Embed Size (px)
Citation preview

GOOD MORNING

NECK DISSECTION
ByDr.Rehana sultanaIIIrd yr post graduate(OMFS)

Contents • Introduction • History• Surgical anatomy• Levels of lymph nodes• TNM staging • Classifications• Definitions of types of dissections• Surgical procedure• Complications• Algorithm • Conclusion• References

Some simple questions…..
• What is neck dissection??• Why it is done??• When it has to be done??• Who developed it??• Where it is done??• How it is done??• What are the structures involved??• Any complications??

Introduction
• Cervical node metastasis is the single most important prognostic factor in head and neck squamous carcinomas.
• Cure rates drop in half when there is regional lymph node involvement

Definition
• The term neck dissection refers to a surgical procedure in which the fibrofatty contents of the neck are removed for the treatment of cervical lymphatic metastases

EVOLUTION • 1880 – Kocher proposed removing nodal metastases• 1906 – George Crile described the classic radical neck
dissection (RND)• 1933 and 1941 – Blair and Martin popularized the RND• 1953 – Pietrantoni recommended sparing the spinal accessory
nerves• 1967 - Bocca and Pignataro described the “functional neck
dissection” (FND)• 1975 – Bocca established oncologic safety of the FND compared
to the RND• 1989, 1991, and 1994 – Medina, Robbins, and Byers respectively
proposed classifications of neck dissections

ANATOMY • Skin:
– Blood supply:• Descending branches:
– The facial – The submental– Occipital
• Ascending branches– Transverse cervical– Suprascapular
– The branches perforate the platysma muscle, anastomose to form superficial vertically-directed network of vessels

• Platysma muscle:
– Wide, quadrangular sheet-like muscle
– Run obliquely from the upper part of the chest to lower face
– Skin flap is raised immediately deep to the muscle
– The posterior border is over or just anterior to IJV and great auricular nerve

• Sternocleidomastoid muscle:
– Differentiated from the platysma by the direction of its fibres
– Crossed by the EJV and the great auricular nerve from inferior to posterior deep to platysma
– The posterior border represent the posterior boundary of nodes level II - IV

OMOHYOID MUSCLE
• Inferior belly passes behind the sternocleidomastoid
• Superior belly lies close to the lateral border of the sternohyoid and inserted into the lower border of the body of the hyoid bone
• The central tendon of this muscle is held in position by a fascial sling derived from investing layer of deep cervical fascia and is prolonged down to be attached to the clavicle and first rib

• MARGINAL MANDIBULAR NERVE:
– Located 1 cm in front of and below the angle of the mandible
– Deep to the superficial layer of the deep cervical fascia
– Superficial to adventitia of the anterior facial vein

• Spinal Accessory nerve:
– Emerge from the jugular foramen medial to the digastric and stylohyoid muscles and lateral and posterior to IJV (30% medial to the vein and in 3 -5% split the vein)
– It passes obliquely downward and backward to reach the medial surface of the SCM near the junction of its superior and middle thirds, Erb’s point

• Trapezius muscle:
– Its anterior border is the posterior boundary of level V
– Difficult to identify because of its superficial position
– Dissect superficial to the fascia in order to preserve the cervical nerves

• Digastric Muscle: Posterior belly:– Originate from a groove
in the mastoid process, digastric ridge
– The marginal mandibular nerve lie superficial
– The external and internal carotid artery, hypoglossal and 11th cranial nerves and the IJV lie medial

• Brachial Plexus & Phrenic nerve:– The plexus exit between the
anterior and middle scalene muscles, pass inferiorly deep to the clavicle under the posterior belly of the omohyoid
– The phrenic nerve lie on top of the anterior scalene muscle and receive its cervical supply from C3 – C5

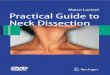
• Thoracic duct:
– Located in the lower left neck posterior to the jugular vein and anterior to phrenic nerve and transverse cervical artery
– Have a very thin wall and should be handled gently to avoid avulsion or tear leading to chyle leak

Hypoglossal nerve:
• Exit via the hypoglossal canal near the jugular foramen
• Passes deep to the IJV and over the ICA and ECA and then deep and inferior to the digastric muscle and enveloped by a venous plexus, the ranine veins
• Pass deep to the fascia of the floor of the submandibular triangle before entering the tongue

Anatomy of the vascularization of neck skin
• Kambic and Sirca 1967 stated that arterial supply is in a vertical direction.
• descending branches: facial and occipital artery
• ascending branches: transverse cervical and supraclavicular arterial branches .

