Embed Size (px)
Citation preview

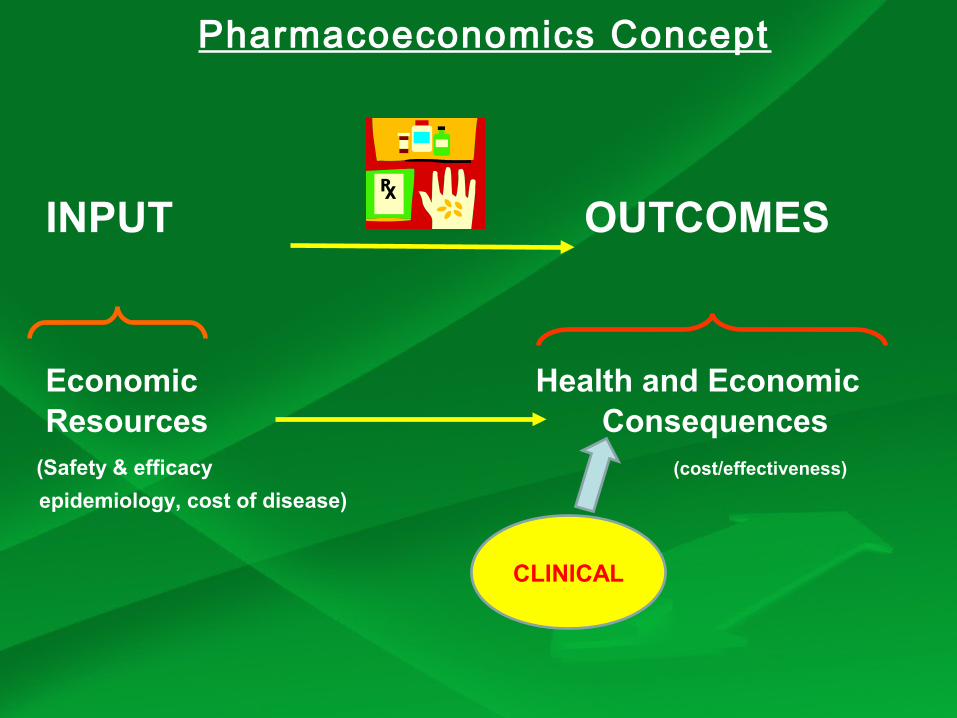
Pharmacoeconomics Concept
INPUT OUTCOMES
Economic Health and Economic Resources Consequences
(Safety & efficacy (cost/effectiveness)
epidemiology, cost of disease)
CLINICAL
Domains to perform economic evaluations
Economic evaluations can be performed 1. To analyze efficacy and effectiveness studies. 2. To study the costs associated with adverse effects
(eg.: neutropenia, nausea, and vomiting). 3. To study palliative therapies.
4. To study treatments in various settings (i.e., inpatient vs. outpatient care). 5. In evaluating diagnostic techniques, cancer screening programs, primary and secondary therapy.
Why is there an increase in health expenditures?(DATE)
Demand [Western culture (patient autonomy, family and informal care)]
Aging (geriatric longevity)
Technologies– Broader indication as technologies become less invasive– Half way technologies (no cure, generate a lot of care)– Little substitution of innovations with existent technologies
(co-existence)
Economic Growth
Why are prescribing costs increasing???
Demographic changes in the population that have resulted inan aging population which is living longer and has greater
pharmaceutical needs.
Health screening programmes and improved diagnostic techniques that are uncovering previously non-identified
diseases which subsequently require treatment.
The marketing of new medicines that offer more effective and less toxic alternatives to existing agents, and which are
invariably more expensive.
Medicines being used in preference to invasive treatments.
The use of existing agents becoming more widespread as additional indications for their use are found.
Pharmacoeconomic research, evaluation and decision making
Pharmacoeconomic research is the process of identifying, measuring and comparing the costs, risks and benefits of various alternatives (programs/services/therapies) and determining which alternative produces the best health outcome for the resource invested.
Pharmacoeconomic evaluation provides us with the methodology to determine those treatment options, which will yield the maximum health gain per unit of currency spent.
