Embed Size (px)
Citation preview
NEONATAL INFECTIONS
NEONATAL INFECTIONS
Infections occur frequently in the
neonate, causing illness and possibly death.
There are several reasons for the neonate to
get infections like the variety of organisms
usually present in the uterus during
gestation, in the cervix and vagina during
delivery, and in the environment of hospital
and community; and immature host defense
that causes the neonate to be overcome by
these organisms.
Pathophysiology
fetus can acquire microorganisms transplacentally
or during delivery
nosocomial infections
Mode of infection
Antenatal:
Transplacental
Amnionitis
Intranatal:
early rupture of membranes
Contamination while passing through the vagina
Ophthalmia neonatorum (gonococcal infection)
Oral thrush (candida albicans)
Cord sepsis from improper asepsis while cutting cord
Postnatal:
Transmission from infected mother, relatives or
hospital staff
Cross infection from another infected baby
Infected articles used for feeding, bathing, clothing
etc.
Clinical manifestations of
infections in the neonate
General:
Fever, hypothermia
“Not doing well”
Poor feeding
Lethargy
Scleroderma
Gastrointestinal system:
Abdominal distention
Anorexia, vomiting
Diarrhoea
Hepatomegaly
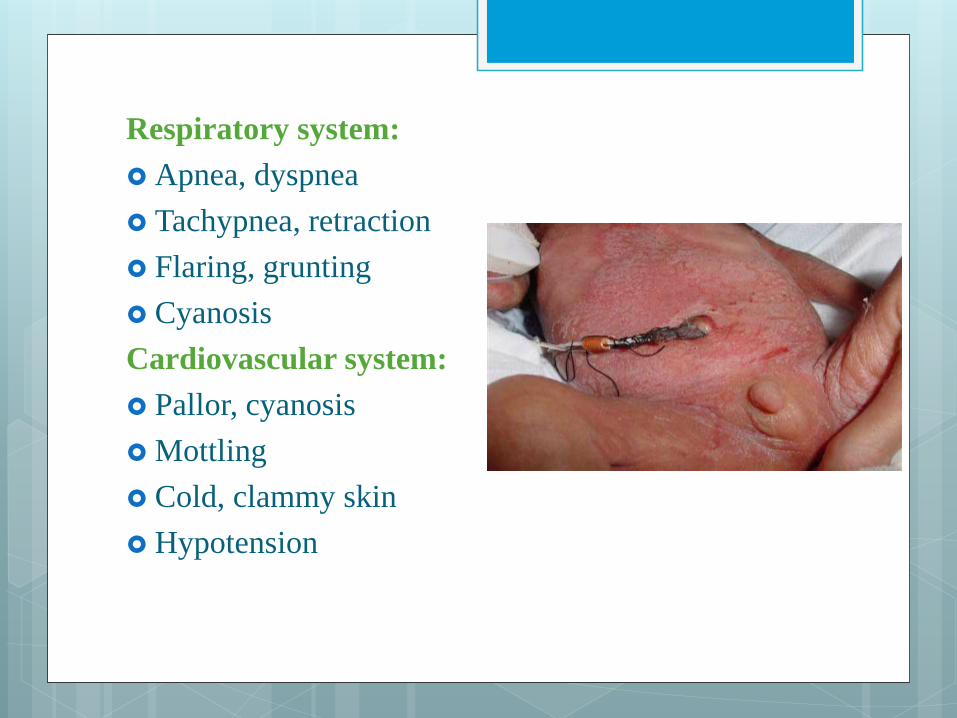
Respiratory system:
Apnea, dyspnea
Tachypnea, retraction
Flaring, grunting
Cyanosis
Cardiovascular system:
Pallor, cyanosis
Mottling
Cold, clammy skin
Hypotension
Central nervous system:
Irritability
Tremors, seizures
Hyporeflexia
Abnormal Moro reflex
Irregular respirations
Full fontanel
Hematologic system:
Jaundice
Splenomagaly
Pallor
Petechiae, purpura
Bleeding
TOXOPLASMOSIS
The host of this parasite is the cat and the
organism is acquired in humans either by direct
faeco- oral ingestion of undercooked meat
containing toxoplasma cysts.
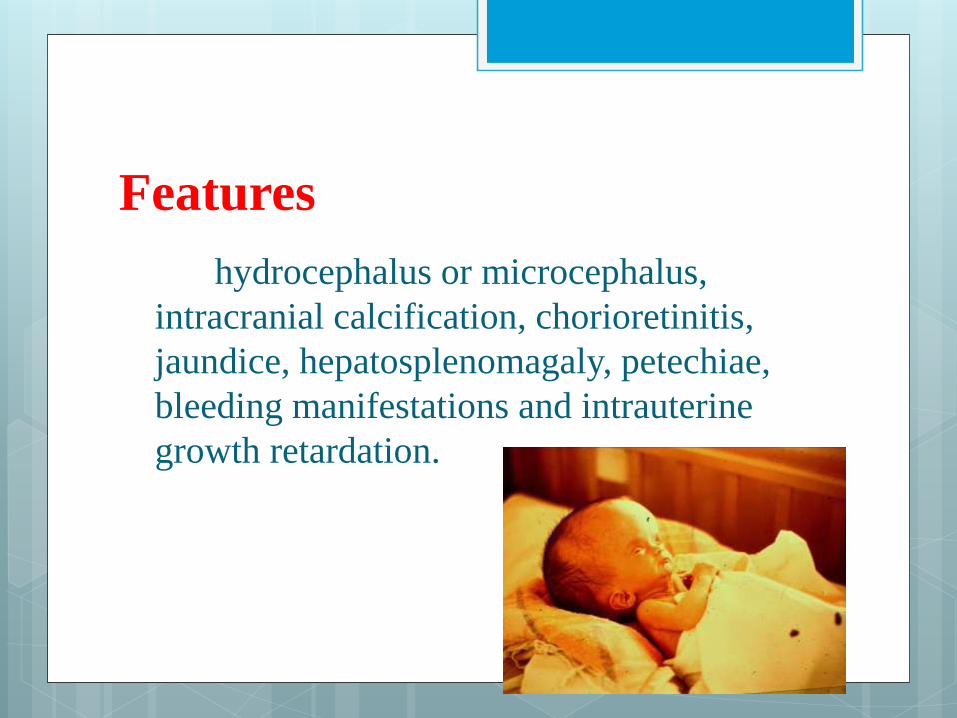
Features
hydrocephalus or microcephalus,
intracranial calcification, chorioretinitis,
jaundice, hepatosplenomagaly, petechiae,
bleeding manifestations and intrauterine
growth retardation.