The vasculature can be summarized into
• upper neck region - anterior to the angle of mandible - branches of facial and submental arteries.
• upper lateral neck - the area between ramus of mandible and the sternocleidomastoid muscle-Occipital and external auricular branches of external carotid .
• Lower half of neck - The transverse cervical artery and suprascapular artery
• Large platysma-cutaneous branches and branches of superior thyroid supplying the front middle portion of the neck.

LYMPH NODES OF HEAD & NECK
Conventionally divided into three systems
• Waldeyers internal ring• Superficial lymph node system (Waldeyers external ring)• Deep lymph node system (cervical lymph nodes proper)

Waldeyer’s ring
• Circular collection of lymphoid tissue within the pharynx at the skull base.
• Ring includes the adenoids, tubal and lingual tonsils, palatine tonsils, aggregates on the posterior pharyngeal wall.

Superficial nodal system• Drains the superficial tissues of
the head and neck.
• Two circles of nodes, one in the head and the other in the neck.
• In the head – nodes are situated around the skull base
• In the neck – submental, submandibular and anterior cervical nodes.

Deep lymph nodal system
Deeper fascial structures of the head and neck drain either directly into the deep cervical nodes or through the superficial system.
• A. junctional nodes• B. internal jugular nodes• C. spinal accessory nodes• D. Supraclavicular nodes• E. nuchal nodes• F. Deep medial visceral
nodes

Classification of lymphnode levels by Memorial Sloan-Kettering Cancer Center
The boundaries of each being defined by
surgically visible bones, muscles, blood
vessels or nerves.
Robbins KT, Medina JE, Wolfe GT, Levine PA, Sessions RB, Pruet CW. Standardizing neck dissection terminology. Official report of the academy’s committee for head and neck surgery and oncology. Arch Otolaryngol Head Neck Surg 1991;117:601–5.

Levels of lymph nodes

Draining areas

Spread of cancer in lymphatics
• Embolisation
• Permeation

T Classification
• T – Primary tumour :
• T x primary tumour that cannot be assessed.• T 0 No evidence of primary tumour.• T is Carcinoma in situ.
• T 1 Tumour 2 cms or less in the greatest diameter.• T 2 Tumour 2cms but not more than 4cms in the
greatest diamension.
• T 3 Tumour more than 4 cms in the greatest dimension.

T 4 a – Lip : Tumour invades through the cortical bone, inferior
alvoelar nerve, floor of the mouth or skin.T 4 a – oral cavity : Tumour invades through the cortical bone into the deep
extrensic muscles of the tongue ( genioglossus, hypoglossus, palatoglossus, styloglossus ) , maxillary sinus or skin of the face.
T 4 b – lip and oral cavity : Tumour invades the massetric space, pterygoid plates, skull
base or encases the internal carotid artery.

T staging

N staging

• Distant metastases – M
• M x – distant metastases that cannot be assessed.
• M 0 – No distant metastases.
• M 1 – distant metastases.

Staging
N0 N1 N2 N3
T1 I
T2 II T3
III
T4 IV

Impact of pattern of nodal metastasis on neck dissection
Level of nodal involvement Site of primary tumour
Submental(IA) Floor of mouth, lips and anterior part of tongue
Submandibular(IB) Retromolar trigone, glossopalatine pillars,lateral floor of mouth& anterior tongue
Jugulodigastric(II) Hypopharynx, base of tongue, tonsil, nasopharynx & larynx
Mid jugular(III) Hypopharynx, base of tongue, tonsil, nasopharynx & larynx
Lower jugular(IV) Thyroid, nasopharynx & hypopharynx
Supraclavicular(V) Lung, thyroid, gastrointestinal & genito urinary system
Posterior triangle(VI) Nasopharynx

Factors affecting nodal metastasis
• Anterior portions < posterior portions. • Young patients > older patients. • Risk of neck involvement by metastasis increases with an
increase in tumor size. • Perineural and perivascular invasion are associated with a
high risk of nodal metastasis. • Poorly differentiated tumors > well-differentiated tumors.

