualization for grouping is not expressed so explicitly.
An alternative usage extends the term “neurodevelopmen-tal disorders” much more broadly to include single-gene dis-orders such as Williams syndrome or Prader–Willi syndrome(Tager-Flusberg, 1999) or disorders deriving from prenatalinsults or toxins, such as fetal alcohol syndrome (Harris,1995). These conditions develop on the basis of neuralimpairment, involve cognitive deficits of various kinds, and,as with the specific disorders of psychologic development, arecharacterized by a steady course without remissions orrelapses. However, whereas the Axis 2 ICD-10 disorders aredefined in terms of a profile of specific impairment of linguistic,scholastic or motor skills, these disorders are defined in termsof etiology. Although it can sometimes be fruitful to comparethe deficits associated with a particular known etiology andthose in a specific developmental disorder, it is potentially confusing to classify these different types of disorder together,and in this chapter we restrict consideration to those dis-orders with a putative multifactorial etiology. For similar reasons, we would argue against adopting a definition thatincludes mental retardation, cerebral palsy, traumatic braininjury and epilepsy under the rubric of neurodevelopmentalpsychiatric disorders.
Neurodevelopmental Disorders:Conceptual IssuesDorothy Bishop and Michael Rutter
3
Rutter’s Child and Adolescent Psychiatry, 5th edition. Edited by M.Rutter, D. Bishop, D. Pine, S. Scott, J. Stevenson, E. Taylor and A.Thapar. © 2008 Blackwell Publishing, ISBN: 978-1-4051-4592-3.
9781405145923_4_003.qxd 3/07/2007 15:06 Page 32
UNCO
RREC
TED
PROOF

There are two more modest ways in which the concept of neurodevelopmental disorder can be broadened beyondspecific disorders of psychologic development. First, many people include both autism spectrum disorders (ASD) and atten-tion deficit/hyperactivity disorders (ADHD) in the overallgrouping of neurodevelopmental disorders. At first sight, it might be objected that there are several ways in which both of these are rather different. Thus, neither reflects astraightforward impairment in a development-based skill thatis closely related to biologic maturation. Also, both involvedeviant functioning (i.e., that which is not normal at any age)as much as impaired functioning (i.e., that which is normalin form but impaired in level). Nevertheless, the reason whythey have come to be grouped with neurodevelopmental dis-orders is that they share with the other disorders the facts thatthey are multifactorial in origin; are present from early life;tend to improve with increasing age but are also associatedwith disordered functioning that extends right into adult life;they involve a strong genetic influence; and both show a markedmale preponderance. Furthermore, they are characterized byneuropsychologic impairments, in aspects of executive func-tion in ADHD (see chapter 34), and in social cognition, central coherence and executive function in ASD (see chap-ter 46). Strikingly, epidemiologic and clinical studies have shownthat these two disorders often co-occur with the ICD-10 Axis2 disorders of psychologic development, and genetic findingshave similarly begun to point to a possible shared genetic liability (as well as a liability that is more syndrome specific;Grigorenko, submitted). In addition, although autism may beassociated with other forms of psychopathology that do showremission and relapses (Hutton, Goode, Murphy et al., in press)the basic disorder is persistent rather than recurrent. Muchthe same applies to ADHD (see chapter 34).
A further possible broadening of the concept of neurode-velopmental disorders brings in life-course-persistent anti-social behavior (Moffitt, 1993) and schizophrenia (Rapoport,Addington, & Frangou, 2005). At one time, both of these wouldhave been regarded as acquired disorders but there is now anabundance of evidence that schizophrenia is often associatedwith impairments in the development of both language andmotor function and with cognitive impairments that precedethe development of overt schizophrenia (see chapter 45).Similarly, unlike adolescence-limited antisocial behavior, thelife-course-persistent variety of antisocial behavior begins inthe preschool years and is associated with hyperactivity andimpairments in information processing and social cognition (seechapter 35). For the purposes of this chapter we have notincluded either of these disorders under the rubric of neuro-developmental disorders for two main reasons. First, both antisocial behavior and schizophrenia do show fluctuations in their manifestations that are more akin to the remissionsand relapses associated with the broad run of mental dis-orders than with the relatively steady state of the specific disorders of psychologic functions. Second, there is not the same evidence of a shared genetic liability. For these reasons,we prefer to conceptualize these as disorders that have their
origins in a neurodevelopmental abnormality rather than asa neurodevelopmental disorder as such, and confine the termneurodevelopmental to those disorders traditionally regardedas specific developmental disorders, plus ASD and ADHD.
Are the Neurodevelopmental DisordersDistinct Conditions?
Both traditional medical, and traditional psychologic, appro-aches have tended to operate with discrete diagnostic categories.Thus, reading disability continues to be conceptualized as“developmental dyslexia,” with the implication that it is a discrete neurologic condition (Démonet, Taylor, & Chaix,2004). For many years, specific language impairment wastermed developmental dysphasia (Zangwill, 1978) with the same kind of implication. This terminology has now gone out of fashion because of the recognition that impairments inlanguage development differed in important ways fromacquired disorders of language. In psychiatric classifications,both ASD and ADHD are treated as if they were conditionsthat were entirely separate from other disorders of psychologicdevelopment. In line with this conceptualization, cognitive psychologists have looked for a single specific underlyingdeficit that is responsible for each disorder, the nature of thedeficit differing for each one (Morton & Frith, 1995).
There are two main reasons for challenging this view of neuro-developmental disorders as a set of independent conditions.First, there is substantial co-occurrence among them. Second,both etiologic and psychologic studies indicate that multipledeficit models are more consistent with the multifactorial andprobabilistic etiology of such disorders (Pennington, 2006), and that significant developmental impairment may arise onlywhen there is more than one risk factor present (Bishop, 2006).As in internal medicine, the same pathologic endpoint can arise through multiple, rather different, causal pathways (cf.Rutter, 1997). In the following sections, we present evidenceto support the case that rather than looking for the cause of each type of neurodevelopmental disorder, we need to takeaccount of the commonalities among them, and develop morecomplex models that can explain the patterns of associationand dissociation among deficits.
Commonalities Among DevelopmentalDisorders
Research findings across the whole of psychopathology, bothin childhood and adult life, have been consistent in showingthe high frequency with which individuals have multiple, sup-posedly separate, disorders (Angold, Costello, & Erkanli, 1999;Caron & Rutter, 1991). This is strikingly apparent for the neurodevelopmental disorders – indeed, it has been argued thata pure disorder is the exception rather than the rule (Gilger& Kaplan, 2001; Kaplan, Dewey, Crawford et al., 2001) –and is reflected in the ICD-10 category of mixed developmental
NEURODEVELOPMENTAL DISORDERS
33
!