Diagnosis is by isolating the organism in
body fluids by culture or polymerase chain
reaction and serological tests.
Treatment consists of pyrimethamine and
sulphadiazine.
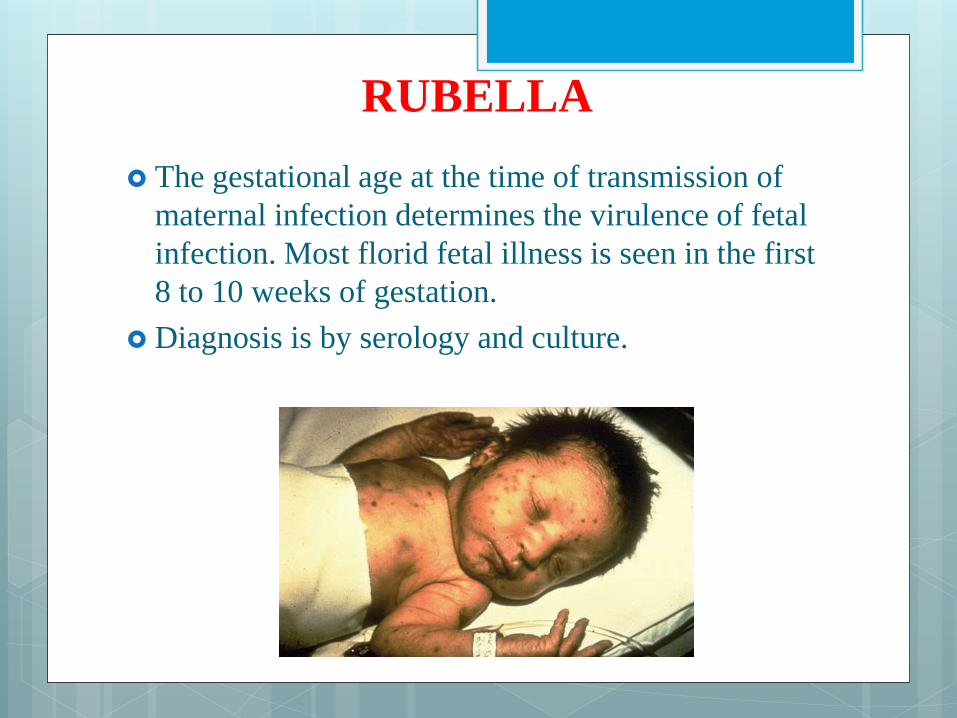
RUBELLA
The gestational age at the time of transmission of
maternal infection determines the virulence of fetal
infection. Most florid fetal illness is seen in the first
8 to 10 weeks of gestation.
Diagnosis is by serology and culture.
Congenital defects include sensorineural deafness,
cardiovascular malformations like patent ductus
arteriosus, microcephaly and mental retardation,
IUGR, cataract, glaucoma and retinopathy and
thrombocytopenic purpura.
There is no effective treatment for congenital
rubella
CYTOMEGALOVIRUS
common features are microcephalus, intracranial
calcification, hepatosplenomegaly, petechiae and
jaundice.
Diagnosis is made by culture of the organism &
specific IgM antibodies in the blood.
There is no specific treatment.
