Embed Size (px)
Citation preview

DR MOHAMMAD A.S KAMIL
CONSULTANT NEUROLOGIST
NEUROSCIENCES HOSPITAL

• MYOPATHIES ARE A HETEROGENEOUS GROUP OF DISORDERS THAT CAN BE
CHALLENGING TO DIAGNOSE.
• THE PURPOSE OF THIS REVIEW IS TO PROVIDE A DIAGNOSTIC APPROACH BASED
PREDOMINANTLY ON THE CLINICAL HISTORY AND NEUROLOGIC EXAMINATION.
• IN APPROACHING THE EVALUATION OF A PATIENT WITH A SUSPECTED
MYOPATHY, ONE OF THE MOST IMPORTANT COMPONENTS IS A COMPREHENSIVE
MEDICAL HISTORY.

MYOPATHIES ARE DISORDERS AFFECTING
channel
structure
Metabolism
of skeletal
muscle
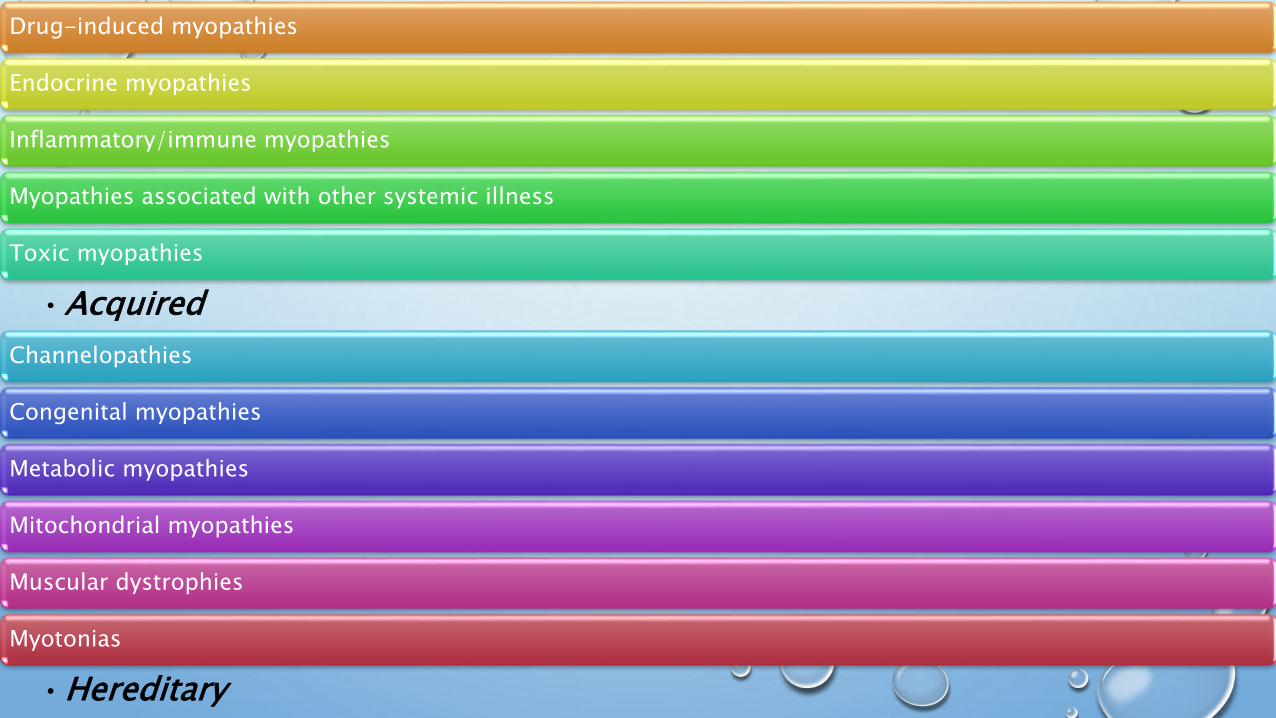
Drug-induced myopathies
Endocrine myopathies
Inflammatory/immune myopathies
Myopathies associated with other systemic illness
Toxic myopathies
•Acquired
Channelopathies
Congenital myopathies
Metabolic myopathies
Mitochondrial myopathies
Muscular dystrophies
Myotonias
•Hereditary

Which ‘‘positive’’ and/or ‘‘negative’’ symptoms does the patient experience?
What is the temporal evolution (presentation,episodic,constant,acute)
Does the patient have a family history of a myopathic disorder?
Are there precipitating factors that trigger episodic weakness or stiffness (drugs,exercise,fever,high carbohydrate,cold)
Are any associated systemic symptoms or signs present (cardiac,respiratory,hepatomegaly,cataract,rash)
What is the distribution of weakness?

