Embed Size (px)
Citation preview

m a g a z i n e
2 0 0 9 , I s s u e 2
n a t i o n a l C o u n c i lsharIng Best PractIces In Mental health & addIctIons treatMent
A quarterly publication from the National Council for Community Behavioral Healthcare
www.thenationalcouncil.org
the time is right, Page 2
Mental health First aid, Page 14
geoffrey canada on his harlem Miracle, Page 20
It takes a community, Page 24
From the Field, Page 30
Prevention and Early Intervention for Mental & Addiction Disorders

40th National Mental Health and Addictions Conference & Expo
March 15-17, 2010 Disney’s Coronado Springs ResortFlorida
INSPIRED SOLUTIONS NEW DIRECTIONS COOL CONNECTIONS
www.TheNationalCouncil.org/Conference | 202.684.7457
Register and reserve your hotel now!Call for Papers open through Sept 15, 2009.

National Council Magazine is published quarterly by the National Council for Community Behavioral Healthcare, 1701 K Street, Suite 400, Washington, DC 20006.
www.TheNationalCouncil.org
Editor-in-Chief: Meena Dayak
Specialty Editor, Prevention and Early Intervention: Chris Loftis
Editorial Associate: Nathan Sprenger
Editorial and advertising queries to [email protected] or 202.684.7457, ext. 240.
Mental illnesses and addiction disorders remain an
unsolved mystery to many. Against the backdrop of stigma,
lack of access to quality care, and funding constraints,
prevention-early intervention remains the missing piece of
the puzzle. It’s the piece that completes the equation of
total care for those we serve and commitment to improve
the communities we live in.
Many community-based healthcare organizations have been
operating model programs in prevention–early intervention
for mental and substance use disorders with impressive
outcomes. These programs reach a range of populations —
children, youth, older adults, veterans, and persons already
diagnosed with one form of mental illness or addictions who
may be at risk for other disorders. The programs comprise
a broad range of initiatives—public education, screening in
primary care, school-based initiatives, suicide prevention,
employee assistance programs, and more. This issue of
National Council Magazine profiles some of these model
programs and features the views of policy and clinical
experts on why prevention-early intervention is important as
we attempt to piece the healthcare puzzle together.
PolIcY PersPectIVes
2 Prevention and Early Intervention: The Time is Right Editorial by Linda Rosenberg
4 Point/Counterpoint: Prevention — What Does It Really Save? Media Excerpts
6 IOM Report on Prevention and Carl Bell Interview Meena Dayak, Chris Loftis
10 Saving Jobs, Saving Public Dollars Vidhya Alakeson
12 Call to Include Prevention in Healthcare Reform SAMHSA Core Consensus Principles
eVIdence-Based earlY InterVentIons
14 Mental Health First Aid Educates and Transforms Communities Lea Ann Browning McNee, Susan Partain
20 Geoffrey Canada on His Harlem Miracle Meena Dayak, Chris Loftis
22 Nurse-Family Partnership: Effective and Affordable Peggy Hill
24 It Takes a Community William R. McFarlane, Donna Downing, Anita Ruff
26 A Long-term Approach to Early Psychosis Intervention Tamara Sale, Ryan Melton
29 SBIRT: Effective Interventions for Alcohol-Related Health Problems Maureen Fitzgerald
FroM the FIeld
30 Getting a Head Start on Mental Health: Children’s Programs
36 Saving Our Future: Youth Substance Use and Suicide Prevention
44 Across the Spectrum: Working with Special Needs Populations
targetIng hIgh-rIsK PoPulatIons
50 HOPE for Homeless Youth and Families Nisha Beharie, Mary McKay, Kosta Kalogerogiannis
54 InSHAPE: Promoting Wellness, Saving Lives Ken Jue interviewed by Laura Galbreath
PDF available at www.TheNationalCouncil.org
n a t i o n a l C o u n c i lM A G A Z I N E
Prevention and early Intervention for Mental & addiction disorders
National Council Magazine, 2009, Issue 2
p.14

4 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Policy Perspectives
E pic arguments are being waged regarding the pros and cons of disease prevention. However,
few, if any, are offering serious insight as to how to address the host of mental health disorders estimated to affect 14 to 20 percent of America’s young people in any given year. A perfect storm is brewing, exacerbated by a troubled economy, rising unemployment, increasing bankruptcies and home foreclosures, and dwindling funds for programs. Dismal realities affect families and threaten the mental health of our nation’s youth.
Passionate exchanges tout the medical benefits and lives saved through the early detection of breast cancer, stroke, and heart disease, while the stigma surrounding mental illness persists. Workplace shootings, familicides, and the overdose deaths and suicides of notable celebrities prompt frequent news coverage, with discourse on preven-tion and early detection in an everyday setting tak-ing a noticeable backseat. The public interprets the message: the mentally ill aren’t safe to be around. As a result, would-be-patients fly below the radar to avoid detection. Without the increased use of prevention strategies that are scientifically proven to work, and a correspondingly swift uptick in early detection efforts and community awareness and education in national media, mental disorders con-tinue to fester like an undetected cancer.
The discussions regarding preventative healthcare are more than politically fueled punditry about dollars and cents. Saving money is important, how-ever, the bottom line should include safeguarding a quality of life. When it comes to mental health-care, or lack thereof, individuals and their families are hoping for anyone to throw them a lifeline, to
live a “normal” life. According to the March 2009 Institute of Medicine (IOM) report brief for policymakers: Preventing Mental, Emotional, and Behavioral Disorders Among Young People, Progress and Possibilities, evidence-based approaches are proving to prevent certain mental health disorders, and limit risk factors, and are likely to be far more cost-effective at addressing mental, emotional, and behavioral disorders (MEBs).
Most MEB disorders erupt during childhood and adolescence. The IOM report suggests that the “window of opportunity” when symptoms first ap-pear, typically 2 to 4 years before the onset of the disorder, is the prime time when prevention strat-egies have the most impact. Persons with mental health disorders have usually been identified only after they dropped out of school, and shuffled through the criminal justice system, and multiple hospitals, leaving extraordinary healthcare bills in
their wake. The Early Detection and Intervention for the Prevention of Psychosis Program, a national ef-fort launched by the Robert Wood Johnson Founda-tion and spearheaded by program director, William R. McFarlane, MD, estimates the cost to society to be higher than $10 million over the lifespan of a person who has schizophrenia. The National Council supports early intervention, before costs escalate and the prospects of a happy, healthy life disintegrate. The ensuing discussions beg the ques-tion — just how much is an improved quality of life worth these days?
The National Council recognizes that the issue reaches beyond the bread and butter aspects of healthcare, and becomes muddled when editori-als sound the alarm of diagnosing millions with a disease that requires treatment. An op-ed piece by David Harsanyi in The Denver Post insists that expanding the definition of diseases such as dia-
linda rosenberg, MsW, President & CEO, National Council for Community Behavioral Healthcare
Prevention and Early Intervention: The Time is Right
Saving money is important, however,
the bottom line should include safeguarding a quality of life.
ditorial

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 5
betes, high cholesterol, and osteoporosis, has already placed millions more Americans at the swelling healthcare trough. The idea that patients shouldn’t be identified for having a disease, or the potential to develop one, is a precarious one, especially for men-tal health. Sweeping mentally ill patients under the carpet has been going on for years and has hindered even the most ardent efforts of dedicated mental health professionals. Harsanyi is blunt — end of life care is costly, and free will overrides the patient’s de-cision to follow the doctors’ advice anyway. Part of the stigma plaguing mental illness is the notion that one can simply “snap out of” depression, or that persons “choose” to be mentally ill.
Chicago Tribune reporter Carla Johnson acknowledges in her article, Disease Prevention Often Costs More than it Saves, that disease prevention won’t neces-sarily save money, but that some efforts to prevent illness are necessary. Johnson quotes Robert Gould, president of the nonprofit Partnership for Preven-tion, saying that “Many of the services that don’t save money, improve people’s lives at relatively low cost.” A “pro-prevention” piece, More Attacks on Prevention and Its Role in Health Reform That Make No Sense, by Kenneth Thorpe in The Huffington Post, cautions against using “imprecise language” when it comes to policy-making, and strongly supports effective preven-tion programs that work simply “because they reach the right people at the right places with the right in-terventions.” Precisely steering back to that “window of opportunity” and the value of a healthy mind and a sound quality of life.
To further illustrate what research reveals, this issue of National Council Magazine focuses on stories of early intervention success.
The National Council has helped to bring the ev-idence-based public education program, Mental Health First Aid to the U.S. The program has trained more than 3,000 persons in its first year. Studies show that persons trained in what to do when someone is experiencing a mental health crisis have a greater likelihood of actually helping the person, and show a decrease in attitudes that encourage stigma and misperceptions.
The Early Detection and Intervention for the Preven-
tion of Psychosis Program uses evidence-based in-terventions that help youths succeed, without stigma, before they experience the negative effects of a fully developed mental illness.
Geoffrey Canada’s Harlem Children’s Zone, launched in 1970 as a community-based truancy prevention program, has grown to include diverse programs and serve more than 10,000 youth. The proven results — in 2008, nearly all students in third and eighth grade in HCZ charter schools outperformed the average New York student in math.
College Dreams, an alcohol and drug prevention pro-gram in Oregon, has saved thousands of youth from school dropout, substance abuse, and delinquency. The program is based on scientific evidence regarding the risk factors for substance abuse and the protec-tive factors that lead to long-term success for children who are beset by multiple and severe life adversities.
Based on recommendations in the March 2009 IOM report described in further detail in this issue, the National Council offers the following suggestions to increase public awareness and education efforts, and to fortify the case for evidence-based research and the use of proven practices regarding prevention and early detection:
Taking charge on a national level: The IOM report recommends that “the White House create an entity to lead toward a broad implementation of evidence-based prevention approaches and to direct research on interventions.” Public goals must be set for pre-venting specific disorders and promoting mental health, and funding must be provided to launch and improve evidence-based programs.
Dovetail efforts: Many mental disorders have common developmental pathways. Resources must be aligned between the departments of Education, Justice, and Health and Human Services. The National Institutes of Health should develop a comprehensive 10-year plan to research ways to promote mental health and prevent mental disorders in young people. State and local agencies should coordinate efforts and foster a multi-agency approach to ensure a comprehensive developmental perspective.
Equality in research funding: At present, a great deal of research leans toward treatment. Research
needs to move from laboratory settings to real world settings, and must be responsive to community so-cioeconomic needs, diversities, values, and goals. The IOM report also cautions that funding should not sup-port programs that lack empirical evidence, despite their popularity within communities.
Identifying children with risk factors: Screenings can be a helpful tool if parents and communities are aware of the purposes and methods of screenings, and have the ability to decline if they do not want their children included. But all families can learn to be aware of warning signals for teen depression, for example, and to distinguish between signs of impend-ing psychosis, and teenage angst that falls within the norm of behaviors prompted by the transition from children to teens to young adults.
Speak up: Programs that work need media attention to thrive. Seek out members of the media, distribute press releases, and invite the media and the public to “community education nights” that highlight preven-tion and early intervention efforts that build strong, healthy communities and improve the quality of life.
Society can no longer afford to ignore the risk factors for and the onset of mental illnesses and substance use disorders. Ignoring prevention and early interven-tion is issuing a personal invitation to cut a young life drastically short.
With more than 30 years of distinguished service in mental health policy, services, and system reform, Rosenberg is a leading mental health expert. Under Rosenberg’s leadership since 2004, the National Council for Community Behavioral Healthcare has grown to 1,600 member organizations, employing 250,000 staff and serving 6 million adults and children in communities across the country. Prior to joining the National Council, Rosenberg was the senior deputy commissioner for the New York State Office of Mental Health. In addition to responsibility for New York’s state-run adult, child, and forensic hospitals, she tripled New York’s assertive community treatment capacity, expanded children’s community-based services, developed an extensive array of housing options for people with mental illnesses and addictions, implemented a network of jail diversion programs including New York’s first mental health court, and promoted the adoption of evidence-based practices and consumer and family programs. A certified social worker, as well as a trained family therapist and psychiatric rehabilitation practitioner, Rosenberg has held faculty appointments at a number of schools of social work, serves on numerous agency and editorial boards, and writes and presents extensively on mental health and addictions issues including the impact of organizational and financing strategies on consumer outcomes.

6 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Policy Perspectives
P
My wife tried to tell me the other day that she had just “saved” us money by buying on sale a couple of
things for which we have no earthly use. She then pro-ceeded to tote up all our “savings” from said purchases and gave me a figure that represented the money we had generated, which we could now spend... she had me going for a minute.
I mention this because I have similar problems with the way President Obama hopes to pay for the huge and costly health reform package he has in mind that will cover all Americans; he is counting on the “savings” that will come as a result of investing in preventive care and investing in the electronic medical record among other things. It’s a dangerous and probably an incorrect pro-jection.
Prevention of a disease, we all assume, should save us money, right? An ounce of prevention...? Alas, if only such aphorisms were true we’d hand out apples each day and our problems would be over.
If the prevention strategies we are talking about are be-havioral things—eat better, lose weight, exercise more, smoke less, wear a seat belt—then they cost very little and they do save money by keeping people healthy.
But if your preventive strategy is medical, if it involves us, if it consists of screening, finding medical conditions early, shaking the bushes for high cholesterols, abnor-mal EKGs, or markers for prostate cancer such as PSA, then more often than not you don’t save anything and you might generate more medical costs. Prevention is a good thing to do, but why equate it with saving mon-ey when it won’t? Think about this: Discovering high cholesterol in a person who is feeling well, is really just discovering a risk factor and not a disease; it predicts that you have a greater chance of having a heart attack than someone with a normal cholesterol. Now you can reduce the probability of a heart attack by swallowing a statin, and it will make good sense for you personally, especially if you have other risk factors (male sex, smok-ing, etc.) But if you are treating a population, keep in mind that you may have to treat several hundred people to prevent one heart attack. Using a statin costs about $150,000 for every year of life it saves in men, and even
more in women (since their heart-attack risk is lower)—I don’t see the savings there.
Or take the coronary calcium scans or heart scan, which most authorities suggest is not a test to be done on people who have no symptoms, and which I think of as the equivalent of the miracle glow-in-the-dark minnow lure advertised on late night informercials. It’s a money maker, without any doubt, and some institutions actually advertise on billboards or in newspapers, luring you in for this “cheap” and “painless” way to get a look at your coronary arteries. If you take the test and find you have no calcium on your coronaries, you have learned that...you have no calcium on your coronaries. If they do find calcium on your coronaries, then my friend, you have just bought yourself some major worry. You will want to know, What does this mean? Are my coronary arteries narrowed to a trickle? Am I about to die? Is it nothing? Asking such questions almost inevitably leads to more tests: a stress test, an echocardiogram, a stress echo, a cardiac catheterization, stents and even cardiac bypass operations—all because you opted for a “cheap” and “painless” test—if only you’d never seen that billboard.
Poor McAllen, Texas. It happens to be the focus of a re-cent “New Yorker” piece by Atul Gawande, a piece that President Obama referred to in his speech to the AMA, because health care costs in McAllen are twice that of comparable cities while health outcomes are no dif-ferent. The reasons are complex but probably because good physicians are ordering lots of tests, calling in lots of consultants, making good use of the equipment they own and the imaging centers they might have a stake in (and yes, they think they can be objective in order-ing an MRI or CAT scan that sends the patient to their own facility); it has to do with hospitals competing with each other for the kinds of patients with conditions that are reimbursed well, and wooing patients, wooing high-volume physicians (some of whom are invited to invest in the hospital) to make full use of their PET scan, their gamma knife, their robotic-surgery facility, their cancer center, their birthing center. That was Atul Gawande’s conclusion, and I would concur.
Which brings me to my problem with the president’s
plan: despite being an admirer, I just don’t see how the president can pull off the reform he has in mind without cost cutting. I recently came on a phrase in an article in the journal “Annals of Internal Medicine” about an axi-om of medical economics: a dollar spent on medical care is a dollar of income for someone. I have been reciting this as a mantra ever since. It may be the single most important fact about health care in America that you or I need to know. It means that all of us—doctors, hospitals, pharmacists, drug companies, nurses, home health agencies, and so many others—are drinking at the same trough, which happens to hold $2.1 trillion, or 16% of our GDP. But reform cannot happen without cutting costs, without turning people away from the trough and having them eat less.
We may not like it, but the only way a government can control costs is by wielding great purchasing power to get concessions on the price of drugs, physician fees, and hospital services; the only way they can control ad-ministrative costs is by providing a simplified service, yes, the Medicare model (with a 3% overhead), and not allowing private insurance to cherry-pick patients.
Contrary to what we might think, comparative studies show us that the U.S. when compared to other advanced countries, does not have a sicker population: We actual-ly use fewer prescription drugs, and we have shorter hos-pital stays (though we manage to do a lot more imaging in those short stays—got to feed the MRI machines). The bottom line is that our healthcare is costly because it is costly, not because we deliver more care, better care, or special care. Alas, a solution that does not address the cost of care, and negotiate new prices for the services offered will not work; a solution that does not put caps on spending and that instead projects cost-savings here and there also won’t cut it. Leaders have to make tough and unpopular decisions, and if he is to be the first president to successfully accomplish reform there does not seem to be much choice: cut costs.
Abraham Verghese is professor and senior associate chair for the Theory and Practice of Medicine at Stanford University. He is the author of the novel “Cutting for Stone.”
Excerpts from an essay by Abraham Verghese in the Wall Street Journal, June 20, 2009
A doctor explains why it doesn’t pay to stay well. Decoding what works, what falls short in Obama’s plans to reform healthcare.
Perspectives from General HealthcarePrevention: What Does It Really Save?
The Myth of Prevention
oint/Counterpoint

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 7
Two recent newspaper pieces on prevention by Carla Johnson (Associated Press) and David Harsanyi (Denver
Post) repeat some long-standing misperceptions about prevention. Because prevention is central to health reform, it’s time to set the record straight.
Both the articles suffer from baby-with-bathwater syn-drome, brought on by lumping all kinds of prevention into one big pot. Imprecise language is dangerous, particularly in the realm of policy-making. It leads to fuzzy thinking and that produces bad policy.
Research shows that scientifically sound prevention programs for both individuals and populations improve health and save money. Research also shows that ef-fective prevention programs are targeted. They work because they reach the right people at the right time in the right places with the right interventions.
Prevention can be divided into three parts: Things we do to avert disease (primary prevention), like vaccinations for children or the YMCA diabetes program mentioned in the article. Things we do to find and treat disease in its earliest stages (secondary prevention), like mammograms and co-lon cancer screenings. And things we do to avoid complica-tions when people are already ill (tertiary prevention), like programs to help older people with multiple chronic condi-tions manage their care at home, like the PACE (Program of All-Inclusive Care for the Elderly) and similar initiatives. Dumping various interventions for various groups together and concluding prevention doesn’t save money is just plain wrong.
Not all prevention programs work, many because they aren’t grounded in science. Not all of them save money. All medical interventions including secondary and tertiary prevention cost money. Screening for common and costly diseases, like diabetes, high blood pressure, and high cholesterol, may actually raise spending in the short-term, because people who need treatment will get it. But over the long-term, that treatment is likely to avert even more costly complications, and thereby avoid higher spending.
Many studies show well-designed prevention programs are cost-saving. For example, a significant reduction in total health care spending is linked to community-based life-style interventions (primary prevention). Research shows that savings range from a short-term return on investment of $1 for every $1 invested, rising to more than $6 over the longer term. An investment of $10 per person per year in community-based programs tackling physical inactivity, poor nutrition, and smoking could yield more than $16 bil-lion in medical cost savings annually within 5 years. This is a remarkable return of $5.60 for every dollar spent, with-out considering the additional gains in worker productivity,
reduced absenteeism at work and school, and enhanced quality of life.
Worksite health promotion programs, too, are effective at both primary and secondary prevention. A systematic re-view of more than 50 studies meeting rigorous guidelines for review by the U.S. Task Force on Community Preventive Services found strong evidence of WHP program effective-ness in specific areas: reducing tobacco use, dietary fat consumption, high blood pressure, total serum cholesterol levels, and days absent from work due to illness or dis-ability, as well as improve other general measures of worker productivity. At Citibank, for example, a comprehensive health management program showed a return on invest-ment of $4.70 for every $1.00 in cost. A similar compre-hensive program at Johnson & Johnson reduced health risks, including high cholesterol levels, cigarette smoking, and high blood pressure, and saved the company up to $8.8 million annually.
As far as tertiary prevention goes, there’s evidence of effec-tiveness for that, too. Here’s one of the best: For nearly 25 years, senior researchers at the University of Pennsylvania have implemented a series of large, randomized controlled trials with high-risk elders. Their studies have demonstrated that comprehensive tertiary prevention focused particularly on transitional care produces better health outcomes and significant cost savings. Their most recent research showed a 56% reduction in readmissions and 65% fewer hospi-tal days for patients in transitional care. At the 12-month mark, average costs were $4,845 lower for these patients. If this model were scaled nationally with an investment of $25 billion over 10 years, savings could reach $100 billion over the same period.
The AP article’s Mrs. Jones is 55 years old, obese, and at risk for diabetes. Studies show that in 10 years, when she turns 65 and enters Medicare, the government will spend $20,000-$40,000 more on Mrs. Jones’ health care than Mrs. Smith’s, who’s the same age but a normal weight. Over 30% of the recent rise in Medicare spending in the last decade is associated with the persistent rise in obesity in the Medicare population. The increase in obesity-related chronic diseases among all Medicare beneficiaries and particularly among the most expensive 5% is a key factor driving growth in traditional fee-for-service (FFS) Medicare. Six medical conditions, all related to obesity — diabetes, hypertension, hyperlipidemia, asthma, back problems, and co-morbid depression account for most of the recent rise in spending in the Medicare population.
Chronic disease resulted in more than $987 billion in pri-vate spending most of it covered by private health insur-ance, which means higher premiums for everybody. Nearly
all of every Medicare dollar 96 cents of each and every one, or more than $447 billion last year and 85 cents out of every dollar in Medicaid nearly $300 billion go to care for chronic disease, most of which is preventable. In one year, total, this amounts to approximately $1.7 trillion spent treating patients with one or more chronic diseases roughly 75 percent of all U.S. health care spending. This is essen-tially a hidden tax on every taxpayer in America. Anyone who cares about long-term health spending, particularly govern-ment health care spending, should support prevention. It’s common sense.
Mr. Harsanyi’s argument that we should avoid prevention be-cause “the longer people hang around, the longer they utilize the healthcare system” and drive up costs is hardly worth addressing. It’s a bizarre concept that a civilized so-ciety would let people die of preventable causes. And it’s economically inaccurate. Obese and chronically ill Ameri-cans tend to live shorter lives, but chronic diseases and obesity are linked to two-thirds of the growth in U.S. health spending since the mid-1980s. We’re not cutting any cor-ners in health care costs by allowing these people to meet the Grim Reaper earlier.
The other major point both Mr. Harsanyi and Ms. Johnson miss is the “how” of prevention. How are policymakers proposing to increase effective prevention inside and out-side the health care system? Contrary to how their articles describe it, the idea isn’t to insert one-off prevention ef-forts into the existing system. Instead, Congress and the president are proposing fundamental changes to the way we deliver prevention, care, and treatment. That means improving community-based primary and secondary pre-vention, strengthening primary care (primary and second-ary prevention), and incentivizing providers and patients to better prevent and manage diseases (secondary and tertiary prevention). In sum: A comprehensive prevention plan rather than scattershot, unconnected, and ineffective efforts.
By preventing costly diseases or better managing them, we can help contain our out-of-control health spending. We can boost productivity. In our troubled economy, we need to do both. Even if it didn’t save money, preventing suffering when we can is the right thing to do. Research, common sense, and ethics all tell us the same thing: An ounce of (science-based) prevention is worth a pound of cure.
Kenneth Thorpe, PhD, is the Robert W. Woodruff Professor and Chair of the Department of Health Policy & Management in the Rollins School of Public Health of Emory University. He serves as the executive director of the Partnership to Fight Chronic Disease.
Lydia L. Ogden, MA, MPP, is the chief of staff for the Institute for Advanced Policy Solutions of the Center for Entitlement Reform at Emory University.
Excerpts from an article by Kenneth Thorpe and Lydia Ogden in The Huffington Post, June 26, 2009
More Attacks on Prevention and Its Role in Health Reform That Make No Sense

8 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Policy Perspectives
Summary of the Institute of Medicine’s report “Preventing Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities” (2009) Based on report briefs and press release at www.bocyf.org
eatured interview dr. Carl Bell
New IOM Report on Prevention Calls for Leadership, Collaboration, and Emphasis on Research
T he federal government should make promotion of mental health in young people a national
priority, says a new Institute of Medicine report, “Preventing Mental, Emotional, and Behavioral Dis-orders among Young People.”
Mental, Emotional, and Behavioral (MEB) disorders which include depression, anxiety, conduct disorder, and substance abuse are about as likely as frac-tured limbs in children and adolescents; inevitable and not at all uncommon. Almost one in five young people have one or more MEB disorders.
Many disorders have life-long effects that include high psychosocial and economic costs, not only for the young people, but also for their families, schools, and communities. Among adults, half of all MEB disorders were first diagnosed by age 14 and three-fourths by age 24. The financial costs in terms of treatment services and lost productivity are estimated at $247 billion annually. MEB disor-ders also interfere with young people’s ability to ac-complish developmental tasks, such as establishing healthy interpersonal relationships, succeeding in school, and making their way in the workforce.
Clear windows of opportunity are available to prevent MEB disorders and related problems be-fore they occur. Risk factors are well established, preventive interventions are available, and the first symptoms typically precede a disorder by 2 to 4 years. And because mental health and physical health problems are interwoven, improvements in mental health also improve physical health.
Early identification and intervention of MEB prob-lems, before they warrant a formal diagnosis, of-fer the best opportunity to protect young people. Such interventions can be integrated with routine healthcare and wellness promotion through policies and practices that target young people with specific risk factors; promote positive emotional develop-ment; and build on family, school, and community resources. Making use of the evidence-based in-terventions already at hand could potentially save
billions of dollars by preventing or mitigating disorders that would otherwise require expensive treatment.
Yet the nation’s approach has largely been to wait to act until a disorder is well-established and has already done considerable harm. All too often, op-portunities are missed to use evidence-based ap-proaches to prevent the occurrence of disorders, establish building blocks for healthy development, and limit the environmental exposures that increase
Preventing mental, emotional, and behavioral disorders among young people may be one of the best investments a society can make: The benefits include higher productivity, lower treatment costs, less suffering and premature mortality, and more cohesive families, as well as happier, better adjusted, and more successful young people.

