Embed Size (px)
Citation preview

Hypoglycemia, Infant of a Diabetic Mother
Dr. Kalpana MallaMD Pediatrics
Manipal Teaching Hospital
Download more documents and slide shows on The Medical Post [ www.themedicalpost.net ]

Karlsen, 2006
Preparation for Birth
• Newborn’s blood glucose 60-70 % of maternal level falls during first 24 hrs (lowest at 3 hrs)transient rise during next 24 hrs falls again at 3-4 days stable

What is Normal?
• Defining a normal glucose level remains controversial – 50 – 110 mg/dl (Karlsen, 2006)
– > 40 mg/dl (Verklan & Walden, 2004)
– > 30 term, > 20 preterm (Kenner & Lott, 2004)
– > 45 mg/dl (Cowett, R. as cited by Barnes-Powell, 2007)

Incidence of Hypoglycemia
• Incidence = 1- 5/1000 live births– Normal newborns – 10% if feeding is delayed for
3-6 hours after birth – At-Risk Infants – 30%
• LGA – 8%• Preterm – 15%• SGA – 15%• IDM – 20%
McGowan, 1999 as cited by Verklan & Walden

Hypoglycemia
Definition: Blood glucose < 40mg/dl (< 2.2 mmol / L)at any time regardless of gestational age**Normal glucose level 30-60mg/dl (1.7-
3.3mmol/L)** Target 1st D >40 mg/dl > 40-50 mg/dl thereafter

• Incidence - 8.1% of term LGA 14.7 % of SGA

ETIOLOGY
Increased utilisation of glucose- - Infant of diabetic mothers- LGA babies- Erythroblastosis fetalis- Beckwith-Weidemann syndrome- Insulin producing tumors- UA catheter- used to infuse glucose - After exchange transfusion

Decreased stores or decreased production
• Prematurity• IUGR• Decreased calorie intake• Delayed onset of feeding

Increased utilization/decreased production
• Perinatal stress - Sepsis- Shock - Asphyxia- Hypothermia- RDS
• Defects in CHO metabolism
- glycogen storage disease - galactosemia

• Endocrine causes- Adrenal insufficiency- Glucagon deficiency- Epinephrine ” ”- Congenital
hypopituitarism- Hypothalamic
deficiency
• Defects in amino acid metabolism
- MSUD- Tyrosinemia, etc• Others: - Polycythemia - Maternal use of drugs - After exchange
transfusion

Causes
1. Decreased production/store - Preterm , IUGR 67%, LGA 38% - Inadequate intake2. ↑utilization/↓production - Perinatal stress - Septicemia, birth asphyxia, Hypothermia - Defect in CHO metabolism- IEM - Endocrine defic - adrenal insufficiency - cong hypopituitarism - Polycythemia

Causes3. Increased utilization of glucose -
hyperinsulinism - I/O diabetic mother - Erythroblastosis - Beckwith –Weidmann syndrome - Abruptly stopping high –glucose infusions - Insulin producing tumors- islet cell adenoma

SYMPTOMS• Asymptomatic• Lethargy, apathy and limpness • Apnea• Cyanosis• Weak or high pitched cry• Seizures, coma• Poor feeding, vomiting• Tremors, jitteriness or
irritability

DIAGNOSIS• Reagent strips – Glucostix - Confirmatory lab test is
required- Serial measurements for those
having symptoms
• Hypoglycemia lasting > a week require endocrine work up -insulin, GH, cortisol, ACTH, T4, glucagon, amino acids and urine for ketones, reducing substance, amino acids and organic acids

MANAGEMENT• Well neonates who are at risk –
Monitor/ feed• Symptomatic- IV 10% dextose 2-
5ml/kg. Follow this by infusion 8mg/kg/min recheck after 30 min and hourly until stable. Increase infusion as required.
• Other therapy- Hydrocortisone, glucagon, Epinephrine, diazoxide and growth hormone

Infant of diabetic mother

Infants of Diabetic Mothers
**Babies born to diabetic or gestational diabetic mothers
• 1st trimester------diabetic embryopathy• Last trimester---------macrosomia• Birth weight > 4000 g - 90th percentile GA

Introduction:
• Gestational diabetes (GDM): defined as carbohydrate intolerance of variable severity first diagnosed during pregnancy
• Affects 3 % of all pregnancies• Risk factors for GDM: - advanced maternal age - multifetal gestation - increased BMI - family h/o DM

Hypoglycemia
• Pedersen Hypothesis– Maternal hyperglycemia – Fetal hyperglycemia– Fetal b-cell hyperplasia– Neonatal hyperinsulinemia

Maternal Hyperglycemia
• Dose and time dependent• Post implantation rat embryo 100% teratogenic
dose 950 mg/dl D-glucoseDay 10 primary neural tube defectDay 11 cardiac defectsDay 12 no defects

