Embed Size (px)
Citation preview

Nerve injury
Hamad emad dhuhayr
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby

OUTLINE
DEFINITION. TYPES OF NERVE INJURIES. FATE (pathophysiology) AND
REHABILITATION. ETIOLOGY. PRESENTATION. DIAGNOSIS. CLINICAL EXAMPLES: (ERB’S,CARPAL TUNNEL,RADIAL,ULNAR,SCIATIC AND
PERONEAL N.)
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby
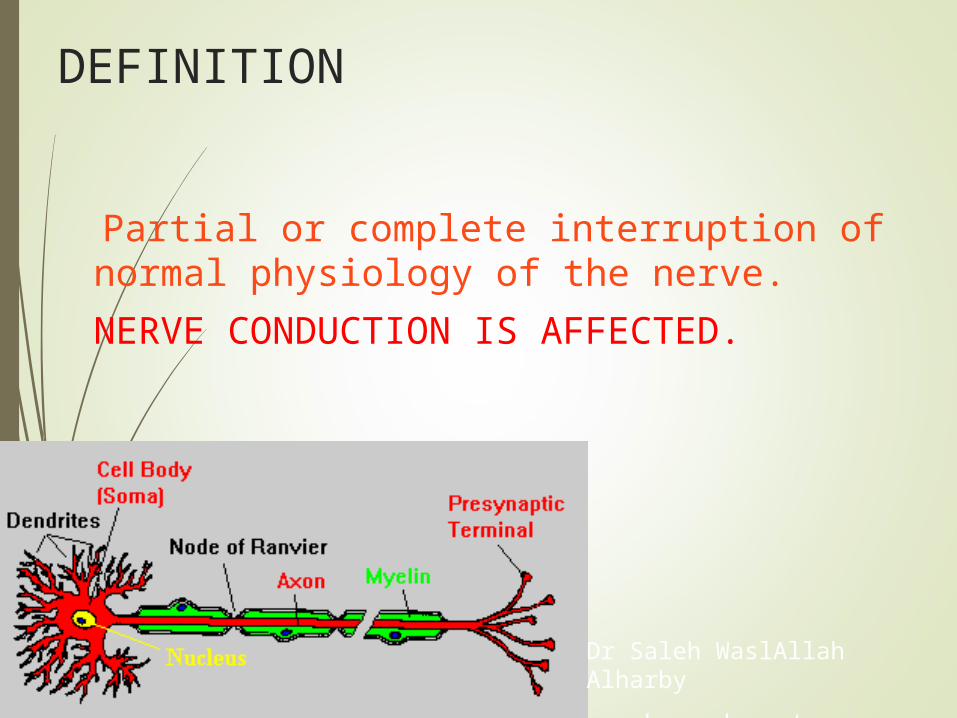
DEFINITION
Partial or complete interruption of normal physiology of the nerve.
NERVE CONDUCTION IS AFFECTED.
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby

Classification Of Nerve Injuries
Seddon, Sunderland and lately by Mackinnon
6 degrees

Degrees Of Nerve Injury
1st degree of injury(neuraparaxia)
Segmental demylination
Axons intact
Recovery in 12 to 16 wks
2nd degree injury(axonotmesis)
Axonal injury/ distal wallerian degeneration
Regeneration at rate of 1 inch per month
Complete slow recovery
Degrees Of Nerve Injury
3rd degree injury Axonal injury & fibrosis of endoneurium Incomplete recovery
4th degree injury Axonal injury Damage to endo and perineurium with
dense scarring Needs surgical intervention

Degrees Of Nerve Injury
5th degree injury(neurotmesis) Complete nerve division
6th degree injury Variable combination of previous
five degrees of nerve injury

FATE AND REHABILITATION
WALLERIAN DEGENERATION
1 MM PER DAY
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby

REHABILITATION
PAIN CONTROL.
SPLINT. (AVOID PRESSURE SORES) NERVE AND MUSCLE STIMULATION.
NEARBY JOINTS RANGE OF MOTION.
MONTHS ----- YEARS .
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby

Nerve Injury
Focal contusion (gunshot wounds) Stretch/traction injury Drug injection injury Compression Crush injuries Avulsion Laceration Electrical burns Idiopathic Others(Viral infections, metabolic and neural disorders)

PERSENTATION
PAIN LOSS OF SENSATION LOSS OF MOTION LOSS OF POWER LOSS OF REFLEXES WASTING TROPHIC CHANGES
(skin,sc,neurovascular,bones,muscles)
CONTRACTURES
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby

DiagnosisDiagnosis
Motor functionMotor function
Movements, muscle atrophyMovements, muscle atrophy
sensory functionsensory function
Tinel sign, Ten testTinel sign, Ten test
Two point discriminationTwo point discrimination
Touch, vibrationTouch, vibration
•HistoryHistory•Examination Examination