@#
9781405145923_4_003.qxd 3/07/2007 15:06 Page 33
UNCO
RREC
TED
PROOF

disorders. Thus, there is considerable overlap between specificreading disability (SRD) and specific language impairment (SLI) (Bishop & Snowling, 2004; Eisenmajer, Ross, & Pratt,2005), between SRD and ADHD (Dykman & Ackerman, 1991;Willcutt & Pennington, 2000) and between SLI and ADHD(Beitchman et al., 1996). Less work has been carried out ondevelopmental coordination disorders (DCD), but there isevidence for an overlap between motor impairment and bothSLI (Hill, 2001) and ADHD (Kadesjö & Gillberg, 1998). Asfar as autistic disorder is concerned, the defining criteria disallow a diagnosis of SLI in a child meeting criteria for autistic disorder, but it is clear that at the symptomatic levelthere is considerable overlap, with many affected children showing the kinds of structural language deficits that charac-terize SLI (Tager-Flusberg & Joseph, 2003). Furthermore,many children with SLI or ADHD show in milder form thekinds of social/pragmatic impairments that are characteristicof autistic disorder (Bishop & Norbury, 2002; Clark, Feehan,Tinline et al., 1999; Farmer, 2000; Geurts et al., 2004). SRDco-occurs with mathematical difficulties at a higher level thanpredicted from the prevalence of either disorder on its own(Lewis, Hitch, & Walker, 1994).
It has become accepted to refer to these patterns of co-occurrence as “comorbidity,” but this is misleading becauseit ignores the possibility that much of the supposed com-orbidity is simply a function of the invalid, and artificial, diagnostic subdivisions in classification systems (see chap-ter 2). Thus, for example, it seems likely that much of the co-occurrence of supposedly different anxiety disorders issimply a consequence of these disorders being slightly differ-ent manifestations of the same underlying condition (seechapter 39). Might the same apply to neurodevelopmental disorders? Clearly it could.
Thus, SLI and reading disability both comprise disorders of language – the former with respect to spoken language and the latter with respect to written language. It would berather surprising if there was no co-occurrence between thetwo. That is not to argue that all cases of reading disabilityderive from oral language impairment, because manifestlythey do not (Bishop & Snowling, 2004); but it is to suggestthat co-occurrence of some degree is to be expected.
However, the co-occurrence of neurodevelopmental dis-orders does not apply only to language-related disorders; asnoted above, there are also overlaps between language andmotor impairments, attention deficit and social deficits, andthese cannot readily be explained as different manifestationsof a common cognitive disability. To some extent, overlapscould reflect referral bias in clinical samples: for instance, achild whose reading or language disability is accompanied bysocial impairment or attentional deficit would be more likelyto referred to a psychiatrist than one who had an isolatedimpairment. However, this cannot be the whole explanation,because overlaps are seen in epidemiologic samples (e.g.,Beitchman et al., 1996), and second, the rates of co-occurrenceare higher than would be predicted from knowledge of thefrequency of individual disorders.
A “Syndrome” of NeurodevelopmentalDisorder?
One might start to wonder if, rather than differentiatingbetween neurodevelopmental disorders, it would make moresense to group them all together into an overarching category,treating them as variant forms of a common underlying disorder. However, there are sufficient differences among theneurodevelopmental disorders to preclude such a conceptual-ization. First, molecular genetic studies have been successfulin identifying chromosomal regions associated with risk forreading disability, SLI, ADHD and ASD, but there has beenlittle or no overlap between the linkages reported for thesedifferent disorders. For instance, Fisher (2006) noted thatwhereas linkages to dyslexia have been found on chromosomes1, 2, 3, 6, 15 and 18, those to SLI have been found on chro-mosomes 13, 16 and 19. Fisher pointed out that we need tobe careful in interpreting such findings: it would be danger-ous to assume that there are highly specific pathways fromgenotype to phenotype, especially because few studies have used multivariate methods to look at more than one disorderat a time. Undoubtedly there are some genes whose effects are common to more than one neurodevelopmental disorder(e.g., Willcutt et al., 2002), but behavior genetic studies alsousually find evidence for specific as well as common geneticinfluences on co-occurring disorders (e.g., Martin, Piek, & Hay,2006). Second, there are differences among disorders in drugresponse. It is striking, for example, that whereas ADHD showsa marked beneficial response to stimulant medication (see chapter 34), no drugs have other than a slight inconsistent effecton the basic problems associated with ASD (see chapter 46).Similarly, although medication may provide some symp-tomatic improvement with the other neurodevelopmental disorders, there are not the marked benefits that are seen withADHD. Third, although it is difficult to compare acrossimaging studies because of variations in the ways in which theyhave been conducted (Peterson, 2003), patterns in the vari-ous neurodevelopmental disorders do not seem at all closelysimilar: for instance, fronto-striatal systems are implicated inADHD (see chapter 34), whereas in dyslexia there is reducedactivation in left temporo-parietal cortex (see chapter 48).Fourth, at a behavioral level, there are differences among neurodevelopmental disorders in short and long-term course(Rutter, Kim-Cohen, & Maughan, 2006a). Finally, althoughmost neurodevelopmental disorders are characterized by a preponderance of males, sex ratios vary across disorders,with the male excess being far more striking for ASD than for other neurodevelopmental disorders (Rutter, Caspi, &Moffitt, 2003). Arithmetic difficulties stand out from the rest, with boys and girls equally likely to be affected (Lewiset al., 1994; Rourke, 1989; Shalev, Auerbach, Manor, & Gross-Tsur, 2000).
Clearly, it is not feasible to treat the whole gamut of neurodevelopmental disorders as a single condition, but can we nevertheless identify distinct syndromes within this category, in which a pattern of deficits arises from a common
CHAPTER 3
34
9781405145923_4_003.qxd 3/07/2007 15:06 Page 34
UNCO
RREC
TED
PROOF

neurobiologic cause? Rourke’s (1989) account of “non-verballearning disability” (NLD) is such a model: a distinctive pattern of strengths and weaknesses in sensorimotor skill,scholastic achievement, and socioemotional development areseen as all originating from destruction or dysfunction of whitematter in the right cerebral hemisphere. The deficits seen as characterizing NLD encompass specific arithmetical dis-order, DCD and Asperger syndrome. The construct of NLDexplains the co-occurrence of these deficits in terms of aspecific neurobiologic basis. However, the validity of the category is questionable. The different deficits certainly canand do co-occur, and the association of the symptomatologyof Asperger syndrome with the neuropsychologic manifesta-tions of NLD has been empirically demonstrated (Klin,Volkmar, Sparrow, et al., 1995). However, the associationappears too weak to justify treating it as a syndrome: this is demonstrated in studies showing that a high proportion ofchildren with a clinical picture of NLD do not show specificdeficits thought to characterize this disorder (Drummond,Ahmad, & Rourke, 2005; Pelletier, Ahmad, & Rourke,2001). If we embrace the construct of NLD, we end up inexcluding numerous cases because they do not show theanticipated combination of deficits, meaning that we either haveto dilute the “syndrome” to be too general to be useful, orwe have to devise additional categories to encompass the casesthat do not fit. Similar problems arise if we try to fit language,literacy and speech disorders into a broader syndrome; we canfind many children who show this constellation of impairments,but there are also many who do not (Bishop & Snowling, 2004;Pennington, 2006).
