Embed Size (px)
Citation preview

National Iodine Deficiency Disorders
Control Program - Dr Aravind Gandhi P
PG-MD Community Medicine VMMC & Safdarjung Hospital
Moderator: Dr Geeta Pardeshi

Contents• Introduction• IDD Spectrum• Scenario of IDDs• Chronology and Evolution of IDD programme in India• NIDDCP• Activities & Indicators• Budget and Organogram• Achievements• Limitations and Constraints• Future

IntroductionWhat is Iodine?• Discovered by French chemist Bernard Courtois• Belongs to Halogen group• Atomic number- 53, Mass number- 127, with other isotopes existing Recommended Daily Allowance (RDA):0-59 months- 90 mcg6-12 yrs- 120 mcg>12 yrs- 150 mcgPregnant and Lactating women- 250 mcg

• Forms: Iodide and Iodate of Sodium and Potassium• Sources: Seaweed (with max DV), Cod, sea fishes, Iodised salts- Absorbed in duodenum and jejunum. Excreted by KidneysMetabolism: Iodine trapping- Na-I sympoter, Secretion of Thyroglobulin, Oxidation of iodide, Iodination of tyrosine to MIT and DIT. T4 and T3 formed -T3 most potent.

• Contraindications or Medical advice required: While patient is on Anti-Thyroid drugs, ACE inhibitors and K sparring diuretics.
• Adverse effects: Endemic goitre areas- Jod-basedow effect
• Goitrogens are substances (whether in drugs, chemicals, or foods) that disrupt the production of thyroid hormones by interfering with iodine uptake in the thyroid gland.
Sulfadimethoxine, propylthiouracil, potassium perchlorate, Lithium, cassava, soya beans, sweet potatoes, bamboo shoots, turnips, cabbage

Importance of Iodine: Iodine deficiency remains the single most largest preventable cause of MR (first 1000 days)By helping the production of Thyroxine hormone
Iodine sufficient brain Iodine deficient brain

• IQ level of 13 points difference between Iodine deficient and normal children. • 1 point increase in IQ associated with 0.11% increase in GDP• The brain damage in IDD, only the tip of the iceberg will be visible.

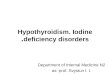
Tip of the Iceberg?
Loss of Energy due to Hypothyroidism
Loss of IQ Mild and Moderate Brain Damage
Cretinism Goitre
Severe Brain Damage

Iodine deficiency disorders and Soil:• Iodine deficiency disorders (IDD) refer to all of the consequences of
iodine deficiency in a population that can be prevented by ensuring that the population has an adequate intake of iodine
• IDDs – Disease of soil. Iodine present in top soil is constantly leached- Iodine deficient crops- Iodine deficient food- IDD in humans and animals

Spectrum of IDDs:• Foetus: Abortions/stillbirths/congenital anomalies/increased perinatal
mortality/neurological cretinism- deaf mutism, mental deficiency, spastic diplegia, squint/ dwarfism• Neonates: neonatal Goitre/Hypothyroidism• Child and Adolescents: Goitre/ juvenile hypothyroidism/impaired
mental function• Adults: Goitre with its complications/ impaired mental
functions/hypothyroidism

Scenario of IDD • 1.88 billion people are at risk of iodine deficiency and 241 million children have
an inadequate iodine intake (Andersson et al. 2012). Half lives in SEAR and Africa• 111 countries- adequate iodine nutrition (mUIC)• 30 countries remain iodine-deficient, 9 are moderately deficient, 21 are mildly
deficient (2013)• In India, estimated 350 million people are at risk of IDD as they consume salt
with inadequate iodine.• 1962- Total Goitre Rate (TGR) was in the range of 5.5% to 85.35%.• Current- 337 out of 400 districts surveyed have TGR of >5%• NCT Delhi - all the 9 districts are endemic for Goitre

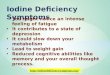
Global Scorecard of Iodine Nutrition 2014-2015
Based on median urinary iodine concentration (mUIC) in school-age children

Chronology and Evolution of IDD programmes India
• Iodine manifestations have been known to mankind from ancient times. • First documented in India in the Himalayan region by McCarrison in 1908
Phase 1: Research Leading to a programme (1956-83)Khangra Valley study:First of its kind in IndiaProvided evidence for iodine and goitre relationshipMajor reason for formulation of NGCP