In those who present with the above signs, the
mortality rate is 20 to 30%
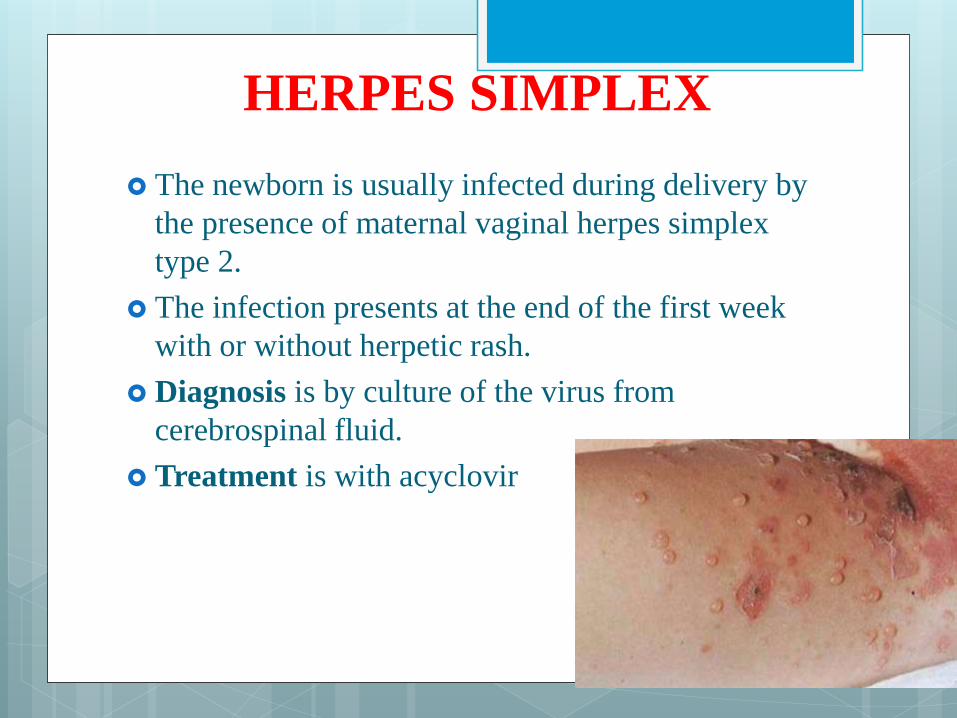
HERPES SIMPLEX
The newborn is usually infected during delivery by
the presence of maternal vaginal herpes simplex
type 2.
The infection presents at the end of the first week
with or without herpetic rash.
Diagnosis is by culture of the virus from
cerebrospinal fluid.
Treatment is with acyclovir
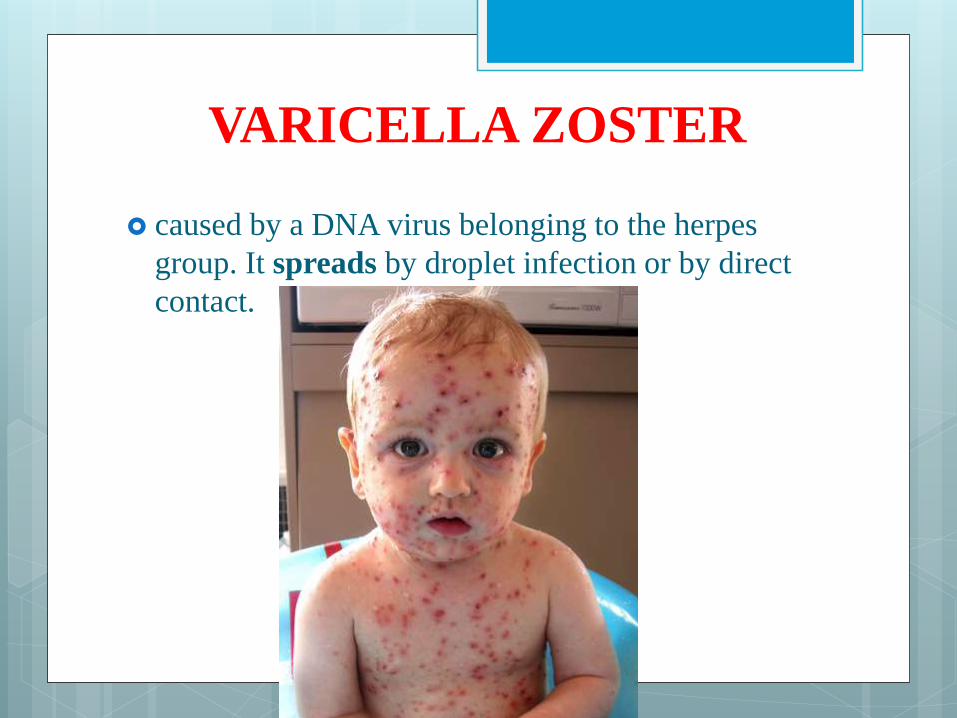
VARICELLA ZOSTER
caused by a DNA virus belonging to the herpes
group. It spreads by droplet infection or by direct
contact.
Following the incubation period of 12- 16days, a
prodrome characterized by fever, malaise and
myalgia is usual. A rash then appears in crops of
pruritic clusters of vesicles progressing to pustules
seen on the skin and mucous membrane in a
centripetal distribution. It is common to see all
stages of rash on the trunk.
complications like pneumonia, aseptic meningitis,
encephalitis, myocarditis, glomerulonephritis and
thrombocytopenia may occur.
Diagnosis is based on clinical manifestations,
examination of Giemsa- stained smears and the 4
fold rise in the serum antibody titre.
treatment includes acyclovir, Varicella zoster
immunoglobulin
HEPATITIS B
The neonate infection rate from the carrier mothers
ranges from 10 to 40%. If the newborn is affected,
85 to 90% will become chronic carriers (HBsAg
positive) and many will experience progressive
hepatic damage, with the likelihood of
hepatocellular carcinoma
an incubation period of 35 to 50 years.
The infant rarely demonstrates the classical
symptoms; the great majority has subclinical
infection and enters the carrier state.
In infants born to high risk mothers, hepatitis B
immunoglobulin 200 IU IM is given soon after
birth together with hepatitis B vaccine IM in a
different limb and followed by similar dosage of
vaccine at 1 and 2 months of age. Universal
immunization (1st dose after birth, then at 1 and 6
months of age) of all infants is recommended
ACQUIRED IMMUNO
DEFICIENCY SYNDROME
retrovius that primarily infects cells of immune
system, including helper T lymphocytes (CD4 T
lymphocytes), monocytes and macrophages.