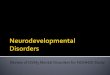
Neurodevelopmental disorders thus pose a considerablechallenge for a classification system. On the one hand, we needto explain why there is common co-occurrence of differentdeficits, while at the same time allowing for dissociationsbetween different types of deficit, and variable patterns of asso-ciated features. The causal model shown in Fig. 3.1 providesa framework for conceptualizing these questions. In thismodel, first put forward in the context of SLI and dyslexia,a neurodevelopmental disorder is identified on the basis of aconstellation of behaviors; these result from specific cognitivedeficits, which have particular neurobiologic bases, which arein turn affected by genetic or environmental factors. Whenextending the model to cover the whole gamut of neurode-velopmental disorder, the “cognitive” level is taken to includea wide range of underlying mental operations that cannot bedirectly observed, but are inferred from behavior, includingperceptual-motor skills, language, memory, social cognition,reasoning and executive functions. Relationships among thedifferent levels of functioning are not one-to-one, but involvecomplex multifactorial influences going from etiology to neu-robiology, from neurobiology to cognition, and from cogni-tion to behavior. Viewed from this perspective, it is clear thatoverlaps between observed behavioral impairments may arisefrom shared cognitive deficits, shared neurobiologic originsand/or shared etiology. We now turn to consider evidence forthese different causal mechanisms.
Causal Models of NeurodevelopmentalDisorders
Cognitive DeficitsOne goal of developmental neuropsychology is to uncover the underlying nature of deficits seen in neurodevelopmentaldisorders. As shown in Fig. 3.1, the same behavioral deficitmay arise for different reasons, and one would hope that asour conceptual understanding advances, we might be able tocategorize disorders not in terms of surface behavior, but in terms of underlying cognitive deficits. For instance, mostchildren with reading disability have difficulties with phono-logic analysis which are evident even when they are tested usingmethods that do not require any reading or writing (see chap-ter 48). Other poor readers have visual difficulties, problemslearning specific spellings of irregular words or poor com-prehension of written texts. A focus on underlying cognitivedeficits thus could help identify new subgroups. It also sug-gests that some of the existing distinctions among disordersmay be unrealistic; for instance, increasingly speech, languageand literacy problems are regarded as different manifestationsof a common phonologic impairment, whose behavioral correlates would vary depending on the age at which the childwas observed and the severity of the impairment (Bishop & Snowling, 2004). Nevertheless, if we try to categorize disorders in terms of underlying deficit rather than observedbehavior, this does not necessarily simplify our nosology,because multiple deficits are the rule rather than the excep-tion, at the cognitive as well as the behavioral level. Thus,although one can identify children who fit the picture of“phonologic dyslexia” or “surface dyslexia,” most poorreaders present a mixed picture (Snowling & Nation, 1997).
NEURODEVELOPMENTAL DISORDERS
35
gene1
gene2
gene3
env1
env2
beh1
beh2
beh3
beh4
env3
cog 1 cog 2 cog 3 cog 4
etiology
neurobiology
cognition
behavior
Fig. 3.1. Levels of causation for developmental disorders. Thedashed line emphasizes that children’s behavior (beh) can affect the environment (env) they experience. [From Bishop, D. V. M., & Snowling, M. J. (2004). Developmental dyslexia and specificlanguage impairment: Same or different? Psychological Bulletin,130, 858–886 with permission.]
9781405145923_4_003.qxd 3/07/2007 15:06 Page 35
UNCO
RREC
TED
PROOF

Even if one looks at impairments in very different domains,associated disorders are common.
Pennington (2006) conducted a series of studies comparingchildren with pure dyslexia, pure ADHD, and comorbiddyslexia and ADHD. He was interested in the possibility thatcomorbidity among these disorders might reflect the influenceof one behavior on another (e.g., attentional difficulties mightarise because the child who could not read well became boredand distractible; or conversely, the child’s difficulty in attend-ing could lead to scholastic deficits). If the first account weretrue, then the comorbid children should resemble the puredyslexic cases in terms of underlying impairment. If the second account applied, then the comorbid children shouldresemble the pure ADHD cases. In fact, the pure dyslexia grouphad phonologic deficits, the ADHD group had inhibitiondeficits, but the comorbid group had evidence of both phono-logic and inhibition deficits. These results are consistent withconventional wisdom that links dyslexia to poor phonologyand ADHD to weak inhibition, but it leaves unexplained theco-occurrence of these two impairments.
We can summarize by saying that it was hoped that, by studying underlying impairments, we would obtain clearer dis-tinctions between disorders and find that apparent comorbiditywas a consequence of poor specification of disorders. In fact,studies such as this show that comorbidity is just as apparentat the level of cognitive impairment as it was at the level ofobserved behavior. This suggests we need to seek an explana-tion for the associations among neurodevelopmental disordersat a different causal level.
Neurobiologic BasesNeuropsychologic studies of adults highlight how fairlyspecific impairments in functions such as language, reading,arithmetic or motor programming can arise as a consequenceof a focal brain lesion (McCarthy & Warrington, 1990).When one sees analogous impairments in children, it istempting to assume a similar etiology via underlying brain damage, with the precise pattern of observed impairmentdepending on the extent, location and severity of the damage.This kind of model was put forward in the 1950s byPasamanick and colleagues, who proposed a “continuum ofreproductive casualty,” suggesting that whereas major neuro-logic insult resulting from birth trauma, intracranial hemor-rhage or anoxia can lead to clear signs of neurologic damagesuch as cerebral palsy or epilepsy, milder damage may leadto more subtle learning difficulties. However, this conceptu-alization of the etiology of neurodevelopmental disorders hasnot received much empirical support. There is good evidencethat such damage often gives rise to behavioral and cognitivesequelae (Pasamanick & Knobloch, 1966), but the suggestionthat neurodevelopmental disorders often arise from damageduring the obstetric process has not proved to be the case.Nichols and Chen (1980) found only weak associationsamong neurologic soft signs, hyperactivity and learning dis-orders, and even weaker associations between these variablesand perinatal complications.