National Goitre Control Programme, 1962Launched by GoI, under MoH&FP during 2nd five year planWith 3 objectives focussing on • surveys of goitre in endemic areas• production and distribution of iodised salt in those areas,• resurveys after 5 years to assess the impact

The programme did not achieved its intended objectives because:• Low priority• Focussed only on endemic districts- Himalayan specific• Public sector only production(Hindustan salt ltd) • Problems in transport, distribution and supervision• Poor monitoring of nominees for supply of salt at district level• Poor enforcement of PFA, non-commitment of states towards surveys. • IDD was seen as cosmetic. Administrative incompetence, lack of intersectoral co-
ordination, rampant vested and commercial interests. 1983- The central health council adopted USI as policy (hints)1992- NIDDCP & National level Ban on non-iodised salt.

Phase 2: From Goitre to IDD (1983-2000)Failure of NGCP to address IDDsShift from NGCP to NIDDCP Phase 3: Flip-Flops in ban of non-iodised salt (2000-05) 1997- Ban on Non-iodised salt2000- Ban lifted (Cost, Politics, Research lack, Personal choice)Iodised salt introduced in PDS

Phase 4: (2005-present)2005- Ban Reinstated Revised Policy guidelines on NIDDCP, 2006Consolidation of sustainable elimination of IDDs2015- First National Iodine and Salt Intake survey

National Iodine Deficiency Disorders Control Program
• 100% centrally sponsored programme, launched in 1992.• Currently under NHM, under MoH&FW.• Last Revision of Guidelines- 2006
Goal:Reduce the prevalence of Iodine Deficiency Disorders below 10 percent in the entire country by 2012 A.D.
(12th five year plan- 5%)

Objectives:• Surveys to assess the magnitude of the Iodine Deficiency Disorders.• Supply of iodinated salt in place of common salt.• Resurvey after every 5 years to assess the extent of Iodine Deficiency
Disorders and the impact of iodinated salt.• Laboratory monitoring of iodinated salt and urinary iodine excretion.• Health education and Publicity.

Activities:1.Iodisation2.Survey3.Monitoring and Reporting4.Information Education Communication activities

1. IodisationSalt Salt- Central subject. • 60% for industrial purposes. 25% for human consumption.• Refined and Unrefined USI- Universal Salt Iodisation- Policy• Adequate iodisation of salt consumed by human and animals.Rationale of USI:• Disease of soil. Hence present in all times. Effects are irreversible. Prevention is better than
cure.• USI has been recognised as the most cost-effective and viable solution to prevent and control
IDD.• Universal Salt Iodization (USI) is key strategy for control of IDD.


Standards:• Standards for Salt Iodisation was originally prescribed under PFA act, Now its
been covered under FSSAI, 2006• Packed in HDPE lined jute bags for 50 kg if wholesale, plastic pouches for 500 or
1000 g/pack in retail. • Iodine Content: Not less than 30 ppm at production level Not less than 15 ppm at household level Moisture: Not more than 6% of the salt weight Na Cl: Not less than 96% of the salt weight on dry basis Anti-caking agent: Not more than 2% of salt weightPunishment: 10 lakhs fine and/or 3 years imprisonmentCost- 0.05$/person/year

Transport:• The Salt Commissioners Office (SCO) is responsible for ensuring the
production of Iodised salts and its transport to the states. About 57 per cent of salt for human consumption moves by rail and the rest by road. • Railways shift the salt under priority B• Salt transport for human consumption requires certificate by
SCO/authorised agents.

2. Surveys:• Population: 6-12 years old children.• Sampling technique: Probability Proportionate to Size (PPS)
systematic random sampling is applied- equal ratio of boys and girls- enrolled in schools as well as out-of school children according to the % in the respective area.• Sample size- 2700 (30 clusters*90 samples) for Goitre • Data collected- Goitre rate, Salt iodisation level, adequacy and mUIE
(age, sex wise)• Frequency- Once in 5 years ,district-wise

3. Monitoring and Reporting:
Monitoring:Lab Monitoring of NIDDCP- 3 level• Primary- estimation of iodine in salt • Secondary- Estimation of urinary iodine content (for bio-availability of
iodine)• Tertiary- Neonatal monitoring for TSH