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 9
risk — approaches that are likely to be far more cost-effective in addressing MEB disorders in the long run. Because risk factors tend to come in clusters and to be associated with more than one disorder, a focus on prevention and wellness can have far-reaching benefits that extend beyond a specific disorder.
Research has shown that a number of programs are effective at preventing these problems and promot-ing mental health. Meta-analyses and numerous randomized trials have demonstrated the value of:
>> Strengthening families by targeting problems such as substance use or aggressive behavior, teaching effective parenting skills, improving communication, and helping families deal with disruptions (such as divorce) or adversities (such as parental mental illness or poverty).
>> Strengthening individuals by building resilience and skills and improving cognitive processes and behaviors.
>> Screening to identify individuals at risk for some specific disorders, such as anxiety or de-pression, and making simple interventions such as cognitive training or social supports easily accessible.
>> Promoting mental health in schools by offer-ing support to children encountering serious stresses; modifying the school environment to promote prosocial behavior; developing stu-dents’ skills at decision making, self-awareness, and conducting relationships; and targeting vio-lence, aggressive behavior, and substance use.
>> Promoting mental health through health-care and community settings by supporting programs that teach coping skills, and target modifiable lifestyle factors that can affect be-havior and emotional health, such as sleep, diet, activity and physical fitness, sunshine and light, and television viewing.
The key to most of these approaches is to identify risks — biological, psychological, and social fac-tors — may increase a child’s risk of MEB disorders. Some of these risks reside in specific characteris-tics of the individual or family environment (such
can you tell us about your role on the IoM committee? I was on that committee because I’ve been a cli-nician for 30 years. I do business I’m a CEO of a comprehensive mental health center on the south side of Chicago and that gives a very different per-spective. I am a researcher, usually in high-risk set-tings, community psychiatry settings, urban poor, African-American, HIV, violence prevention, children exposed to violence, and trauma. And I have expe-rience translating academic efficacy and research-based science into real world settings.
Is the delay from research to implementa-tion a translation or funding issue?Both. They’re prevented from doing research with the process. NIMH is charged with research and SAMH-SA is charged with overseeing programs. It’s difficult to do research in a culture that is prevention defi-cient, illness-based, and overly focused on tertiary issues. And the bulk of what they are talking about is treatment prevention and not primary prevention.
Money is of course a problem, too! There is ample evidence in the report that says it’s likely that vio-lence can be prevented, drug abuse can be pre-vented, post partum depression can be prevented, and depression in children can be prevented. But how is it all funded?
What three recommendations from the re-port are likely to have the most impact?The first one would be to have the White House create a cabinet level group to put prevention into place in the U.S. A great example is how prevention of violence against women has worked with presi-dential support.
We’ve learned that children who are traumatized have twice the rates of cancer, twice the rates of heart disease, four times the rate of lung cancer, and twice the rates of liver disease because trauma causes children to eat, drink, smoke, and trade
sexual affections so they have triple the rate of HIC infection. There is evidence we can prevent children who experience trauma from participating in these behaviors as adults. This report could fix 1/3 of healthcare problem.
Then there is the issue of braided funding. If we could get CDC, NIH, NIDA, SAMHSA, and NIMH all working on prevention in concert, we would get somewhere with this.
the IoM had published a report on preven-tion in 1994. how is this new 2009 report an improvement?Science, tons and tons of science! This new report shows you how to implement this science for differ-ent socio-economic groups. We’re closer than we’ve ever been.
The other issue that is crystal clear is that now is the time! There are so many other things coming together that make this possible. There’s a tremen-dous amount of synergy between the brain science and the psycho-social science. The problem is that we haven’t put them together yet, but now is the time do it as the science has exploded.
Is there anything from the IoM report that is getting traction in the healthcare debate?Obama knows about the report. The problem is, Obama’s infrastructure hasn’t been in place yet. There has been a bit of pushback on some aspects of the report because some don’t want the govern-ment intrusion in their lives–a fear of big brother. It really takes presidential leadership to remind people of our interdependence!
What can leaders of community health cen-ters take away from this report? If they want to stay in business, they need to change their business. We’re in a different world. And if they don’t keep up with the times, they’re being unethical because the science is there.
Meena dayak, Director of Marketing and Communications and chris loftis, Phd, Director of Practice Improvement for the National Council for Community Behavioral Healthcare spoke to Dr. Carl C. Bell, member of the IOM Committee that authored the report on preventing mental, emotional, and behavioral disorders.
an Interview with carl Bell

10 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Policy Perspectives
as parental mental illness or substance abuse or serious family disruptions), but they also include so-cial stresses such as poverty, violence, lack of safe schools, and lack of access to healthcare. Most risk factors tend to come in clusters and are associated with more than one disorder.
Early symptoms typically occur two to four years before the onset of a full-blown disorder, creating a window of opportunity when preventive programs might make a difference. And some programs have shown effectiveness at preventing specific disorders in at-risk groups. For example, the Clarke Cognitive-Behavioral Prevention Intervention, which focuses on helping adolescents at risk for depression learn to cope with stress, has prevented episodes of ma-jor depression in several controlled experiments.
Other programs have demonstrated broader pre-ventive effects in populations of young people. Pro-grams that can be offered in family or educational settings show particular promise in promoting men-tal health and addressing major risk factors. One example of an effective school-based program is the Good Behavior Game, which divides elementary school classes into teams and reinforces desirable behaviors with rewards such as extra free time and
other privileges. Studies have
shown that the program significantly reduces ag-gressive and disruptive behavior during first grade. The one-year intervention also has benefits over the long term, lowering the students’ risk of alcohol and drug abuse, as well as rates of suicidal thoughts and attempts. And it significantly reduces the likelihood that highly aggressive boys will be diagnosed with antisocial personality disorder as adults. Research has shown that programs that focus on enhancing social and emotional skills can also improve stu-dents’ academic performance.
Other programs improve children’s mental health and behavior by enhancing parenting skills. The Positive Parenting Program, for example, uses a range of approaches, from a television series on how to handle common child-rearing problems to in-person skills training for parents struggling to handle children’s aggressiveness or lack of coop-eration. These methods have been shown to lower kids’ disruptive behaviors, a positive change that persisted one year later.
The IOM report emphasizes the value of promoting mental health and considering mental health within a developmental framework. The mental health re-search spectrum should include not just the preven-tion of MEB disorders, but also a focus on wellness the promotion of mental health. Good prevention
and mental wellness promotion interventions are grounded in research on the interrelationships among the principal milestones of healthy devel-opment and the family, school, and community fac-tors that are associated with them.
PolIcY IMPlIcatIonsOfficials at the local, state, and federal levels all play a role in mental health promotion and the pre-vention of MEB disorders. Many providers and agen-cies are responsible for the care, protection, or sup-port of young people: the child welfare, education, and juvenile justice systems, as well as medical and mental health care providers and community orga-nizations. Yet resources within these agencies are scattered, not coordinated, and often do not effec-tively support prevention programs or policies. The result is a patchwork that does not perform as an integrated system and fails to serve the needs of
many young people and their families.
National leadership is necessary to make sys-tematic prevention efforts a high priority in the healthcare system as well as an integral aspect of the network of local, state, and federal programs and systems that serve young people and families. The IOM report makes several recommendations, including::
>> A White House-created leadership body to devel-op an inter-departmental strategy that identifies specific prevention goals, directs multiple fed-eral agency resources toward these goals, and provides guidance to state and local partners (however, the report cautions that federal and state agencies should not support programs that lack empirical evidence, even if they have commu-nity endorsement).
>> Develop state and local systems that support partnerships among families, schools, courts, health care providers, and local programs to create coordinated approaches that support healthy development.
>> Invest in prevention and promotion, including setting aside resources for evidence-based pre-vention in mental health service programs and investment in proven prevention approaches by school systems.
>> Workforce training, including development of prevention training standards and training pro-grams across disciplines including health, edu-cation, and social work.
>> Long-term tracking of the prevalence and fre-quency of MEB disorders.
>> Implementation and evaluation of screening with community involvement, parental support, valid tools, and interventions to address identified needs.
>> Continued research on both the efficacy of new prevention models and real-world effectiveness of proven prevention and wellness promotion inter-ventions.
>> Adaptation of research-based programs to cul-tural, linguistic, and socioeconomic subgroups.

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 11
>> Public education, with mass media and the inter-net offering the opportunity to greatly expand the reach of specific messages about risk factors and available resources, to reduce stigma, and to de-liver some kinds of interventions.
role oF research Research has exploded in recent decades on efforts to prevent MEB disorders. Findings include improved understanding of the origins of MEB disorders and advances in methodological approaches that al-low causal inferences to be drawn from evaluations of preventive interventions and to track effects over multiple years. Many interventions have been tested in multiple randomized trials and show long-term reductions in MEB disorders and related problem be-haviors, such as aggression, high-risk sexual behavior, and substance use, as well as such positive outcomes as improved grades and higher self-esteem.
Neuroscience research may lead to early identifica-tion of specific young people at risk for MEB disorders and to the refinement of specific, targeted interven-tions. Related research has identified opportunities to change environments in ways that might influence the expression of specific genetic or biological pre-dispositions, for both current generations and their offspring.
The report encourages more collaboration between traditional prevention and wellness researchers with developmental neuroscientists in order to widen the body of research focused on advancing health and preventing disorders, rather than the more traditional emphasis of research focused on diagnosed disorders after they are well established and have done consid-erable harm. Greater collaboration between research fields—specifically, the testing of hypotheses across the disciplines—will yield both theoretical and practi-cal advances in prevention.
The IOM report also urges continued research to build understanding of what interventions work for whom and when, and how best to implement them. The National Institutes of Health should develop a com-prehensive 10-year plan to research ways to promote mental health and prevent MEB disorders in young people. In addition, agencies and foundations should establish equality in research funding between ways
to prevent mental and behavioral disorders and ways to treat these problems, the report says; currently, the balance is weighted toward research on treatment.
coMMunItY releVanceInterventions are unlikely to be implemented, or implemented with fidelity, if they are not respon-sive to community needs and priorities. Communi-ties often have substantial expertise and professional wisdom but have developed approaches that are not supported by empirical evidence. Researchers and communities need to develop partnerships to evalu-ate interventions that have both a solid theoretical grounding and are responsive to community needs. Increasing relevance to a community also calls for consideration of such other issues.
Adaptation: The effectiveness of evidence-based in-terventions may be significantly facilitated or impeded by aspects of the ethnic, linguistic, and cultural envi-ronment in which they are implemented. Research is needed to identify the specific factors that influence effectiveness and the adaptations that are needed to serve different populations.
Screening in conjunction with intervention: Screen-ing can be done in a number of ways and for a variety of risk and early symptoms. Community acceptance, parental endorsement, and the capacity to respond to needs that are identified are critical to its value. Re-search on the effectiveness of linking screening with
evidence-based intervention is needed.
Economic analyses: Funding for prevention programs is increasingly made in an environment of decreased resources. Evidence of the economic benefits of pre-ventive interventions is a critical policy tool. Yet, many research designs do not include information about the costs of an intervention against which a commu-nity could weigh the benefits. Even fewer include cost-effectiveness analyses. Guidelines for conducting this type of analysis, as well as incentives for researchers to conduct it, are necessary.
Copies of Preventing Mental, Emotional, and Behav-ioral Disorders Among Young People: Progress and Possibilities are available from the National Acad-emies Press; 202.334.3313 or 800.624.6242 or at www.nap.edu.
Carl C. Bell is president and CEO of the Community Mental Health Council & Foundation, Inc. in Chicago. He is also the director of public and community psychiatry and a clinical professor of psychiatry and public health, University of Illinois at Chicago. He is a member and former chairman of the National Medical As-sociation’s Section on Psychiatry; a fellow of the American College of Psychiatrists; a fellow of the American Psychiatric Association, a founding member and past board chairman of the National Commission on Correctional Health Care. Dr. Bell has published more than 350 articles on mental health.
Meena Dayak has 15+ years of experience in marketing and public relations for nonprofit healthcare organizations. She leads National Council efforts to help consumers and providers tell a compelling story so that the world will recognize that mental illnesses and addictions are treatable health conditions from which people can recover and lead full lives. Prior to joining the National Council, she managed marketing initiatives for healthcare standards and information programs at the United States Pharmacopeia.
Chris Loftis offers practice improvement and legislative guidance to the National Council’s more than 1,600 member organizations that provide treatment and rehabilitation to individuals with men-tal illnesses and addiction disorders. Loftis has served as a policy analyst for the National Health Policy Forum in Washington, DC, a nonpartisan organization that provides health policy programming for senior staff in Congress and the executive agencies. He also has worked as a practitioner and researcher, and has completed advanced specialty training in pediatric neuropsychology. Loftis has a doctorate in clinical psychology with a specialization in neu-ropsychology from the University of Florida and completed a clini-cal internship at the Kennedy Krieger Institute at Johns Hopkins in Baltimore, MD, where he worked with children with traumatic injuries, developmental disabilities, and chronic illnesses.
Nathan Sprenger, the National Council’s marketing and communi-cations associate, provided administrative and research support for this article and interview.

12 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Policy Perspectives
J uan was a delivery driver, but his health prob-lems were putting him at risk of losing his job.
His diabetes was poorly controlled and had caused foot ulcers that made it difficult for him to walk. He also had bipolar disorder, which was not being con-trolled. When he joined the Working Well program in Harris County, Texas, Juan worked with a case man-ager to get orthopedic shoes, to receive support in developing a diabetic diet and exercise plan, and to make an appointment with a psychiatrist to bring his mental health condition under control. As a re-sult, Juan was able to continue working full time as a delivery driver and received a raise for exceptional performance (Bohman, Stoner, & Chimera, 2009).
Working Well is part of the Demonstration to Main-tain Independence and Employment, which is funded by the Centers for Medicare and Medicaid Services. The DMIE is one of the federal initiatives currently evaluating the impact of earlier intervention for people with mental illnesses (earlier interventions in the context of this article refer to interventions prior to application for Social Security Benefits but do not include first onset interventions).
Current federal policy provides support, through So-cial Security Disability Insurance and Supplemental
Security Insurance, for people who are no longer able to work. These programs, in turn, act as gate-ways to health insurance — Medicare in the case of SSDI and Medicaid for those who quality for SSI. This safety net is vital for people who are too disabled to work. Once people qualify for Social Security, how-ever, they rarely move off it, despite strong evidence that many people with mental health problems want to and can work. People with mental illnesses now constitute the largest and most rapidly growing
group of Social Security disability beneficiaries, and every year only 1 percent of people who qualify for SSDI on the basis of a mental illness leave the rolls and return to work.
The DMIE represents a break with existing policy. Its purpose is to actively support people who are at risk of becoming too disabled to work, so that they
can remain in their jobs and do not apply for public disability programs. Two of the demonstration sites, Texas and Minnesota, focus on people with serious mental illnesses and people with chronic physical health problems who also have a mental health condition. The ingredients that make up the service packages in Minnesota and Texas are similar: com-prehensive health insurance, including dental and vision services as well as behavioral health benefits; employment supports; and a “broker” who works
with participants to help them keep their jobs. The broker’s role is broad; it can range from helping a participant get an appointment with a psychiatrist to finding him or her a place to live to organizing child care (Gimm & Weathers, 2007).
Early results are promising. In Minnesota, the DMIE intervention is proving to be effective in improving
The Demonstration to Maintain Independence and Employment,
funded by CMS, is evaluating the impact of actively supporting people
with mental illnesses who are at risk of becoming too disabled to
work, so that they can remain in their jobs. The intervention is proving
to be effective in improving clients’ access to healthcare services,
health and functional status, job stability, and earnings.
This article represents the views of the author and not those of the U.S. Department of Health and Human Services.
Vidhya alakeson, Policy Analyst, Office of the Assistant Secretary for Planning and Evaluation, Department of Health and Human Services
Saving Jobs, Saving Public Dollars:
Intervening Before Disability

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 13
clients’ access to healthcare services, health and functional status, job stability, and earnings. It has also reduced the number of applications for SSDI (Linkins & Brya, 2009). Analysis indicates that earlier interventions, such as the DMIE, could make sound financial sense for the federal government as well as for clients. A new study by Drake, Skinner, Bond, and Goldman (2009) concluded that providing integrated behavioral healthcare and supported employment to a third of Social Security applicants with mental health conditions to help them return to work and stay off the disability rolls could save the government $48 million in providing all the necessary services.
One of the challenges of adopting a more comprehen-sive approach to earlier intervention is the absence of strong evidence as to how to effectively support people before they become Social Security beneficia-ries. DMIE is one federal effort to address this evi-dence gap; the Recovery After an Initial Schizophrenia Episode program is another. RAISE is a major new initiative from the National Institute for Mental Health that will be launched this summer. For most people, the first onset of schizophrenia occurs in adolescence or early adulthood. Emerging evidence suggests that intervening at this point can reduce the likelihood that a patient will develop full-blown schizophrenia, but researchers have not reached a consensus as to which early interventions work best. RAISE will test two sets of interventions to assess whether they can effectively prevent the development of the condition and reduce long-term disability as a result of mental illness.
Research has indicated other opportunities for earlier intervention to prevent long-term dependence on dis-ability programs. A recent study by the Urban Institute showed that close to 14 percent of recipients of Tem-porary Assistance for Needy Families have an emotion-al or mental health problem (Loprest & Maag, 2009). States have to meet strict work participation criteria for the TANF population, and participation in mental health treatment does not qualify as work participa-tion. As a result, it is often in the state’s interest to try to move women with mental health problems and other disabilities onto SSI. A focus on earlier interven-tion, by contrast, would seek to address the mental health needs of women on TANF and support them
back into work, following the principle that economic self-sufficiency is in the best interest of their families. The Social Security Administration is currently working with the Administration for Children and Families to look in greater depth at the movement of beneficia-ries between TANF and SSI.
Drake et al. (2009) concluded their analysis of the potential savings from earlier intervention with sev-eral policy proposals. First, they suggested that states provide supported employment and mental health services early in the course of mental illness. Initia-tives such as the DMIE and RAISE are testing that approach. Second, they suggested that health insur-ance be delinked from disability status. The two rec-ommendations are intimately connected. For people with any kind of chronic condition, including a men-tal illness, access to healthcare is vital. The only way some people can access healthcare is to qualify for disability benefits. Fear of losing healthcare then be-comes a major barrier to moving off benefits. In this respect, current discussions around extending health insurance to the uninsured are particularly important. Earlier intervention will only take hold if patients have a route to accessing healthcare that does not depend
on qualifying for disability benefits.
Vidhya Alakeson is a policy analyst in the Office of the Assistant Secretary for Planning and Evaluation at the Department of Health and Human Services where she leads work on mental health and disabilities. Prior to taking up this position in 2008, she was a Harkness Fellow in Healthcare Policy based at HHS and supported by the Commonwealth Fund in New York. Prior to working in the US, Vidhya worked for the UK Government and in several leading UK think tanks conducting policy research in the areas of health, human services, and education. She has a first class degree from Oxford University and a masters from the London School of Economics.
REfEREncESBohman, T., Stoner, D., & Chimera, D. (2009, April). Working Well: Preliminary findings. Paper presented at the Centers for Medicare and Medicaid Services MIG/DMIE Employment Summit, San Francisco.
Drake, R. E., Skinner, J. S., Bond, G. R., & Goldman, H. H. (2009). Social Security and mental illness: Reducing disability with sup-ported employment. Health Affairs,28, 761−770.
Gimm, G., & Weathers, B. (2007). What is the Demonstration to Maintain Independence and Employment (DMIE) and who is participating? Princeton, NJ: Mathematica Policy Research.
Linkins, K., & Brya, J. (2009, April). MN DMIE: The role of personal navigation and employment supports in client outcomes. Paper presented at the CMS MIG/DMIE Employment Summit, San Francisco.
Loprest, P., & Maag, E. (2009). Disabilities among TANF recipi-ents: Evidence from the NHIS, Washington, DC: Urban Institute.
Providing integrated behavioral healthcare and supported employment to a third of Social Security applicants with
mental health conditions to help them return to work and stay off the disability rolls could save the government $48 million in
providing all the necessary services.
A program ofVietnam Veterans of America
Veterans & Their Families:
WHAT YOURHealthCareProviderSHOULD KNOW…
www.veteranshealth.org
10706 VVA.mech2:magazine ad 6/5/09 4:40 PM Page 1

14 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Policy Perspectives
T he Substance Abuse and Mental Health Ser-vices Administration reached out to hundreds
of stakeholder and consumer groups and dozens of nationally and internationally recognized experts in the fields of mental health and addictions to solicit insight and recommendations on the most critical issues related to mental and substance use dis-orders facing the American population today, with an emphasis on identifying opportunities to ensure that imminent health reform efforts include preven-tion and treatment for these disorders.
With consistency and solidarity, mental health and substance abuse professionals, consumers, and family members from every part of the country, every cultural and socioeconomic group, and every diag-nosis and condition spoke with a single voice: “Our nation is crying out for a health system that makes prevention and treatment for mental and substance use disorders a priority rather than an afterthought, that considers the whole person rather than physi-cal symptoms alone, and that seeks to eliminate the stigma and fragmented systems that interfere with Americans’ ability to access necessary preven-tive and treatment services fundamental to achiev-ing recovery and enabling them to lead healthy and productive lives.”
Based on stakeholder input, SAMHSA has developed a set of NINE CORE CONSENSUS PRINCIPLES:
Our nation needs a national health and wellness plan that provides for comprehensive, community-wide prevention, screening, health, and wellness services from infancy through old age. The plan should provide for public education, prevention, early intervention, treatment, and recovery services, and must be a holistic, standardized system that emphasizes promoting wellness and resilience, pre-venting risky and unhealthy behaviors before they occur to avoid the onset of illness or drug use, and addressing symptoms when they first emerge rather
than waiting until they become acute or chronic.
The national plan should utilize a public health model for prevention that organizes multiple com-munity sectors to plan, implement, and evaluate appropriate strategies and programs designed to change community norms and environments to promote healthy choices and behaviors. Universal screening tools should be used to detect medical conditions including mental and substance use dis-orders early and treat them at a low level of acuity. These approaches will slash billions of dollars from annual healthcare costs and dramatically improve the overall health of Americans.
Equal treatment for people with serious mental illness and substance use disorders must mean access to effective services and high-quality care. Children and adults with mental and substance use disorders are medically vulnerable populations. Many will not access needed primary health care or comply with medical treatment without signifi-cant support. Mechanisms developed under health reform to expand coverage for currently uninsured populations must require compliance with the new parity law. Similarly, the discriminatory IMD exclu-sion under Medicaid must be modified.
Achieving universal coverage will also help to pro-mote health equity and increase access by requiring that priority attention be given to populations dis-proportionately affected by chronic disease. Such populations include racial and ethnic minorities, groups with low socioeconomic status, residents of rural areas, chronically unemployed populations, women, children, older adults, persons with multiple chronic conditions, persons with disabilities, and criminal and juvenile justice–involved populations. Health reform must recognize the need for special-ized mental and substance use disorders services to enable these populations to benefit from health-care coverage.
There is a substantial body of evidence to demon-strate that providing adequate levels of mental and substance use disorders prevention and treatment services as well as integrating these services with primary healthcare can improve outcomes; cut and/or control the growth of overall healthcare costs; lessen the rate, duration, and intensity of dis-ability of many illnesses; improve productivity; and control the size and growth of other social costs. By including information about preventing as well as detecting mental and substance use disorders in primary healthcare, institutional, and community settings, we create an environment that enables early, low-cost treatment, thereby avoiding escala-tion to expensive, urgent-care facilities; minimizing impact to family members, workmates, and others; and reducing the likelihood of lasting adverse ef-fects to the consumer. Further, this cultivates a whole-health, person-centered approach that fos-ters not only recovery but also resilience.
Excerpts from SAMHSA’s “A Framework for Discussion: Ensuring U.S. Health Reform Includes Prevention and Treatment of Mental and Substance Use Disorders: Core Consensus Principles for Reform from the Mental Health and Substance Abuse Community” at www.samhsa.gov/Healthreform/docs/HealthReformCoreConsensusPrinciples.pdf
Call to Include Prevention in Healthcare Reform
1 articulate a national health and Wellness Plan for all americans
2 legislate universal coverage of health Insurance with Full Parity
3 achieve Improved health and long-term Fiscal sustainability
4 eradicate Fragmentation by requiring coordination and Integration of care for
Physical, Mental, and substance use conditions
Our nation is crying out for a health system that makes prevention and treatment for mental and substance use disorders a priority rather than an after-thought, that considers the whole person rather than physical symptoms alone, and that seeks to eliminate the stigma and fragmented systems that interfere with Americans’ ability to access necessary preventive and treatment services funda-mental to achieving recovery and enabling them to lead healthy and productive lives.”