Assessment of cervical lymph nodes
• Computed tomography• Magnetic resonance imaging• Ultrasound
• Ultrasound guided fine needle aspiration cytology
• Radionuclide scanning• SPECT• PET
• Sentinel node biopsy• Lymphoscintigraphy

• PET scan showed the highest specificity (82%) while ultrasound had highest sensitivity (84%)
• Due to high number of small lymph node metastases from oral cavity carcinoma, the non-invasive neck staging methods are limited to a maximum accuracy of 76%
• Elective neck treatment should be mandatory for all patients with squamous cell carcinoma of the oral cavity

• Sentinel lymph node is defined as a lymph node to which a tumor first metastasizes
• SLNB if negative for metastases, lymph node dissection is not necessary.
• use in oral cancer – controversial
• One of the main problem of SLNB of oral cancer is skip metastasis in which the disease by passes level 1 and 2 nodes and goes directly to level 3-4
Sentinel node biopsy

When neck dissection has to be done?
• The incidence of metastatic disease for the upper aerodigestive tract varies widely, from 1-85%, depending on the site, size, and differentiation of the tumor.
• The rate of ipsilateral metastatic disease in patients with stage T3-T4 squamous cell carcinoma of the oral cavity, oropharynx, hypopharynx, or supraglottis is approximately 50%.
• The rate of bilateral or contralateral metastatic disease in these patients varies from 2-35%.
• 20 – 30 % of the malignancies of tongue metastasize to clinically undetectabe cervical nodes

Patterns of cervical lymph node metastasis from squamous carcinomas of the upper aerodigestive tract.
Am J Surg. 1990 Oct;160(4):405-9
• A consecutive series of 1,081 previously untreated patients undergoing 1,119 RNDs for squamous carcinoma of the head and neck was reviewed to study the patterns of nodal metastases.
• Predominance of certain levels was seen for each primary site. Levels I, II, and III were at highest risk for metastasis from cancer of the oral cavity.
• SOHND (clearing levels I, II, and III) for NO patients with primary squamous cell carcinomas is recommended

• For patients with clinical cervical lymph node metastases a therapeutic neck dissection is necessary and a modified
radical dissection is regarded as the safest option.
Management of the neck in patients with T1 and T2 cancer in the mouthBJOMS Vol 40, issue 6 .December 2004, Pages 494-500

•Excluding the hard palate and lip, approximately 30% of patients with oral cavity cancer will present with cervical metastases• Depth of invasion greater than 8 mm was associated with a 41% rate of occult metastasis.•Tumour depth > 5mm --- Increased risk of neck metastasis

Does No neck require treatment??
• The metastases rate to the neck from oral cancer is 34%.• Observation if probability is less than 20%• Elective neck dissection - >20 %• The lymph nodes at the highest risk of metastases from oral cavity
cancers are those at level I, II, III.• Contralateral neck dissection: The primary oral cancer is midline
,bilateral along the tip of tongue or approaches /crosses midline.

• The following surgical outline was suggested:– SCC oral cavity anterior to circumvalate papilla
• Supraomohyoid– SCC Oropharynx, larynx and hypopharynx
• level I- IV or level II-V– SCC with N+ nodes
• RND – SCC with 2-4 positive nodes or extracapsular spread
• RND and adjuvant therapyShah Cancer July 1;109-113: 1990

Goals
• Remove gross disease in patients with clinical evidence of nodal involvement (therapeutic neck dissection)
• Remove occult metastases in patients whose tumor characteristics make one suspicious of occult cervical metastases (elective neck dissection or END)

The definition of the different types of neck dissections were outlined in the 1991 classification :
1) The radical neck dissection is considered to be a standard basic procedure for cervical lymphadenopathy.
2) When one or more of the non lymphatic structures are preserved which otherwise are routinely removed during radical neck dissection then it is termed as modified radical neck dissection.

3) When the alteration involves preserving the 1 or more lymph node groups / levels routinely removed in radical neck dissection the it is termed as selective neck dissection.
4) When the alteration involves the removal of additional lymph node groups or non lymphatic structures relative to the radical neck dissection the procedure is called as extended radical neck dissection.