Collection, dispatch and analysis of salt:• 50 samples/district/month- 25 rural house, 15 urban house, 7 rural
retailers, 3 urban retailers- labelled• Quantity of sample- 100g if loosely avail, full if packed• Brought to Distort level monitor lab- iodine analysed• Quality control- 10% 0f samples will be sent to state level monitor lab• Compiled report of Iodine analysis will be sent to central IDD cell in
DGHS, monthly• Besides District IDD, Food inspectors under FSSAI collect two samples
for analysis, monthly

• At Community Level the salt samples is been tested for Iodine Content by Health Functionaries (ANM’s), ASHA workers and other field Health staff. • The Iodine content in salt samples at household level is tested with
the help of Salt Testing Kits (STK). • The STK has colour indicator which helps to know the level of Iodine
content such as 15ppm, >15ppm and <15ppm

Salt Testing Kits• Easy to measure• Not too much technicality present• Cheap• Easy Portability- Hence access to difficult areas
Disadvantages:-Inter-observer variations of specificity is as low as 40% in multi-observer scenario-Recent studies limit STKs as only qualitative but not quantitative measure

Collection, dispatch and analysis of urine:• 25 samples/district/month- sent to state monitor lab directly• Collected from 6-12 years old- 15-20 ml tight screwed bottle,
despatched same day- labelled• 3-5 ml of urine is collected casually from all individuals for spot UIE• Monthly report sent to central IDD through state programme officerPeriod frequency of Reports:• 1.Monthly - Activities• 2. Quarterly- Progress

4. IEC activities:October 21 World IDD dayTV/Radio broadcasts10 minutes video clip on IDDPamphletsPosters depicting manifestations of IDDsSTKs awareness programmes among General publicArt of song and drama are also employed in collaboration with Doordarshan and All India Radio

Indicators:

BudgetUnion:• 2014-15: 40 cr but only 30.88 cr was spent.• 2015-16: No separate budget• 2016-17: Rs. 37.61 crore.Delhi: 2015-16: 30 lakhs

Organogram:
Central-Nutrition & IDD cell (under DGHS) Nodal officer- Adviser (nutrition) of DGHS IDD cell under Deputy Asst DGHS+ Research Officer (IDD)+ teamState- Independent state IDD cells State Health Directorate. State Programme officer IDD monitoring LaboratoriesDistrict: Salt surveys Front line workers- ANMs and ASHA

Salt Commissioner Office- Jaipur• Salt Commissioner’s Organization is the Nodal Agency for monitoring
the production and quality of iodized salt at the production level & ensuring its equitable distribution in the country.
• For maintenance of 26 quality control lab at production level+ 8 mobile labs. Uses Management Information System for real time data.
• The Iodine Deficiency Disorder (IDD) division is headed by a Dy. Salt Commissioner (NIDDCP)

Intersectoral co-ordination committee Under MoH&FW:1. Central steering committee- Chairman: Secretary, MOH&FW- FOR OVERALL Review & new formulations of the programme2. Programme implementation committee- Chairman: DGHS- asses implementation, monitoring & evaluation of the programmeAdviser (nutrition) is the convenor of both committeesUnder SCO:• Committee of stakeholders- Chairman- Salt Commissioner

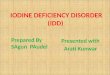
Various departments working together for IDD
Ministry of Finance
1. Ministry of Health & Family Welfare
2. Salt Commissioner
3. Ministry of Railways
Ministry of Road Transport and
Highways
Ministry of Panchayat raj
Ministry of Law and Justice
Ministry of Information and
Broadcasting
Ministry of Human Resources and Development
Niti Ayogh
Ministry of Women and Child
Development

NGOsIDD Experts
Salt Industry
Government
Policy MakersEducators
Consumers
Agriculturalist
Consumers
Various stakeholders: IDD

• National Coalition established in 2006• 2009 Secretariat of NCSII set up at ICCIDD, New Delhi

Achievements:
As on 1st week of December 2016,706 salt iodisation plants including refineries in india.
Total iodisation capacity- 224.10 Lakh MT (2015-16)
Iodised salt produced- 64.76 Lakh MT, Refined- 44.64 unrefined- 20.12 (2 lakh tones in 1983)According to MoH&FW, there is no gap between supply and demand of iodised salt
Ministry of Health shows that 71% population in country have access to adequately iodised salt (Coverage Evaluation Survey, 2009).NIDDCP has been included in the 20 point program of the prime minister.