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 15
Complicating the challenges faced by the current treatment system for mental and substance use disor-ders is the frequent co-occurrence of these disorders, often together with other chronic health conditions. Our current system promotes disconnection among interrelated diseases and conditions leading to frag-mentation and frustration among providers and con-sumers. The presence of multiple concurrent health conditions makes it increasingly difficult to engage consumers successfully in treatment and sustained recovery.
Provide for a Full Range of Prevention, Early Interven-tion, Treatment, and Recovery Services that Embodies a Whole-Health Approach
Addressing physical health including mental and sub-stance use disorders through effective prevention ef-forts that promote healthy environments, norms, and behaviors rather than waiting for the development of full-blown acute or chronic diseases is the most cost-effective approach. It is essential that any health reform regard mental and substance use disorders as chronic diseases that are preventable, treatable, and often co-occurring with other physical illnesses. As with other chronic ailments such as asthma or diabe-tes, they may require lifelong management; but those who experience these disorders can achieve recovery and lead full, healthy, and productive lives in the com-munity with the proper supports. Managing chronic disease has also been shown to be essential to long-term fiscal sustainability of any health reform plan.
Reimbursement guidelines and benefits should be tied to need and severity regardless of payer. These guidelines must link quality improvement with reim-bursement and both encourage and reward the use of evidence-based practices without restricting cover-age for those consumers who may not achieve desired outcomes with the least-costly alternative. Compara-tive effectiveness may be one consideration in making treatment decisions, but not be the wholesale substi-tute for the many factors that should be considered for coverage. Promoting health equity, especially for populations disproportionately affected by chronic
disease, needs to be a key consideration if health reform is to succeed with achieving improved health outcomes. Accordingly, we must invest in research and accelerate the transfer of new science and anecdotal reports into evidence-based practices that take into account diverse populations.
Our reformed health system must build on the in-creasing availability of HIT to provide a system of electronic health records that is universally available, affordable, and accessible to large and small provid-ers nationwide and is one that provides for captur-ing overall health information including both physical health and mental health and substance use. EHRs allow the sharing of information across providers and facilitate care coordination, while also enabling national and regional data collection to monitor and measure access to and cost effectiveness of care. To maximize the value of these tools, a uniform language and format are required, and consumers must retain control and ownership of their health data.
Lack of adequate healthcare for mental and sub-stance use conditions is a constant cycle exacerbated by a system that has failed to grow with the needs of a quickly expanding society and has not equipped its workforce with the right tools and experience to provide sorely needed care. Because there are simply too few specialists in mental and substance use dis-orders available, large numbers of Americans who re-quire services for serious mental or substance abuse disorders receive them from general health care practitioners, who largely lack training in mental and substance use disorders prevention, treatment, and recovery services. It must become a national priority to increase the mental and substance use disorders workforce and provide appropriate compensation and professional support for these key members of the U.S. health system. Such incentives as loan forgive-ness may attract professionals to train in the mental health and addictions fields, and increased funding for graduate medical education will expand the avail-ability of psychiatric training programs. We must also develop a national, centralized credentialing and privileging system across all payers, and a national system for clinician licensing and the licensing and regulation of care delivery systems.
Locating and dedicating the funds needed to bring about health reform will, by necessity, result in in-creased pressures to shift funding away from exist-ing strategies and services and instead to repurpose these resources toward new healthcare reform pri-orities. Prevention has historically been underutilized and under-resourced in relation to its potential to cut healthcare costs. In addition, far too many Americans with diagnosable mental and substance use disorders already do not have access to treatments and ser-vices that are known to be effective. We can ill afford to dismantle the current safety net of block grants to states and other resources that in many states and communities are the only blockade between even higher rates of risky behaviors, illness, disability, death, healthcare costs, and lost productivity. Assum-ing expanded access to private and public insurance (Medicaid) for people with mental and substance use disorders will require a reexamination of the role of the public system at the local, state, and federal levels. Absent clear evidence that newly substituted health reform programs, systems, and processes are fully implemented and effective, it is imperative that our nation’s current safety net that finances health services, including school and community-based pre-vention programs and treatment programs for mental and substance use disorders, not be dismantled pre-maturely.
Healthcare reform is indeed a moral imperative — but it will be meaningless if it does not incorporate men-tal and substance use disorders prevention and treat-ment as central to national wellness. Screening and early intervention, access to and funding of compre-hensive services, and lifelong care mean lower health costs for individuals, communities, and the nation. We can no longer dismiss the connection between men-tal health, addiction, and medical health and before us now is an unprecedented opportunity to build and traverse the bridge between the two.
By making prevention, early intervention, and treat-ment of mental and substance use disorders a health priority, we will not only reduce costs and strain on our systems, but will also create stronger families, stron-ger communities, and a stronger nation.
5 Provide for a Full range of Prevention, early Intervention, treatment, and recovery ser-
vices that embodies a Whole-health approach
6 Implement national standards for clinical and Quality outcomes tied to reimburse-
ment and accountability
8 Invest in the Prevention, treatment, and recovery support Workforce
9 ensure a safety net for People with the Most serious and disabling Mental and
substance use disorders
7 adopt and Fully utilize health Information technology

Evidence-Based Early Interventions
16 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Healthy Minds, Strong communities
L aunching a new program is a bit like eating an elephant. Even though you’ve got a great vision and a huge goal, you still have to
tackle it one bite at a time.
That’s the approach the National Council has taken with launching Mental Health First Aid in the United States. We envision Mental Health First Aid becoming as commonplace as CPR and First Aid within the next fifteen years. Some may call that an elephant, but the results of our first program year demonstrate that the challenge is immensely doable especially with a few extra-large bites.
Since it’s launch last year, more than 300 instructors have been certified in Mental Health First Aid, a program that builds mental
health literacy and teaches non-clinicians basic skills in how to help someone experiencing a mental health problem or crisis. A Mental Health First Aider learns to provide assistance until
the problem resolves or until other appropriate help is engaged.
“It’s evident that Mental Health First Aid is the right program coming at the right time,” says Linda Rosenberg, president and CEO of the National Council. “When we began this initiative, we were hoping to
lea ann Browning Mcnee, Outreach and Development Officer and susan Partain, Outreach Associate — National Council for Community Behavioral Healthcare
Mental health First aid usaEducates and Transforms Communities, 3,000 Trained in One Year
Mental Health First Aid USA by the Numbers
300 instructors certified 33 states running the program
180+ community trainings 3,000 individuals trained
1,000,000 media impressions

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 17
Mental Health First Aid was created in 2000 by Profes-sor Anthony Jorm, a respected mental health literacy professor, and Betty Kitchener, a nurse specializing in health education, to improve the mental health lit-eracy of members of the Australian community. The program is auspiced at the ORYGEN Research Center at the University of Melbourne, Australia.
Mental Health First Aid includes a 5-day instructor training course to certify suitable candidates to be-come MHFA instructors who deliver the 12-hour MHFA course to their communities. This 12-hour course is designed to give members of the public some skills to help someone developing a mental health problem or in a mental health crisis situation. The philosophy behind the course is that mental health crises, such as suicidal and self-harming actions, may be avoided through early intervention with people developing mental disorders. If crises do arise, then members of the public can take action to reduce the harm that could result.
To date, Mental Health First Aid has been replicated in Cambodia, Canada, England, Finland, Hong Kong, Japan, New Zealand, Northern Ireland, Scotland, Sin-gapore, South Africa, Thailand, USA, and Wales.
The National Council for Community Behavioral Healthcare, the Maryland Department of Health and Mental Hygiene, and the Missouri Department of Mental Health chose to help bring Mental Health First Aid to the USA due to the strong evidence supporting the program.
Five published studies, based on effectiveness trials and qualitative surveys in Australia, show that Men-tal Health First Aid saves lives, improves the mental health of the individual administering care and the one receiving it, expands knowledge of mental ill-nesses and their treatments, increases the services provided, and reduces overall stigma by improving, mental health literacy.
One trial of 301 randomized participants, 5-6 months after they received Mental Health First Aid training, found that those who trained have greater confidence in providing help to others, greater likelihood of advis-ing people to seek professional help, improved con-cordance with health professionals about treatments, and decreased stigmatizing attitudes. Studies also found that Mental Health First Aid improved the men-tal health of the participants themselves.
In summary, Mental Health First Aid has been proven to improve
KNOWLEDGE: Improved agreement with health professionals about treatments.
BEHAVIOR: Improved helping behavior
INTENTIONS: Greater confidence in providing help to others
ATTITUDES: Decreased social distance from people with mental disorders.
Mental health First aid: history and evidence Base
certify about twenty organizations to introduce Mental Health First Aid in their communities. As of this summer — the end of our official pilot year we have nearly one hundred fifty organizations offering the program.”
The growth of the program has not surprised many of the National Council’s board leaders, who were among the first to adopt Mental Health First Aid. “The multiple wins of the program were obvious from the start,” says Dr. Carl Clark, first vice chair of the National Council Board and CEO of the Mental Health Center of Denver, one of the initial pilot sites. “We can enhance community resilience, offer potential partners an easy-to-understand service, broaden our focus beyond serious mental illness, and further secure our role as community problem-solvers.”
Don Miskowiec of North Central Behavioral Health Systems agrees. “Even though we’re dealing with devastating and demanding budget cuts here in Illinois, we are committed to Mental Health First Aid. If anything, it’s even more necessary in our current environment.” After participating in the initial training, Miskowiec’s center added six additional instructors to his team for 2009.
The program focuses on three key elements: recognizing warning signs, increasing skills to help individuals reach out to those with mental health challenges, and understanding how professional and self-help supports can help.
From hospitals and the workplace to college campuses and the general public, Mental Health First Aid address-es not only stigma, but also the real desire to help someone who is struggling. “ Mental Health First Aid makes it okay to reach out,” explains Rosenberg. “So often people want to help, but we’re not sure what to do and don’t
“Mental Health First Aid — with it’s new
emphasis on recovery — has the power
to transform communities, the power to
change beliefs, and the ability to con-
nect people in ways they never would
have connected otherwise.”
Larry Fricks National Consumer Leader
“What struck me most about Mental
Health First Aid is the interest it gener-
ates among people who don’t have a
direct connection to the mental health
field,” says David Johnson, CEO of the
Bert Nash Center. “It’s obvious that this
is a program than can move us beyond
usual constituencies to truly build a
healthy community.”
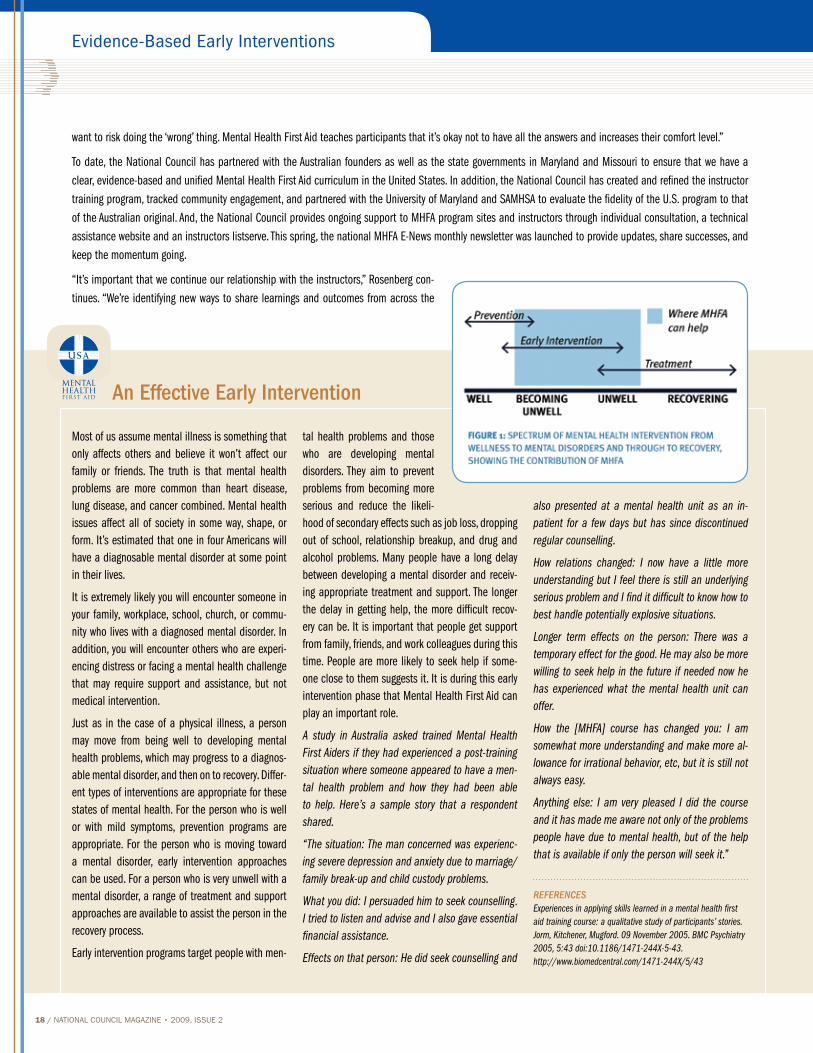
Evidence-Based Early Interventions
18 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
want to risk doing the ‘wrong’ thing. Mental Health First Aid teaches participants that it’s okay not to have all the answers and increases their comfort level.”
To date, the National Council has partnered with the Australian founders as well as the state governments in Maryland and Missouri to ensure that we have a clear, evidence-based and unified Mental Health First Aid curriculum in the United States. In addition, the National Council has created and refined the instructor training program, tracked community engagement, and partnered with the University of Maryland and SAMHSA to evaluate the fidelity of the U.S. program to that of the Australian original. And, the National Council provides ongoing support to MHFA program sites and instructors through individual consultation, a technical assistance website and an instructors listserve. This spring, the national MHFA E-News monthly newsletter was launched to provide updates, share successes, and keep the momentum going.
“It’s important that we continue our relationship with the instructors,” Rosenberg con-tinues. “We’re identifying new ways to share learnings and outcomes from across the
Most of us assume mental illness is something that only affects others and believe it won’t affect our family or friends. The truth is that mental health problems are more common than heart disease, lung disease, and cancer combined. Mental health issues affect all of society in some way, shape, or form. It’s estimated that one in four Americans will have a diagnosable mental disorder at some point in their lives.
It is extremely likely you will encounter someone in your family, workplace, school, church, or commu-nity who lives with a diagnosed mental disorder. In addition, you will encounter others who are experi-encing distress or facing a mental health challenge that may require support and assistance, but not medical intervention.
Just as in the case of a physical illness, a person may move from being well to developing mental health problems, which may progress to a diagnos-able mental disorder, and then on to recovery. Differ-ent types of interventions are appropriate for these states of mental health. For the person who is well or with mild symptoms, prevention programs are appropriate. For the person who is moving toward a mental disorder, early intervention approaches can be used. For a person who is very unwell with a mental disorder, a range of treatment and support approaches are available to assist the person in the recovery process.
Early intervention programs target people with men-
tal health problems and those who are developing mental disorders. They aim to prevent problems from becoming more serious and reduce the likeli-hood of secondary effects such as job loss, dropping out of school, relationship breakup, and drug and alcohol problems. Many people have a long delay between developing a mental disorder and receiv-ing appropriate treatment and support. The longer the delay in getting help, the more difficult recov-ery can be. It is important that people get support from family, friends, and work colleagues during this time. People are more likely to seek help if some-one close to them suggests it. It is during this early intervention phase that Mental Health First Aid can play an important role.
A study in Australia asked trained Mental Health First Aiders if they had experienced a post-training situation where someone appeared to have a men-tal health problem and how they had been able to help. Here’s a sample story that a respondent shared.
“The situation: The man concerned was experienc-ing severe depression and anxiety due to marriage/family break-up and child custody problems.
What you did: I persuaded him to seek counselling. I tried to listen and advise and I also gave essential financial assistance.
Effects on that person: He did seek counselling and
also presented at a mental health unit as an in-patient for a few days but has since discontinued regular counselling.
How relations changed: I now have a little more understanding but I feel there is still an underlying serious problem and I find it difficult to know how to best handle potentially explosive situations.
Longer term effects on the person: There was a temporary effect for the good. He may also be more willing to seek help in the future if needed now he has experienced what the mental health unit can offer.
How the [MHFA] course has changed you: I am somewhat more understanding and make more al-lowance for irrational behavior, etc, but it is still not always easy.
Anything else: I am very pleased I did the course and it has made me aware not only of the problems people have due to mental health, but of the help that is available if only the person will seek it.”
REfEREncESExperiences in applying skills learned in a mental health first aid training course: a qualitative study of participants’ stories. Jorm, Kitchener, Mugford. 09 November 2005. BMC Psychiatry 2005, 5:43 doi:10.1186/1471-244X-5-43. http://www.biomedcentral.com/1471-244X/5/43
an effective early Intervention

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 19
Mental Health First Aid USA runs a 5-day instructor training program to certify trainers from community-based organizations that then offer the public 12-hour Mental Health First Aid program to target audiences in their local area. Each Mental Health First Aid site develops individualized plans to reach their commu-nities, but all deliver the core 12-hour program and each participating site undergoes tight credentialing to guarantee fidelity to the original, tested model, while also maintaining the flexibility necessary to reach its unique citizens’ needs and demographics. Sites receive significant support from the National Council for ongoing implementation of Mental Health First Aid through individual consulting, national track-ing and monitoring, continuous networking with other sites and instructors, teaching materials, tips and re-sources for funding and marketing, and more.
The interactive 12-hour program can be conducted as one 2-day seminar, two 1-day events, or four 3-hour sessions. Mental Health First Aid certification must be renewed every three years, and introduces par-ticipants to risk factors and warning signs of mental health problems, builds understanding of their impact and overviews common treatments.
Knowledge and skills serve us well in navigating an emergency, and can potentially prevent a medical emergency through early intervention. Mental Health First Aid aims to do both — teach members of the
public how to respond in a mental health emergency, and offer support to someone who appears to be in emotional distress.
Mental Health First Aid offers education on signs and symptoms of a variety of diagnosable mental disor-ders. It describes, in detail, how a “Mental Health First Aider” can assume a helpful role when encountering a distressed individual, the program is not used to diagnose or to replace a therapist. Mental Health First Aid recognizes that just as with physical health, people may use many effective alternative and com-plementary strategies to recover from mental health challenges.
Specifically, Mental Health First Aid participants learn:
>> The potential risk factors and warning signs for a range of mental health problems, including: de-pression, anxiety/trauma, psychosis and psychotic disorders, eating disorders, substance use disor-ders, and self-injury
>> An understanding of the prevalence of various mental health disorders in the U.S. and the need for reduced stigma in their communities
>> A 5-step action plan encompassing the skills, re-sources and knowledge to assess the situation, to select and implement appropriate interventions, and to help the individual in crisis connect with appropriate professional care
>> The evidence-based professional, peer, social, and self-help resources available to help someone with a mental health problem.
Mental health First aid certification & 12-hour Program
Who Can Be A Mental Health First Aider
From policymakers to the general public, a broad array of audiences is interested in Mental Health First Aid. To date, the following groups have received training in the USA
>> Educators/School administrators
>> Employers
>> Faith communities
>> Homeless shelters
>> Hospitals and primary care health centers
>> Law enforcement/other first responders
>> Mental health authorities
>> Nursing homes
>> Policymakers
>> Substance abuse professionals
>> Families and caring citizens
country and connecting to common needs, such as supplemental programs and standardized evaluation tools.”
Recognizing that the popularity of Mental Health First Aid also increases the need for significant support, capacity and branding, Rosenberg emphasizes that the National Council is in this for the long haul. She calls the pilot’s success “both fulfilling and a little intimidating.” Perhaps a bit like eating an elephant.
BRING IT TO YOUR COMMUNITYLearn more about Mental Health First Aid at www.MentalHealthFirstAid.org. To find out about bringing the program to your community, please contact Susan Partain at [email protected] or 202.684.7457 ext. 232.

Evidence-Based Early Interventions
20 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
coMMunItY outREAcH
The National Council has certified instructors from more than 180 organizations in the USA. Here’s a snapshot of where some of our pilot sites are with rolling the program out in their communities.
BERT NASH CENTERPartnering with the Chamber of Commerce was just the first step in launching Mental Health First Aid in Lawerence, Kansas. The group had the program added to the curriculum of the Chamber’s Leadership Lawrence program, reaching diverse community leaders from the fields of business, academics, and finance. The Center also launched a comprehensive pub-lic outreach program, certified additional MHFA instructors and their efforts were recently featured on Kansas Public Radio.
COMMUNITY COUNSELING CENTERS OF CHICAGO (C4) Since certifying two instructors in February 2008, C4 has trained more than 100 community members throughout Chicago in Mental Health First Aid, focusing their efforts on training a variety of community members including employees, volunteers at homeless shelters, and substance abuse and addictions groups. Partnering with fellow pilot site North Central Behavioral Health, C4 certified six additional instructors in December 2008 to expand their MHFA offerings in the Chicago area in 2009.
GATEWAY HEALTHCAREFrom partnering with law enforcement to reaching employers, Gateway has made tremen-dous headway in certifying a large number of key groups throughout Rhode Island as Mental Health First Aiders. Since last April, their partnership with the Rhode Island Municipal Police Academy has certified more than 100 officers from all over the state, including members of security forces from colleges and universities. Gateway also secured support of their community programs through Blue Cross Blue Shield of Rhode Island. Blue Cross recently featured the program in their quarterly magazine to all of their members and stakeholders across the state.
NORTH CENTRAL BEHAVIORAL HEALTH SYSTEMSIn their first six months, NCBHS made incredible headway in improving understanding of mental health among Illinois residents, certifying more than 130 Mental Health First Aiders, including hospital personnel, educators, and members of the general public. In December 2008, NCBHS certified six additional instructors to enable expansion of their program even further in 2009.
IOWA DEPARTMENT OF HUMAN SERVICES, DIVISION OF MENTAL HEALTHIowa holds the distinction of the only state to have its mental health commissioner certified as a MHFA instructor. After that initiation, Iowa formed a strategic plan to reach 7,500 state residents with MHFA in a single year. So far, they are well on their way, hosting two statewide instructor training programs that included the National Guard, emergency services, higher education, and nursing in addition to mental health and addictions professionals.
SEMINOLENot content to merely serve their own community, Seminole took the lead in creating a comprehensive Mental Health First Aid initiative across the state of Florida. Last fall, the agency hosted an instructor training of 24 additional instructors to expand efforts.
alasKaCenter for Rural HealthDenali Family ServicesDHSS Behavioral Health/Prevention Early
Identification Services OfficeState of Alaska Division of Behavioral Health
arIZonaCommunity Partnership of Southern ArizonaNAMI Phoenix
calIFornIaAsian Americans for Community Involvement
(Catholic Charities)Bill Wilson Center (Catholic Charities)Mental Health America of San Diego County
coloradoArapahoe/Douglas Mental Health NetworkAurora Mental Health CenterCentennial Mental Health CenterColorado West Regional Mental Health Center Community Reach CenterConnectionsJefferson Center for Mental Health Larimer Center for Mental Health Mental Health Center of DenverMental Health Center Serving Boulder and
Broomfield CountiesNCMC Foundation, IncNorth Range Behavioral HealthPikes Peak Mental HealthRed CrossWICHE Mental Health Program
connectIcutAbility Beyond DisabilityBridges MilfordUnited Services, Inc.Yale Department of Psychiatry
FlorIdaAmerican Foundation for Suicide PreventionCircles of CareDepartment of Children and FamiliesFlorida Council for Community Mental HealthFlorida Department of Children and Families
through July 15, 2009
sites trained in Mental health First aid by the national council

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 21
Florida Partners in CrisisLakeside Behavioral HealthMeridian Behavioral Healthcare, Inc.NAMI Central FloridaSeminole Community Mental Health Center
georgIaPastoral Institute
IdahoDHW/Children’s Mental HealthProject ACCESS
IllInoIsBen Gordon CenterCommunity Counseling Centers of ChicagoNorth Central Behavioral Health SystemsRush University
IndIanaBehavior Services & Therapy
IoWaBackbone Area Counseling/Community Circle of CareBlack Hawk Grundy RSNDecatur County Community ServicesDepartment of Human Services, Mental Health/
Disability ServicesDHS Case ManagementHumboldt County Mental Health CoalitionIowa Department of Public HealthIowa State Deptartment of HealthIowa State PatrolMagellan Health MECCA National GuardOrchard Place Child Guidance CenterPlains Area Community Mental Health CenterPolk County Health ServicesPottawattamie County Community ServicesSE Polk Community SchoolsSt. Luke’s HospitalUrbandale Community SchoolsVera French Community Mental Health CenterWinneshiek County CPC (Luther College)Youth and Shelter Services, Ames
KansasCOMCARE of Sedgwick CountyHigh Plains Mental Health CenterThe Bert Nash Center
KentucKYKentucky River Foothills Community Action Agency
MIchIgan
Behavioral Health Professionals, Inc./CareLink/ConsumerLink
Washtenaw Community Health Organization
MInnesotaAfrican American Adoption AgencyBelgrade Ave. United Methodist ChurchEast Metro Womens Council DBTFamily and Childrens ServiceFamily Life Mental Health CenterH.C. Child Crisis ServicesNAMI MinnesotaNormandale CollegeNorthern Pines Mental Health CenterNorthwestern Mental Health centerPeople Inc.Public Health SolutionsRangeMental Health CenterRSI is Residential Services, Inc.Snyder Health Care Upper Mississippi Mental Health CenterWoodland Centers
MIssIssIPPICommunity Counseling ServicesMHA of the Capital Area
MIssourIMental Health, IndependenceState of Missouri
neBrasKaBehavioral Health SpecialistsRegion 3 Behavioral Health
neW JerseYCare Plus NJGreater Trenton Behavioral Healthcare
north carolInaCenterpointCherokee County Safe Schools Healthy Students CrossroadsCumberland County Mental HealthEastpointeFive County Mental Health AssociationMental Health PartnersNAMI IredellNorth Carolina Council of Community ProgramsPiedmont Behavioral HealthSoutheastern Regional Mental Health CenterWake Center for Families and ChildrenWestern Highlands Network
north daKotaDepartment of Health and Human Services
ohIoOhio Association of Occupational Health Nurses
oKlahoMaLong Term Care Authority of TulsaOklahoma Community Mental Health Services
oregonWallowa Center for Wellness
PennsYlVanIaAdams Hanover Counseling Services, Inc. Community Services GroupMental Health Association of the Captial Region
rhode IslandGateway HealthcareKent Center
south daKotaSouth Dakota Division of Mental Health
tennesseeValueOptions
teXasAustin Travis County MHMREl Paso MHMRMHMRA of Harris County Sunwest Behavioral Health OrganizationThe Burke CenterTropical Texas Behavioral Health
VIrgInIaAMERIGROUP Community CareValueOptions
WashIngtonBehavioral Health ResourcesCascade Mental Health CareCatholic Family & Child ServiceCentral Washington Comprehensive Mental HealthCommunity Psychiatric ClinicCompass HealthKitsap Mental HealthLower Columbia Mental Health CenterNAVOSQuality Behavioral HealthSpokane Mental HealthValley Cities Counseling & ConsultationWashington Community Mental Health CouncilYouth & Family Link
WYoMIngCloud Peak Counseling ServicesFremont Counseling ServicesUPLIFT

Evidence-Based Early Interventions
22 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Meena dayak, Director of Marketing and Communications and chris loftis, Phd, Director of Practice ImprovementNational Council for Community Behavioral Healthcare
Geoffrey Canada on His Harlem Miracle
I n 2008, nearly all students in third and eighth grade in Harlem Children’s Zone charter schools outperformed the average New York student in math.
“The math thing is just so far above anything I’ve ever seen,” says Roland Fryer, a Harvard economist, in the Wall Street Journal. “The real hard work is to figure out why it’s working and whether that kind of thing can be exported so we can help more kids.”
What’s working is the “conveyor belt” con-cept of the Harlem Children’s Zone® (HCZ) project, started in 1997 to give children an intensive experience in a succession of programs until they graduate from college. Described as “One of the most ambitious social-service experiments of our time,” by the New York Times, HCZ is a unique, holis-tic approach to rebuilding a community so that its children can stay on track through college and go on to the job market.
HCZ creates a “tipping point” in the neigh-borhood so that children are surrounded by an enriching environment of college oriented peers and supportive adults, a counterweight to “the street” and a toxic popular culture that glorifies misogyny and antisocial behavior. The fundamental principles are simple: (1) Help kids as early in their lives as possible, and (2) create a critical mass of adults around them who understand what it takes to help children succeed.
The HCZ pipeline begins with The Baby College®, a series of workshops for par-ents of children ages 0-3. Meanwhile, their kids attend “Harlem Gems,” HCZ’s pre-kindergarten. After that, they move on to charter schools. A bevy of other programs psychological and financial counseling for parents, health clinics and after-school arts, computer, and karate classes supports their path. The pipeline goes on to include best practice programs for children of every age through college. The network includes in school, after school, social service, health, and community building programs. “The objective is to create a safety net woven so tightly that children in the neighborhood just can’t slip through,” says the New York Times Magazine.
The comprehensive system of programs extends to nearly 100 blocks of Central Harlem. HCZ also works to reweave the social fabric of Harlem, which has been torn apart by crime, drugs, and decades of poverty.
The founder of HCZ, Geoffrey Canada, settled on a career in social work when he was about nine, living in a rodent-infested apartment with his mother and three broth-ers in the South Bronx during the 1960s. His father left when he was four years old. He says he spent most of his childhood fighting in gangs. He also says he stared down guns. Despite brushes with violence, Mr. Canada was a bookworm who did well in school. He got a scholarship to Bowdoin College in Maine and then earned a master’s in educa-tion from Harvard.
In an interview with the Wall Street Journal, Canada shared that one of the saddest mo-ments in his life was when his mother told him Superman didn’t exist. “I really believed in Superman,” Canada said, recalling he thought it would take a superhero to clean up his neighborhood. “And then I suddenly
realized ... there’s no one coming to rescue us.” He says he vowed then to help poor children one day.
The National Council interviewed Geoffrey Canada about the highlights of HCZ and his advice for others wanting to travel down the road of early intervention through community building.
Is there some aspect of the Harlem children’s Zone model that is often missed or not fully appreciated?Yes, our work in rebuilding communities is often glossed over. We not only sup-port physical rebuilding of communities, but we also work with the adults in our program to help them reclaim their communities as their own, to drive change. We believe that for children to do well, their families have to do well. And for families, to do well, their community must do well.
Community Pride is the community organizing and housing stabilization arm of the Harlem Children’s Zone. In the 11 years since it was founded, HCZ’s
What has been your best moment with HCZ? When President Obama said he wants to replicate our model. His budget allocates $10 million to create ‘Promise Neighborhoods’ across the nation. And we are eager to be helpful. We don’t want to run a ‘Promise Neighborhood’ anywhere else but we can share what we’ve learned and what works.