Classification 1991 classification
1. Radical neck dissection2. Modified radical neck
dissection3. Selective neck dissection a ) supra omohyoid b ) lateral c ) posterolateral d ) anterior4. Extended neck dissection
2001 classification
1. Radical neck dissection2. Modified radical neck
dissection3. Selective neck dissection Here each variation is
depicted by the term “ SND “ and the use of parentheses to denote the levels or sublevels removed
4. Extended neck dissection

Medina classification (1989)
– Comprehensive neck dissection• Radical neck dissection• Modified radical neck dissection
– Type I (XI preserved)– Type II (XI, IJV preserved)– Type III (XI, IJV, and SCM preserved)
– Selective neck dissection

Spiro’s three- tiered classification-1994
• Radical (4 or 5 levels resected)• Conventional radical neck dissection• Modified radical neck dissection• Extended radical neck dissection• Modified and extended radical neck dissection
• Selective (3 node levels resected)• Supra-omohyiod neck dissection• Jugular dissection (levels 11-1V)• Any other 3-node levels resected
• Limited (no more than 2 nodes levels resected)• Para tracheal node dissection• mediastinal node dissection

Radical neck dissection• Indications
– Extensive cervical involvement or matted lymph nodes with gross extracapsular spread and invasion into the SAN, IJV, or SCM
– Significant operable neck disease (N2a,2b,2c)– Access prior to pedicled flap reconstruction– Occult primary– lymphangioma, haemlymphangioma, residual branchial
cyst, fistula

Contraindications– Untreatable primary tumor– Patients unfit for tumor surgery– Distant metastasis– Inoperable neck disease– Significant bilateral neck disease

Extent:
Removes Nodal groups I-VSCM, IJV, XISubmandibular gland, tail of
parotid
PreservesPosterior auricularSuboccipitalRetropharyngealPeriparotidPerifacialParatracheal nodes

Preoperative Considerations1. Age and Sex of the patient2. Consent /any allergies/ lab reports/vital signs3. Location of the Primary4. Unilateral vs. Bilateral Neck Dissection5. Location of Adenopathy/ Type of Neck Dissection6. Likelihood of Postoperative Radiation7. Patterns of Skin Necrosis in different Skin flap designs 8. Potential for Wound healing problems9. Need for reconstructive flaps10. Tracheotomy may affect blood supply of some flap designs

POSITION OF THE PATIENT1. The patient is laid supine 2. The head turned opposite side
and hyperextended, resting on head ring
3.Upper end of the operating table elevated approximately 30 degree.
4.Mastoid tip., Ear lobule, Body of the mandible, midline of the chin, supra-sternal notch, clavicle and region of trapizius muscle insertion should be visible

General Rules
General Rule of Placing the Incisions in Lines of
Relaxed Skin Tension Lines (RSTL)
1. Horizontal Curving Incisions placed at a level in the neck depending on the site of the tumor
2. Facial incisions for parotid tumors can be combined with various neck incisions depending on preoperative considerations
3. High submandibular incisions should be placed at least 2cm below body of mandible
4. General Rule of placing vertical incisions so that weakest blood supply areas and trifurcations are away from (usually posterior to) carotid artery and at right angles for at least 2cm then with a "lazy" S-shape to minimize potential for scar contracture

• 1.Good exposure of the neck and primary disease.• 2. Ensure viability of the skin flaps. Avoid acute angles• 3. Protect carotid artery even in the cases of wound infection• 4.Considered preoperative factor—previous radio or
chemotherapy.• 5. Facilitate reconstruction Example, if pectoral muscle is
used a lower limb should be near the clavicle to enable flap accommodation.
• 6. It should be cosmetically acceptable

Incisions
Y incision Mc fee incision
59
Schobinger Incision
Modified schobinger Conley’s Double Y

Apron incision Half apron incision
60
H incision

Steps of Radical Neck Dissection

Incision

Dissection of the posterior triangle begins at the anterior border of trapezius

Dissection of the posterior triangle medially leads to exposure of brachial plexus, phrenic nerve and
cutaneous roots of the cervical plexus

Specimen reflected posteriorly and anterior flap elevated to expose the sternal head of SCMM

Sternocleidomastoid muscle is detached from the sternum and clavicle and retracted cephalad to
expose the carotid sheath

Internal jugular vein is ligated and divided after common carotid and vagus nerve is exposed and
retracted medially

Dissection proceeds cephalad along the carotid sheath up the skull base

The upper skin flap is now elevated preseving the mandibular branch of the facial nerve

Supraclavicular dissection 70

Dissection of the posterior triangle 71

Retraction of the posterior belly of digastric show the upper end of the IJV in level II
72

Division of the veins related to hypoglossal nerve 73

Levels II-V dissection completed by removing the specimen and
dissecting the IJV from carotid artery and
vagus nerve
74