National Iodine and Salt Intake survey, 2015• the household coverage with iodized salt was 92%, and 78% with
adequately iodized salt (≥15 ppm)• the median UIC was 112.4 μg/L in the households with non-iodized
salt• 123.4 μg/L in the households with poorly iodized salt• 168.4 μg/L in those with adequately iodized salt.


As on August 2015,Total Salt SamplingsAt production levelSamples analysed for iodine: 11494Samples found standard: 10826 (94%) At consumption level (STKs)Samples analysed: 1820398Samples found standard: 1355406 (74%)
Urine SamplingsSamples analysed: 3586 Samples found standard: 3467 (97%)

List of states with IDD cells and labs:
• 26 states and 6 union territories have 1 IDD cell each• 27 states and 6 union territories have 1 IDD lab each• Andhra and Pudhucherry have no IDD cell and Lab• Delhi has both IDD cell and IDD lab• A National reference Laboratory at NCDC, Delhi for training for IDD monitoring in
iodine content of salt and urine.
• 18 states provide Iodised salt via PDS (refined or unrefined or both)• Gujarat and Madhya Pradesh have subsidised the Iodised salt in PDS

Factors critical for the achievements reached in IDD control program of India• Generation of regular, representative, and reliable scientific data• Stakeholder analysis and development of partnership• Institutional continuity and mentorship for achievement of
sustainability• Addressing value system of stakeholders• Legislation for achieving public health goals• Involvement of private sector in public health efforts• Political commitment

Limitations and Problems:• Non-Compliance with International Guidelines:NIDDCP guidelines does not adhere to many standards of WHO/unicef Revised Policy Guideline on NIDDCP, 2006 did not conform to standard guidelines laid down by WHO/UNICEF/ICCIDD for monitoring of IDD control programmes. The cut-off of TGR used to define a region as IDD endemic is 5 per cent, whereas it is 10 per cent as per the revised policy guidelines of NIDDCP.

Target population in district survey is only 6-12 years, leaving a major group- pregnant women.WHO guidelines include UIE of pregnant women as indicator and not TGR, whereas NIDDCP its reverseThe current revised policy guidelines lack any epidemiological rationale both in terms of sampling method and sample size. The recommended sample size as per WHO/UNICEF/ICCIDD guidelines is 1200 school aged children and 300 pregnant women for IDD survey.Sub-national level data

Testing kits, IEC and Left-out areas:• The methodology used in Indian surveys, STKs, has low validity. Still the
data is valuable from a comparative point of view over the years. • No monitoring of food industry, whether the products are made from
iodised salts.• No information available regarding salt used in livestock industries• Consumer awareness regarding salt iodization is also inadequate in
India. A study done in rural households in India, reported that only 62% per cent households were aware of iodization and goitre relationship, and only 35.4 per cent respondents knew that iodine deficiency causes “less mental development and diminished intelligence• No records of other IDD spectrum diseases, apart from Goitre

Zonal and Legal barriers:• Salt iodization especially by small scale producers who contribute to
approximately 66 per cent of total iodized salt production. But the quality is still questionable, in terms of levels of iodisation, packing • Transport especially in roadways • There is marked variation of iodised salt coverage between urban and
rural. Zonal variations also exists, south being worst (National Iodine and Salt Intake survey)• Poor implementation of FSSAi act. And the loopholes present in the
Act itself.

Budget and ministerial level issues:The committees established has not been effective, resulting in poor coordination and a lack of leadership for the USI programmeBudget: Inadequate and underspending of even the allotted amount in the union Budget50000 rs/district provided to conduct IDD survey is insufficient.Inadequate tertiary monitoring of neonatal hypothyroidism- No national data available.

WHO indicators for IDD elimination:


Success or failure?• Hence a mixed opinion arises out, regarding the success of the NIDDCP.
• It has achieved its goal of reducing TGR< 10% as envisaged in the revised document of 2006 • The production, distribution of Iodised salt has reached the higher level,
with a massive 20% increase in household usage of adequately iodised salt to 71% in 4 years(2009) and reached 78% in 2015
• The Shifting of Goal post of NIDDCP to TGR<5 % by 2017 under the 12th year plan bear witness to its success, from the programme point.