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 23
Community Pride has made remarkable strides towards achieving its goal: revital-izing the structure and spirit of central Harlem. Community Pride has worked with thousands of community residents to help tenants purchase the homes they live in, establish low-income rental programs, plant community gardens, paint public hallways, and beautify neighborhood streets. Hand in hand with community resi-dents, Community Pride works to establish and accrue social capital in Harlem. The work is accomplished holistically, through HCZ programs linked to provide residents with comprehensive services, from prenatal care to family development, from employment counseling to assistance in receiving Social Security benefits.
What is HcZ’s approach to addressing mental health and addictions challenges?We believe in an approach where we help people heal themselves. And we have four outreach workers in our program who provide mental health and addictions services through individual counseling and motivation. We also have two of the largest Narcotics Anonymous meetings on site. We have a strong prevention focus — we work with high-risk families, say where a parent has an addiction disorder, and we educate youth on the consequences of alcohol, tobacco, and drug use. We hold health fairs where we encourage youth themselves to take a lead role. Our prevention efforts are supplemented by intensive support; we believe that support and care should be seamless, no matter how someone comes in the door.
What has been your best moment with HcZ?When President Obama said he wants to replicate our model. His budget allocates $10 million to create “Promise Neighborhoods” across the nation. And we are eager to be helpful. We don’t want to run a ‘Promise Neighborhood’ anywhere else, but we can share what we’ve learned and what works.
President Obama’s fiscal 2010 budget proposal calls for neighborhoods to im-prove the lives of children living in poverty through programs modeled after the Harlem Children’s Zone. As a presidential candidate, Obama said “If we know it works, there’s no reason this program should stop at the end of those blocks in Harlem. It’s time to change the odds for neighborhoods all across America. And that’s why when I’m president, the first part of my plan to combat urban poverty will be to replicate the Harlem Children’s Zone in 20 cities across the country.”
Has your model already been replicated elsewhere? If so, what are the lessons learned?Boston, Philadelphia, San Francisco, and most major cities have been replicating the Harlem Children’s Zone model, but not on the same scale. The biggest lesson learned is that you need massive infusion of financial resources to do something on an effective scale. Public dollars are best to support a venture of this magnitude.
We hear you lost millions in donor support with the Wall Street col-lapse. How are you surviving and how do you plan to make good?Yes, we have been hurt but our board has been wonderful and has really stepped up. We’ve had to cut back but we tried to cut back through layoffs rather than service cuts. We’ve tried to put together a 2-year survival plan if the economy worsens.
The Wall Street Journal reports that Wall Street’s meltdown and money manager Bernard Madoff’s alleged financial fraud threaten the donor base that bankrolls Geoffrey Canada’s work. His Wall Street support had reached upwards of $15 million annually. His budget has grown at least 15% annually in eight of the past nine years, to $68 million from just under $12 million. His charity’s endowment stands at around $94 million. Revenue in the last fiscal year ending June 2009, probably fell 7%, or $5 million. The board, with Mr. Canada’s support, unanimously approved cutting about 140 employees, or 10% of the staff. In addition, Canada had to shelve plans to add another 1,000 children to HCZ in the months ahead. All programs were protected, but many with reduced staff. The outlook for the current fiscal year is uncertain.
What is the secret of the massive donor support you’ve gotten?People give because they realize communities must be accountable.
President Clinton noted that “If you volunteer or give money to the Harlem Chil-dren’s Zone, you know you will get a high rate of return.” When Geoffrey Canada launched HCZ, he emphasized a long-term plan with measurable results to show potential donors. His central argument was “Spending $3,500 annually to keep a poor child out of jail trumps the $50,000 Americans would spend each year to keep the same kid behind bars. He says, “We need a movement in America... We’re saying let’s intervene early, pay the money upfront and not have to pay the money on the back end. We think there’s a positive net benefit for society.”
from your recent and past fundraising efforts, in good and bad times, what is your advice for other communities interested in replicating aspects of your work? Don’t go in for a project of this scale if you don’t have the infrastructure. You have to be able to count on support from foundations, corporations, wealthy individuals, and public sources.
If you do embark on a project like HCZ, start with your strength. Community build-ing requires managing and delivering multiple programs and relationships that address different developmental stages. But you can’t do everything at once. We started with education and kids, as that was our strength.
Most important, you must have a passion to help those you are helping to succeed. And the focus on integrity and ethics is key.
In the HcZ model, do you run all your programs or collaborate with others? What works better?We run 75% of our own programs and for the services where we do contract with others, we manage relationships. For instance, Children’s Health Fund runs our health clinics, and we have a terrific relationship with them. We’ve learned that you need partners who deliver quality and share your accountability and values. It must be a win-win to work well.
What are you reading? Outliers by Malcolm Gladwell. It’s an amazing book, emphasizing that there are really opportunities for ALL children.
Evidence-Based Early Interventions
24 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Nurse-Family Partnership: Effective and Affordable
B ehavioral health practitioners and managers will at some point find themselves contemplating a
life lived in what I call the “life preserver paradox.” You are intervening with an ever-growing number of children and families who are diagnostically com-plex, on what appears to be an ever-shrinking bud-get, and you wonder if you can ever stop saving the drowning long enough to figure out how to keep kids and families out of the whitewater rapids of evolving dysfunction to begin with.
That’s where Nurse-Family Partnership® can help the program puts young families on a physically, socially, psychologically, and economically healthy trajectory from the very beginning of their lives as a family. Nurse-Family Partnership engages first-time parents living in poverty in home visits by nurses beginning early in the mother’s pregnancy through their child’s second birthday. Home visits are structured to help parents focus on goals related to improved pregnancy health, infant and toddler social-emotional attachment and healthy develop-ment, and economic self-sufficiency. Nurse-Family Partnership nurses are trained to think ecologically about human development, looking at the individual and family as part of a larger social and economic system where stress and support comes from many points in that system, and individual and family cul-ture, values, and beliefs significantly impact devel-opmental pathways.
David Olds, PhD, a developmental psychologist cur-rently on faculty at the University of Colorado at Denver Health Sciences Center, designed and test-ed this preventive intervention in randomized, con-trolled research trials in Elmira, New York (1977); Memphis, Tennessee (1987); and Denver, Colorado (1993). Families in both control and experimental groups were followed longitudinally to determine whether or not effects were sustained beyond the two year nursing intervention. Findings from the three trials serving diverse populations living in ur-ban and rural settings over the past three decades demonstrate that the Nurse-Family Partnership reli-ably produces the following outcomes:
>> Reductions in child abuse and neglect, early childhood injuries, mental health problems, to-bacco use, and crime
>> Improvements in prenatal health; birth out-comes (including greater intervals between births); child development, school readiness, and academic achievement; and maternal em-ployment.
Three independent studies have found that invest-ments in Nurse-Family Partnership lead to signifi-cant returns to society and government; depending on which outcomes are monetized for the evalua-tion, estimates of economic return can easily reach $34,000 per family served in net benefit to public funding (over program cost) when the program is appropriately targeted to higher-risk families. Since the problems Nurse-Family Partnership successfully prevents touch so many domains of individual and family functioning, the sources of those savings ac-crue to many systems: health (including Medicaid), child welfare, education, employment, juvenile jus-tice and corrections.
Nurse-Family Partnership costs approximately $5,000/family/year. A minimum start-up program in a given community serves 100 families, with ap-proximately a $500,000 budget. Planning budgets are available from the NFP National Office. Nurses’ salaries are the primary factor affecting the total budget, and salaries vary by geographic region, with highest costs typically found in urban centers on ei-ther coast and in hospital-based programs. Due to variations in the type of staff employed, caseloads, training, supervision, and worker turnover costs, there may or may not be a cost differential between Nurse-Family Partnership and other home visitation programs.
A nursing team serves a minimum of 100–200 fami-lies and comprises four to eight nurses (each carrying a caseload of no greater than 25 families), one full-time nurse supervisor, and administrative support. Nurse-Family Partnership nurses visit families every one to two weeks from early in pregnancy through the child’s second year of life, making about 65
visits during the course of the program.
Nurse-Family Partnership is typically administered by state and local public health agencies, commu-nity-service oriented hospitals, or health-focused community-based organizations. Women may be re-ferred to Nurse-Family Partnership by a wide variety of people each agency’s referral system should be built to engage anyone and any agency that is likely to be a woman’s first contact when she learns she is pregnant for the first time. That usually includes pregnancy testing centers or family planning clinics, school nurses, counselors, WIC clinics, obstetrics practices, and informal support systems or leaders who are imbedded within many minority communi-ties.
Programs are supported by a range of public and private funding sources, including Medicaid, Mater-nal and Child Health Block Grant (Title V), tobacco settlement funds, Temporary Assistance for Needy Families, Child Care Development and Social Ser-vices Block Grants, child development and school readiness initiatives, mental health services and prevention funds, and state and local general funds.
If approved by Congress, a newly-proposed federal initiative sponsored by President Obama will make $8.6 billion available over the next 10 years in matching grants to states to implement evidence-based home visitation programs with a goal of pro-viding service to all eligible families: Nurse-Family Partnership is one of the programs that will read-ily qualify if Congress approves this new initiative. President Obama cited Nurse-Family Partnership in several of his campaign speeches and in his White
Peggy hill, Director of Program Development, Nurse-Family Partnership National Service Office
Investments in nurse-Family Partnership lead to significant returns to society and government; estimates of economic return can easily reach $34,000 per family served in net benefit to public funding when the program is appropriately targeted to higher-risk families.

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 25
House governing platform as an example of a “pro-gram that works” and warrants federal investment.
Nurse-Family Partnership currently is serving approxi-mately 18,000 families a day in 28 states across the nation. Demand for Nurse-Family Partnership services is growing, and the program is being widely and suc-cessfully replicated in urban, rural, and suburban com-munities across nearly all racial/ethnic populations.
It typically takes 12–18 months to develop a solid plan for program implementation and fiscal sustain-ability within a community. Statewide or large urban, multi-site implementations may take longer, depend-ing on the number of nursing teams and families served, what the administrative sponsor envisions, and the sponsors’ usual processes for developing and managing request for proposal processes. Expe-rienced Nurse-Family Partnership program develop-ment staff work closely with state and local leaders to engineer these initiatives, including development of local agency implementation plans. We urge those who are building implementation plans to include their local mental health centers and providers many
of the women in the program need mental or behav-ioral healthcare and/or substance abuse treatment, and it is recommended that an experienced mental health provider be part of each nursing team’s in-terdisciplinary counsel for continuing education and case conferencing.
Implementation plans must be approved by the Nurse-Family Partnership National Service Office (headquarters) prior to each local agency hiring their nursing staffs who subsequently receive required training from Nurse-Family Partnership expert nurse consultants. Learning to conduct this unique prac-tice with diverse families takes time and coaching. Experienced nursing teams say it takes at least 12–18 months before practitioners feel confident utilizing all of the program’s resources flexibly and competently and can manage a full caseload efficiently.
Data about family characteristics, program imple-mentation, and outcomes are entered locally into Nurse-Family Partnership’s Web-based national data collection and reporting system. Reports enable local program managers to monitor and enhance program
quality over time and ensure that early indicators of desired outcomes are strong. When program size is adequate, reports may be used to describe the im-pact the program is making among participating families. These data prove extremely useful in con-tinuously monitoring and improving program quality and performance; and in documenting the impact the program is having locally.
The Nurse-Family Partnership National Office wel-comes contacts from state and local officials and oth-ers interested in establishing and expanding Nurse-Family Partnership where local needs exist. For more information, visit www.nursefamilypartnership.org.
Peggy Hill is director of program development for the Nurse-Family Partnership National Service Office. She has 20 years of experience establishing and replicating community-based programs to improve family and child health and prevent child abuse. She was instrumental in laying the groundwork for early community implementation of the Nurse-Family Partnership, assuring that new program sites had the resources and support needed to achieve outcomes comparable to those achieved in the randomized trials. She earned a masters degree in counseling and community organization from Purdue University with a focus on social change and community systems of care.
www.TheNationalCouncil.org(Click on Resources and Services, then on SPQM Dashboards)
NOT JUST
ANOTHER
SOFTWARE
PROGRAM
...AN ESSENTIALMANAGEMENTCONSULTATION
TOOL!
Take the SPQM test drive andunleash your company’s potential
Executive Dashboard ProvidingKey Indicator Measurement
Today’s environment demands accountability: from clinicaloutcomes to demonstrated, proven cost-effectiveness.
David Lloyd and the SPQM Consultantswill work closely with your management teamto help identify strategic quality service processoutcomes/variances, compliance levels andperformance measurement.
Take a free SPQM test drive: Schedule a complimentaryInternet-based consultation and SPQM report set today.919-387-9892 or [email protected]

Evidence-Based Early Interventions
26 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
R ecognizing the tremendous anguish that severe mental illness inflicts on young people, their
families, and entire communities, the Robert Wood Johnson Foundation launched a national effort, the Early Detection and Intervention for the Prevention of Psychosis Program, that builds on the pioneering work of the Portland Identification and Early Refer-ral (PIER, see sidebar) Program in Portland, Maine. This work holds the promise of redefining mental health services and redirecting the course of treat-ment to stop the progression of severe mental ill-ness in adolescents and young adults. With $16.9 million in funding from RWJF and with six participat-ing sites across the nation, EDIPPP is the founda-tion’s largest investment in mental health to date. The program is focused on gathering the evidence practitioners need to better meet the mental health needs of adolescents and young adults at risk for severe mental illness before the illness develops.The six sites that are part of this national endeavor use a combination of evidence-based practices to treat the early warning signs of serious mental ill-ness (schizophrenia, bipolar disorder with psycho-sis, and major depression with psychosis):
>> PIER Program at the Maine Medical Center in
Portland, Maine (this site also serves as the na-tional program office for EDIPPP)
>> Early Diagnosis and Preventative Treatment of Psychosis Illness Program at the University of California, Davis, Medical Center in Sacramento, California
>> Early Assessment and Support Team Program at Mid-Valley Behavioral Care Network in Salem, Oregon
>> Michigan Prevents Prodromal Progression Pro-gram at Washtenaw Community Health Organi-zation in Ypsilanti, Michigan
>> Recognition and Prevention Program at Zucker Hillside Hospital in Glen Oaks, New York
>> Early Assessment and Resource Linkage for Youth Program at the University of New Mexico and Mind Research Network in Albuquerque, New Mexico
Psychotic illnesses, such as schizophrenia, are known to be disabling and expensive in multiple ways. There is a tremendous cost to individuals with these illnesses, as well as to their families and com-munities, e.g., lost productivity, increased family stress, increased physical illnesses, diminished self-
esteem, increased dependency, repeated need for hospitalizations, inability to maintain friendships, and difficulty attaining life goals, such as complet-ing school and working. It has been estimated that the cost to society can be higher than $10 million over the course of an individual’s lifetime, espe-cially if they have schizophrenia. When we con-sider that psychosis can derail a young person’s life permanently, it is hopeful to think that offsetting an illness process early in its development is possible.
EDIPPP works with young people ages 12 to 25 and their families in a defined geographic area. The program uses evidence-based interventions that can help youths achieve their full potential, without stigma, before they exhibit the negative effects of a fully developed mental illness.
The evidence-based treatment tools used in EDIP-PP are as follows:
>> Family psychoeducation, which helps families understand the illness process and how to help their loved one.
>> Education and employment support to ensure success in life skill areas.
>> Family-aided assertive community treatment, which provides rapid access to a multidisci-plinary team to assess and treat young people.
>> Medication, as needed, to minimize the most extreme symptoms.
Community outreach and education are a major component of EDIPPP; they serve as a mechanism for referrals and allow program professionals to convey specific information about early signs of psychosis, to connect with community members outside the mental health system, and to demystify and destigmatize mental illness. EDIPPP’s leaders hope that if specific community stakeholders are offered information and support, they will develop collaborative relationships with EDIPPP staff, which will lead to early referrals of at-risk youths. Stake-
It Takes a Community: Stopping Progression of Severe Mental Illness in Youth
William r. McFarlane, Md, Director; donna downing, Ms, otr/l, Director of Training; and anita ruff, MPh, ches, Director of Administration—Early Detection and Intervention for the Prevention of Psychosis Program
EDIPPP Community Outreach and Education Activities by Site April 2007–April 2009
EDIPPP site# of community outreach and
education events# of participants
Early Assessment and Resource Linkage for Youth Program 64 1,442
Early Assessment and Support Team Program 91 1,276
Early Diagnosis and Preventative Treatment of Psychosis Illness Program 123 2,513
Michigan Prevents Prodromal Progression Program 149 3,552
Portland Identification and Early Referral Program 98 3,315
Recognition and Prevention Program 40 916

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 27
holders are defined as people in a unique position to identify young people who demonstrate the early mental changes predictive of a developing psy-chosis, and they include staff at medical practices, educational institutions, and community organizations.
Because community outreach and education are critical to the successful identification of young people experiencing early warning signs of mental ill-ness, all EDIPPP sites have devoted a significant amount of time and energy to community outreach and education. Between April 2007 and April 2009, 565 community outreach and education events took place and reached 13,014 people in the EDIPPP communities.
As a result of the community outreach and education efforts, more than 725 people have been referred to the respective EDIPPP programs across the country. As EDIPPP continues, the program’s professionals are trying to evaluate the effectiveness of the community outreach and education activi-ties, examining whether outreach and education participants have increased knowledge, intend to refer youths to the program, understand the referral process, and, eventually, make a referral. Led by staff of the University of Southern Maine’s Muskie School of Public Service, this evaluation will pro-vide important information on the role of community outreach and education in increasing the public’s awareness of EDIPPP, understanding and use of its referral process, and identification of young people at risk.
William R. McFarlane, MD, is the director of the Early Detection and Intervention for the Prevention of Psychosis Program and the director of the Center for Psychiatric Research at Maine Medical Center. He has received numerous awards and honors for his work in the field of psychiatry.
Donna Downing, MS, OTR/L, is the director of training for the Early Detection and Intervention for the Prevention of Psychosis Program and oversees the clinical functions of each replication site. She served as the first team leader of the Portland Identification and Early Referral Program, from 2000 to 2006. She has worked in various psychiatric inpatient and community settings throughout her career and has taught at the university level. Her area of expertise is family psychoeducation.
Anita Ruff, MPH, CHES, is director of administration for the Early Detection and Intervention for the Prevention of Psychosis Program. She has worked in federal, state, and local public health organizations throughout her career and has expertise in community health education, social marketing, and program evaluation.
Excerpts from an article on the PIER program from National Council Magazine, 2007, Volume 3
T he mission of the Portland Identification and Early Referral Program is to identify young people between the ages of 12 and 25 who might be at risk
for psychosis in the Greater Portland area, and then offer appropriate treatment.
Starting in December of 2000, the multidisciplinary PIER team began educating community stakeholders about the early signs of psychosis.
PIER’s outreach effort to educate community members was based on initiatives developed in Australia, Norway, and Denmark, where the focus was to interrupt the progression of schizophrenia and other severe psychotic disorders. PIER’s goal was to improve outcomes and prevent the onset of the psychotic phase of those illnesses. The Australian and Norwegian initiatives identified stakeholders outside of the mental health system who could participate in early detection and show commitment to the effort.
It was reasoned that if specific community professionals were offered information and support, collaborative relationships between them and the PIER staff would develop and lead to early referrals of “at risk” youth. The community education presentations and outreach activities were designed to give specific information about early signs of psychosis, to network with community members outside the mental health system, and to demystify and destigmatize mental illness. These trainings offered important information about the biology of the brain, which raised awareness about brain disorders versus personality disorders. They also offered resource and referral suggestions for stakeholders.
The result of PIER’s outreach was that school professionals, teachers, health pro-fessionals, parents, and mental health practitioners became familiar with PIER’s message, knowledgeable about the importance of making early referrals as a deterrent to disability, and learned how to make referrals. PIER has been de-signed to respond quickly to referrals and to partner with young persons and their families from the start through the intake assessment process and then through various client-centered psychosocial interventions, such as family psy-choeducation, counseling, supported education, and supported employment. When appropriate, clients have also had occupational therapy assessments to better understand cognitive and functional difficulties results and recommenda-tions are then shared with the family and treatment team.
Most participants have been on low-dose medications, but overall, their symp-toms have subsided as they and their families have learned to keep stress low and identify early signals of symptom recurrence. Research has been an impor-tant component of the program because much still needs to be learned about the early phases of illness, what works in terms of interventions, and what indi-viduals and their families need. The result is that the majority of young people who have participated in the program have stayed in school, graduated, held jobs, maintained relationships, participated in extra-curricular activities, and set goals for the future.
More About PIER
EARLY SIGNS OF PSYCHOSIS
A combination of at least two of the following:
> Being fearful for no good reason
> Jumbled thoughts and confusion
> Feeling “something’s not quite right”
> Declining interest in people, activities, and self-care
> Hearing sounds or voices that are not there
> Trouble speaking clearly, not understanding others
> Declining mental acuity, memory, or attention
Don’t ignore the early symptoms!
www.preventmentalillness.org

Evidence-Based Early Interventions
28 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
I n 2001, the Mid-Valley Behavioral Care Network, based in Salem, Oregon, launched the first sys-
tematic effort to implement early intervention for schizophreniform and bipolar spectrum psychosis in a U.S. public managed care system through a program called the Early Assessment and Support Team. In 2007, the Oregon legislature funded dis-semination of the EAST approach through the Early Assessment and Support Alliance. The goal was to make the services available across Oregon. These efforts are part of a statewide effort to maximize recovery through services that are based on current research.
MVBCN is an intergovernmental managed mental healthcare organization that has succeeded in bring-ing evidence-based and preventive approaches to its local communities. In 1999, MVBCN hired Patri-cia Mrazek, a mental health prevention researcher, to identify and recommend evidence-based preven-tion programs that could be implemented across its network. MVBCN specifically requested models associated with early intervention or prevention of
schizophrenia, given that the observed outcomes of people dealing with this illness were particularly poor. Mrazek introduced MVBCN to the work of the Early Psychosis Prevention and Intervention Center (now called Orygen) in Melbourne, Australia.
After a yearlong review and planning process, MVBCN launched EAST in January 2001. EAST based its ser-vices on Australian guidelines and consultation. As EAST evolved, it incorporated the multifamily group process and integrated practice elements from best practice methods developed in the United States, such as the family-aided assertive community treat-ment model developed by the Portland Identifica-tion and Early Referral program (see page 24-25).
Initially, seven of MVBCN’s 16 provider agencies and several separate subprograms were included in the clinical implementation team. Each agency con-tributed clinical staff, and MVBCN provided direct funding for the clinical services in addition to a full-time coordinator and training expenses. EAST also brought in partners from allied systems, including
public health, secondary and postsecondary educa-tion, the medical community, vocational rehabilita-tion, and business. Local and national foundations contributed significant funding to allow EAST to serve all clients regardless of insurance coverage and to document its results to create the needed momentum. From EAST’s inception, the MVBCN partners viewed the program as a community-based public health strategy and system reform effort.
As a result of the Oregon legislature’s investment in 2007, more than 60 percent of Oregon’s population has access to early psychosis (first-episode) inter-vention based on EAST’s approach. Core elements of the program model are as follows:
>> Ongoing community education focused on schools, doctors, parents, and other potential re-ferral sources to increase identification of early symptoms.
>> Attempts to eliminate financial, regulatory, cul-tural, and logistical barriers to care.
>> Emphasis on voluntary, empowering approaches
tamara sale, Ma, EAST Program Coordinator and Ryan Melton, LPC NCC, Clinical Coordinator—Mid-Valley Behavioral Care Network
A Long-term Approach to Early Psychosis Intervention

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 29
that assume a hopeful long-term prognosis.
>> Active efforts to reach out to, welcome, and be-friend each client, use his or her explanatory lan-guage, and emphasize his or her strengths and goals.
>> The perspective that clients and families are full partners and, accordingly, a transparent decision-making process; the ultimate goal is to prepare clients and their families for their role as “owners” of the treatment and support process.
>> Provision of service to clients within the same team regardless of their youth or adult status.
>> Encouragement of multifamily group psychoeduca-tion as a core service.
>> Support of vocational, educational, and other de-velopmental goals.
>> Careful use of medications at low doses as appro-priate, with an emphasis on patient education and side-effect monitoring.
>> Inclusion of occupational therapy, with an empha-sis on identifying and addressing the sensory and cognitive issues that often underlie functional dif-ficulties.
Oregon’s experience offers important insights.
The benefits of early intervention for psychosis are easily established compared with the tremendous costs of acute and extended illness. EAST and, now, the EASA programs have followed the pattern of other international programs in showing an immediate and dramatic decrease in hospitalizations among the cli-ents served. Approximately 50 percent of the people who entered EAST and EASA programs were hospital-ized in the 3 months before intake. After intake, the hospitalization rate dropped to 10 percent or less per quarter, with a further decline over time. A similar de-cline was seen in the number of arrests.
Where early psychosis services are not easily avail-able, people often experience repeated acute invol-untary hospitalizations and legal involvement rather than a more positive and effective entry into servic-es. This approach not only is far more expensive but also can result in a host of negative consequences, such as trauma, future treatment resistance, fam-
ily burden, job loss, homelessness, accidental death, suicide, or entry into lifelong dependency on the dis-ability system.
The lifetime course of one person’s illness can easily cost in the millions of dollars, including acute care, legal expenses, disability and medical costs, housing, food stamps, and both the client’s and the family’s lost wages and increased illness. Research compiled by Orygen has documented that the cost of the first 5 to 7 years of treatment alone for people who receive early intervention is one-third the cost of treatment for people who do not receive such intervention.
Evidence-based care at the early stages of illness requires leadership and system redesign. For ex-ample, systems must be able to accept diverse fund-ing sources and to serve clients during both teen and adult years. If efforts are to be successfully sustained in spite of funding and political changes, consistent commitment and prioritization of efforts are critical. During the EASA dissemination process, multiple ses-sions for senior administrators included in-depth dis-cussions of the unique and challenging requirements of supporting this program development. Communi-cation and strategizing with senior staff are ongoing. The support of senior management champions is necessary to sustain the effort required. In addition, leadership at the state level has been critical.
To support long-term recovery, the larger system of ongoing care must have adequate resources, an ori-entation toward recovery, evidence-based care, and easy access for clients who experience psychotic illness. International data are clear that without con-tinued support, the benefits of short-term intervention can be lost within the first 5 years. The ability to tran-sition clients into long-term supports that are based on a philosophy consistent with the early intervention program is important to sustain the benefits. Thus, programs that applied to be part of EASA’s dissemina-tion process were required to demonstrate how EASA would fit into the mission and direction of their orga-nization. Likewise, at the state level, the features of early psychosis intervention parallel other efforts to move the system toward recovery-oriented, evidence-based care.
EAST, EASA, and other national efforts are only begin-
ning to lay the groundwork for the system that is ulti-mately needed. Much remains to be done:
>> Expanding early psychosis intervention alternatives to the rest of Oregon.
>> Ensuring continuity of quality care beyond the ini-tial couple of years of early intervention.
>> Restructuring disability support and insurance alternatives to encourage clients’ maximal partici-pation in the workforce without endangering their access to healthcare.
>> Participating in research and dissemination that will create a system of early psychosis services na-tionwide.
>> Systematically incorporating emerging research into practice, including developing program mod-els that provide support for early symptoms with-out making inappropriate assumptions about the ultimate diagnosis or prognosis.
Without continued support, the benefits of short-term intervention can be lost within the first 5 years. To support long-term recovery, the larger system of ongoing care must have adequate resources, an orientation toward recovery, evidence-based care, and easy access for clients who experience psychotic illness.