Fetal Hyperglycemia
• 1-2 hours of fetal hyperglycemia can have detrimental effects
• insulin secretion– Storage of excess nutrients macrosomia– Post natal hypoglycemia

IDM – Effects on Fetus
• Glucose crosses the placenta
• Insulin does not cross the placenta
• Results – fetus produces own insulin in the presence of elevated glucose from the mother

IDM – Risks > general population
• Birth injury is doubled • C/S is tripled• NICU admission is quadrupled• Stillbirth is x 5 greater• Congenital anomalies are x 2 – 5 greater

Congenital Malformations• Overall incidence---5 to 9%
– 2-3 fold higher than general population– Predominantly with IDDM
• Malformations of CNS seen most often• Diversity-No malformation considered
pathognomonic

Congenital Malformations
• No increase in major congenital malformations among offspring of– Diabetic fathers– Prediabetic women– GDM after first trimester

Congenital Malformations
Skeletal/CNS• Caudal regression syndrome
not considered pathognomonic occurs 600 x more frequently among IDDM
• Neural tube defects • Microcephaly

Caudal Regression Syndrome• Spectrum of malformation
– cessation of growth of rostral portion of spinal cord
– abnormal neural, muscular, skeletal and vascular components
Caudal Regression with limbsintact but malformed
SirenomeliaAbsence of hind limbs, external genitalia, anus and rectum; Potter sequence secondary renal agenesis

Congenital Malformations
Cardiac• Transposition + VSD• Ventricular septal defect • Coarctation + VSD or PDA• Atrial septal defect• Hypertrophic Cardiomyopathy

Congenital Malformations
Renal • Hydronephrosis• Renal agenesis• Ureteral
duplication

Congenital Malformations
GI• Duodenal atresia• Anorectal atresia• Small left colon
syndrome

Perinatal and Neonatal Complications
• Disorders of fetal growth• Intrauterine and perinatal asphyxia• Hypoglycemia• Respiratory distress syndrome

Macrosomia• Birth Weight > 4000 g or > 90th %-ile• Incidence 15 to 45% among IDM• Increased rate of C-section• Birth Trauma
® shoulder and body dystocia® brachial plexus injury® facial nerve injury® asphyxia® abdominal trauma

Pathogenesis • Maternal hyperglycemia → Fetal
hyperglycemia → Leads to islet cell hyperplasia → Fetal hyperinsulinemia
↓ ↓A) Prenatal: ↑wt of placenta• Insulin acts as an anabolic hormone for
fetal growth. Organomegaly -not brain/kidney

• Myocardial hypertrophy• Extramedullary hemopoesis• Hyperinsulinism---acidosis----still birthB) Post natal:• Hypoglycemia 1-3hrs (lack of maternal
glucose supply + Persistent hyperinsulinemia

Problems
• Antenatal :• Polyhydramnios• Pre-eclampsia• Pyelonephritis• Previous H/O still birth, premature
delivery, abortion

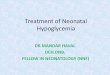
Shoulder Dystocia
www.drsarma.in 39
Erb’s palsy

Problems• Natal :• Fetal macrosomia-difficult delivery,
birth injury - Erb’s palsy, Clavicle fracture, Phrenic N palsy
• Sudden unexpected fetal death –ketoacidosis
• Usually LSCS • Large placenta• Premature delivery• TTN

Problems (post natal)
• Hypoglycemia- within 1-3 hrs of birth IDM -75% get in 1st 24 hr GDM -25% get in 1st 24 hr
• Hypocalcemia 24-72 hrs of birth(50%)• Polycythemia• Hyperbilirubinemia

Problems (post natal) • Respiratory distress – HMD Large
baby( LFD)
• Delayed passage of meconium delayed devl of left colon
• Hypomagnesemia –related with maternal hypomagnesemia with DM

Associated Cong anomalies
• 3-4 times more common• Hyperglycemia induced teratogenicity1. CNS- neural tube defects- Anencephaly, holoporencephaly,
meningocele2. Vertebral –caudal regression syndrome –
lumbo sacral agenesis3.Renal – R. vein thrombosis, renal agenesis hydronephrosis

4.Cardiac
• 5 times more common—
• Transient hypertrophic subaortic stenosis
• Septal hypertrophy,• Hypertrophic
cardiomyopathy• CCF

Associated Cong anomalies
4. Cardiac….. – VSD, ASD, Co.Aorta, TGA
5.Gastrointestinal - Small left colon syndrome-abdominal distension, Duodenal or anorectal atresia

Verklan & Walden, 2004
Signs & Symptoms of Hypoglycemia
• Jitteriness• Irritability• Hypotonia• Lethargy• High-pitched cry• Hypothermia
• Poor suck• Tachypnea• Cyanosis• Apnea• Seizures• Cardiac arrest