Future…Iodisation: -Strengthen the supply chain of iodized salt- Transport-Focus shift towards formulating and introducing Iodine rich foods in dietSurvey and Monitoring:-Clarity and updated guidelines- Methodology must be made robust and in consistent with WHO standards-Quality Control and number of salt testing laboratories-Track progress- Bringing a surveillance system and changing indicators-Regular National level data must be achieved-Special focus on vulnerable groups: pregnant women and new born children

• IEC activities:-Reaching the unreached by strengthening IEC• Administration and Law:-Bureaucratic hurdles- In strengthening the NCSI-Strengthen the regulatory framework- Legal loopholes plugged-Sustain and strengthen partnerships- state level coalitions External Reviews:-Inviting Reviews from WHO/UNICEF

• Technology: -Management Information system to be extended to surveys and monthly reports• Indicators at various levels must be ensured • Sustain progress Other techniques of Iodine supplementation:Iodised oil- 1-2 ml/yearIodised water- Irrigation-china- 1994Iodised bread- NetherlandsDrops and tabletsJeevan Bindi- 2015-Maharashtra- Tribal woman

Double Fortified salt- the next level in salt fortification?? Iron- 800-1100 ppm
As of now, there is no declared government policy for universal double fortification of salt. But in 2011, PMO meeting and MoW&CD has issued mandatory guidelines for DFS usage in Mid-day meals and ICDSChattishgarh, Andhra Pradesh, Himachal Pradesh, Karnataka, Tamil Nadu, RajastanTNSC- Started DFS in 2004. Manufactures and supplies DFS 2500 tonnes per annum to each Tamil Nadu and Karnataka for Noon meal schemeRSFCC- Supplies DFS to 650 tonnes/month in fair price shops via private biddingPrivate players have been allowed under FSSAI to manufacture DFS• Rs 25/kg (Tata plus)

References• National Iodine Deficiency Disorders Control Programme http://www.
http://nrhm.gov.in/nrhm-components/national-disease-control-programmes-ndcps/iodine-deficiency-disorders.html
• National Iodine Deficiency Disorders Control Programme mohfw.nic.in/WriteReadData/l892s/rtiNICRT-81756647.pdf
• http://www.saltcomindia.gov.in/• http://iqplusin.org/index.php/about-idd/pink-booklet• Assessment of iodine deficiency disorders and monitoring their elimination
http://www.who.int/nutrition/publications/micronutrients/iodine_deficiency/9789241595827/en/• Sustainable Elimination of Iodine Deficiency https://www.unicef.org/publications/index_44271.html• Global prevalence of iodine deficiency disorders http
://www.who.int/nutrition/publications/micronutrients/iodine_deficiency/54015_mdis_workingpaper1/en/
• National Iodine Deficiency Disorders Control Program, India. http://www.jmap.in/national-iodine-deficiency-disorders-control-program-india/
• http://planningcommission.gov.in/plans/planrel/12thplan/pdf/12fyp_vol3.pdf

• The changing epidemiology of iodine deficiency https://www.ncbi.nlm.nih.gov/pubmed/22473332
• Global Iodine Nutrition: Where Do We Stand in 2013? http://www.ign.org/cm_data/2013_Pearce_Global_iodine_nutrition-Where_do_we_stand_in_2013_Thyroid.pdf
• Iodine deficiency disorders (IDD) control in India https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3818611/
• Evolution of Iodine Deficiency Disorders Control Program in India: A Journey of 5,000 Years http://www.ijph.in/article.asp?issn=0019557X;year=2013;volume=57;issue=3;spage=126;epage=132;aulast=Pandav
• National Iodine and Salt Intake survey, 2015 http://www.ign.org/cm_data/IDD_nov15_india.pdf
• Towards universal salt iodisation in India: achievements, challenges and future actions http://ign.org/cm_data/2013_Rah_Towards_universal_salt_iodisation_in_India_MCH.pdf
• Right To Information DTGHS/R/2016/50022 & DOIPP/R/2016/50623 • http://wcd.nic.in/fnb/fnb/guidelines/icdsdtd22022012.pdf• dghs.gov.in• http://www.ign.org/newsletter/idd_nl_may11_india_rural.pdf

• Thank you..