Tinel Sign
Tinel sign: - peripheral tingling or
dysaesthesia' provoked by percussion of the nerve
Positive in axonal injuries

Electrical Stimulation Tests:
EMG
NCS
Intra operative nerve action potential

CLINICAL EXAMPLES
ERB’ PALSY
CARPAL TUNNEL SYNDROME(MEDIAN NV)
RADIAL NERVE INJURY
ULNAR NERVE INJURY
SCIATIC NERVE INJURY
LATERAL POPLITEAL NERVE INJURY
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby
ERB’S PALSY
BIRTH INJURY (DIFFICULT LABOUR) TRACTION ON NERVE ROOTS C5-6 STRETCH-RUPTURE-AVULSION UPPER LIMB IN EXTENSION MOTHER NOTICE NO MOTION 90% GOOD RECOVERY ROLE OF SURGERY AFTER 3 MONTHS REMEMBER PROPER REHABILITATION
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby
CARPAL TUNNEL SYNDROME
MEDIAN NERVE ENTRAPMENT BY FLEXOR RETINACULUM PAIN,NUMBNESS,NIGHT
MANUAL WORKERS
DIAGNOSIS
SURGERY
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby

RADIAL NERVE INJURY
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby

ULNAR NERVE INJURY
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby

SCIATIC NERVE INJURY
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby
PERONEAL NERVE INJURY (LPN)
FOOT DROP
TIGHT POP
SKELETAL TRACTION
DIRECT INJURY (RARE)
DYNAMIC SPLINT
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby

Principals Of Nerve Repair
Microsurgical techniques
Adequate magnification
Microsurgical instruments & sutures
Different techniques:
Primary nerve repair
Nerve grafting
Nerve transfer
Nerve conduits
Nerve allografts

Timing Of The Nerve Repair
Sharply transected nerves
Immediate repair
Crushed, avulsed, blast injuries
Nerve ends tacked together
Repair delayed for 3 weeks or until wound bed permits
Re-exploration
Neuroma excision, nerve grafts
Acute nerve grafting in the 1st sitting
Bleeding control ,trimming of fascicles ,loose epineural suturing
Closed injuries treated expectantly for 12 weeks


Primary Nerve Repair
Primary nerve repair Epineural repair Grouped fascicular repair

Epineural Repair
Standard repair

Fascicular Repair
Restore the continuity of fascicles Internal topography Intra-operative nerve stimulation Neurolysis with the eyes Priority to the motor recovery(radial
and peroneal nerve)

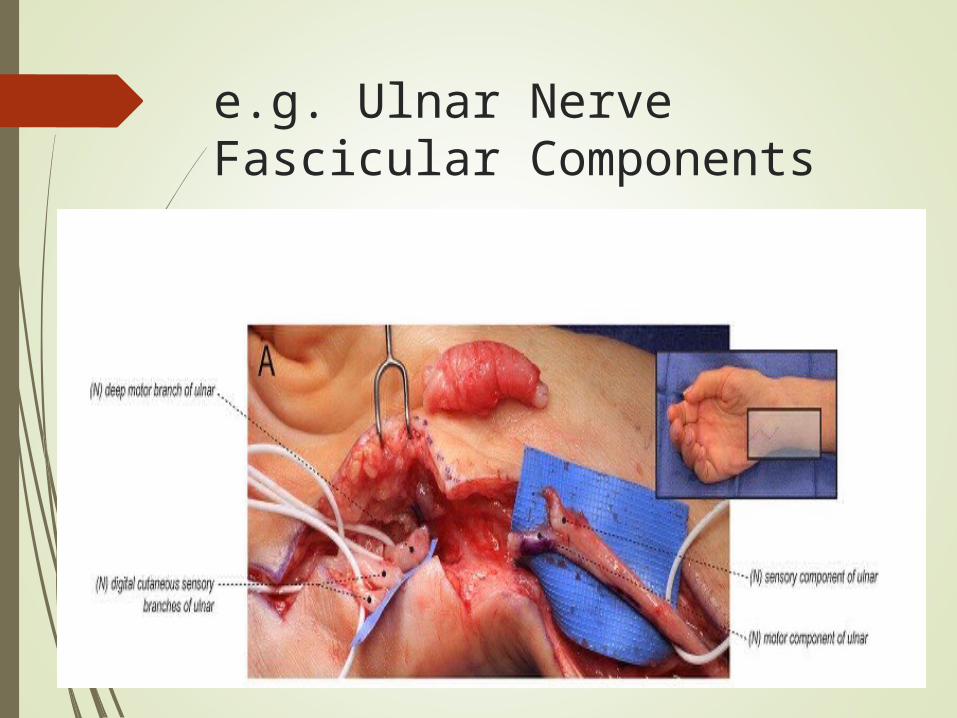
e.g. Ulnar Nerve Fascicular Components
Nerve Grafts
Tension at site of repair
Need of postural positioning
Alignment of sensory & motor components
Maximize number of axons
Reversal of graft
Exclusion of expendable nerve
Options For Nerve Grafts
Sural nerve
30-40cm
Lateral peroneal communicating br : 10-20cm
Lateral antebrachial cutaneous nerve(LABC)
8cm
Medial antebrachial cutaneous nerve (MABC)
Anterior & posterior division
20 cm
Expendable nerves(peroneal and radial)
Sensory branches of ulnar and median nerves
Distal anterior interosseous nerve and so on…