Furthermore, the notion that “birth injury” was the mainrisk factor fell into disrepute in view of the evidence that manyof the risks supposedly associated with obstetric complica-tions actually derived from prenatal problems. A geneticallyabnormal fetus is more likely to have a low birth weight and to be born following premature gestation. That pro-bably accounts for the somewhat inconsistent associationbetween obstetric complications and ASD (Bolton et al.,1997). Undoubtedly, extremely low birth weight does lead toan increased rate of motor, language, scholastic and attentionaldifficulties (Marlow, 2004; Marlow et al., 2005). However,the association is not strong when assessed in the opposite direction (i.e., by starting with children with neurodevelop-mental disorders and studying their perinatal history). Withthe possible exception of developmental co-ordination dis-order (for review see Cermak, Gubbay, & Larkin, 2002), obstetric complications do not have a particularly importantassociation with any of the neurodevelopmental disorders. Itis family history that provides the key differentiator.
The Concept of Maturational LagGiven that neurodevelopmental disorders are, on the onehand, familial, and on the other hand, not caused by acquiredbrain lesions, we need to seek another causal mechanism atthe neurobiologic level. There is often an implicit assumptionthat genetic or other prenatal influences have led to some failure of neurodevelopment that leads to abnormality that isfunctionally equivalent to a focal brain lesion – hence the anal-ogous syndromes seen in neurodevelopmental disorders andadult acquired disorders (Temple, 1997). According to this view,the brain of a child with a neurodevelopmental disorder hasan underlying abnormality that persists through childhood. Analternative possibility is that these disorders are no more thanan extreme of the normal variation in the timing of develop-ment. We know that there are huge differences in the timingof puberty in both males and females, and marked differences,too, in the timing of the eruption of teeth. In similar fashion,there is marked individual variation in the timing of speechacquisition. When such a delay is followed by later normalfunctioning it may be regarded as a maturational lag of somekind. The implication is that the problem involves a normalvariation in the development of certain brain systems respons-ible for cognitive functioning, rather than in some abnormaldifference in brain systems, and that there can be a highly selective delay in the maturation of just one brain system.Associations between neurodevelopmental disorders wouldthen arise in cases where the maturational lag extended toencompass several brain regions, or where there is pluripo-tentiality (i.e., a given brain structure is involved in a rangeof cognitive functions; Noppeney, Friston, & Price, 2004).
A key prediction from the “lag” hypothesis is that not onlyshould the pattern of functioning resemble that of a normalyounger child but also, as the children with a neurodevelop-mental disorder get older, the main difference from normalfunctioning should be found for later-maturing functions and not for early-maturing functions (Bishop & Edmondson,
CHAPTER 3
36
9781405145923_4_003.qxd 3/07/2007 15:06 Page 36
UNCO
RREC
TED
PROOF

1987; Bishop & McArthur, 2004, 2005). The limited avail-able evidence is in keeping with that expectation and runsagainst the outmoded static lesion notion. However, for mostneurodevelopmental disorders, although there is a generaltendency for gains in function with increasing age, delayed earlydevelopment is not followed by later normal functioning(Rutter et al., 2006a). Can a maturational lag account haveany explanatory value in such cases?
Two main possible explanations, both speculative, have been proposed for why children with a neurodevelopmentaldisorder do not ultimately catch up. First, the persistence couldderive from what Stanovich (1986) termed a “Mattheweffect,” whereby the poor (poor readers) get poorer (make slowprogress), while the rich (good readers) get richer (make goodprogress) as a result of literacy experience boosting further language and literacy development. Furthermore, a poorreader may lack the necessary experiences later (i.e., readingis not usually taught in secondary schools, and such books asare available are likely to be too advanced to be intelligible).There could also be more indirect effects whereby early impair-ments create a negative spiral affecting other skills (e.g., theeffects on intimate social relationships of communicationdifficulties in early childhood). Because of the importance of experiences in the development of psychologic functions,there is little doubt that something of this kind could have a contributory role. What is much less certain is whether it could account for the severe problems in intimate social relationships in adult life found for many individuals with asevere receptive SLI in adult life reported by Clegg, Hollis,Mawhood et al. (2005) – because the relationship deficits were not a function of the severity of the earlier language deficits (at least in terms of those measured), and because the nature of the deficits appeared so different from those usually associated with social rejection. It is also noteworthythat persistence of disorder is often seen in young people withSLI who have been enrolled in special education throughoutthe secondary as well as primary school years (Conti-Ramsden,Botting, Simkin, et al., 2001; Haynes & Naidoo, 1991).Perhaps the key empirical finding is provided by Francis,Shaywitz, Stuebing, Shaywitz et al.’s (1996) individual growthcurves comparison of 69 children with a reading disability and334 children with no reading problem. Nine yearly longitud-inal assessments showed that both groups tended to plateauat about 13 years of age, with no narrowing or expansion ofthe gap between the group. They differed in level but not intrajectory. The finding rather runs counter to the Stanovich(1986) proposition.
A second kind of explanation for persistence of disorder wasproposed in the context of language and literacy deficits byWright and Zecker (2004). They invoked a decline in neuro-plasticity as a limiting factor, and suggested that neurobiologicevents at age 10 years associated with the onset of pubertyhalted auditory development at whatever level it has reached,so that the adolescent was left with a lasting residue ofdeficit. This viewpoint is consistent with evidence that thereare sensitive periods for aspects of language acquisition, so that
it is difficult to become fully competent in the phonology and syntax of a second language acquired after puberty(Mayberry & Lock, 2003; Oyama, 1976). However, criticalperiods for auditory development have not been demon-strated, and there is electrophysiologic evidence that devel-opment of the auditory system (Albrecht, von Suchodoletz, & Uwer, 2000) as well as of some other cortical systems con-tinues right up into adulthood (see chapter 12). Longitudinalstudies using magnetic resonance imaging (MRI) have con-firmed that brain development continues well after the onsetof puberty, with higher-order association areas maturing onlyafter lower-order somatosensory and visual areas (Gogtay et al., 2004; see also chapter 12), and that such changes – espe-cially in the frontal cortex – are associated with intellectualfunctions (Shaw et al., 2006a). There is considerable vari-ation from one cortical region to another, with some showingradical changes at puberty and others unaffected (Nelson et al., 2002). Clearly, further research is required in order toprovide an understanding of both brain development (and its functional consequences) in typically developing indi-viduals and in those with neurodevelopmental disorders. Asthe evidence currently stands, the postulate that the relevantbrain systems lose plasticity around the time of puberty remainshighly speculative, and to test it we would need studies thatcompare the impact of training on brain and behavior in pre- and postpubertal individuals. The trajectory findings ofFrancis et al. (1996) are compatible with the suggestion of achange in brain plasticity in adolescence but they provide nodirect support.