Through pharmacoeconomic decision making, hospitals will be able to make decisions about using expensive drugs and supportive care agents when drug budgets are shrinking and drug costs are rising.
This involves weighing the cost of providing a pharmacy product or service against the consequences (outcomes). This is done by initially using all the alternatives (products or service), to determine which alternative yields the optical outcome per unit of currency spent.
This information can assist clinical decision makers in choosing the most cost-effective treatment options.
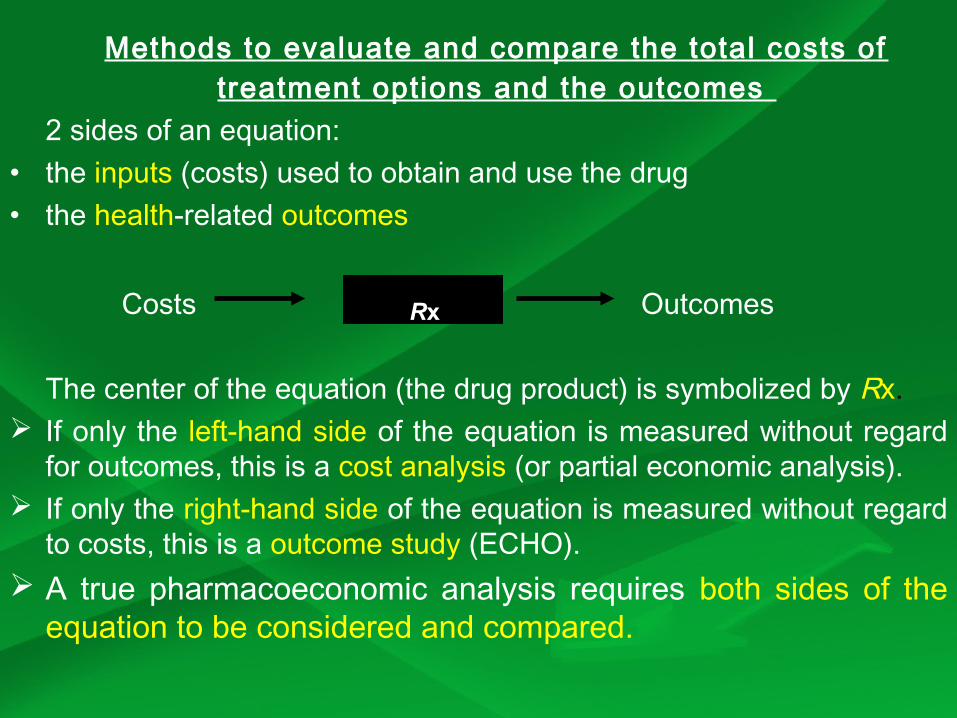
Methods to evaluate and compare the total costs of treatment options and the outcomes
2 sides of an equation: • the inputs (costs) used to obtain and use the drug • the health-related outcomes
Costs Outcomes
The center of the equation (the drug product) is symbolized by Rx. If only the left-hand side of the equation is measured without regard
for outcomes, this is a cost analysis (or partial economic analysis). If only the right-hand side of the equation is measured without regard
to costs, this is a outcome study (ECHO). A true pharmacoeconomic analysis requires both sides of the
equation to be considered and compared.
Rx
Scenario
You have a headache and a fever, your bones are aching and your nose feels slightly blocked. You are still able to do all the things you usually do but, are more tired than usual. The symptoms started to appear four days ago, and were slightly worse when you woke up this morning.
Which would you prefer?Option 1 Option 2
Management Self care GPAvailability / Span 1 hour 1 or 2 daysCost Less High
Or DO NOTHING
For the symptoms presented, General preference will be for doing something (rather than ‘do nothing’).
Relative preferences for type of management will be
• Self-care
• Community pharmacy
• GP consultation
• Practice nurse
• Complementary medicine

Reasons for practising self-care
• Faster treatment/ relatively easier access to medicine.
• Use of complementary treatments
• Avoidance of unwanted treatments
• Feelings of control/independence
• Advice from friends, relatives or media
• Perception that condition is self-inflicted
• Belief that GP will be of limited help
• Does not want to waste Dr’s time
Reasons for NOT practising self-care
• Lack of knowledge
• Chance of missing an important condition
• Chances of drug interactions
• Chance of making things worse
• Belief that nothing can help (stoicism).