Incidence
Without intervention, 15 to 30% of infants born to
HIV infected women will be affected.
Transmission
HIV is transmitted by sexual contact, percutaneous
exposure to contaminated blood and mother to child
transmission. Vertical transmission may occur in
utero, at the time of delivery, or via breast feeding.
Risk factors
High maternal plasma HIV RNA
Advanced maternal disease stage
Low CD4 lymphocyte count
Premature delivery
Increased exposure to maternal blood or cervical
secretions at the time of delivery

Clinical manifestations
Primary acute infection
Non specific symptoms
Infections related to immunodeficiency:
Organ system disease
Malignancy
Diagnosis
HIV antibody is measured by ELISA
Confirmatory test is by Western blot
HIV nucleic acid, RNA or DNA can be detected by
PCR, branched DNA chain assay and nucleic acid
sequence- based amplification
Prevention
Limit the vaginal examinations to a minimum.
Avoid using scalp electrodes or intrauterine
monitoring catheters.
All linen should be collected in a vessel containing
hypochlorite solution.
All cotton swabs, dressing pads, mops must be
discarded in a container with hypochlorite
solution.
All needles, syringes and sharp blades must be
collected and disposed off with due precautions.
After delivery, the flooring must be cleaned with
antiseptic solution by an attendant who observes
all precautions as detailed above.
Fumigate the labor room or theatre.
Autoclave all instruments after proper washing and
cleaning.
The patient should be explained the need for
protection of the staff.
Intrapartum therapy
Zidovudine 2mg/kg IV during the first hour of labor,
there after 1mg/kg/hour throughout the rest of labor.
Zidovudine the same dosage 4 hours before cesarean
section.
Avoid artificial rupture of membranes
Cap, mask, gown, double gloves, goggles should be
worn.
Caesarean section decreases 50% risk of vertical
transmission.
Sterilize the instruments and linens.
Health care workers should protect themselves
Post exposure prophylaxis
Use disposable syringes and discard properly.
Postpartum care
After delivery, all the newborns are administered zidovudine
oral syrup in the dose of 2mg/kg body weight 4 times daily
for 6 weeks postpartum.
Babies born to HIV infected mothers are HIV positive
because of passive transfer of maternal antibodies to the
newborn. Levels of these antibodies gradually decline and by
the end of 6 months most non infected babies will become
seronegative.
Majority of the babies born to HIV infected mothers have no
physical signs of infection. Rarely, they may exhibit the so-
called HIV embryopathy characterized by growth retardation,
microcephaly and craniofacial abnormalities.
Breast feeding
Contraception
Counseling
Management
Decrease fetal viral exposure by preventing
chorioamnionitis, shortening the duration of labour,
delay rupture of membranes.
The practice of elective caesarean section at term/
onset of labour to prevent exposure of the fetus
Zidovudine is the only drug proven to be of value in
reducing perinatal transmission risk of HIV from 25%
to about 7%.
The practice of advocating elective caesarean section
close to term to reduce the risk of vertical
transmission of the disease is still debatable.
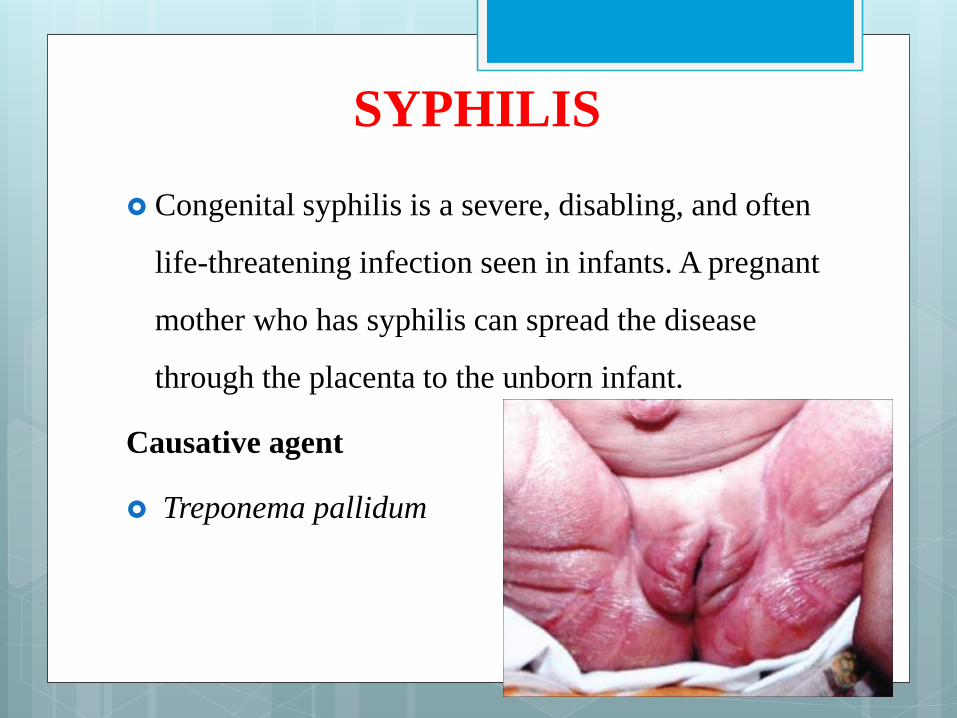
SYPHILIS
Congenital syphilis is a severe, disabling, and often
life-threatening infection seen in infants. A pregnant
mother who has syphilis can spread the disease
through the placenta to the unborn infant.