On examination
• Large , plump, Plethoric, features of preterm
• Hypotonic, hypothermia
• Hypertrichiosis- hairy pinna

On examination
• Hypoglycemia-jitteriness, lethargy, cyanosis, poor feeding, vomiting, tremor, seizures Apnoeic spells
• Tachypnia-HMD,CCF• Asociated cong anomalies +

On examination
• Polycythemia— if PCV>65% • signs of hyperviscosity —jitteriness,
tachypnoea, cyanosis ,seizures, poor feeding. At times RV thrombosis, hyperbilirubinemia

DIAGNOSIS
Babies at high risk should be screened within the first 1-2 hours
reagent strips-measure whole blood glucose-15% lower than plasma levels
Confirmatory blood sugar determination is required- and the blood should taken to the lab immediately since glucose levels can fall 18 mg/dl/hour in the blood sample that awaits analysis
Septic screen

Monitoring in IDM:
• Check blood glucose level at 1,2,3,6,12,24,26 and 48 hrs
• Hematocrit at 1 and 24 hrs• Calcium levels if baby appears jittery or sick• Bilirubin if clinically jaundiced

Investigations
• C BC-hct • Blood sugar-1st hr of birth ,then
2,3,6,8,12,24,48th hrs of birth• S.calcium, S. magnesium• CXR – Cardiomegaly 30% HF- 10% Features of HMD• USG-renal, gut anomalies• ECHO

Management: mother
• 1. Proper control of maternal DM- - No Oral Hypoglycemics- due to
teratogencity/intractable hypoglyce - Insulin to keep BSL<120mg• Assessment of fetal maturity—signs of
lung maturity—L:S ratio >3.5 (normally>2)
• Elective LSCS

Treatment
• Asymptomatic- breast feeds/formula- repeat blood test in one hour- if glucose does not come up-aggressive therapy is required
• IV therapy-indications - Symptomatic - Inability to tolerate oral feeds - Glucose level < 25 mg% - oral feedings do not maintain glucose levels

IV Dextrose:
• 2 ml/kg of 10%dextrose• For symptomatic hypoglycemia- 10 %
dextrose 4 ml/kg• Continuing treatment- 6-8mg/kg/min• Recheck 20-30 min and hourly until stable• Additional bolus infusion-2 ml/kg of 10%
dextrose• If glucose is stable-feeding reintroduced
and glucose infusion tapered

continued
• Increase glucose infusion upto 12-15 mg/kg/min• In these cases-hydrocortisone 10 mg/kg/day may be
used• Glucagon (25-300 micrograms) -may be used in
neonates with good glycogen stores- temporary measure-until IV access is available
• Other drugs- diazoxide/verapamil-refer to a tertiary centre

hypoglycemia
10 % dextrose 2 ml/kg glucose infusion 6 mg/kg/min gRBS 20-30 min still low 10 % dextrose 2 ml/kg glucose infusion 8 mg/kg/mingRBS still low hydrocortisone 10 mg/kg/d
gRBS still low glucagon IM (0.025-0.3 mg/kg)
diazoxide 2-5 mg/kg q8hr PO
epinephrine/ GH subtotal pancreatectomy

Management: baby
1. Asymptomatic & normoglycemic: Early feeding Frequent BSL2.Asymptomatic & Hypoglycemic: Frequent feed IV glucose 10% 2ml/kg bolus

Management: baby
3.Symptomatic & hypoglycemia If symptoms – 4ml /kg 10% glucose IV followed by 10% glucose drip 8mg
(.08ml /kg / m for 2 days - monitor BSL 2 hrly until >40mg/dl ,then monitor 4-6 hrly – Then gradually decrease rate if stable for 24-48 hrs

If recurs
• Hypertonic glucose 12-20% IV hydrocortisone oral prednisolone IM GH• If hyperinsulinemic hypoglycemia oral diazoxide oral octretide

Management: baby
• Treat complications• Treat infections• If severe polycythaemia—partial ET
with plasma/saline

Complications - DM
1 Acute complications
2. Intermediate complications
2.Long-term complications
3.Complications by associated autoimmune diseases.