Evidence-Based Early Interventions
30 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
EAST is currently one of six sites across the nation participating in a study funded by the Robert Wood Johnson Foundation Early Detection and Intervention for the Prevention of Psychosis Program, which replicates PIER’s FACT model for people who have less severe psy-chotic symptoms or who have had acute symptoms for less than 1 month. Because extensive evidence shows that the disability associated with schizophrenia often begins during the prodrome, or preacute, stage of illness and because acute psychosis is highly disruptive and potentially life threatening, earlier identification holds the potential to significantly improve outcomes (more about EDIPPP and PIER on page 24).
In a community behavioral health system driven all too often by crisis and rigid funding requirements, EAST and EASA are helping to demonstrate that it is possible to move out of a reactive mode and reorient services in a way that is most beneficial for the people who use them. The clients served by EAST and EASA will help shape and direct the next generation of mental health system development.
Given Oregon’s early experiences and the work of mental health advocates across the United States, we anticipate that recovery from psychosis will begin to be viewed as commonplace, in the same fashion as other chronic illnesses.
Tamara Sale has been program coordinator for EAST since its inception in 2001. Tamara has 20 years of experi-ence focused on mental health service system development. Tamara has a masters degree in management of public and nonprofit organizations with a concentration in fiscal policy. Her experience includes eight years as a state leader in the National Alliance on Mental Illness in Oregon.
Ryan Melton is the EAST clinical coordinator. Ryan has been a clinician with EAST since 2001. He has a masters degree in counseling psychology from Pacific University, and is currently a PhD candidate in counselor education at Oregon State University and a psychology instructor at Chemeketa Community College.
REfEREncESAmerican Psychiatric Association. (2007). Silver and bronze achievement awards. Psychiatric Services, 58, 1372−1373.
Bertolote, J., & McGorry, P. (2005). Early intervention and recovery for young people with early psychosis: Consensus statement. British Journal of Psychiatry, 187(Suppl. 48), S116−S119.
Birchwood, M., & Macmillan, F. (1993). Early intervention in schizophrenia. Australian and New Zealand Journal of Psychiatry, 27, 374−378.
Edwards, J., & McGorry, P. (2002). Implementing early intervention in psychosis. London: Martin Dunitz.
Egnew, R. C. (1993). Supported education and employment: An integrated ap-proach. Psychosocial Rehabilitation Journal, 17(1).
Ehman, T., & Hanson, L. (2002). Early psychosis: A care guide. Vancouver: Department of Psychiatry, University of British Columbia.
Ehman, T., Yager, J., & Hanson, L. (2004). Early psychosis: A review of the treat-ment literature. Vancouver: University of British Columbia.
International Early Psychosis Association Writing Group. (2005). International clinical practice guidelines for early psychosis. British Journal of Psychiatry, 187(Suppl. 48), s120−s124.
Johannesen, J. O. (2001). Early recognition and intervention: The key to success in the treatment of schizophrenia? Disease Management & Health Outcomes, 9(6).
Killackey, E., & Yung, A. (2007). Effectiveness of early intervention in psychosis. Current Opinion in Psychiatry, 20, 121−125.
McFarlane, W. (2002). Multifamily groups in the treatment of severe psychiatric disorders. New York: Guilford Press.
McFarlane, W. R., Dushay, R. A., Stastny, P., Deakins, S. M., & Link, B. (1996). A comparison of two levels of family-aided assertive community treatment. Psychiatric Services, 47, 744−750. McGorry, P. D., Edwards, J., Mihalopoulos, C., & Harrigan, S. M. (1996). EPPIC: An evolving system of early detection and optimal management. Schizophrenia Bulletin, 22, 305−326.
McGorry, P., & Jackson, H. (Eds.). (1999). The recognition and management of early psychosis: A preventative approach. Cambridge, England: Cambridge University Press.
McGorry, P., Killackey, E., Elkins, K., Lambert, M., & Lambert, T. (2003). Summary Australian and New Zealand clinical practice guideline for the treatment of schizophrenia. Australasian Psychiatry, 11(2), 136−147.
Mikalopoulos, C., McGorry, P. D., & Carter, R. (1999). Is phase-specific, communi-ty-oriented treatment of early psychosis an economically viable alternative? Acta Psychiatrica Scandinavica, 100, 47−55.
Mrazek, P. J., & Haggerty, R. J. (Eds.). (1994). Reducing risks for mental disor-ders: Frontiers for preventive intervention research. Washington DC: National Academies Press.
National Early Psychosis Project Working Party. (1998). The Australian clinical guidelines for early psychosis. Melbourne, Australia: University of Melbourne.
National Institute for Mental Health in England, Department of Health Policy Research Program. (2003). Early intervention for people with psychosis. Leeds, England: Author.
Power, P., Elkins, K., Adlard, S., Curry, C., McGorry, P., & Harrigan, S. (1998). Analysis of the initial treatment phase of first-episode psychosis. British Journal of Psychiatry, 172(Suppl. 33), 71−76.
Rupp, A., & Keith, S. J. (1993). The costs of schizophrenia: Assessing the burden. Psychiatric Clinics of North America, 16, 413−423.

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 31
“We’re seeing that simple screening can reduce healthcare costs and build hap-pier families and healthier communities,” says Rich Brown, who directs the Wisconsin Initiative to Promote Healthy Lifestyles, a screening and assistance program for alcohol and drug abuse coordinated by the Department of Family Medicine at the University of Wisconsin–Madison. The 5-year project is funded by a $12.6 million grant from the federal Substance Abuse and Mental Health Services Administration and administered by the Wisconsin Department of Health Services.
This innovative program aims to address problem drinking, which the state has identified as a major public health issue. Between 2002 and 2006, alcohol abuse rates among Wisconsin residents ages 12 and older ranged from 9% to 11%, compared with the na-tional rate of 8%. In addition, Wisconsin’s per capita driving-under-the-influence arrests are 1.5 times those of the United States as a whole, and the state’s rate of drinking and driving is the highest in the nation. Accord-ing to a 2008 needs assessment project report by the Wisconsin Department of Health and Family Services (now the Wisconsin Department of Health Services), the state’s healthcare, social services, and criminal jus-tice systems incur more than $2.6 billion in costs each year from alcohol-related injuries, hospitalizations, ar-rests, treatments, and deaths.
Since March 2007, WIPHL has administered screening, brief intervention, and referral to treatment (SBIRT) through 21 participating primary care settings across the state. The brief screening consists of four questions asked of each patient once a year during a routine healthcare visit. People who score positive and are at risk for alcohol abuse see an on-site health educator who has received WIPHL training. Patients’ responses to a lengthier set of questions the Alcohol, Smoking and Substance Involvement Screening Test indicate
their levels of risk or problems. Most patients receive an intervention of about 20 minutes and, perhaps, a follow-up visit or phone contact. Interventions are based on motivational interviewing techniques and are conducted on site by trained WIPHL health educators.
Studies have shown SBIRT to be one of the most effec-tive interventions for alcohol-related health problems. According to the National Commission on Prevention Priorities, alcohol SBIRT services are ranked fourth among clinical preventive services for cost-effective-ness and clinically preventable burden, which is de-fined as “the disease, injury and premature death that would be prevented if the service were delivered to all people in the target population”.
“Evaluations are showing that SBIRT is making an impact on patient drinking,” says Brown. For many pa-tients, this early and brief intervention, which includes one to three follow-up consultations, is enough to help them significantly decrease or stop their alcohol and drug use.
Primary care providers at the Wisconsin SBIRT sites are also pleased with the project. Adds Brown, “They’re already challenged to address three clinical problems in the 15 minutes they spend with a patient, and the response to having a trained health educator on site to conduct the screening has been very positive.”
To date, WIPHL clinics have screened 60,000 patients and conducted 10,000 brief interventions. More clinics will be added in coming years, and the effort includes a focus on changing public policy and standards of care so that services continue to be delivered on a perma-nent basis.
SBIRT both improves people’s lives and helps lower so-cietal costs. A 2002 Wisconsin study showed that the state saves nearly $1,000 in healthcare and criminal justice costs for every patient who receives screen-ing and brief intervention services. This study counted reductions in motor vehicle accident and injury, and medical, and legal event costs as benefits of the pro-gram.
Less widely recognized but just as significant is the toll that substance abuse problems take in the workplace. Absenteeism and “presenteeism”coming to work hung
over or under the influence pose substantial costs to an employer, given that such workers are at high risk for low productivity, workplace injuries, worker’s compen-sation claims, and potentially lifelong payouts.
A recent study by researchers Andrew Quanbeck, Katha-rine Lang, and Kohei Enami at the University of Wiscon-sin–Madison showed that employers have a lot to gain by making sure that their insurance companies and healthcare providers offer SBIRT. The analysis quanti-fied how employers benefit by requiring insurers to adopt the SBIRT program. The researchers calculated the likely costs of problem drinking for a representative Wisconsin firm that does not currently provide SBIRT services. They then constructed a cost−benefit model in which the firm would fund SBIRT for its employees through a group health insurance plan. The authors estimated the net present value of SBIRT adoption by comparing costs due to problem drinking both with and without SBIRT.
When absenteeism, presenteeism, and healthcare costs were explicitly considered from the employer’s perspective, the net present value for the representa-tive firm was $1,464 per employee. Benefits of the re-duction in motor vehicle accidents are shared between society and employers. Societal net present value, with the exclusion of quality of life values, was estimated to be $3,405 per employee. “While absenteeism and pre-senteeism costs are difficult to estimate empirically, we used the best estimates available from the literature,” noted Quanbeck et al. “Notably, SBIRT is cost-benefi-cial from the employer’s perspective if healthcare costs alone are considered. There appears to be a business case for employers to fund SBIRT services, since the costs are minimal and many of the benefits accrue di-rectly to the employer,” the researchers said.
“This study helps show that SBIRT is cost-beneficial from both societal and employer perspectives,” says Brown. “It makes economic sense for employers to make sure that SBIRT is a benefit covered in the group health insurance plans they offer,” he concludes.
Maureen Fitzgerald is an editor for NIATx, based at the national program office on the University of Wisconsin-Madison campus. She writes frequently on the NIATx model of process improvement and its successful application in behavioral health settings.
Maureen Fitzgerald, Editor, NIATx National Program Office
SBIRT: Effective Interventions for Alcohol-Related Health Problems

From The Field
32 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
I n June 2008, we interviewed 254 clients at seven BHS outpatient and residential treatment sites
about their access to general medical services and medical need. 66% of clients interviewed were in res-idential treatment, 33% were women, and 37% were Latino; 44% had less than a high school education, and half had been released from jail or prison within 6 months of starting treatment.
The Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Child-hood (Zero to Three, 2005) was introduced in 1994 and revised in 2005 as a way to evaluate and under-stand how very young children display developmental differences and emotional difficulties.
75 percent of brain growth and development occurs during the first three years of life. Early social and
emotional development provides the foundation for all later experiences in life, including the ability to self-regulate, the capacity to relate to others, flex-ibility in adaptive problem solving, and all academic achievements (Committee on Integrating the Science of Early Childhood Development, Youth and Families Board on Children, 2000). All of these aspects of early life growth and development occur in the context of the infant’s relationships with significant caregivers during the first 3 years of life.
Much research shows that young children who have difficulty regulating their emotions and relating to others are more likely to have persistent and serious mental disorders later in life (Keenan, Shaw, & Del-liquadri, 1998). Poor outcomes in social and emo-tional development and academic achievement are
associated with insecure attachment relationships (Ainsworth & Marvin, 1995). In the juvenile justice system, a large percentage of juveniles with violent offenses have a history of conduct disorders and disrupted social and emotional development in early childhood (Evans, Gonnella, Marcynyszyn, Gentile, & Salpekar, 2004).
Many cost–benefit studies support investing in high-quality early intervention. Relationship-based dyadic therapy with a primary caregiver and an infant or young child can be seen as promoting healthy de-velopment in young children and preventing later disorders. In a perfect world, every family would have this kind of comprehensive support during the first year of a child’s life to promote an enduring, strong foundation.
christy Kimpo, Phd, MHP, Infant Mental Health Specialist and Victor Place, LMFT, Program Director, Child & Family—Navos, Seattle, [email protected]
Prevention and Early Intervention Programs for Children
Focus on Relationships: Parent-Infant Psychotherapy at Navos
Community mental health organizations across the country share examples of
infant and child mental health promotion through successful prevention programs.
GettinG a Head Start on Mental HealtH

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 33
Parent−infant psychotherapy a relationship-based, dy-adic form of intervention that focuses on the interac-tions between caregivers and their children is currently viewed as a promising practice (Zero to Three, 2007) for promoting early social and emotional development and preventing later mental illness. Early evaluation studies analyzing the efficacy of dyadic relationship–based therapy suggest that parent−infant psychothera-py may be quite effective in helping families cope with traumatic events (Lieberman, Weston, & Pawl, 1991). In addition, dyadic therapy is highly effective in reducing relationship problems between caregivers and young children (Sameroff, McDonough, & Rosenthal, 2004).
Navos is a comprehensive mental health center whose Mindful Beginnings program, run by five full-time staff, serves Medicaid-eligible, low-income, high-risk in-fants, toddlers, and preschoolers and their caregivers together through weekly visits in the home, office, or community. Parent−infant psychotherapy is a key com-ponent of this work. Sessions focus on a variety of ar-eas, including meeting the concrete needs of families, providing information on typical development in early childhood, offering emotional support, and promoting healthy social and emotional development by working to create strong attachment relationships. Families are referred for services by primary care physicians, public health nursing staff, child protective and child welfare services, the dependency court system, child care cen-ters, early childhood educational settings, substance abuse treatment centers, detention centers and jails, and other clients. In addition to therapy, infant mental health work involves rigorous case management and
collaboration with other systems throughout the course of treatment to ensure comprehensive care for the family.
Home visits, a key part of this type of work, often cen-ter on developmentally appropriate play between the caregiver and the child. Caregivers and infants play together while the therapist observes and “notices” each dyad member’s emotional responses. The goals of these play sessions include identifying capacities of the dyad, helping the caregiver read and understand the nonverbal cues of his or her child, interpreting the child’s response to the caregiver’s efforts, and helping both partners be attuned (emotionally “in synch” with each other) in the context of a nonthreatening activity — play. The therapist may also focus on helping caregiv-ers match their play’s content, intensity, and pacing to that of the child. This, in turn, allows the young child to begin to regulate his or her emotions and arousal and gives the child a beginning sense that he or she has some control over the environment.
Caregiver−child interactions are imbued with a set of meanings, including the caregiver’s own experience as a very young child. Many families in our program have an intergenerational history of trauma, abuse, and neglect. Fraiberg, Adelson, and Shapiro (1975) called these intrusions from the past “ghosts” and introduced the model of parent−infant psychotherapy as a means of helping families exorcise the “ghosts in the nursery.” Dyadic therapy helps troubled caregivers deal with emotional issues from their past by exploring how those experiences may interfere with the caregivers’ ability to be present in the moment with their own infants or tod-
dlers. By working with the dyad together, therapists can help very young children and their primary caregivers form close attachment relationships.
REfEREncESAinsworth, M., & Marvin, R (1995). On the shaping of attach-ment theory and research: An interview with Mary Ainsworth. Monographs of the Society for Research in Child Development, 60(2−3), 3–21.
Committee on Integrating the Science of Early Childhood Develop-ment, Youth and Families Board on Children. (2000). In J. P. Shonkoff & D. A. Phillips (Eds.), From neurons to neighborhoods: The science of early childhood development. Washington, DC: National Academy Press.
Evans, G., Gonnella, C., Marcynyszyn, L., Gentile, L., & Salpekar, N. (2004). The role of chaos in poverty and children’s socioemo-tional adjustment. Psychological Science, 16, 560−565.
Fraiberg, S., Adelson, E., & Shapiro, V. (1975). Ghosts in the nursery: A psychoanalytical approach to the problems of impaired mother-infant relationships. Journal of the American Academy of Child Psychiatry, 14, 387−421.
Keenan, K., Shaw, D., & Delliquadri, E. (1998). Evidence for the continuity of early problem behaviors: Application of a developmental model. Journal of Abnormal Child Psychology, 26, 441−452.
Lieberman, A., Weston, D., & Pawl, J. (1991). Preventive interven-tion and outcome with anxiously attached dyads. Child Develop-ment, 62, 199–209.
Sameroff, A., McDonough, S., & Rosenthal, K. (2004). Treating parent-infant relationship problems: Strategies for intervention. New York: Guilford Press.
Siegel, D. J., & Hartzell, M. (2003). Parenting from the inside out. New York: Tarcher/Putnam.
Zero to Three. (2005). DC0−3 R: Diagnostic classification of mental health and developmental disorders of infancy and early childhood, revised. Washington, DC: Zero to Three Press.
Zero to Three. (2007, November). Keynote address, National Training Institute, Orlando, Florida.
R ecognizing that there are cost-effective ways to sup-port youths and families for better outcomes and
to reduce the negative effects of violence, crime, sub-stance abuse, and mental illness, Eastern Shore Psy-chological Services in Maryland operates three preven-tion programs — Healthy Families, School Based Mental Health, and the Psychiatric Rehabilitation Program.
The Healthy Families program, now in its 10th year, is a home visiting program open to any pregnant wom-an and her family unit. The family can remain in the program until the youngest child is 5 years old. This strengths-based program celebrates the children’s
and the family’s successes every day and throughout the year. Fathers are encouraged to participate. Well-trained paraprofessionals bring developmentally ap-propriate activities, toys, and resources to the home and teach family bonding and child development. The program is based on the Olds home visiting program, which has been proven to prevent child abuse and de-linquency.
Eastern Shore delivers individual and group therapy, teacher and staff education, consultation, and resourc-es in its School-Based Mental Health program. Social workers are placed in every school in a particular rural
county to help in early identification of children who are experiencing mental and behavioral problems and pro-vide services to help these children. Six years of data show reduced behavior and mental health problems and increased attendance and self-esteem for youths who participate in the program. Parents are included in the program when possible, to ensure better results.
Many children with mental health and behavioral problems also have delays in social and personal skill development, such as communication, interpersonal, task, self-management, and adaptive skills. The Psychi-atric Rehabilitation staff at Eastern Shore are trained
Kathryn seifert, Phd, CEO/Owner, Eastern Shore Psychological Services, Salisbury, MD / [email protected]
From Home to School: A Multi-Pronged Approach at Eastern Shore

From The Field
34 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
to provide skill-building activities that are fun, engaging, and based on the skill level of the child. The staff also reinforce values such as respect and kindness to others.
Eastern Shore’s strengths-based programs have flourished and help support many families emotionally, educationally, and de-velopmentally. All three programs are based on wellness research program models. In combination, they foster success in children, families, and communities.
E arly childhood educators are seeing a rapid rise in disruptive and aggressive behaviors in preschool
children. Studies at the Devereux Institute indicate that the increase in these behaviors corresponds to a decrease in the protective factors (LeBuffe & Na-glieri, 1999) of attachment, self-control, and initia-tive. Prevention and early intervention research indi-cates that raising the protective factors associated with resilience at an early age has a direct impact on the number of children who commit crimes and have serious emotional and mental health issues as teenagers and young adults.
The Child Access Program is a grant-funded project that currently serves 160 children in three preschools in Framingham, Massachusetts. The model is facili-tated by a team of three mental health clinicians we call “child specialists” and a program coordinator to oversee daily operations.
The program has two tiers. The first tier, the inter-vention tier, is basic and involves responding to the significant behavioral problems and mental health needs of identified children by assembling a team of parents and professionals to provide the children with appropriate services. The services are short
term, billable, and evidence-based. This aspect of the program is easily measured in dollars per hour per service type.
The second tier of the model is prevention-based and founded on core principals of the Devereux Early Childhood Assessment program. This aspect of the program uses a strengths-based approach to analyzing and problem solving. It offers teachers an opportunity to reflect on and explore changes in their teaching practices and to increase their competency in the program’s core training areas: resiliency, ob-jective observation, and management of challenging behaviors.
A workshop series for parents offers them new skills for raising a resilient child and coping with behavior-al challenges. In addition, each child receives three DECA social and emotional competency screenings during the course of the school year. The goal for these assessments over a 10-month period is to see an increase in protective factors and a reduction in problem behaviors for all children. Child specialists create universal classroom profiles based on DECA results to look for patterns that may indicate a need for changes in the environment or daily practices in
the classroom. The specialists develop and imple-ment positive (behavior) plans for individual children to increase protective factors and respond to con-cerns or challenges identified as a result of the DECA screening. Weekly meetings with each teacher in and outside of the classroom provide ongoing profes-sional development.
The program’s outcomes are excellent. Each year since the program began, we have seen an increase in one or more protective factors for all children. Teachers and parents report increased confidence and competency as well as a reduction in challeng-ing behaviors.
TCAP is in its third year, and we have just received word that the grant will be funded by the MetroWest Community Health Care Foundation for another cycle. In these difficult economic times, receiving such funding is no small feat. The grant approval is also an affirmation that early intervention and prevention provide long-term, sustainable outcomes and raise confident and resilient children who are poised to contribute positively to their world.
T he Young Children’s Assessment and Treatment Services program of Samaritan Behavioral Health
in Dayton, Ohio, is dedicated to meeting the mental health needs of children from birth through age 5.
YCATS provides intensive behavioral therapy groups for behavior-disordered children ages 3 to 5. Two spe-cially trained early childhood mental health thera-pists guide each group of 8 to 10 preschoolers. YCATS
operates eight intensive behavioral therapy groups: three at Samaritan’s main facility and five co-located in the community in YCATS’ partner early childhood education settings.
sally sweitzer, Ma, Program Coordinator, The Child Access Program, Framingham, MA / [email protected]
John d. Kinsel, Ms, lPcc-s, YCATS Clinical Supervisor, Samaritan Behavioral Health, Inc., Dayton, OH / [email protected]
Screening and Problem-Solving: Preschool Interventions at Child Access Program
Intensive Behavioral Therapy Groups Foster Wellness at Samaritan

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 35
Intensive group interventions are strengths-based and focus on the three resiliency factors of attachment, self-control, and initiative, as identified in compre-hensive studies of trauma-exposed children (Werner & Smith, 1982). The intervention’s intent is to ameliorate problem behavior by promoting prosocial functioning. Progress is tracked with the Devereux Early Childhood Assessment–Clinical Form (LeBuffe & Naglieri, 2003).
Children are eligible for intensive group therapy if they have been or are at risk of being suspended or expelled from their early childhood education program. Other young children with home-centered or trauma-based issues are assigned to individual treatment with thera-pists who work with them and their families in play and dyadic therapies. YCATS clients may also access on-site psychiatric consultation and sensory integration–based
occupational therapy if such a need is assessed.
YCATS also sends early childhood mental health consul-tants into the community to consult on site with a wide array of early childhood education programs. Services, which are based on the Georgetown model (Substance Abuse and Mental Health Services Administration, 2001), include early childhood education staff training, center- and classroom-based consultation, and indi-vidual child- and family-focused consultation.
Infant mental health needs are addressed through partnership with local organizations that serve children from birth to age 3. The infant mental health specialist meets with the parent−child dyad in their home to ad-dress issues of attachment, behavior management, and specific disorders of infancy (Zero to Three, 2005).
By promoting emotional wellness in young children, YCATS helps to prevent future emotional and behav-ioral problems.
REfEREncESLeBuffe, P. A., & Naglieri, J. (2003). The Devereux Early Childhood Assessment—Clinical form. Lewisville, NC: Kaplan Press.
Shonkoff, J. P., & Phillips, D. A. (2000). From neurons to neighbor-hoods: The science of early childhood development. Washington, DC: National Academies Press.
Substance Abuse and Mental Health Services Administration. (2001). Early childhood mental health consultation. Washington, DC: Author.
Werner, E. E., & Smith, R. S. (1982). Vulnerable but invincible: A longitudinal study of resilient children and youth. New York: McGraw-Hill.
Zero to Three. (2005). Diagnostic classification 0–3: Diagnostic classification of mental health and developmental disorders of infancy and early childhood. Washington, DC: Author.
S ome children are labeled as problem children because their behavior is unacceptable they act out, cannot
sit still for circle time, do not make friends easily, and do not do well in day care settings. The experts at the Providence Center’s Early Childhood Institute, in Provi-dence, Rhode Island, believe that behavior has meaning and that understanding that meaning is the first step in making the early years a positive experience for children, their families, and their early childhood care providers.
For children from birth to nearly 6 years old who have behavioral, social, or emotional difficulties or delays, it can be difficult to succeed in a day care or Head Start program or to enter kindergarten ready to learn. The staff at the ECI works with children and their families to explain inappropriate behavior and teaches families, early childhood educators, and the children strategies that help children succeed both at home and in early childhood settings.
“When children are referred to us, we believe they are simply ‘misunderstood,’” says Simmy Carter, LICSW, RN, clinical supervisor of the ECI. “Our goal is to understand the family’s goals for the child and the causes of their behavior and teach strategies that help not only the children but also their families and early childhood pro-viders.”
Referrals to the ECI include children who are exhibiting disruptive behaviors and are in danger of being asked to leave their day care. At the request of a parent, pediatri-cian, day care provider, school district, or state agency,
an ECI clinical therapist goes to the child’s day care to observe the child and identify his or her developmental, emotional, or behavioral needs. The clinical therapist then works with the adults in the child’s life to make the child’s environment more supportive and to teach him or her better social and emotional management skills. Sometimes therapists discover that the challenging “problem” behaviors are the result of a developmental delay.
“After an ECI clinical therapist observed my son, she thought that he might have difficulty in processing lan-guage,” said an ECI parent. “A speech and language test confirmed this, and it all made sense he didn’t under-stand what we were telling him, so that’s why he was misbehaving.”
After the observation, the ECI staff work to develop a positive relationship between the child and his or her family. They teach the family the importance of emotion-al regulation, about typical development and the ways in which young children are very different than adults, and the power of strong relationships. Families learn strate-gies that will help them manage their child’s challenging behavior with understanding and control, including giv-ing clear instructions, maintaining consistent routines, calming down, and having fun as a family.
“If a child is having bedtime hassles, we work with the family to develop an evening routine that makes bedtime special instead of a fight,” explains Carter. “Most impor-tantly, we remind parents that a positive relationship
with their child is vital to good behavior.”
Some children also attend the ECI Day Treatment Center for several consecutive weeks to hone their emotional management skills, their communication skills, and their ability to take turns, wait, and make choices. Designed to look like a traditional day care, the ECI Day Treatment Center implements a developmentally appropriate cur-riculum that promotes social−emotional development while engaging children in typical play centers that encourage interaction as the children explore dramatic play, art, and basic reading and math concepts.
Early childhood specialists also provide consultation and training for childcare providers in the community on how to promote healthy social and emotional development in their students. During interactive trainings, teachers learn the power of positive relationships and high-quality supportive environments as well as how to observe be-havior.
“Kids talk to us through their behaviors,” says Bryna Hebert, MEd, the ECI clinical therapist who conducts the trainings for early childhood educators. “We help teachers learn the function of the child’s behavior and how to create a plan to replace inappropriate behaviors with more acceptable behaviors.” Training units include Building Positive Relationships, High-Quality Supportive Environments, Supporting Social and Emotional Devel-opment, Behavior Has Meaning, and Parenting Survival Skills.
Kristle l. gagne, Marketing Communication Specialist, The Providence Center, Providence, RI / [email protected]
Providence Center Focuses on Understanding Behaviors