• No advice from Doctor/pharmacist
• Belief that only medical help will work
The ‘Influencing factors’
Type of management (self-care, GP, pharmacy, practice nurse, do nothing)
Time for treatment (the time you have to wait for an appointment, travel time and time taken to get any treatment) (0,1,5 hours, 1,2,5 days)
Cost (travel costs and the cost of any treatment e.g. any consultation fee, over-the-counter medicines, complementary remedies etc.)
Costs can be described in many ways
• Cost / unit (eg.: cost/tablet, cost/vial)• Cost / treatment• Cost / person• Cost / person / year• Cost / case prevented• Cost / life saved• Cost / DALY (disability-adjusted life year)
Patient’s Perspective
Patient perspective is paramount because patients are the ultimate consumers of health care services.
Costs from the perspective of patients are essentially what patients pay for a product / service (the portion not covered by insurance).
When assessing the impact of drug therapy on QoL consider if a patient will pay ‘out-of-pocket expenses’ for a health care service.
Consequences, from a patient’s perspective, are the clinical effects (both positive and negative), of a program or treatment alternative.
Provider’s Perspective
Costs from the provider’s perspective are the actual expense of providing a product or service, regardless of what the provider charges.
Providers can be hospitals, managed-care organizations (MCOs), or private-practice physicians.
From this perspective, direct costs such as drugs, hospitalization, laboratory tests, supplies, and salaries of health care professionals may be identified, measured, and compared.
Indirect costs may be of less importance to the provider.
Payer’s Perspective
Payers include insurance companies, employers, or the government. From this perspective, costs represent the charges for health care products and services allowed, or reimbursed, by the payer.
The primary cost for a payer is of a direct nature. However, indirect costs, such as lost work days and decreased productivity, also may contribute to the total cost of health care to the payer.
When insurance companies and employers are contracting with MCOs or selecting health care benefits for their employees, then the payer’s perspective should be employed.
Societal Perspective
The perspective of society is the broadest of all perspectives because it is the only one that considers the benefit to society as a whole.
Theoretically, all direct and indirect costs are included in an economic evaluation performed from a societal perspective.
Costs from this perspective include patient morbidity, mortality and the overall costs of giving and receiving medical care.
An evaluation from this perspective also would include all the important consequences an individual could experience. In countries with nationalized medicine, society is the predominant perspective.
Costs
Once a perspective is chosen, the costs and consequences associated with a given product or service may be identified and measured using pharmacoeconomic methods.
A comparison of two or more treatment alternatives should extend beyond a simple comparison of drug acquisition costs.
Health care costs or economic outcomes can be grouped into several categories: direct medical, direct non medical, indirect non medical, and intangible .
The costs that are identified, measured, and ultimately compared vary depending on the perspective.
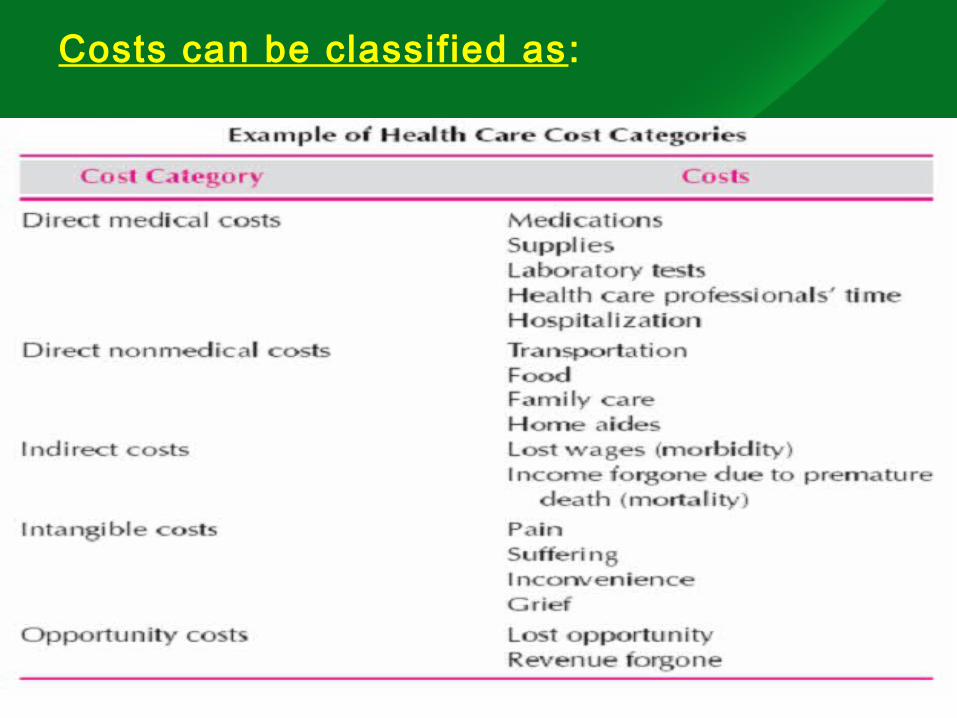
Costs can be classif ied as:
Direct medical costs
Direct medical costs are the costs incurred for medical products and services used to prevent, detect, and/or treat a disease.