Causative agent
Treponema pallidum
Classification
Early
Newborns may be asymptomatic and are only
identified on routine prenatal screening. If not
identified and treated, these newborns develop poor
feeding and rhinorrhea.
After, they can develop late congenital syphilis.
Symptomatic newborns, if not stillborn, are born,
with hepatosplenomegaly, skeletal abnormalities,
pneumonia and a bullous skin disease known as
pemphigus syphiliticus.
Late
Late congenital syphilis is a subset of cases of
congenital syphilis.
Symptoms:-
blunted upper incisor teeth known as Hutchinson's
teeth
inflammation of the cornea known as interstitial
keratitis
Deafness from auditory nerve disease
frontal bossing (prominence of the brow ridge)
saddle nose (collapse of the bony part of nose)
hard palate defect
swollen knees
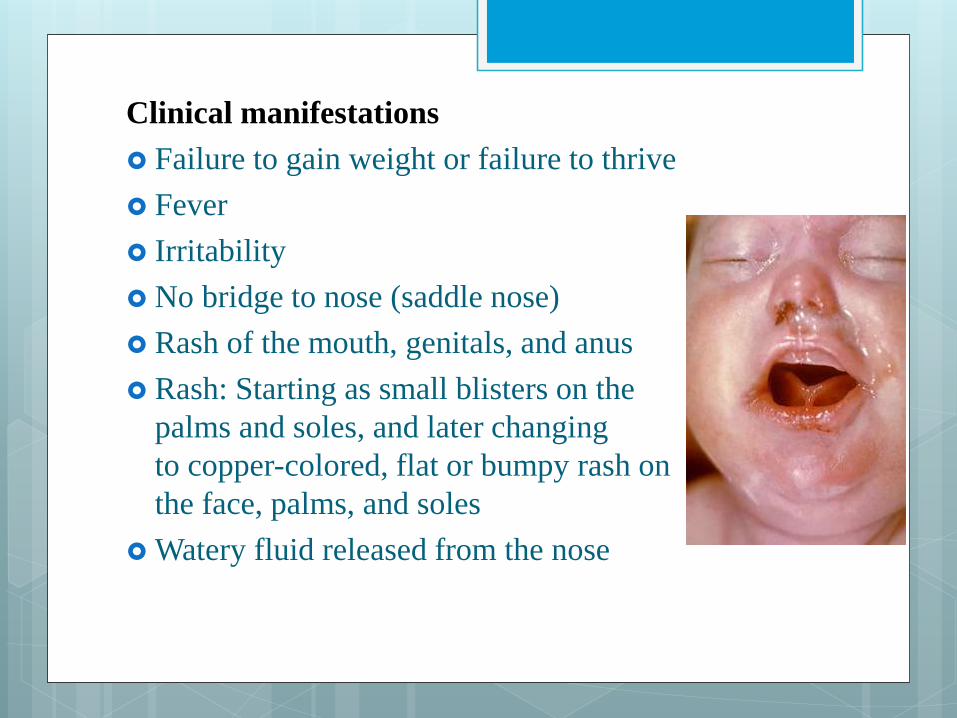
Clinical manifestations
Failure to gain weight or failure to thrive
Fever
Irritability
No bridge to nose (saddle nose)
Rash of the mouth, genitals, and anus
Rash: Starting as small blisters on the
palms and soles, and later changing
to copper-colored, flat or bumpy rash on
the face, palms, and soles
Watery fluid released from the nose
Mulberry molars (permanent first molars
with multiple poorly developed cusps).
Frontal bossing
Poorly developed maxillae
Enlarged liver and spleen
Petechiae
Diagnosis
physical examination of the infant may show signs
of liver and spleen swelling and bone inflammation.
A routine blood test for syphilis is done during
pregnancy.
The mother may receive the following blood tests:
Fluorescent treponemal antibody absorbed test
(FTA-ABS)
Venereal disease research laboratory test (VDRL)
An infant or child may have the following tests:
Bone x-ray
Dark-field examination to detect syphilis bacteria
under a microscope
Eye examination
Lumbar puncture
Treatment
Penicillin is used to treat all forms of
syphilis. IM procaine Penicillin G
50,000units per Kg Per each day for 10 days.
Complications
Blindness
Deafness
Deformity of the face
Nervous system problems
Death from pulmonary hemorrhage
Prevention
Safer sexual practices may help prevent syphilis.
Prenatal care is very important. A routine blood
test for syphilis is done during pregnancy.
ACQUIRED NEONATAL
INFECTIONS Adequate hand washing with an antibacterial
solution before examination or contact with the
neonate
Avoidance of overcrowding
Individual equipment is required for each cot
Communal areas should be kept clean. Scales should
be covered with disposable paper for each weighing.