From The Field
36 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
R esearch on postpartum depression makes it abun-dantly clear that maternal depression not only
affects the women who suffer from it but also has long-term deleterious effects on their children. The literature shows a great consensus that maternal de-pression is related to cognitive and language delays during infancy that often persist into adolescence. Maternal depression is also associated with childhood depression, early conduct disorders, sleep disorders, childhood injuries, and lack of involvement in school activities and is linked to physical health problems such as asthma.
Many of these difficulties can persist into adulthood and may predict later pathologies, such as physical, mental health, and substance abuse issues. Fortu-nately, outcomes for children of mothers who receive treatment are much more favorable. Efforts to identify and treat postpartum depression are therefore critical to the prevention of childhood illnesses and mental health issues that can affect lifelong health and pro-ductivity.
Ulster County Healthy Start and Dutchess County Healthy Families are home-visiting programs of the Institute for Family Health, in New York, New York, that provide prenatal and parenting education and support to at-risk families. Program goals include supporting child development and parent−child bonding and preventing child abuse and neglect by conducting home visits that use an evidence-based parenting cur-riculum. Professional home visitors hold sessions that focus on strengthening the parent−child relationship, assisting families in meeting self-sufficiency goals, and helping children reach developmental milestones.
The programs recently implemented depression screening for all participants to address the evidence
that depressed mothers are at increased risk for ne-glecting their infants, create less consistent and less stimulating parenting environments, and may tend to use more punitive parenting behaviors. Currently, mothers who are identified as depressed are given ap-propriate referrals to mental health treatment.
As a further intervention, the Institute for Family Health is developing a cognitive−behavioral curriculum that home visitors can implement in addition to their regu-lar parenting curriculum. This intervention is designed to specifically target dysfunctional mother−child interactions, which are typical when mothers have postpartum depression. This 12-week curriculum will be used with all new mothers who are recognized as having significant symptoms of depression, defined as mothers who score 10 or greater on the Patient Health Questionnaire Nine-Symptom Checklist, a validated tool for identifying depression.
The Institute for Family Health is currently in the initial phases of the project and has begun screening all par-ticipants in the home-visiting programs. The interven-tion that uses the new cognitive−behavioral curriculum is expected to be launched in January 2010. After this point, comparisons will be made between depressed participants who received the existing curriculum and those who receive the newly developed intervention curriculum. The intervention is expected to improve depression for mothers with postpartum symptoms. The increased positive parent−child interactions that the curriculum will encourage are known to influence development; therefore, the intervention is also ex-pected to improve cognitive and other developmental scores for infants.
By implementing this cognitive−behavioral interven-tion, the Institute for Family Health expects to improve
depression symptoms for mothers and improve de-velopmental scores for infants to generate long-term protective benefits.
A unique aspect of this project is its reliance on home visitors who are not formally trained clinicians. The cognitive−behavioral strategies endorsed in the new curriculum are easy to master and communicate to families and do not require an academic background in psychology or social work. The Institute for Family Health will provide the home visitors with specialized training in administering the activities to ensure that they are prepared to use the techniques.
Home visitors will give the new mothers colorful, user-friendly handouts that focus on creative ways to ad-dress lack of contact and emotional bonding with their infants. For example, one activity will promote eye contact and co-smiling (i.e., shared smiling between mother and infant) and will provide psychoeducation to mothers about the importance of these gestures for infant brain and social development. The home visi-tor will guide mothers through the activities and leave them with homework to practice with their babies until the next visit. Although these techniques are specifical-ly designed to help improve infant outcomes, they are also expected to help reduce maternal depression.
Because this project will be administered by noncli-nicians, it is economically feasible and applicable to many other programs and organizations that work with at-risk families. Therefore, other home-visiting programs could easily adopt the model. If success-ful, this model will provide an effective intervention to decrease depression in mothers at risk of developing a major depressive episode and will increase positive child health outcomes.
M any professionals have examined engagement to illuminate the need for increased enrollment and
retention of clients in mental health treatment (McKay, 2004; Spooner, 1996). The New York State Office of Mental Health Workgroup (2008) studied and reported on the importance of family and child engagement as an early intervention and prevention strategy. Engage-ment is increasingly being recognized as an important
part of the therapeutic process.
Engagement is important for two reasons. First, treat-ment and other services may be available, but if they are not accessed, then people do not benefit. If people use available treatment, then the use of more costly services is avoided. Second, people experience more stability when they take advantage of available services rather than go through the revolving door
of treatment starts and stops. Engagement is even more pertinent as it relates to prevention and early intervention.
Care providers interested in prevention and early intervention use engagement efforts to reach out to clients in their real-life environments rather than wait for them to walk through the door. Engagement is most effective when it is on the client’s terms,
nikki Pison, lMhc, Program Director, Institute for Family Health, New York, NY/ [email protected]
stephen Watters, Ma, Executive Director, Youth and Family Link, Longview, WA / [email protected]
Addressing Maternal Depression Fosters Child Development at Institute for Family Health
Youth and Family Link Obtains Results through Engagement for Early Intervention

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 37
F etal alcohol spectrum disorders is an umbrella term describing the range of effects that can occur in an
individual whose mother drank alcohol during pregnancy. These effects include physical, mental, behavioral, and/or learning disabilities. FASD is believed to be underre-ported and obtaining an exact estimate of prevalence is difficult. In 2001, it was estimated that about 1 percent of children have an FASD.
FASDs are the leading preventable cause of develop-mental disabilities and birth defects. All FASDs are 100% preventable if a woman does not drink alcohol while she is pregnant or could become pregnant. Presently, there is no known “safe” amount of alcohol that can be consumed during pregnancy. Fathers can also play an important role in helping mothers abstain from drinking alcohol during pregnancy by encouraging avoidance of social situations that involve drinking and by not drink-ing alcohol themselves. Communities and health and social service organizations can help prevent FASDs through education and intervention.
Children with an FASD who receive special education are more likely to achieve their developmental and educa-tional potential. These children need a loving, nurturing, and stable home life to avoid disruptions, transient life-styles, or harmful relationships. Children with an FASD who live in abusive or unstable homes or who become in-volved in youth violence are much more likely than those who do not have such negative experiences to develop secondary conditions.
Until recently, screening, diagnostic, and intervention ser-vices specifically designed to meet the unique needs of children with an FASD were not available in Philadelphia, PA. COMHAR, Inc., a private, not-for-profit community-based human services agency in Philadelphia, PA was one of eight providers nationwide awarded a subcontract in 2008 for FASD Screening, Diagnosis and Treatment/Intervention with Northrop Grumman Corporation, a contractor for SAMHSA’s FASD Center for Excellence. This initiative boasts a partnership with two diagnostic entities: St. Christopher’s Hospital for Children – Center for Children with Special Health Care Needs in North Philadelphia, representing a site-specific diagnostic model during which children are evaluated by a team in one day, and Center City Pediatrics in South Philadel-phia, representing a networking diagnostic model, where children are evaluated over a period of time by various independent professionals, completing the process with the developmental pediatrician. Both models offer diag-nostic teams that may include a pediatrician or develop-mental pediatrician, nurse/nurse practitioner, medical specialists in dysmorphology, occupational therapist, child psychologist, social worker, parent advocate, and when necessary a physical therapist and speech lan-guage pathologist.
The goal of The Philadelphia FASD Screening, Diagnosis and Treatment Initiative is to improve the functioning and quality of life of children and their families by diagnosing those with an FASD and providing interventions based on
the diagnosis. Our priority target population is children birth through seven years of age presently receiving ser-vices in COMHAR’s Early Intervention or Behavioral Health programs. This initiative fosters medical homes (central-ized bases for all medical treatment) and coordination of care resources for children with FASD and their families. The project includes screening, assessing, diagnosing a child with an FASD, providing needed interventions/sup-ports (SDT), and case management (follow up).
Integration of the FASD-SDT initiative into COMHAR’s existing system of care expands the range of services available to our children. Because participation in this initiative is voluntary and mothers often have difficulty admitting to behavior that may have contributed to their children’s disabilities, education and advocacy are very important. Having met specific criteria for risk of an FASD, children are eligible to receive a screening. Follow-ing positive screening results, families are referred for a multidisciplinary diagnostic evaluation to confirm or rule out an FASD. With this additional information, we are better able to assist the family with specific interven-tions and tailored strategies to meet the needs of the child and family.
The information in this article about FASD has been printed with permission from the Department of Health and Hu-man Services – Centers for Disease Control and Preven-tion. Content source: National Center on Birth Defects and Developmental Disabilities. For more information, go to www.cdc.gov.
linda s. Bamberger, lsW, Director of Children’s Services and Jaimee Arndt MBA, Program Director, COMHAR, Inc., Philadelphia, PA / [email protected]
COMHAR Addresses Fetal Alcohol Spectrum Disorders
nonthreatening, and provided in a progressive manner that takes small steps. Engagement recognizes clients’ lack of involvement not as resistance to treatment but as the result of system barriers that deter them from participation.
Youth and Family Link, a licensed mental health agency in Cowlitz County, Washington, specializes in engagement with children and families. Youth and Family Link’s par-ent agency, Toutle River Ranch, which has served youths since 1960, developed the program in 1997 to engage youths and families to enroll in mental health treatment and to remain in treatment. The agency’s hope was that the program would help youths avoid unnecessary hospi-talizations, decrease their frequent use of crisis services, and decrease their visits to the hospital emergency room. Outcome data have shown a significant reduction in use of these costly services and an increase in prosocial behav-ior, such as family involvement and school attendance.
Early intervention engagement has a double definition:
(a) to engage the child and family early in life or (b) to engage the child early in the intervention process. Either approach encourages the child and family to access and use available services and thus avoids adding further complexity and difficulty to the family’s already stress-ful life.
By working closely with other mental health providers, Youth and Family Link staff reach out at the earliest stage of involvement to engage the child and family. The initial contact might occur in the hospital, emergency room, home, school, or other setting. Referrals come from a variety of professionals as well as from family members and self-referrals.
Youth and Family Link staff, who are trained in engage-ment approach and techniques, respond to referrals by initiating contact within days or even hours. They try to respond during the critical window of opportunity when the child and family may be receptive to services but will not follow through if left to take the initiative.
Early intervention engagement helps the child and family through the barriers that either deter them from enrolling in services or keep them from returning after they have begun treatment. Clients who access and use treatment are involved in proactive mental healthcare; problems therefore do not deteriorate to the point that they re-quire more costly services (e.g., hospitalization, emer-gency room treatment, and crisis services).
Whether it takes place early in a child’s life or early in the intervention process, engagement helps the child and family through the barriers that deter them from beginning or continuing treatment. Early intervention engagement in mental health services provides greater opportunity and benefit so the client may succeed in accomplishing his or her treatment goals. If early inter-vention engagement is a primary part of the therapeutic process, more clients could become involved in treat-ment, remain in treatment, live more comfortably, and be less costly to the system.

From The Field
38 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Saving our future substance use and suicide Prevention Programs for Youth
Recognizing their critical role in saving and improving communities, many behavioral health organizations
reach out to prevent substance abuse and suicide among youth through education and promotion programs.
C ollege Dreams was founded in 1998 as an al-cohol and drug prevention program for 33 sixth
graders at two middle schools in Josephine County, Oregon. Josephine County is a rural timber county in southwest Oregon with a population of 81,618, including 16,508 children from infancy to age 18. Oregon’s preliminary March 2009 unemployment rate of 12.1% is the second highest nationally, and Josephine County’s 16.8% rate is 38% above the Oregon average. During 2008, College Dreams pro-vided prevention services for approximately 1,238 children, youths, and family members.
College Dreams promotes healthy development for children and youths, especially those who have multiple risk factors for school dropout, substance abuse, and delinquency. Our framework is based on scientific evidence regarding the risk factors for substance abuse and the protective factors that lead to long-term success for children who are be-
set by multiple and severe life adversities. College Dreams has interagency agreements with both local school districts and provides regularly scheduled outreach services to 428 “Dreamers,” who attend all nine local secondary schools. Long-term services begin during middle school, continue throughout high school, and are still being provided for 280 alumni who are in postsecondary education, train-ing, or vocational settings. Descriptions of core Col-lege Dreams programs follow.
The College Incentive Program, a program for re-siliency development, serves students with three or more risk factors for school dropout, substance abuse, and delinquency. Our longitudinal studies show that without help, 58% of students with such risk factors drop out of high school and 44% have been arrested by 10th grade. Their odds of delin-quency and substance abuse are 10 to 15 times higher than those of low-risk students. Dreamers
earn college scholarship awards, barrier removal funds, and special outings through good atten-dance, good grades, healthy youth activities, and community service. Our prevention specialists de-velop powerful long-term relationships with Dream-ers as role models, skill trainers, counselors, crisis intervention specialists, and life success coaches. An external program evaluation conducted by RMC Research (Portland, Oregon) found that the Col-lege Incentive Program produced large effect sizes for Dreamers (vs. a matched comparison group) in terms of reduced dropouts and delinquency arrests as well as increased rates of acceptance into the National Honor Society and preparation for college.
Fostering Success was developed to provide spe-cialized resiliency development opportunities (e.g., summer day camps, recreational outings, service projects) for children and youths who are in foster care. Research on foster care has clearly document-
tom and Judie drummond, Codirectors, College Dreams, Grants Pass, OR / [email protected]
College Dreams Begin in Middle School

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 39
S kills Training And Recognition is a primary preven-tion program that is based on the Participate and
Learn Skills program tested by physicians Marshall Jones and David Offord (1989). STAR was implement-ed by Five Town Communities That Care in midcoastal Maine in the fall of 2004 to increase levels of three protective factors: community recognition for proso-cial involvement, rewards for prosocial involvement, and prosocial involvement. In 2008, the Substance Abuse and Mental Health Services Administration awarded Five Town CTC its Science and Service Award for substance abuse prevention, one of only seven such awards given nationally.
The service area for STAR is a rural community with a population of 13,000 in which local rates of youth substance abuse, suicide, delinquency, and violence are elevated and have been the focus of much effort since 2004. STAR was chosen as a good match for the community’s risk and protective profile.
STAR is offered as an after-school program to all local students in grades 5 through 8. It provides opportuni-ties for children to learn new skills, recognizes them as they master those skills, and connects them with places in the community where they can use these
newly mastered skills. For the past 2 years, an analy-sis of grade cohorts has shown that more than 50% of the current grade 5 through 8 population had at-tended STAR at least once during middle school. Many students attend multiple cycles.
Students attend STAR 3 days per week in 6-week cy-cles. Two days each week are spent with skill instruc-tors and are focused on learning new skills. The third day is a “Fun Friday,” when all students in the program gather for loosely structured activities designed to help them get to know one another before they come together as part of the same student body at the local high school.
STAR offers training in skills that run the gamut from the arts to athletics. Past classes have included ani-mal husbandry, yoga, tennis, rock climbing, painting, cooking, knitting, and snowshoeing. Any skill set that can be used in the local community in a prosocial way is a candidate for a STAR class. The program is supported entirely by grants and local contributions. There is no cost to participants or their families.
At the end of each cycle, participants, their families, program staff, and the general public gather for a community celebration to recognize each student’s
accomplishments. The program is offered 3 times a year — in the fall immediately after the start of the school year, in the winter, and in the spring before school summer vacation.
STAR uses the original Participate and Learn Skills program model, which included a focus on “chunk-ing” skills into levels that can be mastered in approxi-mately 8 hours of focused practice and instruction. Dividing the skills into such chunks provides enough challenge to be motivational but not so much that students get discouraged and give up.
An integral part of STAR’s adaptation of the Partici-pate and Learn Skills program is the infusion of social development theory into staff training. Staff learn how to offer young people opportunities to learn new skills and to provide recognition as students progress in or-der to increase the likelihood that they will internalize the standards and beliefs staff express. Skill-specific feedback is important both for skill mastery and for the bonding that takes place. Rather than saying, “Good job,” for example, the tennis instructor learns to say, “Lisa, your follow-through on that swing was excellent.” Not only does Lisa get reinforcement for her follow-through, she knows that the instructor was
ed that foster children are at exceptionally high risk for academic failure, substance abuse, mental health issues, homelessness, and lifelong problems. Through a contract with our child welfare branch office, we are serving 32 children in Fostering Success.
The Guiding Lights Mentoring Program is a school-based mentoring program that has 132 adult and stu-dent mentors who volunteer to meet weekly with 137 “most in need” fourth-grade to ninth-grade students at five middle schools, four high schools, the YMCA, and the Boys and Girls Club. The middle school stu-dents selected for Guiding Lights had a mean grade point average of 1.61 and a 9.2% absence rate when they entered the program. Mentored students receive academic motivational enhancement services, in-cluding special outings, recognition ceremonies, and earned incentives for academic improvement. Initial program evaluation results from Portland State Uni-
versity’s Regional Research Unit indicate significant improvement in academic grades and attendance for mentored participants in contrast to random com-parison students.
Dream$avers: Sixty-one low-income students current-ly participate in our Oregon Individual Development Account Program, which provides each Dream$aver with financial education, individualized planning, and a $6,000 college scholarship match when he or she saves $2,000 in a special trust fund account. Dream$avers serves as a powerful incentive for high-risk students to excel in school and to avoid alcohol and drug problems that interfere with academic success.
Strengthening Families is an evidence-based family camp program run by College Dreams. In the three family camps held so far, Strengthening Families has served 49 families (totaling 137 family members, in-
cluding infants, toddlers, children, teens, and adults). Approximately 86% of the families “graduated” from the program. Most of the participating families were referred by local treatment programs, schools, and the child welfare office because of serious issues with substance abuse, youth behavior problems, or crimi-nal justice issues.
College Dreams has received numerous awards for academic excellence from Oregon foundations and organizations. Our program has been recognized as a National Prevention Network “promising practices” program for promoting academic excellence and pre-venting substance abuse, has completed a nation-ally competitive Substance Abuse and Mental Health Services Administration Service-to-Science contract, and was selected for two national SAMHSA workshop panels.
dalene dutton, Executive Director, Five Town Communities That Care, Rockport, ME / [email protected]
Five Town Sees Results from Skill Building and Recognition

From The Field
40 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
S pectrum Programs started the You Gotta Know Campaign at a large university in South Florida.
First, we assessed the students’ alcohol use, the consequences they experienced, and their knowl-edge of drinking. A total of 1,229 students were sur-veyed during three time periods in 2008 and 2009. Students were 45% male and 53.7% female and
were an average of 21.6 years old. They were 10.1% White, 17.9% Black, 56.9% Hispanic, 5.1% Asian, 0.1% American Indian, and 7.3% other ethnicities.
The survey showed that 59.7% of students had con-sumed alcohol in the past 30 days and that 30.8% had engaged in binge drinking. Some gender differ-ences were found — 67.4% of men had consumed
alcohol in the past month, whereas only 53.2% of women had done so. Most believed that the typical student usually has between five and six drinks in one sitting.
Students reported several alcohol-related con-sequences: driving under the influence (17.7%), having unprotected sex (15.0%), physically injuring
rhonda Bohs, Phd, Vice President of Research Development and Emy Lou Pesantes, MSW, Research Coordinator — Spectrum Programs, Miami, FL / [email protected]
You Gotta Know: Spectrum’s Peer Educators Spread the Word on Prevention
S uicidal ideation is common among youth who live in impoverished urban communities. These young
people may see gun battles between warring drug traffickers every night. They may live with adults who are addicted to drugs or who periodically sexually or physically abuse them.
Early in my career, I worked with a truly extraordinary pediatrician, Michelle Horlein, who was completing her developmental pediatrics residency at Johns Hopkins Hospital. She administered to adolescents a computerized risk assessment tool and found that they were willing to reveal to the computer program what they would not tell an adult. Some of the adolescents were my clients with whom I felt I had formed an open and close relationship but they disclosed to the computerized assessment program high-risk behaviors that they would not dare to share with me.
When I learned of Dr. Horlein’s findings, I discovered a dangerous assumption of my own: I believed that adolescents tell their therapists everything, whereas the truth may be that they tell us only a fraction of
what they feel inside. The adult−adolescent thera-peutic alliance is a cross-cultural encounter riddled with as much distrust and anxiety as any clash of two very different human beings. The cultural rift is one of vast generational difference.
Some years later, I learned that Columbia Univer-sity was experimenting with a computerized mental health screening tool, TeenScreen, and had discov-ered the same phenomenon adolescents would disclose to TeenScreen suicidal thoughts and be-haviors that they would not discuss with the adults closest to them, including, at times, their guidance counselor or therapist.
Two years ago, I initiated TeenScreen at the GUIDE Program in Laurel, Maryland, in one of our middle school mental health programs. On a spare com-puter, I set up the TeenScreen computerized as-sessment software. It essentially works as a talking psychiatric interview that produces a summary of the child’s risk factors for suicide and other men-tal illnesses. After appropriate parental consent is obtained, the adolescent is placed in front of the
TeenScreen-installed computer to complete the in-terview, out of the clinician’s view.
Soon, a child in the care of two perceptive and seasoned school mental health professionals was referred to me and revealed suicidal thoughts to TeenScreen that he had not disclosed to the clini-cians working so closely with him.
The interface between an adolescent and a com-puter screen creates an anonymity that allows more honest disclosure by the adolescent. The comput-erized screening process removes the shame of disclosing socially unacceptable thoughts or symp-toms.
Clearly, today’s youth see the computer as a re-source for connection with others and not as a cold, impersonal technology, as my generation of therapists have. Computerized assessment may be the next advancement in mental health screening, and I think TeenScreen is leading the way with this potentially life-saving new technology.
paying attention to her to see that swing.
Staff do not ignore comments about substance use, violence, bullying, or suicide but address and discuss them. Healthy choices and behaviors are consistently emphasized.
Five Town CTC is engaged in ongoing evaluation of the STAR program. Results are encouraging com-parison of community youth survey data from 2004 and 2008 revealed that grade 8 rates of community recognition for prosocial behavior have increased
by 42% and lifetime alcohol use has dropped by 28%. To date, rates of the targeted protective factors have been steadily increasing, and rates of problem behaviors are trending downward.
lawrence epp, edd, Director of School Mental Health Services, GUIDE Program, Inc., Laurel, MD / [email protected]
Computerized Screening Assesses Risk of Suicide in Youth
NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 41
themselves (13.4%), being involved in a fight (12.2%), binge drinking and driving (8.5%), physically injuring someone else (6.7%), and being forced to have sex (3.9%). These results are alarming compared with those from a national sample; students from the Florida university ranked higher on all but one of the alcoholrelated consequences.
The survey data are consistent with other descriptive studies indicating that college students commonly misperceive their friends and peers as drinking more in quantity and frequency than themselves. Students may not perceive drinking as an impediment to academic achievement because they see it as a normal part of the college experience, or they might expect benefits from drinking that outweigh the risks. A good strategy to discourage on-campus drinking is to educate students about the discrepancy between drinking norms and alcohol expectancies, because most college students have incorrect per-ceptions of their peers’ use. This strategy became the focus of the You Gotta Know campaign.
Group processes including actual and perceived norms for a behavior in a group, modeling of behaviors, and peer support for the behavior influence people’s adoption and maintenance of a behavior. To empower students to develop and implement peer education models, the You Gotta Know cam-paign held a contest soliciting proposals from student organizations and their “ambassadors,” who took leadership roles in educating college students on substance use and abuse risk behaviors. Selected organization ambas-sadors received education on the risks of HIV/AIDS and substance use and abuse among college students, prevention and treatment resources in the community, and how to measure the effectiveness of their activities. Each or-ganization was provided with informational booklets that featured the results of the university survey on substance use.
Along with this information, the student organizations were given a budget of $2,000 to plan, implement, and evaluate their activities. The organiza-tions brought guest speakers to campus to discuss responsible alcohol use and HIV risk behaviors, arranged experiential activities that simulated the effects of alcohol on motor functioning, and held carnivals that provided prizes for increased knowledge concerning alcohol consequences and HIV risk behaviors. Evaluation results indicated that students’ knowledge of peer drinking norms and alcohol expectancies were improved through this peer educator model.
to empower students to develop and implement peer education models, the You gotta Know campaign held a con-test soliciting proposals from student organizations and their “ambassadors,” who took leadership roles in educating college students on substance use and abuse risk behaviors.
From The Field
42 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
“I drank when I was a kid; what’s the big deal?”
“We let our son and his friends drink in our home because we know they’ll be safe.”
“A few drinks won’t hurt them.”
Sheryl Sprague has heard many remarks like these from parents and community members in the 12 years she has worked as a certified prevention professional in Connecticut, which has an underage drinking rate that is 28% higher than the national average.
Sprague currently leads the prevention division of Rushford, one of Connecticut’s largest not-for-profit behavioral health prevention and treatment providers.
“It amazes me that so many parents and community members are unaware of the serious consequences of underage drinking,” says Sprague. “What many people view as a rite of passage is actually life-threatening behavior.”
Underage drinking is the leading cause of death among teens and is a contrib-uting factor to many serious problems, including traumatic injury, burns, violent crime, high-risk sex, and alcohol abuse and dependence.
In 2006, Rushford received two Strategic Prevention Framework grants from the Connecticut Department of Mental Health and Addiction Services to de-velop task forces aimed at helping three large communities prevent underage drinking. The task forces focus on major risk factors associated with underage drinking, including retail availability of alcohol, low enforcement of alcohol laws and policies, and family norms and media messages that accept or encourage alcohol use.
To address retail availability of alcohol to minors, Rushford has purchased hun-dreds of graphic decoders that help retailers easily spot fake identifications and is helping police departments conduct merchant education.
The grant has also funded overtime pay for local law enforcement to target underage drinking parties. “Police will arrest a homeowner who allows minors to drink at his or her home,” said Jeffry Cossette, chief of police for Meriden, Conn. “That’s what this grant is trying to get across, that it’s not OK to let minors drink.” In 2006, Connecticut passed a law that made it illegal to host (or to be aware that one’s home will be used to host) a party at which alcohol is provided to minors. The penalty for breaking the law can range from a fine to one year in prison.
Rushford also developed an aggressive social marketing campaign to combat media messages that encourage alcohol use. Billboards that illustrate the fatal consequences of underage drinking are featured in two high-traffic areas of the state, and a radio campaign spotlights the need for parents to help their chil-dren make healthy choices. Rushford has also collaborated with schools and civic groups to sponsor underage drinking forums, which have been attended by hundreds in the community.
“When you consider the thousands of teens who die senselessly each year as a result of underage drinking, as well as the staggering cost of underage drinking to our country [estimated at more than $53 billion annually], investing in pre-vention activities that help communities build and improve capacity to address the problem is really a no-brainer,” says Sprague.
Research has shown that for every dollar spent on drug and alcohol preven-tion initiatives, communities save between $4 and $5 in treatment and other related costs.
amy hickey, Vice President of Business Development and Community Relations, Rushford, Meriden, CT / [email protected]
Rushford Leads Community Action to Prevent Underage Drinking
underage drinking is the leading cause of death among teens and is a contributing factor to many serious problems, including traumatic injury, burns, violent crime, high-risk sex, and alcohol abuse and dependence.