We may sum up by concluding that there is little hard evidence in support of a maturational lag account. We needmore longitudinal and neurobiologic studies to evaluate thisidea. In its favor, this kind of explanation has the potentialto highlight parallels between causal mechanisms in normaland impaired development, and to account for changingprofiles seen in neurodevelopmental disorders. It provides theimpetus for studies that track neurodevelopment over time:for instance, Shaw et al. (2006b) documented changes in cortical thickness over time in children with ADHD, with evid-ence of normalization in children who had a good outcome.However, a maturational account seems more plausible as anexplanation for transient delays early in development than forsevere and persistent neurodevelopmental disorders.
A final point to note is that it is important not to confusethe hypothesis of a developmental delay with the entirely different hypothesis that the causation of disorders of psy-chologic development, together with ASD and ADHD (as wellas numerous forms of other psychopathology), are based ondimensional genetic and environmental risk factors (Rutter,Moffitt, & Caspi, 2006b). With multifactorial disorders,dimensional liability is the rule rather than the exception. Thequestion of whether or not the dimensional risks are the sameones that apply within the normal distribution is a separateissue and it is one that has been very little investigated up to now, although there has been some relevant research in relation to ADHD (see chapters 23 and 34).
NEURODEVELOPMENTAL DISORDERS
37
9781405145923_4_003.qxd 3/07/2007 15:06 Page 37
UNCO
RREC
TED
PROOF

The Neuroconstructivist ApproachThe “maturational lag” account is not the only alternative to a “static lesion” model of neurodevelopmental disorders.We have become increasingly aware that the brain changes in the course of development, restructuring itself to form newneural systems, both in response to interactions betweenfunctional neuronal networks and in response to environmentalinput (see chapter 12). Karmiloff-Smith (1998) argued that one needs to take such evidence into account when devisingexplanations for neurodevelopmental disorders, and that anapparently specific deficit in a child may be the endpoint ofa process that started with a relatively non-specific disruptionto brain development. This “neuroconstructivist” approachemphasizes interactions between different neural systems, andto that extent would predict the existence of disorders affect-ing more than one domain of functioning. However, this the-oretical perspective is still very young; its main contributionto date has been to question the simple parallels that are some-times drawn between developmental and acquired disorders,and to emphasize the need to put development centre-stage.In order to make more specific predictions about neuro-developmental disorders and their co-occurrence, we need todevelop specific computational models of normal development,which then allow us to identify which perturbations could result in a particular profile of deficit (Thomas & Karmiloff-Smith, 2003).
Etiologic InfluencesFor those conditions where genetically informative designs havebeen applied (SRD, SLI, ADHD, ASD), there is evidence ofsubstantial genetic influences on the liability to disorder (seechapter 23). With respect to neurodevelopmental disorders(together with other multifactorial disorders), these probablyusually reflect the actions of normal variants of multiplegenes of small effect operating together with multiple envir-onmental influences (Gilger & Kaplan, 2001; Rutter et al.,2006b) rather than the determinative effect of major mutantgenes. This view of etiology is reflected in the causal modelin Fig. 3.1, in that there is no one-to-one relationship betweengenes and neurobiology. Rather, a specific neurologic systemis likely to be influenced by a range of etiologic influences andthe given etiology will impact on a range of brain regions. Sucha model allows for both co-occurrence of deficits and the existence of pure disorder. Particular patterns of variation may reflect the influence of either specific combinations ofgenetic or environmental factors, or the operation of chanceinfluences (Wolf, 1997).
This raises the question of whether patterns of co-occurrencebetween disorders indicate a shared liability. Klein and Riso(1993) noted that evidence for overlapping etiology of dis-orders can be found by looking at the familiality of disordersin pure and comorbid cases. In essence, they note that if shared etiology is implicated in causing disorders A and B, thenwe should see an increased risk for disorder B (with or with-out A) in relatives of a person with disorder A, and vice versa. Furthermore, relatives of comorbid cases should show
increased risk for the single disorders A and B, as well as forthe A + B combination. Note that these predictions are notmade by other models of comorbidity: for instance, if the A+ B combination represented a separate subtype of disorderwith distinct causes, then it should “breed true,” and thereshould be no increase in rates of disorder A in relatives of thosewith disorder B (or vice versa). Furthermore, the predictionshold up for any disorder that shows familiality, regardless of whether genes or shared environmental factors are moreimportant.
If the disorders are significantly heritable, it is possible togo further using either quantitative genetic methodologies(such as twin studies) or molecular genetic studies (focusingon individual identified genes) to determine how far there is a shared genetic influence between the two disorders. Fewresearchers to date have adopted this approach; an exceptionis work by Pennington (2006), who studied comorbidity ofSRD and ADHD in a twin sample and concluded that therewas evidence for shared genetic influence on the two dis-orders. In a similar vein, Bishop (2002) found evidence foroverlapping genetic influences on language impairment andmotor immaturity in a sample selected for SLI. Moleculargenetic findings also suggest that susceptibility extends beyondtraditional diagnostic boundaries (Rutter et al., 2006b).
Research Implications of theNeurodevelopmental Disorder Concept
Probably the single most crucial research implication is thatinvestigators need to consider the possibility that the causalinfluences on key features may extend across the range of neurodevelopmental disorders, rather than being specific to just one. Thus, it is striking that, with the exception of arith-metic difficulties, all the neurodevelopmental disorders showa marked male preponderance (Rutter et al., 2004). That standsin marked contrast to the finding that disorders with a markedfemale preponderance all concern syndromes typically begin-ning in adolescence and that involve emotional disturbance,rather than neurodevelopmental impairment, as the key feature. Baron-Cohen and Hammer (1997) have hypothesizedthat ASDs represent an “extreme male brain.” There is a lackof good supporting evidence but, in addition, it is necessaryto ask whether that same explanation should be held to applyto ADHD or SRD or SLI? It does not seem particularly likelythat the causes of the male preponderance are entirely differ-ent in the case of each of the syndromes, although there maybe syndrome-specific factors as part of the explanation.
A further question for research is whether studies shouldcontinue to be focused on “pure” disorders given that theydo not appear to be at all typical. The answer will depend onthe question that is being asked. Pure groups can be useful inidentifying correlates of a specific kind of deficit withoutadditional confounds. For instance, suppose one wants to testthe hypothesis that reading disability is caused by a low-levelauditory perceptual deficit. The goal is to compare a group
CHAPTER 3
38
9781405145923_4_003.qxd 3/07/2007 15:06 Page 38
UNCO
RREC
TED
PROOF

of children with SRD and a control group on a task in whichthey have to listen for small differences between sounds, andmake a manual response to indicate what they have heard. Ifthe sample includes children who have substantial difficultieswith language comprehension, motor dexterity or attentionalcontrol, then it may be hard to disentangle the influence ofthese impairments on task performance. Careful sample selec-tion to exclude such cases may give cleaner results. Havingsaid that, it is worth noting that those who claim to studypure cases may be including large numbers of children withadditional deficits which are missed because they are notassessed. For instance, many studies of SRD fail to assess children’s language or attentional skills. If a sufficientlydetailed assessment battery is used, covering the whole rangeof neurodevelopmental disorders, the numbers of pure casesavailable for study may become vanishingly small. If so, it maybe better to assess associated deficits, so that one can estab-lish how far they are associated with the dependent variableof interest, rather than try to control for their effects by exclu-sion of comorbid cases (cf. Breier et al., 2001).