Surgical field following RND

Shoulder syndrome
“Physical changes occuring in the shoulder joint due to denervation of trapezius leading to destabilization of scapula,pain and weakness and deformity of shoulder girdle,restricting the patient’s ability to abduct shoulder not above 90 ”
-NAHUM

Modified radical neck dissection(MRND)
– Excision of same lymph node bearing regions as RND with preservation of one or more non-lymphatic structures (SAN, SCM, IJV)
– MRND is analogous to the “functional neck dissection” described by Bocca
77

Three types (Medina 1989) .
• Type I: Preservation of SAN• Type II: Preservation of SAN and IJV• Type III: Preservation of SAN, IJV, and
SCM ( “Functional neck dissection”)
78

MRND TYPE I
MRND TYPE I MRND TYPE II

MRND TYPE III Advantages :
– Reduce postsurgical shoulder pain and shoulder dysfunction
– Improve cosmetic outcome– Reduce likelihood of
bilateral IJV resection in a pt with bilateral lymph node metastasis.

Selective Neck Dissection
– Cervical lymphadenectomy with preservation of one or more lymph node groups
– Four common subtypes:• Supraomohyoid neck dissection• Posterolateral neck dissection • Lateral neck dissection• Anterior neck dissectionIndication: primary lesion with 20% or greater
risk of occult metastasis

SND: Supraomohyoid type• Most commonly performed
SND• Definition
– En bloc removal of cervical lymph node groups I-III
– Posterior limit is the cervical plexus and posterior border of the SCM
– Inferior limit is the omohyoid muscle overlying the IJV

Surgical procedure

SND: Lateral Type
• Definition– En bloc removal of the
jugular lymph nodes including Levels II-IV
• Indications– N0 neck in carcinomas of
the oropharynx, hypopharynx, supraglottis, and larynx

SND: Posterolateral Type
• Definition– En bloc excision of
lymph bearing tissues in Levels II-IV and additional node groups – suboccipital and postauricular
• Indications– Cutaneous malignancies
• Melanoma• Squamous cell
carcinoma• Merkel cell
carcinoma– Soft tissue sarcomas of
the scalp and neck

SND: Anterior Compartment
• Definition– En bloc removal of lymph
structures in Level VI• Perithyroidal nodes• Pretracheal nodes• Precricoid nodes
(Delphian)• Paratracheal nodes
along recurrent nerves– Limits of the dissection
are the hyoid bone, suprasternal notch and carotid sheaths
• Indications– Selected cases of
thyroid carcinoma– Parathyroid carcinoma– Subglottic carcinoma– Laryngeal carcinoma
with subglottic extension
– CA of the cervical esophagus

Types of neck dissections

Extended Neck Dissection
• Definition– Any previous dissection
which includes removal of one or more additional lymph node groups and/or non-lymphatic structures.
– Usually performed with N+ necks in MRND or RND when metastases invade structures usually preserved.
• Indications– Carotid artery invasion– Other examples:
• Resection of the hypoglossal nerve resection or digastric muscle,
• dissection of mediastinal nodes and central compartment for subglottic involvement, and
• removal of retropharyngeal lymph nodes for tumors originating in the pharyngeal walls.

ComplicationsINTRAOPERATIVE
• Hemorrhage• Carotid sinus reflux• Pneumothorax• Air embolus• Embolism• Nerve damage• Chylous fistula
POST OPERATIVE
• Hematoma• Wound infection• Skin flap loss• Salivary fistula• Chylous fistula• Blindness • Facial edema• Electrolyte disturbances• Carotid artery rupture

ALGORITHM FOR NECK DISSECTION

Important facts
• High incidence of occult mets in T1 & T2 leisons involving floor of mouth ( 21% & 62%)
• Crossing the midline increases the incidence of contra/ bilateral nodal mets leison 1cm away from midline …15% leison within 1 cms of midline… 15-30% leison crossing the midline……..>30 %
20 – 30 % of the malignancies of tongue metastasize to clinically undetectabe cervical nodes
High incidence of skip metastasis- cancer of tongue

References • Textbook on oral cancer – JATIN .P.SHAH• Robbins KT. Classification of neck dissection: current
concepts and future considerations. Otolaryngol Clin North Am. Aug 1998;31(4):639-55
• Shah JP: Patterns of lymph node metastasis from squamous carcinomas of the upper aerodigestive tract. Am J Surg 1990, 160:405-409.
• Medina JE, Byers RM: Supraomohyoid neck dissection: Rationale, indication and surgical technique.Head Neck 1989, 11:111-122