Complications - DM
• Acute complications - - Hypoglycemia - Hyperglycemia (DKA)

Intermediate complications
• Lipoatrophy – insulin use • Limited joint mobility – flexion
contractures of Metacarpophalangeal & proximal interp jt – inability to approximate palmer surface of hands – prayer sign
• Growth failure - poor metabolic control Mauriac syndrome - extreme growth failure

Intermediate complications
• Delayed sexual maturity –
• Intellectual development – insult to developing brain by hypo or hypryglycemia

Long-term complications
• Rare in childhood– Eye - Retinopathy , Cataracts – Nephropathy - Progressive renal failure– Neuropathy, both peripheral and autonomic – Early coronary artery disease– Peripheral vascular disease, Hypertension – Increased risk of infection

DKA - pathophysiology
Insulin deficiency→ Hyperglycemia
↓
Osmotic diuresis & electrolyte loss
↓
Decreased volume →dehydration
↓
Metabolic acidosis

DKA - pathophysiology
Insulin deficiency→ lipolysis in peripheral tissue ↓ ↓
Glucagon, cortisol, GH →→ FFA ↓ liver/kidney
↓
ketone bodies

Risk Factors - DKA
• ↓insulin therapy• Infections• Trauma/burns• Surgical procedures• Steroid therapy• Any other stress

Classification of DKAVenous blood
Mild Moderate Severe
CO2 mEq/L(20-28)
16-20 10-15 <10
pH(7.35-7.45)
7.25-7.35-Oriented -Alert but -Fatigued
7.15-7.25- Kuss .resp- Oriented- Sleepy but- Arousable
<7.15-Resp –Kussmal / Depressed- Sensorium -Depressed to coma

Diagnosis
• C/F• Assess for – State of consciousness - Severity of dehydration - Severity of acidosis -Precipitating factors

Lab
• Ketonuria• Ketonemia• Blood glucose->250mgldl• pH < 7.3• HCO3 < 20 mEq/L

Management
Correction of - Dehydration - Dyselectrolytemia - Start insulin

Treatment protocol
• 1st Hr- 10-20 ml/kg 0.9 % NaCl or R/L• Insulin drip @ 0.05 - 0.1u / kg /hr ( regular)- NPO- Repeat bolus till dehydration corrected- Check Neurologic status- Have Mannitol at bedside (C. Edema)

Treatment protocol
• Repeat ECG – 6-8 hrly• Electrolytes , pH 2-4 hrly- Monitor I/O, monitor blood glucose
hrly

Treatment protocol
• 2nd hr till DKA resolution –maintenance fluids
• 0.45% NaCl + cont insulin drip + 20 mEq/L potassium
• Blood sugar < 250mg/dl (14mmol/L) - add 5% dextrose to infusate

Treatment protocol
• Correction of acidosis by bicarbonate is required only if pH < 7
• When blood glucose –normal give S/c insulin and stop insulin drip 30 min after this

Treatment protocol
• 0.5-0.7units/kg (IA) insulin + 0.1 units/kg regular insulin SC at 4-6hrly
• Adjust dose daily until satisfactory glycemic control is achieved
• Injection site – rotated to avoid lipohypertrophy• Posterior .upper extremity, anterior
thigh, buttocks, anterior abdominal wall

Long-term complications
Diabetic retinopathy – Within 5 years of onset of diabetes. – 80% with IDDM develop retinopathy.
Diabetic nephropathy – Peak incidence is in post adolescents, 10-15
years after diagnosis– 30% with IDDM.

Long-term complications
Diabetic neuropathy• Autonomic changes - 40% of IDDM
MI and stroke - with IDDM have twice the risk
Atherosclerosis - with IDDM have 4 times risk

Follow up
– Growth assessment
– Injection site examination
– Retinoscopy or other retinal screening
– Blood pressure

Follow up
– Examination of hands, feet, and peripheral pulses, signs of limited joint mobility, peripheral neuropathy, and vascular disease
– Evaluation for signs of associated autoimmune disease
– Urine examination for microalbuminuria

Tips&
Terminologies

Phases of diabetes
• Development of clinical symptoms
• Honeymoon phase
• Relapse
• Total diabetes - irreversible

Honeymoon period
• Phase of remission after initial stabilization
• Due to residual β-cell function –residual insulin secretion
• 75% go into this phase • 5% go into complete remission• Phase – variable ( wks/months /1-2 yrs)

Somogyi phenomenon
• Hypoglycemic episode followed by rapid onset of hyperglecemia
• Due to counter regulatory hormones in response to insulin induced hypoglycemia
• Also described as hypoglycemia begetting hyperglycemia

Dawn phenomenon
• Hyperglycemia at 5-9 am without preceeding hypoglycemia
• Due to Waning effects of biologically available insulin & nocturnal surges of GH
• Normal event

Distinguish ( Somogyi& Dawm P)
• Blood glucose at 3,4,7 am • Dawn P - >80mg/dl in 1st sample (3am)
and markedly higher in last sample & am-↑ evening dose or delay evening dose by 2-3 hrs
• Somogyi P – ≤ 60mg/dl in 1st sample(3am) –rebound hyperglycemia at 7 am -↓ evening dose or delay insulin at 9 pm

Brittle diabetes
• Control of blood glucose fluctuates widely & rapidly despite frequent adjustment of dose of insulin
• Somogyi & dawn phenomenon – most common causes

Thank youDownload more documents and slide shows on The
Medical Post [ www.themedicalpost.net ]