Sterilization or disposal of equipment such as
oxygen and suction tubing
Cleanliness in preparation and storage of feeds
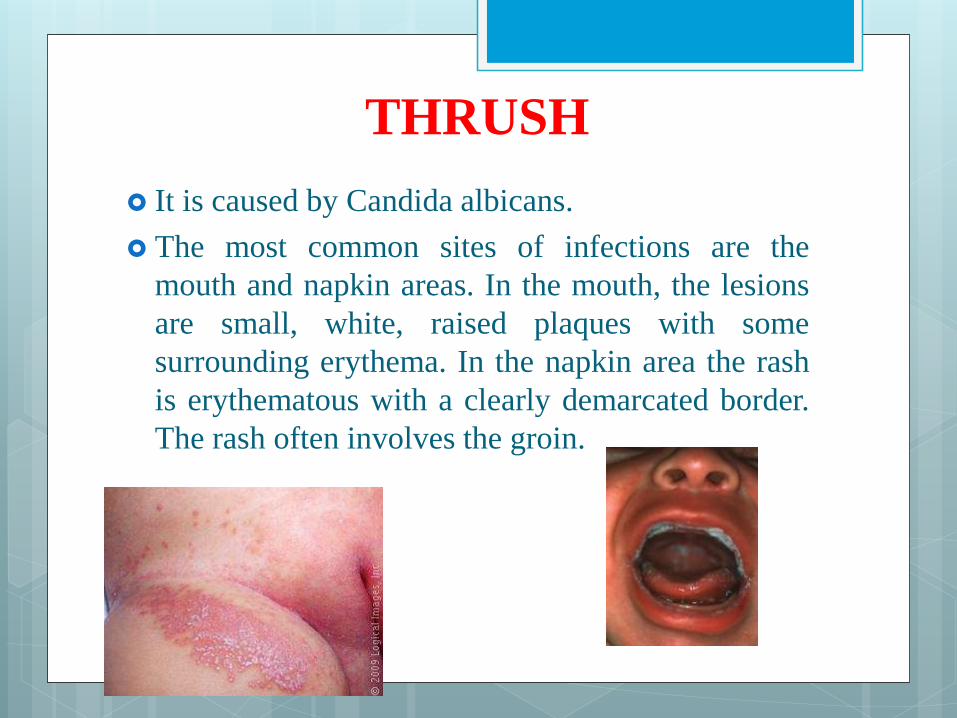
THRUSH
It is caused by Candida albicans.
The most common sites of infections are the
mouth and napkin areas. In the mouth, the lesions
are small, white, raised plaques with some
surrounding erythema. In the napkin area the rash
is erythematous with a clearly demarcated border.
The rash often involves the groin.
It is treated with nystatin mixture orally 1,00,000
units in 1ml 4 times a day after feeds or by oral
application of 1% aqueous solution of gentian
violet or clotrimazole mouth paint. Clotrimzole 1%
or nystatin ointment 2% or miconazole ointment
2% is used for 2 weeks in the nappy and the groin.
Oral administration of nystatin or flucanazole
recommeded for 2 weeks

CONJUNCTIVITIS ( OPHTHALMIA NEONATORUM
Causative agents
Unilateral conjunctivitis after 5 days of life is often
due to Chlamydia trachomatis. Purulent
contunctivitis which may affect one or both eyes
within 48 hours of age. Other microorganisms
causing neonatal conjunctivitis are streptococcus,
Staphylococcus, Pneumococcus, E.coli, Herpes
simplex virus. Chemical conjunctivitis is due to
irritation of silver nitrate, soap and local antibiotic
drops.
Mode of infection
Infected hands of caregivers, infected birth canal
and cross infection from other infected infants
Infection can occur directly from other sites of
infections like skin and umbilicus
Clinical features
Varies with mode of infection and causative
organism
Neonate may present with sticky eyes with or
without discharge from watery or mucopurulent
discharge
Eyelids may be swollen
Closed eyelids due to spasm of orbicularis oculi
muscle
Diagnosis
Diagnosis is made by examination of smear of
the eye discharge and by culture in Thayer- Martin
medium
Management
Antibiotic therapy after detecting causative
organism
Sulfacetamide or framycetin or chloramphenicol
drops or erythromycin ointment are used
Pencillin therapy for gonococcal disease
Clean the eyes with sterile cotton swabs soaked in
saline should be done after hand washing
Prevention
Treatment of maternal infection, aseptic
technique during delivery, special care and
attention in face and breech presentation,
isolation of infected baby and maintenance
of general cleanliness
Complications
Orbital cellulitis
Dacrocystitis with obstruction of nasolacrimal duct
Corneal ulceration
Blindness
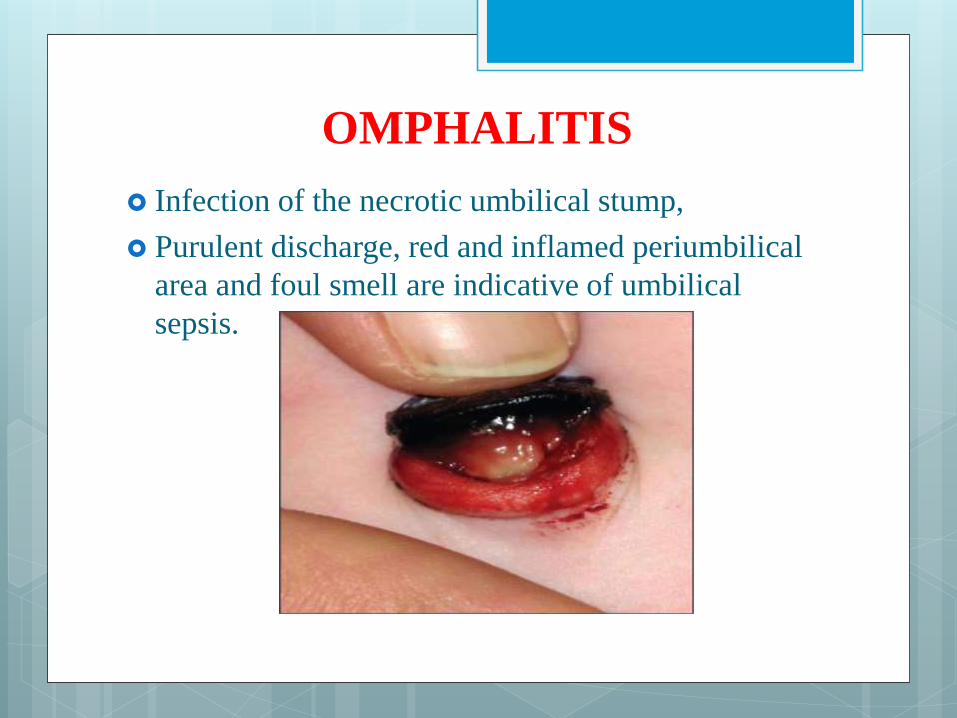
OMPHALITIS
Infection of the necrotic umbilical stump,
Purulent discharge, red and inflamed periumbilical
area and foul smell are indicative of umbilical
sepsis.