In many research contexts, focus on pure groups is not just hard to achieve, it can be seriously misguided. In etio-logic studies, restricting the phenotype to those with a puredisorder may be misleading, if risk factors in fact operate acrossa range of neurodevelopmental disorders. As noted above, inclu-sion of comorbid cases can provide a rich source of evidenceabout the reasons for co-occurrence of disorders, both whenstudying underlying impairments and when the focus is on etiology. Another instance where it may be unhelpful torestrict attention to pure cases is when conducting researchon intervention. For instance, a remedial package that iseffective for children with a pure reading disability may notwork well if there is co-occurring ADHD. Given the commonoverlap between disorders, we need more research that con-siders how presence of a comorbid disorder affects treatmentoutcome, rather than simply ignoring or excluding such cases.
Implications for Clinical Practice
Perhaps the most important point to stress is the need for clinicians to be aware of the complexity of neurodevelopmentaldisorders. Multidisciplinary assessment is key for identifyingeach child’s pattern of strengths and weaknesses. We areaware of cases where a child has received a diagnosis of SLIfrom a speech and language therapist, dyslexia from an edu-cational psychologist, ADHD from a pediatrician, ASD froma child psychiatrist and developmental dyspraxia from an occupational therapist! In part this may be because of the different perspective and expertise brought to the assessmentby different professionals, and in part by genuine changes inthe clinical presentation over time. For instance, a childwhose main problem in the preschool years is unintelligiblespeech may become intelligible but subsequently be diag-nosed as having developmental dyslexia (Bishop & Snowling,2004). Another child who initially seems to be a case of specific
receptive language disorder may subsequently merit a diagnosisof ASD (Conti-Ramsden, Simkin, & Botting, 2006). Most parents will be thoroughly confused by such multiple diagnoses,and conclude that somebody has “got it wrong.” It essentialthat professionals work together to ensure that the childreceives a diagnosis that provides access to the most appro-priate services, while at the same time assessing the whole rangeof areas of function that may be impaired. Intervention willneed to be individually tailored to take into account thechild’s specific strengths and weaknesses.
It is also important that both clinicians and parents recog-nize that diagnostic labels are shorthand descriptors that dotwo things: they summarize the child’s major area of deficit;and they indicate that the problem is neither part of anothersyndrome nor attributable to a known organic etiology. Alltoo often, those interpreting the labels assume they imply morethan this, and treat terms such as “developmental dyslexia”and “developmental dyspraxia” as if they referred to syndromeswith distinctive features and clear boundaries that are distinctfrom normality and have a known biologic basis. In practice,these diagnoses are made on the basis of quantitative differ-ence form normality. A statement such as “My child can’t readbecause he’s dyslexic” is not an explanation, rather it is a circular redescription of the problem. Furthermore, use of a single diagnostic label can oversimplify the complex and multifaceted nature of many neurodevelopmental disorders.
ReferencesAlbrecht, R., von Suchodoletz, W., & Uwer, R. (2000). The devel-
opment of auditory evoked dipole source activity from childhoodto adulthood. Clinical Neurophysiology, 111, 2268–2276.
American Psychiatric Association. (2000). Diagnostic and statisticalmanual of mental disorders, (4th ed.) Text revision. Washington,D.C: American Psychiatric Association.
Angold, A., Costello, E. J., & Erkanli, A. (1999). Comorbidity.Journal of Child Psychology and Psychiatry, 40, 57–87.
Baron-Cohen, S., & Hammer, J. (1997). Is autism an extreme formof the “male brain”? Advances in Infancy Research, 11, 193–217.
Beitchman, J. H., Brownlie, E. B., Inglis, A., Wild, J., Ferguson, B.,Schachter, D., et al. (1996). Seven-year follow-up of speech/languageimpaired and control children: psychiatric outcome. Journal ofChild Psychology and Psychiatry, 37, 961–970.
Bishop, D. V. M. (2002). Motor immaturity and specific speech andlanguage impairment: Evidence for a common genetic basis.American Journal of Medical Genetics: Neuropsychiatric Genetics,114, 56–63.
Bishop, D. V. M. (2006). Developmental cognitive genetics: How psychology can inform genetics and vice versa. Quarterly Journalof Experimental Psychology, 59, 1153–1168.
Bishop, D. V. M. & Edmundson, A. (1987). Specific languageimpairment as a maturational lag: evidence from longitudinal dataon language and motor development. Developmental Medicineand Child Neurology, 29, 442–459.
Bishop, D. V. M., & McArthur, G. M. (2004). Immature corticalresponses to auditory stimuli in specific language impairment: evid-ence from ERPs to rapid tone sequences. Developmental Science,7, F11–F18.
Bishop, D. V. M., & McArthur, G. M. (2005). Individual differencesin auditory processing in specific language impairment: A follow-up study using event-related potentials and behavioural thresholds.Cortex, 41, 327–341.
NEURODEVELOPMENTAL DISORDERS
39
9781405145923_4_003.qxd 3/07/2007 15:06 Page 39
UNCO
RREC
TED
PROOF

Bishop, D. V. M., & Norbury, C. F. (2002). Exploring the border-lands of autistic disorder and specific language impairment: Astudy using standardised diagnostic instruments. Journal of ChildPsychology and Psychiatry, 43, 917–929.
Bishop, D. V. M., & Snowling, M. J. (2004). Developmental dyslexiaand specific language impairment: Same or different? PsychologicalBulletin, 130, 858–886.
Bolton, P., Murphy, M., Macdonald, H., Whitlock, B., Pickles, A.,& Rutter, M. (1997). Obstetric complications in autism: Con-sequences or causes of the condition? Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 36, 272–281.
Breier, J. I., Gray, L., Fletcher, J. M., Diehl, R. L., Klaas, P.,Foorman, B. R., et al. (2001). Perception of voice and tone onsettime continua in children with dyslexia with and without atten-tion deficit/hyperactivity disorder. Journal of Experimental ChildPsychology, 80, 245–270.
Caron, C., & Rutter, M. (1991). Comorbidity in child psychopatho-logy: concepts, issues and research strategies. Journal of ChildPsychology and Psychiatry, 32, 1063–1080.