Disadvantages
Donor site scarring Donor site sensory loss
Patient education

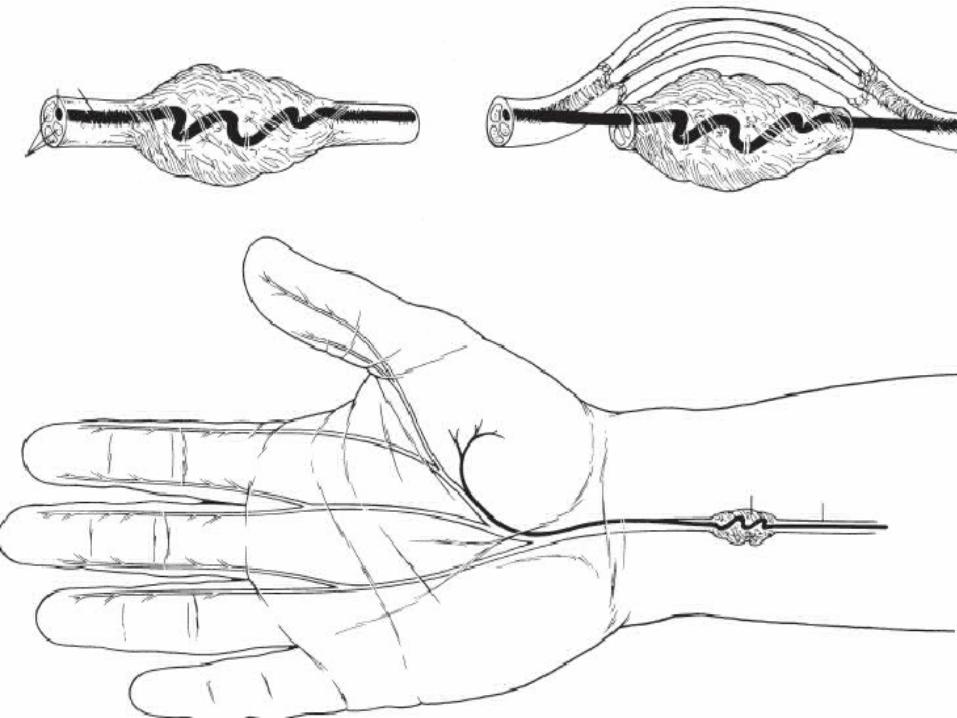
Neuroma In Continuity
Complete : resection and repair with graft


Neuroma In Continuity
Incomplete neuroma
Intra-operative nerve stimulation
Black boxing around neuroma

Nerve Transfer
Indications:
Very proximal peripheral nerve injuries
Root avulsions
Excessive scarring
Level of injury unclear
Idiopathic neuritides
Radiation induced nerve injury

Nerve Transfer
Motor nerve transfer
Pure motor axons
Close proximity
expendable
Synergistic supply
Sensory nerve transfer
pure sensory axons
Innervates non critical area
Expendable and lying in close proximity

Most Common Uses Of Nerve Transfer
elbow flexion
Shoulder abduction
Ulnar-innervated intrinsic hand function
Forearm pronation
Radial nerve function

Transfer of radial nerve to axillary nerve
Nerve Conduits
Veins, pseudo-sheaths, bioabsorbable tubes
short nerve gaps ≤ 3cm Low antigenicity , biodegradability Trials to add a nerve graft inside the
conduit neurotrophic factors


Nerve Allografts
Extensive injuries
Limited donor material
Immunosuppressive agents
FK506( tacrolimus )
Prednisone , azathioprine
Processed acellular cadaveric nerve allografts
AxoGen, Inc. ,Alachua, FL.

Summary
Axon degeneration occurs from mild compression injury
The prognosis for Neuropraxia is poor Axonotmesis is generally caused from
separation of the cell body from the neuron
Wallerian Degeneration typically does not occur in Neuropraxic injury
Surgical reconstruction is necessary in Neurotmesis
Wallerian Degeneration does not occur in Neurotmesis
A ligamentous structure can cause Neuropraxia
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby

Refferences
Special surgery matary
Dr Saleh WaslAllah Alharby
www.ksu.edu.sa/DrSalehAlharby