In mild cases frequent cleaning with spirit or
alcohol and application of antibiotic powder (
containing neomycin, bacitactin and polymyxin O
are enough)
Systemic antibiotics are started after taking a skin
swab, and application of antibiotic creams locally.
SKIN INFECTIONS
Skin pustules or paronychia (infection of the bed
of the nails) are usually caused by Staphylococcus
aureus. Treatment with topical antibiotic
SYSTEMIC INFECTIONS
early’ in the first 3 days, or ‘late’ after usually 7 to
10 days.
The commonly implicated organisms are group B
beta- hemolytic streptococcus, E-coli, Klebsiella,
Psedomonas, Staphylococcus aureus, and in the
very preterm infant, Staphylococcus epidermidis.
Risk factors for systemic infections:
Prolonged rupture of membranes (24 hours)
Known vaginal colonization with group B
streptococcus
Prematurity
Maternal fever
Any breach of the skin such as skin trauma
Indwelling catheters
Presentation
respiratory distress, lethargy, poor temperature
regulation, poor feeding, vomiting, apnea, pallor
and abdominal distention.
Diagnosis
Complete blood count and smears
Blood culture
Urine culture
Lumbar puncture
Chest radiography
Radiograph of abdomen
Radiograph of bone joint
Treatment:
Systemic antibiotics
Transfer the newborn to a special care unit
Provide appropriate supportive
SPECIFIC INFECTIONS
PNEUMONIA
etiology may be congenital or acquired
Transmission of congenital infections may be
either transplacental or via the birth canal.
Clinical features: respiratory distress preceded by
lethargy, apnea, refusal of feeds, vomiting and
temperature instability.
Diagnosis is by chest radiograph and culture of
blood and tracheal aspirate.
Treatment is by appropriate antibiotics and
supportive therapy for respiratory distress.
MENINGITIS
Meningitis is the inflammation of the meninges
Features: The onset usually in the first week, is
gradual with temperature instability, fever, bulging
anterior fontanelle, high pitched cry or excessive
crying, poor feeding, vomiting and convulsions.
diagnosed by lumbar puncture.
It requires 21 days of treatment with
intravenous antibiotics. Broad spectrum
antibiotics like ceftazidime and cefepime
are given.
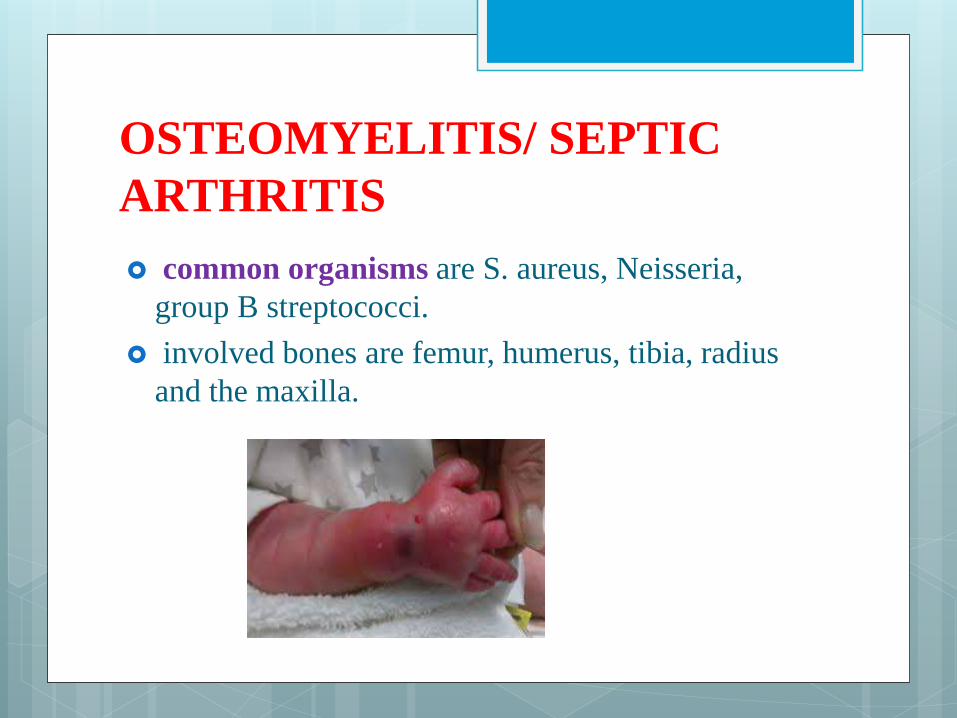
OSTEOMYELITIS/ SEPTIC
ARTHRITIS
common organisms are S. aureus, Neisseria,
group B streptococci.
involved bones are femur, humerus, tibia, radius
and the maxilla.