Cermak, S. A., Gubbay, S. S., & Larkin, D. (2002). What is devel-opmental coordination disorder? In S. A. Cermak & D. Larkin (Eds.),Developmental coordination disorder (pp. 2–22). Albany, NY:Delmar.
Clark, T., Feehan, C., Tinline, C., & Vostanis, P. (1999). Autistic symptoms in children with attention deficit-hyperactivity disorder.European Child and Adolescent Psychiatry, 8, 50–55.
Clegg, J., Hollis, C., Mawhood, L., & Rutter, M. (2005).Developmental language disorder: A follow-up in later adult life.Cognitive, language, and psychosocial outcomes. Journal of ChildPsychology and Psychiatry, 46, 128–149.
Conti-Ramsden, G., Botting, N., Simkin, Z., & Knox E. (2001). Follow-up of children attending infant language units: outcomes at 11 yearsof age. International Journal of Language Communication Dis-orders, 36, 207–219.
Conti-Ramsden, G., Simkin, Z., & Botting, N. (2006). The prevalenceof autistic spectrum disorders in adolescents with a history ofspecific language impairment (SLI). Journal of Child Psychology andPsychiatry, 47, 621–628.
Démonet, J., Taylor, M. J., & Chaix, Y. (2004). Developmentaldyslexia. Lancet, 363, 1451–1460.
Drummond, C. R., Ahmad, S. A., & Rourke, B. P. (2005). Rules for the classification of younger children with nonverbal learningdisabilities and basic phonological processing disabilities. Archivesof Clinical Neuropsychology, 20, 171–182.
Dykman, R. A., & Ackerman, P. T. (1991). Attention deficit dis-order and specific reading disability: Separate but often overlappingdisorders. Journal of Learning Disabilities, 24, 96–103.
Eisenmajer, R., Ross, N., & Pratt, C. (2005). Specificity and charac-teristics of learning disabilities. Journal of Child Psychology andPsychiatry, 46, 1108–1115.
Farmer, M. (2000). Language and social cognition in children withspecific language impairment. Journal of Child Psychology andPsychiatry, 41, 627–636.
Fisher, S. E. (2006). Tangled webs: tracing the connections betweengenes and cognition. Cognition, 10, 270–297.
Francis, D. J., Shaywitz, S. E., Stuebing, K. K., Shaywitz, B. A., &Fletcher, J. M. (1996). Developmental lag versus deficit models of reading disability: A longitudinal, individual growth curvesanalysis. Journal of Educational Psychology, 88, 3–17.
Geurts, H. M., Verté, S., Oosterlaan, J., Roeyers, H., Hartman, C.A., Mulder, E. J., et al. (2004). Can the Children’s CommunicationChecklist differentiate between children with autism, children withADHD, and normal controls? Journal of Child Psychology andPsychiatry, 45, 1437–1453.
Gilger, J. W., & Kaplan, B. J. (2001). A typical brain development:a conceptual framework for understanding developmental learningdisabilities. Developmental Neuropsychology, 20, 465–481.
Gogtay, N., Giedd, J. N., Lusk, L., Hayashi, K. M., Greenstein, D.,Vaituzis, A. C., et al. (2004). Dynamic mapping of human corticaldevelopment during childhood through early adulthood. Proceed-ings of the National Academy of Sciences, 101, 8174–8179.
Grigorenko, E. (submitted). Psychology of individual differences:Triumphs and tribulations of recent advancements in genetics andgenomics.
Harris, J. C. (1995). Developmental neuropsychiatry. New York andOxford: Oxford University Press.
Haynes, C., & Naidoo, S. (1991). Children with specific speech and language impairment (Clinics in Developmental Medicine:Vol. 119). London: MacKeith Press.
Hill, E. L. (2001). Non-specific nature of specific language impair-ment: a review of the literature with regard to concomitant motorimpairments. International Journal of Language and Communica-tion Disorders, 36, 149–171.
Hutton, J., Goode, S., Murphy, M., Le Couteur, A., & Rutter, M.New onset psychiatric disorders in individuals with autism. Autism(in press).
Kadesjö, B., & Gillberg, C. (1998). Attention deficits and clumsinessin Swedish 7-year-old children. Developmental Medicine and ChildNeurology, 40, 796–811.
Kaplan, B. J., Dewey, D. M., Crawford, S. G., & Wilson, B. N. (2001).The term comorbidity is of questionable value in reference todevelopmental disorders: data and theory. Journal of LearningDisabilities, 34, 555–565.
Karmiloff-Smith, A. (1998). Development itself is the key to under-standing developmental disorders. Trends in Cognitive Sciences, 2,389–398.
Klein, D. N., & Riso, L. P. (1993). Psychiatric disorders: problemsof boundaries and comorbidity. In C. G. Costello (Ed.), Basicissues in psychopathology (pp. 19–66). New York: Guilford Press.
Klin, A., Volkmar, F. R., Sparrow, S. S., Cicchetti, D. V., & Rourke,B. P. (1995). Validity and neuropsychological characterization ofAsperger syndrome: Convergence with nonverbal learning dis-abilities syndrome. Journal of Child Psychology and Psychiatry, 36,1127–1140.
Lewis, C., Hitch, G. J., & Walker, P. (1994). The prevalence of speci-fic arithmetic difficulties and specific reading difficulties in 9- to 10-year-old boys and girls. Journal of Child Psychology andPsychiatry, 35, 283–292.
Marlow, N. (2004). Neurocognitive outcome after very pretermbirth. Archives of Disease in Childhood, 89, F224-F228.
Marlow, N., Wolke, D., Bracewell, M. A. & Samara, M., for theEPICure Study Group (2005). Neurologic and developmental dis-ability at six years of age after extremely preterm birth. NewEngland Journal of Medicine, 352, 9–19.
Martin, N., Piek, J. P., & Hay, D. (2006). DCD and ADHD: A geneticstudy of their shared aetiology. Human Movement Science, 25,110–124.
Mayberry, R. I., & Lock, E. (2003). Age constraints on first versussecond language acquisition: Evidence for linguistic plasticity andepigenesis. Brain and Language, 87, 369–384.
McCarthy, R., & Warrington, E. (1990). Cognitive neuropsychology.San Diego: Academic Press.
Moffitt, T. E. (1993). Adolescence-limited and life-course-persistentantisocial behavior: A developmental taxonomy. PsychologicalReview, 100, 674–701.
Morton, J., & Frith, U. (1995). Causal modeling: A structuralapproach to developmental psychopathology. In D. Cicchetti & D. J. Cohen (Eds.), Developmental Psychopathology (Vol. 2, pp. 357–390). New York: Wiley.
Nelson, C. A., Bloom, F. E., Cameron, J. L., Amaral, D., Dahl, R.E., & Pine, D. (2002). An integrative, multidisciplinary approachto the study of brain–behavior relations in the context of typicaland atypical development. Development and Psychopathology, 14,499–520.