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 43
Marty laska, lPcc, lIcdc, nccgcII, Director of Employee Assistance Programs, The Source One Group, Wooster, [email protected]
Seeking Help for Adolescents through Employee Assistance Programs
What do parents do when they recognize behavior changes in their teenagers? What action can parents take when their 12-year-old expresses feelings of depression or anxiety? What should parents do when contacted by the school and advised of changes in the behavior of their 16-year-old? What is an adjustment issue, and what is a more serious disorder?
Often, parents are advised to seek counseling for themselves or their adolescent chil-dren as a method of intervention. Even if parents are comfortable with this choice, they face the very real obstacle of paying for the services. Working parents do not usually qualify for publicly supported services. Even if a family has health insurance, treatment can be expensive: many health insurance companies now offer only high-deductible insurance plans (sometimes as high as $5,000 or more for a family). Counseling, even for a child who is struggling, may be seen as a luxury by parents who can hardly afford regular healthcare. Moreover, wait times for public psychiatric services are often long.
An often overlooked and underused resource for families is the employee assistance program offered by many companies. Most EAP programs offer a set number of coun-seling sessions a anywhere from 3 to as many as 10 which are paid for by the em-ployer. No copay or deductible applies, as with health insurance. This benefit is usually extended to an employee’s dependents as well. The EAP service providers are licensed therapists and counselors with at least a masters degree.
EAPs offer significant benefits, the first of which is not obvious to many and lies in the perceptions of the adolescent and the parent. Working with an EAP counselor is often seen as less intimidating than finding a counselor through traditional methods. Families often cite limited finances as a reason intervention was delayed, and most children today are aware of their family’s financial situation. When families use an EAP, the cost factor is removed as a roadblock to the resistant adolescent. In addition, EAP professionals are equipped to address emergency situations and frequently offer same-day appointments as a normal part of their services. Many professionals book evening or Saturday appointments, which makes scheduling far easier for parents and teens alike. These two factors can help avoid delay and missed opportunities to engage the teen.
EAP professionals often understand the work pressures that may be bearing down on the employee and translated to the home. This knowledge can help them facilitate interactions with family members, save time, build trust, and moves the counseling process forward.
EAPs can easily encourage families to make use of the services by distributing bro-chures and handouts to emphasize availability of the EAP to families before serious problems manifest. Employers can hold orientations on the benefits of the EAP at times families can attend. A “family-friendly” message may encourage employees to share demographic information at health fairs.
Learn more at www.eapassn.org.
Kris Povlsen, Director of Prevention, Ben Gordon Center, DeKalb, IL / [email protected]
Sharing the Truth: Ben Gordon Corrects False Perceptions About Peer Use of ATOD
A s I hung antismoking posters at DeKalb High School in DeKalb, Ill., a 15-year-old student approached me and said, “I didn’t realize I was normal.
I really thought that everyone smoked. Now I realize that everyone doesn’t. Thank you.”
Often, adolescents assume that most of their peers are smoking, drinking, and using drugs, and so they want to experiment with these substances, too. Sur-veys among youths in most communities, however, consistently suggest that a majority of youths do not use such substances. Using social norms prevention to send a positive message that lets adolescents know how their friends and classmates really view these issues gives the community, especially parents, a powerful tool for keeping youth on the right track. This positive social norming strategy seeks to change false perceptions of drug use, and statistics show that it is effective.
The DeKalb County Partnership for a Safe, Active and Family Environment’s ini-tial survey of DeKalb and Sycamore high school students in 1999 revealed that 75% of the teens surveyed chose not to smoke and that 57% said they had not drunk alcohol in the past month. 81% of the teens surveyed reported that they did not smoke at parties, and 65% said that they chose to drink beverages other than alcohol. These statistics support the premise that teens overper-ceive their peers’ use of alcohol, tobacco, and other drugs (ATOD). Using these baseline data, DCP/SAFE launched its campaign, and in the past 10 years it has significantly decreased teens’ use of these substances.
Inspired by the normative statistics from the 1999 survey, DeKalb County’s social norms prevention projects are based on a model of identifying and rein-forcing existing protective norms concerning ATOD issues and correcting misin-terpretations about the extent of ATOD use. The main method of this approach is social marketing, primarily through media and other appropriate methods. After analyzing survey results, each month DCP/SAFE designs posters with a new message and displays them throughout schools. It also mails more than 8,000 postcards and letters each month to the families of all participating high school and middle school students. In addition, coalition volunteers display posters in locations adults frequent throughout the community, including banks, dry cleaners, bookstores, churches, police departments, day care facilities, libraries, and various workplaces. Messages encouraging people to “share the truth” that most students don’t smoke or drink alcohol saturate the community through billboards, radio announcements, and television advertisements.
With these figures at its disposal, the community is empowered to confidently embark on a mission of spreading positive messages to reduce adolescent

From The Field
44 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
alcohol and tobacco use. Follow-up surveys indicate that students, parents, and teachers are changing their perceptions and are successfully communicat-ing with teens. During the first year that DCP/SAFE used social norms prevention as a strategy, parents reported a 15% increase in the positive messages they conveyed to their kids about abstaining from alcohol and marijuana usage, and teachers said they increased their messages by 9%.
“Driving home from work, I heard a radio ad ex-plaining that it is normal for kids to avoid and not drink alcohol. I thought, ‘What a novel, refreshing, and positive approach to the issue,’” says Kathy Hicks, the mother of three children. “That evening at home, I repeated the message that I had heard
to my children. I got them to talk about whether this was the normal experience at their school, and it enabled me to have a dialogue about drug use with them.” This refreshing strategy is an important part of a healthy community response to addressing the substance abuse issue among teens.
Ten years after the project was started, the 2008 DCP/SAFE Annual Student Survey shows:
>> 28.4% reduction in alcohol use by DeKalb and Sycamore High School 10th graders between 1999 and 2008
>> 17.2% reduction in alcohol use by DeKalb and Sycamore High School 9th through 12th graders between 2002 and 2008
>> 11.6% reduction in alcohol use by Hinckley−Big Rock High School students between 2006 and 2008
>> 31.2% reduction in alcohol use by Genoa− Kingston High School students between 2006 and 2008
>> 18% drop below the national average in 30-day alcohol use by 10th graders at the four high schools in DeKalb County (DeKalb, Sycamore, Genoa−Kingston, and Hinckley−Big Rock High Schools) in 2008
>> 5.6% decrease in 30-day marijuana use at DeKalb High School between 2003 and 2008.
R ecognizing the need for prevention/early inter-vention services in New Hampshire, which ranks
46th in per capita spending on treatment and pre-vention, Seacoast Mental Health Center on New Hampshire’s Seacoast has implemented several successful programs with significant potential for replication.
New Heights, an out-of-school program offered since 1987, recently developed and implemented an innovative Mentor Program that utilizes evi-dence-based approaches to increase the resiliency of all Seacoast youth, ages 11 to 18, particularly low-income participants and those with multiple risk factors. New Heights provides a safe haven out-side the home where kids can engage in activities to build skills and confidence and connect to caring and supportive adults who can mentor them when their parents may not be able to.
According to Tracey Tucker, New Heights’ director, the key to the program is its formal Resiliency As-sessment, developed by Seacoast’s Dr. Vance, which allows the staff to track and measure each partici-pant’s progress through the academic school year.
“Data generated from each assessment enables us to completely customize each participant’s experi-ence at New Heights,” said Tucker. “From provid-
ing a kid with more one-on-one mentoring time to experiential-learning activities designed to address specific needs, everything we do is designed to tar-get and promote protective factors.”
Founded in 2006, Seacoast’s Adolescent Substance Abuse Program (ASAP) provides critically needed services and support to youth in grades 7 through 12 who demonstrate early and mid level substance abuse, but do not yet require inpatient/residential treatment.
Following an evidence-based motivational enhance-ment therapy/cognitive behavioral therapy model, ASAP incorporates a comprehensive ‘three-phase’ approach over a 12-week period that include: indi-vidualized assessment and intervention/treatment planning, weekly counseling/education groups, in-dividual/family counseling sessions, and case man-agement and ongoing support.
According to Julie Golkowski, child, adolescent and family services director at Seacoast, ASAP’s strength lies in its collaborative approach. “We actively work with judges, probation officers, area schools and we have to because of the complexity of the issues,” said Golkowski, who noted she rarely sees an ado-lescent with a serious substance abuse problem who doesn’t also have mental health issues.
“A teen whose problems stem from trauma needs something different from a youth who gets into trouble at school due to learning difficulties,” she added, although she acknowledged the importance of providing basic rewards as motivators for absti-nence to all participants.
In addition to its prevention-based youth programs, Seacoast offers the statewide Referral Education As-sistance & Prevention (REAP) Program, which is New Hampshire’s only free prevention program helping all elders with alcohol, drugs, mental health prob-lems, or life changes.
Citing the complex nature of these disorders, which often co-occur, Lucille Karatzas, REAP’s statewide director, said they broadened REAP’s initial focus from solely addressing substance abuse to include various quality of life issues. She noted REAP also educates caregivers of “at-risk” elders on how to intervene if an elder becomes unable or unwilling to accept help.
“Our program has been designed to lessen the stig-ma many elders feel when reaching out for help,” said Karatzas. “A big piece of what we do is edu-cation in order to prevent many of these problems before they begin.”
rob levey, Ma, Development and Communications Associate, Seacoast Mental Health Center, Portsmouth, NH / [email protected]
Seacoast Focuses on Improving Quality of Life

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 45
C hestnut Health Systems is battling the growing problem of adults providing minors with alcohol,
particularly in Mason County, a rural county where we provide prevention services. Many Mason County citizens who strongly disapprove of underage drink-ing and of providing alcohol to minors, feel a need to speak out in a way the entire community will notice. Communities across the state have similar issues. The Illinois Liquor Control Commission decided that a united message needed to be sent across Illinois and coordinated the statewide Project Sticker Shock campaign on April 2, 2009.
Youth and adult volunteers from 50 counties went into participating liquor stores to place hundreds of thousands of stickers on liquor packages, posters on walls, and window clings on refrigerator doors, all of
which reminded buyers that it is illegal to provide al-cohol to minors. Project Sticker Shock was covered in newspapers, radio, and television. The message was supported by youth, liquor retailers, police, com-munity coalitions, schools, parents, and others who participated in Project Sticker Shock.
Project Sticker Shock isn’t new, but it is growing. Teen-agers in Erie, Pennsylvania started the first Sticker Shock program 13 years ago, plastering stickers in participating beer stores in three areas of the state. Since then, several states have established their own Sticker Shock programs, including Maine, Michigan, Virginia, New Hampshire, Virginia, and now Illinois.
In Mason County, we got support from many groups in the communities, including the alcohol retailers. Ten out of the 11 liquor establishments that were
approached in Mason County participated, and many of the liquor retailers in Mason County thanked the youth and adult volunteers. When asked about los-ing business from purchases for minors, Jason Hunter from Country General in Manito, IL said, “I want to lose that business. Kids are our future, and no sale is worth it.”
Community complacency about underage drinking can be deadly and damaging. But with the belief that something can be done, followed by action, the com-munity’s acceptance of underage drinking can begin to change.
For more information about bringing Sticker Shock to your community, visit www.abc.virginia.gov/Education /stickershock/sticker_shock.html
Jason Blanchette, Community Prevention Coordinator, Chestnut Health Systems-Lighthouse Institute, Normal, IL / [email protected]
Project Sticker Shock Involves the Community in Sharing a Message
1-800-845-1209 • Fax: 973-239-6241 [email protected] • www.jjnegley.com
Follow the leaderNegley Associates, founded in 1960, is the leading
underwriting management firm serving the
insurance needs of BEHAVIORAL HEALTHCARE
and SOCIAL SERVICE agencies. We are
proud of our role in the development of
innovative insurance policies designed to meet
emerging coverage needs. We are committed to
providing outstanding service to our insured clients, and
to the nationwide network of insurance professionals who
market our products.
We are proud to announce the launch of our new website
and on-line applications.
To take advantage of this time saving convenient option, please
visit us at www.jjnegley.com

From The Field
46 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Prevention and Early Intervention Programs for Special-Needs Populations
Community mental health organizations share examples
of prevention and early intervention efforts among senior citizens,
the incarcerated, persons with serious mental illness, and other high-needs groups.
S enior Reach is an award-winning, innovative part-nership that provides preventive education, out-
reach, and mental health treatment to adults ages 60 and older in five counties in the Denver, Colorado metro area. The program’s mission is to support the well-being and independence of seniors by educat-ing the community about how to identify and refer elders who may benefit from mental health treat-ment, care management, information and referrals, or wellness programming.
Three agencies (Seniors’ Resource Center, The Men-tal Health Center Serving Boulder and Broomfield Counties, and Jefferson Center for Mental Health) partnered to develop an elder-friendly infrastructure to meet the needs of seniors. The result of the part-nership is reduced duplication of effort, expanded mental healthcare, creation of a “one-stop-shop” call center, and collaboration rather than fragmen-tation across five counties.
Two key strategies for the Senior Reach program are education provided to the community and preven-tion services offered to older adults.
The community-based education is provided in a variety of settings to people who may not know when a referral to mental health would be appropriate. Education is tailored to the needs of the audience and covers such topics as
>> Why Senior Reach is needed.
Vicki K. rodgers, Ms, lPc, Deputy Chief Operating Officer, Jefferson Center for Mental Health, Wheat Ridge, CO / [email protected]
Jefferson’s Senior Reach Educates the Entire Community
aCroSS tHe SpeCtruM

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 47
T he Missouri Department of Mental Health and the Coalition of Community Mental Health Centers
have come together in a preventative health initia-tive to identify people with serious mental illness who are at risk for diabetes. Targeting people with mental illness for screening and identification of prediabetic markers is especially important given that the preva-lence of diabetes is 2 to 4 times higher in people with SMI than in the general American population (16 to 25% vs. 7%, respectively; Dixon et al., 2004). Addition-ally, many people with SMI who have diabetes are not receiving treatment (Nasrallah et al., 2006).
People who have both schizophrenia and diabetes are among the most vulnerable and costly consumers in state Medicaid systems. In a 2005 study of 19,733 Missouri Medicaid consumers diagnosed with schizo-phrenia conducted by Care Management Technolo-gies (a subsidiary of Comprehensive Neuroscience), the CMT risk predictive model found the concurrence of schizophrenia and diabetes to be one of the most significant variables predicting high Medicaid costs and adverse consumer outcomes (Byrd et al., 2005). The goals of the preventive initiative are to help Mis-souri identify people with prediabetic conditions who are receiving mental healthcare services in commu-
nity mental health centers and to improve the coordi-nation of care for consumers diagnosed with diabetes. CMT serves as the clinical data analytics partner for the Missouri Coalition of Community Mental Health Centers in this project. Eli Lilly and Company serves as the funding source for the initiative.
The program assists Missouri with the following:
>> Identification of prediabetes in patients who are receiving mental healthcare.
>> Identification of CMHC consumers who have fully developed diabetes and might not have received the diabetes self-management education and management support recommended by the Ameri-can Diabetes Association.
>> Dissemination of consumer-focused self-manage-ment education tools.
>> Distribution of appropriate case manager educa-
tional materials and referral information.
The program uses Medicaid claims data to iden-tify consumers according to CMT-developed clinical markers for the full spectrum of diabetes disease states treated at CMHCs. Of the 50,097 consumers statewide with markers for prediabetes, about 26,918
have received some type of care by a Federally Quali-fied Health Center or CMHC.
After the identification analysis, the Missouri De-partment of Mental Health strengthened the annual screening requirements for CMHCs and state psychi-atric hospitals to include screening for prediabetes. A screening and documentation tool that follows the ADA−American Psychiatric Association guidelines for follow-up of identified patients was designed and distributed to the CMHC nurse liaisons and state hos-pitals. An online collection tool is being designed to record collected data and improve continuity of care. The Missouri DMH is providing funding for each CMHC to purchase screening equipment for lipid panels and blood glucose and to purchase scales that calculate body mass index, which will assist with ongoing risk evaluation.
During the analysis phase, an additional 6,717 clients served by the Missouri CMHCs were identified as hav-ing Type 1 or Type 2 diabetes. The CMHC nurse liaisons assisted with follow-up and referral of the consum-ers to local diabetes self management education or medical nutrition therapy services, as appropriate. CMHC nurses are also working on a common self-
Joe Parks, Md, Director of Comprehensive Psychiatric Services, Missouri Department of Mental Health, Jefferson City, MO; george oestreich, Pharmd, MPa, MoHealthNet, Jefferson City, MO; tim swinfard, Chief Executive Officer and President, Missouri Coalition of Community Mental Health Centers, Jefferson City, MO; rachelle glavin, Disease Management Coordinator, Missouri Coalition of Community Mental Health Centers, Jefferson City, MO; Kellie shuck, Health Liaison, MHNP, Comprehensive Neuroscience, Inc. (CNS), Morrisville, NC; sandra Ballentine, Diabetes Director, CNS, Morrisville, NC / [email protected]
Missouri’s Diabetes Prevention Efforts Improve Consumer Wellness
>> Signs that could indicate that an older adult needs help.
>> How to approach and refer a senior in need.
>> Realities of aging well, including suicide preven-tion and facts.
Organizations (e.g., businesses, clubs, healthcare providers, and agencies) have invited Senior Reach clinicians to train their staff. In 3 years, more than 6,000 people have become the “eyes and ears” of the community and potential referral sources. Once a referral is made, Senior Reach staff reach out to that senior to develop a solution-focused plan for
next steps. Our work and previous research indicate that 50% to 75% of the older adults referred will need mental health services.
Prevention services include wellness-based classes, safety and prevention assessments, and screening for depression and anxiety. Our goal is to address con-cerns before more serious problems develop. Senior Reach has staff in Wellness Now!, a Jefferson Center for Mental Health team providing myriad wellness classes and services that focus on integrated health. Because of programming designed for elders, more older adults now self-refer and are aware of how a program like Senior Reach can enrich their life. Almost
1,000 prevention services have been provided in the past year, indicating that seniors are interested in liv-ing full, healthy lives and are focusing on nutrition, safety, mental wellness, and life review.
Senior Reach was designed to bring hope, relieve depression, and increase socialization. The program outcomes are statistically significant, but even more important are the dramatic and positive effects seen in the lives of the older adults served. The program is becoming widely recognized as a promising practice to serve seniors and receives high customer satisfac-tion scores.

From The Field
48 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
N outh Carolina’s reform of its mental health, de-velopmental disabilities, and substance abuse
system began in 2001. Since then, concern has grown about psychiatric systems of care and the in-creased use of state-operated psychiatric hospitals. In 2008, the state requested an improvement in the connection for discharge between local manage-ment entities and state-operated psychiatric facili-ties. LMEs are agencies of local government that are responsible for managing, coordinating, facilitating, and monitoring the provision of mental health, de-velopmental disabilities, and substance abuse ser-vices in the catchment area served.
The East Carolina Behavioral Health LME has re-sponded to the state’s request with the Second Mile project. ECBH LME serves a nine-county catchment area surrounding its headquarters in New Bern, North Carolina. The agency has chosen to do more than the system has asked or requires, which is how the project earned the name Second Mile. The proj-ect was developed by Cindy Ehlers, director of clini-cal operations at ECBH LME. Its goal is to prevent people from being rehospitalized in state-operated psychiatric facilities and to support them in transi-tioning successfully back to the community after a hospitalization.
The Second Mile project is off to a great start at Cherry Hospital, a state psychiatric hospital in Goldsboro, thanks in part to the support of LME hospital liaisons and Cherry Hospital employees. Second Mile provides early intervention through
trauma reducing alternative crisis services, such as mobile crisis services, crisis respite centers, and transitional apartments. The project has also pur-chased local hospital psychiatric beds in its nine counties to provide an alternative to state psychiat-ric hospitalization.
The implementation of Second Mile at Cherry Hospi-tal begins when clients are introduced to hope and recovery through the Wellness Recovery Action Plan classes. These classes are led by ECBH LME’s cer-tified peer support specialists, who are also certi-fied WRAP facilitators. WRAP classes promote client awareness that mental health recovery is possible and give people hope that they can take personal responsibility, educate themselves, learn to be self-advocates, and get connected with support systems. Participants develop an individualized plan for stay-ing well, a crisis plan, and a postcrisis plan. WRAP was developed by researcher Mary Ellen Copeland as the result of her own personal search for well-ness.
A considerable body of evidence suggests that peer support and WRAP are effective when included at various stages of a comprehensive service system. These interventions can, for example, reduce the length of inpatient hospital stays, readmission rates, and trauma. Peer support specialists can facilitate access to other necessary mental health and sub-stance abuse services and natural and community support systems.
During a typical month, peer support specialists fa-cilitate WRAP classes weekly in the treatment mall. The goal is for patients to have completed WRAP classes by the time they are discharged from the hospital and have formed an in-depth crisis plan to maintain wellness and avoid rehospitalization. Once a client has completed WRAP and leaves the hos-pital, he or she is able to select a provider from a list that includes those who are trained in recovery. WRAP can then be incorporated into the client’s in-dividual recovery plan.
ECBH LME has developed surveys to measure re-covery variables such as hope, support, education, employment, and stable housing before and after participants take a WRAP class. Follow-up surveys will be conducted after discharge, and readmission rates after hospitalization will also be tracked. ECBH LME hopes to find an aggregate reduction in the use of state hospital bed days, increased use of trauma-reducing alternative crisis services, and successful discharge planning. Prevention and early interven-tion are seen as successful when a discharged per-son is not readmitted within 90 days and lives in the community with links to effective community-based services and natural supports.
ECBH LME will continuously evaluate the effective-ness of the Second Mile project through the data that are being generated. The goal is to replicate this model in other state-operated psychiatric facili-ties in North Carolina.
lisa Bonnett, Ms, Executive Director of Recovery f BS, Recovery Educator and Trainer — East Carolina Behavioral Health Local Management Entity, New Bern, NC / [email protected]
Second Mile Offers Peer Support to Prevent Rehospitalization
management curriculum that is based on estab-lished guidelines to use with consumers who cannot receive locally available DSME or medical nutrition therapy services.
Because diabetes is a common condition among people with serious mental illness, a central pro-gram goal is to facilitate coordination of care. CMT provides primary care case managers and mental health case managers who have educational cross-training on the unique characteristics and problems encountered by diabetic consumers who also suffer
from schizophrenia or other mental illnesses.
According to Dr. Joe Parks, “We anticipate that by increasing early-stage disease identification and providing the necessary education for successful self-management through the CMHCs, this program will ultimately improve the quality of life for those with SMI while simultaneously conserving health-care dollars through prevention-focused interven-tions. Supporting wellness in Missouri consumers is necessary if they are to achieve recovery from their mental illness.”
REfEREncESByrd, J., Parks, J., Oestreich, G., Surles, R., Docherty, J., & Simpson, K. (2005). The identification of schizophrenic consumers at risk for high future healthcare costs. Poster presented at the 57th meeting of the American Psychiatric Association Institute on Psychiatric Services.
Dixon, L. B., Kreyenbuhl, J. A., Dickerson, F. B., Donner, T. W., Brown, C. H., Wolheiter, K., et al. (2004). A comparison of Type 2 diabetes outcomes among persons with and without severe mental illness. Psychiatric Services, 55, 892−900.
Nasrallah, H. A., Meyer, J. M., Goff, D. C., McEvoy, J. P., Davis, S. M., Stroup, T. S., et al. (2006). Low rates of treatment for hypertension, dyslipidemia and diabetes in schizophrenia: Data from the CATIE schizophrenia trial sample at baseline. Schizophrenia Research, 86, 15−22.
NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 49
O n January 16, 2009, the incarcerated population in Kansas was 8,483 the lowest it had been since
2001. At the same time, 5,902 offenders were under parole supervision almost 2,000 more than in 2001. To date, revocation to prison from parole supervision has declined by 51% since FY 2003. The number of felony convictions for crimes committed by offenders while under parole supervision saw a 35% decline from 1990 to 2007.
The success reflected by these statistics is the result of the Kansas Department of Corrections’ shift to a philosophy of reentry and risk reduction within the agency and the department’s active collaboration with state and local partners to effect system wide change and enhance public safety.
The vision statement of the Kansas Department of Corrections is “a safer Kansas through effective cor-rectional services.” The Statewide Risk Reduction Ini-tiative has provided community corrections agencies with the additional resources and knowledge they need to better meet the mental health and substance abuse needs of probationers.
The work done in Kansas with offenders who were released from incarceration to community supervi-sion paved the way for the passage, in 2007, of State Senate Bill 14, which kicked off the Community Cor-rections Statewide Risk Reduction Initiative. This leg-islation expanded reentry and risk reduction beyond
post incarceration supervision into local intensive supervised probation agencies, with the goals of in-creased public safety, reduced risk level of probation-ers who are on community corrections supervision, and increased successful completion of supervision. Four million dollars was appropriated for commu-nity corrections agencies to implement or enhance evidence-based risk reduction efforts to work toward these goals.
The results of this effort are already being realized. Between FY 2006 and 2008, revocations of offenders from community corrections supervision to incarcera-tion decreased by 21.9%, and the percentage of suc-cessful completions increased by 26.2%.
Agencies funded under this initiative have committed to building a system to promote probationer success by targeting the evidence-based factors (e.g., mental health and substance use difficulties) that research shows, increase the risk that offenders will engage in criminal behavior.
Community stakeholder participation and appropri-ate targeting of resources to individual client needs are critical to the ambitious goals of this initiative. Mental health and substance abuse professionals are key collaborative partners in building a system to address the needs of clients involved with both the correctional system and mental health or substance abuse treatment.
Community corrections program design is specific to local probationers’ needs and court procedures; therefore, strategies to address the needs of proba-tioners who are mentally ill or substance abusing vary widely. For example, Northwest Kansas Community Corrections, a rural agency that serves 17 counties, contracts with a psychologist to provide mental health evaluations, individual treatment, close monitoring of treatment and interventions, and anger management groups to probationers. This arrangement is effective for the agency in part because the provider travels to meet the needs of clients across 16,194 square miles.
The Fifth Judicial District Community Corrections agency, which serves two counties and 1,627 square miles, has a full-time substance abuse counselor from the Mental Health Center of East Central Kansas. The counselor (who has offices in both the agency and the mental health center) works primarily with juvenile of-fenders but provides interim crisis intervention servic-es, substance abuse evaluations, and some individual substance abuse counseling for adult offenders.
The Risk Reduction Initiative provides targeted train-ing for officers on topics such as collaborative case planning and client advocacy. Training and technical assistance are ongoing at the agency, stakeholder, and system levels in the design of collaborative risk reduction initiatives.
J ust booked into the Cass County Jail in North Dako-ta, the detainee began licking the floor and exhibit-
ing other odd behaviors. Corrections officers see it all, it seems, and they suspected this prisoner was more than a typical DUI case. The in-house clinical mental health coordinator, whose position is funded by a U.S. Department of Justice grant, was called to the book-
ing area to conduct an assessment. Tests showed no alcohol or substance use to account for the psychosis the detainee was suffering. A representative of South-east Human Service Center arrived in 15 minutes to facilitate the detainee’s admission to the state hospi-tal, and within half a day, the young man was trans-ported from the jail to a facility equipped to provide
the treatment he clearly needed. Charges against him were dropped.
The young man’s family reported that they had taken him to an emergency room three times in the month before his arrest, but the hospital refused to admit him. Sometimes, early intervention for a serious men-tal illness falls on the shoulders of law enforcement,
tina Waldron, Ma, Program Consultant II Community Corrections Services, Kansas Department of Corrections, Topeka, [email protected]
sheree spear, Grant Manager, Cass County Justice and Mental Health Collaboration Project, Cass County Sheriff’s Office, Fargo, [email protected]
Kansas Brings Incarcerated Back into the Community
Cass County Provides Alternatives to Incarceration

From The Field
50 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
and communities like Cass County have launched programs to ensure that people with undiagnosed mental illness are identified and linked to treat-ment, housing, case management, and medication monitoring.
The concept of providing an alternative to incar-ceration isn’t new. In the 1700s, Governor Fauquier of Williamsburg, Virginia, gained financial support from the colonial legislature for the first state hospi-tal specifically for people with mental illness, believ-ing that treatment should be provided rather than incarceration in the public jail. Recent advances in medicine and policy reforms have reshaped the landscape and call for programs designed to fit the new definition of alternative a life in the community and opportunities for employment. Yet, the alterna-tives are still inaccessible to many people who cycle in and out of county jails. Fortunately, today the field has evidence-based practices, a wealth of research, and even an instruction manual to guideg the de-velopment of programs such as the Cass County Justice and Mental Health Collaboration Project.
In 2004, following recommendations put forth by the Criminal Justice/Mental Health Consensus Proj-ect Report and the Center for Mental Health Servic-es’ National GAINS Center, the Cass County sheriff’s office brought together 26 people from community and state agencies to discuss the question, “How can we respond differently to reduce recidivism and improve outcomes for those with mental illness?”
The group the Cass County Jail Intervention Coordi-nating Committee researched programs, collected data, and decided to focus first on developing a jail-based post-booking strategy.
The JICC defined the target population to include people with psychotic or mood disorders who met specific offense criteria. Legal alternatives would be maximized, and services would be provided to qualified people who volunteered for the program. The committee identified gaps in services and de-veloped a programmatic strategy to address risk factors and quality-of-life issues for the target popu-lation. In particular, capacity expansion was needed in two key areas: a full-time clinical mental health coordinator at the jail, and a case manager.
The JICC collected data on how many detainees re-ceived a mental health assessment. Data revealed that in 2005, jail staff referred 191 detainees for a psychiatric assessment, but only 92 actually re-ceived one because of limited resources. JICC made it a goal to close the gap at this critical point. From January through May of 2009, 550 clients received an assessment by the new clinical mental health coordinator. Of those people, 373 were referred for treatment and services, and 10 were transported for inpatient hospitalization or evaluation.
A case manager is the critical link between a per-son with serious mental illness and the community-based services he or she needs. In Cass County,
although many clients are well served, others are placed on waiting lists because of treatment profes-sionals’ heavy caseloads. Grant funding has been dedicated to hiring an additional case manager to help clients establish personal goals and remain engaged with treatment while on the waiting list.
Cass County’s interventions are helping to provide alternatives to incarceration through early identifica-tion.
T he Allegheny County Department of Human Ser-vices’ Office of Behavioral Health, Community
Care Behavioral Health, and Western Psychiatric In-stitute and Clinic of UPMC, all based in Pittsburgh, PA., partnered to create the re:solve Crisis Network. The inception of this network marked a shift from dispersed crisis services that operated across the
county to a coordinated crisis continuum under one provider. Informed by consumer and community in-put, the project’s goal was to unify services, enhance continuity of care, streamline access to services, and clarify performance expectations.
Programming includes telephone, mobile, walk-in, and residential services; as well as assessment,
counseling, referral, and linkages. This continuum is intended to preserve community tenure through in-creased access and service utilization for all county residents (including people who have not previously engaged in behavioral health services) and focuses on prevention and early intervention. Existing litera-ture supports the effectiveness of crisis intervention
eleanor Medved, rn, Msn, Vice President of Ambulatory and Crisis Operations; Frank ghinassi, Phd, Vice President of Quality and Performance Improvement; and Jewel denne, Med, lPc, Clinical Administrator — re:solve Crisis Network; rodney Williams, Md, Medical Director, re:solve Crisis Network and Western Psychiatric Institute and Clinic of UPMC, Pittsburgh, PA; Jill trainor, Communications Manager in Clinical Marketing, UPMC, Pittsburgh, PA; Mary Jo dickson, Administrator, Bureau of Adult Mental Health Services, Allegheny County Office of Behavioral Health, Pittsburgh, PA; debbie duch, MPh, Program Manager, Allegheny HealthChoices, Community Care Behavioral Health, Pittsburgh, PA / [email protected]
Re:solve Markets Crisis Preparation
sometimes, early intervention for a serious mental illness falls on the shoulders of law enforcement, and communities like cass county have launched programs to ensure that people with undiagnosed mental illness are identified and linked to treatment, housing, case manage-ment, and medication monitoring.