Presentation is with fever, bone or joint
tenderness. Radiograph of the appropriate area is
taken to confirm the diagnosis.
Treatment: Septic arthritis may require aspiration
of joint and surgical drainage. Antibiotic treatment
should be for 6 weeks. The prognosis is usually
good.
URINARY TRACT INFECTION
Bacteria may signal generalized sepsis with
hematogenous spread to the kidney
Features: Occasionally kidneys may be enlarged
and palpabe. In all neonate with poor weight gain
inspite of adequate intake of feeds, urine analysis
and culture must be done.
Common organisms are E.coli, Klebsiella and
enterococci.
Diagnosis is by urine culture.
Treatment: cephalosporin and aminoglycoside
until antibiotic sensitivities are obtained. A repeat
culture should have no growth after 48 to 72 hours
of therapy. Until the diagnosis is treated, oral
antibiotic prophylaxis with trimethoprim can be
given in the initial 10 to 14 days.
TETANUS NEONATARUM
Etiology:
Caused by infection by clostridium tetani
Contamination and infection of the umbilical
stump at the time of cutting the cord is an
important cause.
Lack of active immunization with TT contributes
high incidence
Clinical features:
Common onset of symptoms is 5-15 days
It does not manifest during first two days of life
and is rare after two weeks of life.
The infant keeps mouth slightly open due to pull
as a spasm of the muscles of the neck but reflex
spasm of massesters is invoked on trying to
open mouth during feeds.
Reflex spasm of pharyngeal muscles leads to
dysphasia and choking during feeding.
During handling and touching, lock jaw or
trismus is followed by spasm of the limbs.
The usual flexed posture of the baby is replaced
by generalized rigidty and opisthotonous in
extension
The spasm of larynx and respiratory muscles is
associated with apnoea and cyanosis
The spasm is characteristically induced by
stimuli of touch, noise and bright light.
Frequent muscular spasms leads to fever,
tachycardia and tachypnoea
NEONATAL SEPSIS
Neonatal sepsis is the infection in blood that occurs
in an infant younger than 90 days old. Early-onset
sepsis is seen in the first week of life. Late-onset
sepsis occurs between days 8 and 89.
Neonatal sepsis is the clinical syndrome of
bacterimia characterized by systemic signs and
symptoms of infection in the first month of life.
Classification
Early- onset neonatal sepsis
Late- onset neonatal sepsis
Etiology and risk factors
Early-onset neonatal sepsis most often appears
within 24 hours of birth. The baby gets the infection
from the mother before or during delivery.
Babies with late-onset neonatal sepsis get infected
after delivery. The following increase an infant's risk
of sepsis after delivery:
Having a catheter in a blood vessel for a long time
Staying in the hospital for an extended period of time
Clinical manifestations
Body temperature changes
Breathing problems
Diarrhea
Low blood sugar
Reduced movements
Reduced sucking
Seizures
Slow heart rate
Swollen belly area
Vomiting
Yellow skin and whites of the eyes (jaundice)
Diagnosis Blood culture
C-reactive protein:.
Complete blood count (CBC)
Micro ESR: 13-15 mm is abnormal
A lumbar puncture (spinal tap
If the baby has a cough or problems breathing, a chest x-ray will be taken.
Urine culture tests
serum procalcitonin polypeptide
immunologic studies
Treatment
Babies in the hospital and those younger than 4 weeks
old are started on antibiotics before lab results are back.
(Lab results may take 24-72 hours.)
Older babies may not be given antibiotics if all lab
results are within normal limits. Instead, the child may
be followed closely on an outpatient basis.
Babies who do require treatment will be admitted to the
hospital for monitoring.
Antibiotics according to the culture sensitivity reports.
Complications
Disability
Death
Prevention
Preventive antibiotics may be given to pregnant
women who have chorioamnionitis, Group B
streptococcus, or who have previously given birth
to an infant with sepsis due to the bacteria.
Preventing and treating infections in mothers,
providing a clean birth environment, and
delivering the baby within 24 hours of rupture of
membranes, where possible, can all help lower the
chance of neonatal sepsis.
NURSING MANAGEMENT Policy guidelines:
Handwashing:
Housekeeping routines:
Disinfection of equipments:
Procedures:
Surveillance of bacterial flora:
Fumigation
Isolation policies
Prevention of injuries
NURSING DIAGNOSES
Infection related to presence of microorganism in the body
Hyperthermia or hypothermia related to infectious process
Impaired skin integrity related to presence of lesions
Delayed growth and development related to inadequate feeding and presence of infection.
Impaired parenting related to separation secondary to admission in the NICU.
Parental anxiety related to disease condition of the newborn
Impaired gas exchange related to immaturity of the lungs and presence of respiratory infections
Impaired tissue perfusion related to lack of oxygenation secondary to accumulated secretions incase of respiratory infections.
Ineffective airway clearance related to accumulation of secretions due to respiratory infections.
Risk for fluid and electrolyte imbalance related to poor feeding
Thank you