Direct medical costs are the fundamental transactions associated with medical care that contribute to the portion of gross national product spent on health care.
Egs. : drugs, medical supplies and equipment, laboratory and diagnostic tests, hospitalizations, and physician visits.
Direct medical costs can be subdivided into fixed and variable costs.
FIXED COSTS Fixed costs are those which are independent of the number of units
of production and are essentially ‘overhead’ costs (e.g., heat, rent, electricity) that are not readily influenced at the treatment level and thus remain relatively constant.
For this reason, they are often not included in most pharmacoeconomic analyses.
VARIABLE COSTS dependent on the number of units of productivity which change as a
function of volume. Egs.: costs of medicines consumption, fees for professional services,
and supplies. As more services are used, more funding must be used to provide
them. Average costs are the simplest way of valuing the consumption of
health care resources.
Direct Non medical Costs
Direct non medical costs are any costs for non medical services that are results of illness or disease but do not involve purchasing medical services.
These costs are consumed to purchase services other than medical care and include resources spent by patients for transportation to and from health care facilities, extra trips to the emergency department, child or family care expenses, special diets, and various other out-of-pocket expenses.
Indirect Non medical Costs Indirect nonmedical costs are the costs of reduced
productivity (e.g., morbidity and mortality costs)
Indirect costs are costs that result from morbidity and mortality and are an important source of resource consumption (especially from the patient’s perspective).
Morbidity costs are costs incurred from missing work (i.e., lost productivity), whereas mortality costs represent the years lost as result of premature death.
To estimate indirect costs, two techniques typically are used: (1) Human Capital (HC) and (2) Willingness-to-pay (WTP) methods.
HC APPROACH The HC approach attempts to value morbidity and mortality
(primarily wages and productivity) losses based on an individual’s earning capacity using standard labor wage rates.
This approach raises an ethical dilemma because the value of a life is related directly to income.
WTP APPROACH Using the WTP approach (contingent valuation), the indirect and
intangible aspects of a disease can be valued.
Patients are asked how much money they would be willing to spend to reduce the likelihood of illness.
However, the values obtained through this method may be unreliable because of the substantial differences in valuations of life that result from the subjective nature of this approach.
INTANGIBLE COSTS
Intangible costs are those of other non financial outcomes of disease and medical care.
Egs.: pain, suffering, inconvenience and grief.
These are difficult to measure quantitatively and impossible to measure in terms of economic or financial costs but are sometimes captured in measures of quality of life.
In pharmacoeconomic analyses, frequently intangible costs are identified but not quantified formally.
Opportunity Costs
Opportunity costs represent the economic benefit forgone when using one therapy instead of the next best alternative therapy.
The concept of opportunity cost is at the centre of economics and identifies the value of opportunities which have been lost by utilizing resources in a particular service or health technology.
Therefore, if a resource has been used to purchase a program or treatment alternative, then the opportunity to use it for another purpose is lost.
Opportunity cost recognizes that there are limited resources available for utilizing every treatment and therefore the rationing of health care is implicit in such a system.
THE END





