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 51
in prevention and early intervention in terms of im-proved user outcomes and as a cost-effective alter-native to hospitalization for many clients (Jackson, 2005; Ontario Ministry of Health and Long-Term Care, 2005; Robin, Bronchard, & Kannas, 2008; Rosen, 1997; Scott, 2000).
Marketing and outreach efforts were incorporated into the development of a program that transformed the continuum from a multiprovider to a single-provider entity while supporting its person-centered mission and vision. Critical input was collected from consumers, families, and other stakeholders through meetings, surveys, and focus groups.
The program’s name (re:solve Crisis Network) and phone number (1.888.7.YOU.CAN) were chosen to work in tandem to instill confidence and hope and to communicate that problem resolution can be driven by the person in crisis (“You can resolve a crisis”). Early intervention is supported by the advertising message, which begins with the headline “Call before a crisis becomes a crisis” and subsequent tagline “We’re here for you any time, any day, for any reason,” which communicates that the program is accessible 24 hours a day, 365 days a year.
re:solve Crisis Network’s branding includes consistent use of logo, color treatment, and graphic illustrations to support the program’s message. Color is used to acknowledge the tension of crisis, and common sce-narios are used to depict distress (as a precursor to or proxy for crisis) in a nonthreatening, accessible fash-
ion to a diverse, all-county demographic. Although the following list summarizes people’s general identifica-tion with specific graphics, individual interpretations of and responses to the “meaning” of the graphics have been highly variable:
>> Broken plate (represents loss, distress, emotion)
>> Torn family photo (represents relationship or family conflict)
>> Overflowing laundry (represents an overwhelming home life)
>> Poor test results (represents performance or school issues)
>> Overflowing “in−out basket” (represents work problems).
The program uses a variety of marketing campaign tactics to reach the diverse target audience, such as direct mailers (sent to every household in the area served); outdoor advertising (e.g., billboards); transit advertising; ads on radio, newspapers, and in the yellow pages; Internet presence (www.upmc.com/re-solvecrisis); collateral advertising (e.g., displays, mag-nets, pocket cards, key chains), and public relations.
Concurrent with the marketing launch, a comprehen-sive face-to-face outreach initiative was implemented. Scores of meetings and informational sessions have been held with stakeholder groups, including con-sumers, families, community members, government officials, behavioral health professionals, social
service and support professionals, advocates, law enforcement officials, hotline operators, peer service providers, hospital and emergency room profession-als, school employees, providers of services to the homeless, spiritual and religious communities, disas-ter response professionals, youth and aging profes-sionals, emergency medical service providers, and physicians. Many of these sessions have resulted in standing collaborative meetings that provide ongoing performance feedback to re:solve Crisis Network.
Recently, an older gentleman contacted the crisis line because of significant personal and health losses and said that he had received the re:solve Crisis Network postcard but had not previously used behavioral health services. He engaged in dialogue and ultimately accepted community linkages and services that he was not aware were available to him.
Efforts since the program opening in July 2008 have yielded dramatic improvements in the community’s perception of the service. Prevention and early inter-vention are now seen as the hallmarks of the new crisis continuum. Two indicators have been used to measure the desired outcomes: frequency of telephone calls and frequency of mobile crisis visits. Since the imple-mentation of re:solve Crisis Network and marketing and outreach efforts, community engagement in crisis services has significantly increased. Telephone calls have increased by 2,761 per month (34%), and mobile crisis visits have increased by 362 per month (140%).
REfEREncES
Jackson, E. (2005). A community-based comprehensive psychi-atric crisis response service: An informational and instructional monograph. Boston: Technical Assistance Collaborative.
Ontario Ministry of Health and Long-Term Care. (2005). Crisis response service standards for mental health services and sup-ports. Retrieved from www.health.gov.on.ca/english/public/pub/ministry_reports/mentalhealth/cris_resp.pdf
Robin, M., Bronchard, M., & Kannas, S. (2008). Ambulatory care provision versus first admission to psychiatric hospital: Five years follow up. Social Psychiatry and Psychiatric Epidemiology, 43, 498−506.
Rosen, A. (1997). Crisis management in the community. Medical Journal of Australia, 167, 633−638.
Scott, R. L. (2000). Evaluation of a mobile crisis program: Effectiveness, efficiency, and consumer satisfaction. Psychiatric Services, 51, 1153−1156.
The inception of the re:solve Crisis Network
marked a shift from dispersed crisis services that operated across the county to a coordinated crisis continuum under one provider.

52 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Targeting High-Risk Populations
hoPe for homeless Youth and Families
nisha Beharie, MPh, Program Coordinator, Mary McKay, Phd., Professor of Psychiatry & Community Medicine, Kosta Kalogerogiannis, lMsW, Community Collaborative Board — Mount Sinai School of Medicine, Department of Psychiatry
I t has been estimated that as many as 12 to 26 million adults have experienced at least one pe-
riod of homelessness over their lifetime, with up to 6 million adults being homeless annually. Homeless families constitute a significant proportion of the homeless population nationally. In 1995, the U.S. Department of Education estimated that 744,000 school age children and adolescents were home-less during the course of one school year. This esti-mate had increased to one million youth in 2002. Approximately 87% of homeless youth are enrolled in school, but only 77% attend school regularly. The rates of homelessness in New York are equally staggering. Most recently, due to the current reces-sion, the number of families entering New York City homeless shelters increased by 40% from 2007 to 2008 alone.
While the current economic situation has made homelessness among families a more pressing issue, the factors that contribute to a family experiencing homelessness are myriad and complex. At the most basic level, homelessness has been described as a direct result of poverty, inadequate employment
opportunities and welfare benefits, particularly for single women and their children, and lack of afford-able housing. Yet, homeless families often simulta-neously experience an expanded range of difficul-ties that increases their vulnerability to losing their housing and being less able to compete for scarce housing resources and employment. These factors include parental alcohol or other drug-related prob-lems, mental illness, serious histories of childhood abuse and domestic violence, unemployment and poor health. The same set of factors that place families at risk for losing their housing also serve to disrupt parenting and family relationships, thereby placing youth at substantial risk for engaging in a range of problematic behaviors, including early and risky sexual behavior and drug abuse.
Furthermore, adolescent youth may be more im-pacted by homelessness in comparison to younger children as a result of their cognitive capacities that allow for increased awareness of family circum-stances, experiences of stigma related to homeless-ness, and the effects of disruptions that moving into the shelter system creates on peer relations and
school placement. Adolescence covers a large age range, beginning as young as 9 or 10 and lasting to 18 to 24 years of age. Throughout this period, youth are moving between the worlds of childhood and adulthood, experiencing multiple new and stressful challenges. As children move through adolescence toward adulthood, they have basic developmental and psychosocial needs, including being valued as a member of a group, receiving family support, participating in caring relationships, acquiring skills to cope adaptively with everyday life, and believing in a future with real opportunities. Youth who enter this period under adverse circumstances are often ill-prepared to effectively cope with these normative challenges, making this period particularly prob-lematic and potentially associated with high rates of school dropout, early and risky sexual behavior, pregnancy, drug abuse, and suicide. In particular, the experience of homelessness, compounded by residential flux, disruption in schooling, and the stigma associated with homelessness provides a highly stressful context for youth development. In fact, there is a growing body of research that docu-ments the negative impact of homelessness on chil-

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 53
dren’s health, mental health and overall development, which in turn places them at higher risk for engaging in early, high risk sexual activity and drug abuse.
Thus, drug abuse and HIV- focused prevention pro-grams targeting homeless youth must be multi-level and address the needs of the youth for information and skills development. In addition, family-based pro-grams must reduce adult caregivers’ risk behaviors and support and bolster protective family processes particularly in a shelter environment that can decrease parental control and increase contact between youth and peers and other adults using drugs and engaging in risky behaviors.
The Social Learning Theory is very helpful in inform-ing programming to change sexual risk behavior and drug use. Furthermore, recognizing the construct of self-efficacy within the premise of the Social Learning Theory is crucial to understanding human and collec-tive functioning as defined by Albert Bandura. Specific to “learning” protective factors to minimize risk of HIV, research findings have documented the wide-ranging effects of efficacy perceptions on learning and moti-vation. Self-efficacy theory predicts that highly effica-cious individuals will choose to participate in groups more often. They will also expend more effort on chal-lenging learning tasks and persist longer in the face of difficulty. HIV-risk reduction self-efficacy can be dem-onstrated through reinforcement of change efforts, providing opportunities to practice and successfully rehearse skills needed to implement behavior change, and real-life success in risk avoidance.
An example of use of this theoretical model is within urban communities is the HOPE (Homeless Outreach for Parents and Early Adolescents) Family Program.
HOPE was created by key stakeholders in an urban community to address the prevention needs of youth and families experiencing disruptions in housing. The development, delivery, and testing of the program were funded by the National Institute on Drug Abuse.
The curriculum for HOPE consists of eight family workshop sessions that focus on HIV/AIDS, sexually transmitted infections, and drug abuse while taking into account the context of youth and families ex-periencing disruptions in housing. Concepts such as self-efficacy and comfort surrounding health protec-tive sexual communication were also integrated into each workshop. The content of these sessions came from three evidence-based curriculums (CHAMP, Strengthening Families, and SISTA Partnership for the Homeless) and were adapted to meet the needs of the specific population being served.
This program was targeted to adolescent ages 11 to 14 and their care givers and was delivered in com-munity-based sites. Each session was divided into three parts: 1) group welcome (the caregivers and youth were together), 2) parents and youth groups (the caregivers and youth were separate), and 3) the family discussion (the caregivers and youth were together again). Sessions began with a warm-up pe-riod, which provided an opportunity for the families to connect with each other and to share updates about the previous topics and issues that had come up in their families since the previous group meeting. Each parent and youth group allowed the participants to discuss issues openly among their peers to increase the comfort level of the participants during this por-tion of the session.
Following the separate youth and caregiver groups,
the participants came together and were provided with activities for the family discussion to facilitate communication between the parents and youth and engage them in the session topic. During these activi-ties and discussions the caregivers and youth could identify and develop strategies to deal with the core topic of the session together. The family discussion also served as a wrap-up of the session and a means for the facilitators to introduce the next week’s topic.
The goals and content for each session are described below.
sessIon I — Introduction and Family communicationThis session served to introduce families to the HOPE Family Program staff and to each other while discuss-ing why the HOPE Family Program is in their com-munity. This session also focused on one of the main themes of the HOPE Family Program: family communi-cation. Families discussed the importance of commu-nication between youth and caregivers and practiced some methods of effective communication.
sessIon II — Monitoring and supervisionThis session focused on the importance of monitoring and supervising youth as a means to preventing risky behavior. Families discussed rules that currently exist in their home and how these rules change as youth get older. Youth were asked to discuss rules that are “hard to follow” and to also discuss their friendships and how some may help or not help with following rules. Families were also asked to role play scenarios with risky situations and develop alternatives to en-gaging in the high risk behavior.
sessIon III — self respect and Peer PressureIn this session, families discussed the effects of peer pressure on youth and its relation to self-esteem. The discussion focused on the connection between man-aging peer pressure and preventing risky behavior. Families discussed assertive, aggressive, and non-assertive communication when confronted with risky situations. The anticipated outcome was an increase in skills among youth to be able to discuss with their peers their decision to not partake in risky behaviors. Role-plays based on peer pressure scenarios were practiced.
Drug abuse and HIV-focused prevention programs targeting home-
less youth must address the needs of the youth for information
and skills development. Family-based programs must reduce adult
caregivers’ risk behaviors and support protective family processes,
particularly in a shelter environment that can decrease parental
control and increase contact between youth and peers and other
adults using drugs and engaging in risky behaviors.

54 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Targeting High-Risk Populations
sessIon IV — PubertyIn this session, families discussed puberty and its effects on youth and their families. Caregivers dis-cussed and practiced communicating with their youth about puberty. Youth discussed their knowl-edge of puberty while also receiving factual infor-mation. Parents and youth were given an opportu-nity to discuss puberty together and were provided with materials that would aid them in discussing puberty at home.
sessIon V — hIV/aIds/stIsThis session focused on increasing knowledge sur-rounding HIV/AIDS and STIs. Parents and youth were provided with facts surrounding HIV/AIDS, including transmission; myths surrounding transmission were discussed. Other major STIs were discussed with an emphasis on transmission and symptoms as well as reducing risk in high-risk situations. Male and female condom demonstrations were performed, and families had an opportunity to practice using a male condom.
sessIon VI — substance use This session focused on increasing knowledge around the negative effects of substance abuse. Facts on illicit substances were presented. Families learn about addiction and its relation to HIV/AIDS, and STI risk.
sessIon VII — domestic Violence and Intimate Partner ViolenceThis session focused on discussing domestic vio-lence. The signs and manifestations of domestic vio-lence and intimate partner violence were reviewed. Families discussed different ways of recognizing if one is in a domestic violence or IPV situation, as well as ways of leaving a domestic violence situa-tion. Facts on domestic violence and IPV were also presented.
sessIon VIII — hope Family gameThis session served as a review of the topics and information discussed in the previous HOPE Fam-ily Program sessions. Families participated in an interactive game in which they competed with one another while assessing their knowledge of the in-formation. Families also received certificates for their completion of the HOPE Family Program.
Thus far, HOPE has involved 223 parents and youth. High attendance in groups suggested that the com-munity educators were successful in engaging this high risk population. The need was highlighted for additional prevention programs that are sufficiently flexible to achieve high rates of participation and that can incorporate changes in residence and cir-cumstances of these families.
Nisha Beharie received her masters degree in Public Health from the Mailman School of Public Health at Columbia University. Ms. Beharie is a former Peace Corps volunteer who
has worked with underserved populations both internationally and domestically, in various capacities. At Mount Sinai School of Medicine, she has co-directed a NIDA funded grant entitled HIV/AIDS Outreach Program for Parents and Early Adolescents (HOPE) providing HIV/AIDS and alcohol abuse prevention education to families living in NYC family shelters.
Mary McKay is a professor of psychiatry and community medicine. Her interests include identifying the specific mental health and prevention needs of urban youth and their families, as well as testing family and community-based, collaboratively developed interventions.
Kosta Kalogerogiannis is a doctoral student at the Columbia University School of Social Work and an NIMH research fellow with the Council on Social Work Education Underrepresented Mental Health Research Fellowship Program. She has worked in NYC’s inner-city communities for the past decade and has been involved in a range of clinical and research interventions aimed at reducing adolescent and adult risk in the areas of sexual health and mental health.
Acknowledgments: HOPE is supported by National Institute of Drug Abuse (RO1 DA018574). We thank the entire HOPE Family Committee for their tireless efforts. Ervin Torres, Angela Paulino, Ana Miranda, Aida Ortiz, Anita Rivera-Rodríguez, Rhina Paulino, Jason Patrick, Kerby Jean, and Jovan Jones as well as others who worked on the program, Rita Lawrence, Indamora Castro, Natalie Parker, Greg Mudd, Mary Savva, and Nealdow Chambers.
HOPE (Homeless Outreach for
Parents and Early Adolescents)
Family Program was created by key
stakeholders in an urban community
to address the prevention needs of
youth and families experiencing
disruptions in housing.
The development, delivery, and
testing of the program were
funded by the National
Institute on Drug Abuse.
> Quality & compliance best practices
> Regulatory changes
> Enforcement & oversight updates
Compliance WatchA behAviorAl heAlth exclusive
QuArterly Newslettersubscribe at https://store.thenationalcouncil.org

Call Richard Willetts P. 800-970-9778 x 225 * F. 610-941-9889
Plan for the best...prepare for the worst! You can’t always see trouble coming...
Coverages Include: Abuse Liability Automobile Umbrella
We offer an EXCLUSIVE Insurance Program for the Behavioral Healthcare Industry
Property Crime General Liability Professional Liability including Physicians & Psychiatrist

56 / NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2
Targeting High-Risk Populations
InSHAPE: Promoting Wellness, Saving Lives
P eople with severe and relentless mental illness such as schizophrenia and bipolar disorder also
bear a greater physical burden; they are at increased risk for obesity and chronic diseases including diabe-tes, hypertension, cardiovascular disease, and nicotine
dependence. Serious mental illness is an important risk factor for morbidity and morality; these patients die an average of 25 years earlier than the average individual due to higher rates of medical illness than can lead to premature mortality.1
These gloomy statistics inspired Ken Jue, MSW, CEO of Monadnock Family Services in Keene, New Hampshire to start the In SHAPE program. “What we’re trying to do is prevent premature death of persons with serious mental illness,” says Jue.
Research shows that people with schizophrenia and other psychotic and mood disorders who exercise three times a week for approximately 4 months lose weight, gain cardiovascular fitness, and experience less depression and fewer psychiatric symptoms.2 But few programs exist to help people with SMI maintain healthier lifestyles; for example, fewer than 20% of peo-ple with schizophrenia engage in regular exercise, and approximately 40% are completely inactive.3 In SHAPE is one of the few wellness and prevention program for individuals with SMI that seeks to fill this void.
In SHAPE seeks to improve physical health and quality of life, reduce the risk of preventable diseases, and enhance life expectancy of individuals with SMI. Each participant is teamed up with a trained health mentor to create a Self Health Action Plan for Empowerment (SHAPE) that includes physical activity, healthy eating goals, and attention to medical needs. The program enrolls adults in community wellness activities such as exercise, dance classes, weight loss programs, and smoking cessation activities.
Until 2002, Jue continued to attend a number of funer-als of his patients that seemed far too young to be dy-ing. He often looked at his patients’ photographs and noticed that they all looked youthful and active at one
time in their lives. Jue started researching information about comorbid medical illnesses among people with SMI and also interviewed Monadnock staff about pa-tients’ medical conditions. Staff members confirmed that many of their patients had died prematurely or
had a number of other chronic health conditions exac-erbated by their lifestyle choices and their mental ill-ness.4 Jue knew something had to be done to help this unique population, and so he outlined key program elements that he would want to see in a program that helped people with SMI improve their physical health.
Instead of relying on formal referrals from mental health providers, Monadnock encouraged voluntary participation and began to form partnerships with hospitals and organizations that would provide exer-cise, nutrition, and general health services. These part-nerships were critical to In SHAPE’s success. The local hospital provided smoking cessation programs, while a large non-profit medical clinic provided primary care services to participants without a medical home at no charge to the patient. The local YMCA and a dance and fitness center also offered up their services to en-courage creative forms of physical activity. Graduates from Keene State College Department of Health and Fitness were hired to serve as health mentors. They did
not receive formal mental health training so that they would not be influenced to think about and treat the participants as “ill” or “sick” patients.5
Participants were not only given the chance to be edu-cated on leading a healthy lifestyle, but they were also given the opportunity to meet other people with similar challenges and to feel included in the community. Fit-ness assessments were repeated every three months to track progress, and there were regular celebrations during which participants received recognition for their efforts and incentive prizes.
A pilot study was launched with the commencement of the In SHAPE program to gauge participants’ progress in improving their overall health. While Jue only expected 40 people to enroll in the program, he was surprised to see that 65 people had signed up, and more wanted to join but couldn’t due to limited funding. Three months after beginning the program, participants exhibited increased exercise capacity and flexibility, enhanced readiness to change, and improved mental well-being; weight loss was variable across participants. Anecdotal evidence suggests that participants seemed to have greater confidence in social situations, reduction in their waist circumference and blood pressure, and an overall reduction in their depressive symptoms.6 While In SHAPE does not promote exercise as a replacement for pharmacotherapy, preliminary results suggest that the exercise and increased health awareness help pa-tients better cope with their mental illness.
Ken Jue, MsW, CEO, Monadnock Family Services in an interview with laura galbreath, Director of Policy and Advocacy, National Council for Community Behavioral Healthcare
InSHAPE won the National Council’s 2008 Award for Excellence in Innovation
27 -year-old “ Matt” described himself as “A heart attack waiting to happen.” He weighed more than 300 pounds and smoked two packs a day. Diagnosed with bipolar disorder in his senior year in
high school, Matt had been hospitalized twice. During one six week stay, he gained 25 pounds. Matt’s weight had wildly fluctuated before. As a college freshman suffering from depression, he lost 119 pounds on only cigarettes and diet soft drinks.
Matt joined Monadnock’s InSHAPE program, which offered him the services of a personal trainer to focus on health and nutrition. A year after joining the program, Matt looks at diet and exercise differently, and excels in the cooking class. He has learned how to judge the nutritional values of foods by reading the information on the packaging.
He’s also gained self-esteem through his athletic success, particularly in tennis, and gained perspective on his mental illness. “Now I don’t view myself as Matt with this major mental illness. It’s a component of me but not me. I try not to make it forefront of my entire being.”
A true story from Monadnock Family Services, Keene, New Hampshire
While InshaPe does not promote exercise as a replacement for pharmaco-therapy, preliminary results suggest that the exercise and increased health awareness help patients better cope with their mental illness.

NATIONAL COUNCIL MAGAZINE • 2009, ISSUE 2 / 57
Currently, the In SHAPE program is active in New Hamp-shire, Massachusetts, and Maine. Jue and his team at Monadnock have strengthened In SHAPE by developing new programs that help address challenges that come with varying populations with SMI. For example, Parents as Teachers is a new initiative developed for mothers with mental illness on Medicaid. Through home visits, mothers are taught on how to grow and develop rela-tionships with their children with greater continuity and less disruption as a result of their mental illness. While the program presents its own challenges for the mothers involved, most participants are deeply committed to the one-year program and strive to make significant changes for themselves and their families.
Jue encourages other associations to support wellness and build partnerships with their local healthcare clinics and organizations with a few caveats7:
>> Do not underestimate the insight of people with mental illness: Patients with SMI are likely to readily acknowledge the need to make lifestyle changes to improve their health.
>> Emphasize local inclusion: Involving people with SMI in community activities and exercise centers will ulti-
mately improve their quality of life and reduce local stigma.
>> Seek community partnerships: Programs don’t need to have their own exercise centers or nutrition staff; they should leverage use of community resources by creating mutually beneficial partnerships.
>> Employ a patient centered approach: Encouraging participants to set their own goals will increase the likelihood that goals will be achieved. Participants should understand that they have responsibility for and control of their health.
>> Do not “medicalize” the program: Orient the pro-gram as an activity to promote the participant’s health and wellness, not as a response to his or her mental illness or medical comorbidities.
Funding for the In SHAPE program initially came from the New Hampshire Endowment for Health. The Robert Wood Johnson Foundation also provided monies for program expansion and a pilot study to test the effectiveness of the program. Enrolled patients also pay a $5 monthly membership fee to access exercise facilities and classes offered by In SHAPE partners. Recently, the state of New Hampshire agreed to reimburse the In SHAPE program
under the state’s Medicaid program.
REfEREncES1. Shiner B, Whitley R, Van Citters AD, et al. Learning what matters for patients: qualitative evaluation of a health promotion program for those with serious mental illness. Health Promotion Int. 2008 Sep; 23(3): 275-82.
2. Exercise and Nutrition Program Helps Individuals with Serious Mental Illness Develop Healthier Lifestyles, Improves Fitness, and Mental Well-Being Retrieved July 21, 2009, from http://www.innovations.ahrq.gov/content.aspx?id=2444.
3. ibid 4. ibid 5. ibid 6. ibid 7. ibid
As CEO of Monadnock Family Services Ken Jue has instituted many new and innovative programs and services, including New Hampshire’s only organized mental health court, a consumer-directed housing cooperative, a consumer and family directed fund to support consumer initiatives toward independence, and an interagency supported dental practice for consumers. Jue has consulted with international government agencies and nonprofits on public mental health and welfare services and has presented at national and international conferences. He is active in community volunteer activities and has held elected office.
Laura Galbreath supports the National Council’s state and federal policy initiatives and focuses on expanding opportunities for 1,600 member community mental health and addictions services organizations to meet the primary health needs of the people they serve. Galbreath has extensive experience in health policy analysis, community organizing, and project management. Before coming to the National Council, she served as the senior director of healthcare reform at Mental Health America.
Mental Health Risk Retention Group, Inc.
Negley Associates • P.O. Box 206 • Cedar Grove, NJ 07009
(800) 845-1209 • Fax: (973) 239-6241 Email: [email protected] • www.mhrrg.com
The Benefits of Ownership…
As an insured of MHRRG you actually: • Own your insurance company .• Receive the financial benefit of a dividend opportunity.• Your board of directors is comprised of your peers,
giving you direct access to decision making.
You can relax, we’ve got you covered.

The Cost Effective Way to Connect with Your Stakeholders
Essential Learning’s Community Access Site
www.EssentialLearning.com
The Community Access Site (CAS) is a web-based information and public education resource for consumers, family members and community stakeholders served by state and county mental health authorities, provider organizations and provider networks.
Fulfill your mission - provide information to your community and empower your consumers in their recovery
• Community Education - free courses• Links to community/national resources• WRAP® Information Center• Social networking • Build relationships and connect with donors
Affordable subscription pricingFor more information visit www.essentiallearning.com
1-800-729-9198 ext 284 • [email protected]
June_rush2b.indd 1 6/5/09 3:09 PM

Send us your submissions August – September, 2009Awards presented during Conference Gala in Walt Disney World® Resort, Florida, March 15–17, 2010
The industry’s most prestigious awards recognizing innovative programs and outstanding leadership in mental health and addictions
www.TheNationalCouncil.org (click on Membership and then Awards of Excellence).
AwArds of
ExcEllEncE
I n s p I r A t I o n I n n o v A t I o n I n f l u E n c E
Questions? Contact [email protected] or call 202.684.7457.