CHAPTER 3
40
$
%
9781405145923_4_003.qxd 3/07/2007 15:06 Page 40
UNCO
RREC
TED
PROOF

Nichols P. L., & Chen T. C. (1980). Minimal brain dysfunction: Aprospective study. Hillsdale, NJ: Lawrence Erlbaum Associates.
Noppeney, U., Friston, K. J., & Price, C. J. (2004). Degenerate neu-ronal systems sustaining cognitive functions. Journal of Anatomy,205, 433–442.
Oyama, S. (1976). A sensitive period for the acquisition of a non-native phonological system. Journal of Psycholinguistic Research,5, 261–283.
Pasamanick, B., & Knobloch, H. (1966). Reproductive studies on theepidemiology of reproductive casuality: old and new. MerrillPalmer Quarterly, 12, 7–26.
Pelletier, P. M., Ahmad, S. A., & Rourke, B. P. (2001). Classificationrules for basic phonological processing disabilities and nonverballearning disabilities: Formulation and external validity. ChildNeuropsychology (Neuropsychology, Development and Cognition:Section C), 7, 84–98.
Pennington, B. (2006). From single to multiple deficit models ofdevelopmental disorders. Cognition, 101, 385–413.
Peterson, BS. (2003). Conceptual, methodological and statisticalchallenges in brain imaging studies of developmentally based psy-chopathologies. Development and Psychopathology, 15, 811–832.
Rapoport, J. L., Addington, A. M., & Frangou, S. (2005). The neurodevelopmental model of schizophrenia: update. MolecularPsychiatry, 10, 434–449.
Rourke, B. P. (1989). Nonverbal learning disabilities: The syndromeand the model. Guilford Press: New York.
Rutter, M. (1982). Syndromes attributed to “minimal brain dysfunc-tion” in childhood. American Journal of Psychiatry, 139, 21–33.
Rutter, M. (1997). Comorbidity: concepts, claims and choices.Criminal Behaviour and Mental Health, 7, 265–286.
Rutter, M., Caspi, A., Fergusson, D., Horwood, L. J., Goodman, R.,Maughan, B., et al. (2004). Sex differences in developmental read-ing disability: new findings from 4 epidemiological studies. Journalof the American Medical Association, 291, 2007–2012.
Rutter, M., Caspi, A., & Moffitt, T. E. (2003). Using sex differencesin psychopathology to study causal mechanisms: unifying issues andresearch strategies. Journal of Child Psychology and Psychiatry, 44,1092–1115.
Rutter, M., Kim-Cohen, J., & Maughan, B. (2006a). Continuities anddiscontinuities in psychopathology between childhood and adult life.Journal of Child Psychology and Psychiatry 47(3/4), 276–295.
Rutter, M., Moffitt, T. E., & Caspi, A. (2006b). Gene–environmentinterplay and psychopathology: multiple varieties but real effects.Journal of Child Psychology and Psychiatry, 47, 226–261.
Shalev, R. S., Auerbach, J., Manor, O., & Gross-Tsur, V. (2000).Developmental dyscalculia: prevalence and prognosis. European Childand Adolescent Psychiatry, 9(Supplement 2), 58–64.
Shaw, P., Greenstein, D., Lerch, J., Clasen, L., Lenroot, R., Gogtay,N., et al. (2006a). Intellectual ability and cortical development inchildren and adolescents. Nature, 440(7084), 676–679.
Shaw, P., Lerch, J., Greenstein, D., Sharp, W., Clasen, L., Evans, A.,et al. (2006b). Longitudinal mapping of cortical thickness and clinical outcome in children and adolescents with attention-deficit/hyperactivity disorder. Archives of General Psychiatry, 63,540–549.
Snowling, M., & Nation, K. (1997). Language, phonology and learn-ing to read. In C. Hulme & M. Snowling (Eds.), Dyslexia: bio-logy, cognition and intervention (pp. 153–166). London: WhurrPublishers.
Stanovich, K. E. (1986). Matthew effect in reading: some consequencesof individual differences in the acquisition of literacy. ReadingResearch Quarterly, 21, 360–407.
Tager-Flusberg, H. (1999). Neurodevelopmental disorders. Cambridge,MA: MIT Press.
Tager-Flusberg, H., & Joseph, R. M. (2003). Identifying neurocog-nitive phenotypes in autism. Philosophical Transactions of the RoyalSociety of London, Series B, 358, 303–314.
Temple, C. (1997). Developmental cognitive neuropsychology.Journal of Child Psychology and Psychiatry, 38, 27–52.
Thomas, M., & Karmiloff-Smith, A. (2003). Modeling languageacquisition in atypical phenotypes. Psychological Review, 110,647–682.
Wender, P. (1971). Minimal brain dysfunction in children. NewYork, John Wiley & Sons.
Willcutt, E. G., & Pennington, B. F. (2000). Psychiatric comorbidityin children and adolescents with reading disability. Journal ofChild Psychology and Psychiatry, 41, 1039–1048.
Willcutt, E. G., Pennington, B. F., Smith, S. D., Cardon, L. R.,Gayan, J., Knopik, V. S., et al. (2002). Quantitative trait locus forreading disability on chromosome 6p is pleiotropic for attention-deficit/hyperactivity disorder. American Journal of Medical Genetics:Neuropsychiatric Genetics, 114, 260–268.
Wolf, U. (1997). Identical mutations and phenotypical variation.Human Genetics, 100, 305–321.
World Health Organization. (1996). Multi-axial classification ofchild and adolescent psychiatric disorders: The ICD-10 classifica-tion of mental and behavioral disorders in children and adolescents.Cambridge: Cambridge University Press.
Wright, B. A., & Zecker, S. G. (2004). Learning problems, delayeddevelopment, and puberty. Proceedings of the National Academyof Sciences, 101, 9942–9946.
Zangwill, O. L. (1978). The concept of developmental dysphasia. InM. A. Wyke (Ed.), Developmental dysphasia. London: AcademicPress.
NEURODEVELOPMENTAL DISORDERS
41
9781405145923_4_003.qxd 3/07/2007 15:06 Page 41
UNCO
RREC
TED
PROOF

Author Query Form
Book title: Rutter’s Child and Adolescent Psychiatry
Chapter title: Neurodevelopmental Disorders: Conceptual Issues
Query Query RemarksRefs.
1 Axis II changed to Axis 2 as used earlier
2 Update or cite as personal communication
3 Update Hutton et al. in press
4 Delete unless published. If published provide full details
5 Provide published details or cite as unpublished in text
9781405145923_4_003.qxd 3/07/2007 15:06 Page 42
UNCO
RREC
TED
PROOF