SYMPTOMS ASSOCIATEDWITH MYOPATHIESA
Negative
•Exercise intolerance
•Fatigue
•Muscle atrophy
•Weakness
Positive
•Cramps
•Contractures
•Muscle hypertrophy
•Myalgia
•Myoglobinuria
•Stiffness

MUSCLE DISEASES ASSOCIATED WITH MYALGIASEosinophilia-myalgia syndrome
Hypothyroid myopathy
Inflammatory myopathies (dermatomyositis, polymyositis)
Infectious myositis (especially viral)
Mitochondrial myopathies
Myoadenylate deaminase deficiency
Toxic myopathies (statins, chloroquine)
Tubular aggregate myopathyX-linked myalgia and cramps (Becker dystrophy
variant)

MYOPATHIES ASSOCIATED WITH MUSCLE CONTRACTURES
Brody disease
Glycolytic/glycogenolytic enzyme defects
Hypothyroid myopathy
Paramyotonia congenita
Rippling muscle disease

MYOPATHIESASSOCIATED WITH MUSCLE STIFFNESS
Hyperkalemic periodic paralysis
Hypothyroid myopathy
Myotonia congenita
Myotonic dystrophy
Paramyotonia congenita
Proximal myotonic myopathy
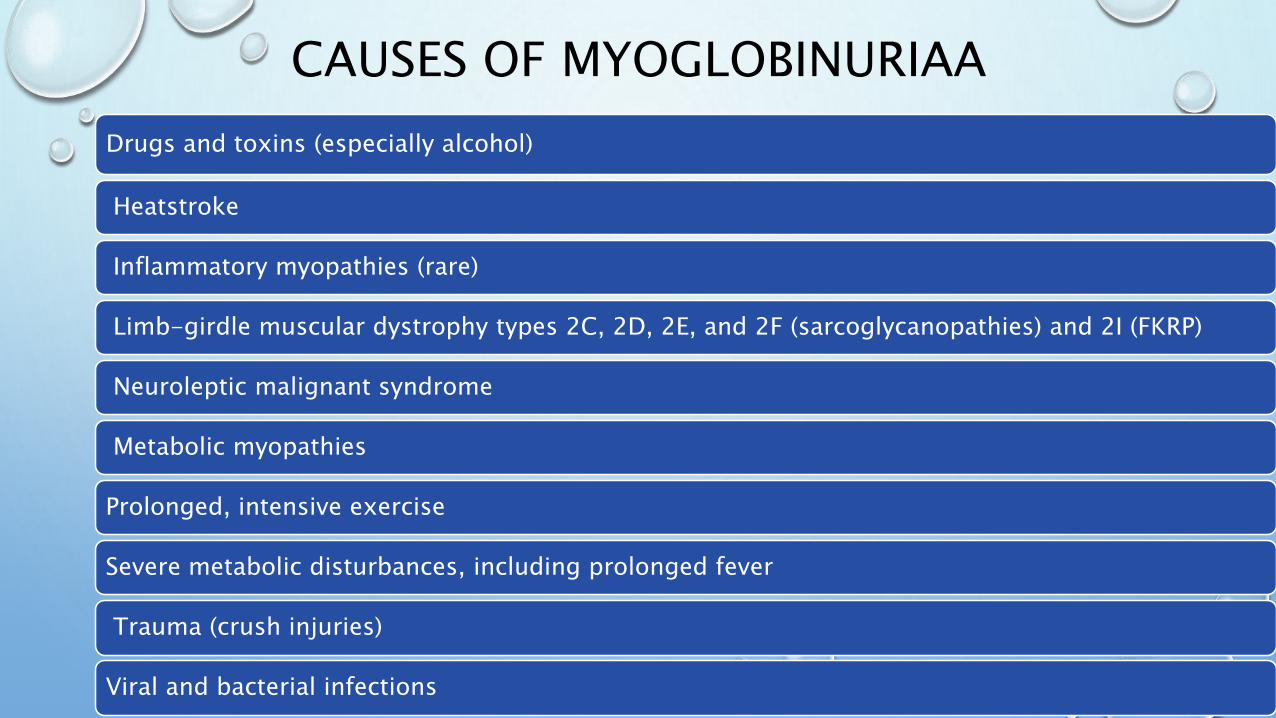
CAUSES OF MYOGLOBINURIAA
Drugs and toxins (especially alcohol)
Heatstroke
Inflammatory myopathies (rare)
Limb-girdle muscular dystrophy types 2C, 2D, 2E, and 2F (sarcoglycanopathies) and 2I (FKRP)
Neuroleptic malignant syndrome
Metabolic myopathies
Prolonged, intensive exercise
Severe metabolic disturbances, including prolonged fever
Trauma (crush injuries)
Viral and bacterial infections

DRUGS THAT CAN CAUSE TOXICMYOPATHIES
Inflammatory
• Cimetidine
• D-penicillamine
• Procainamide
• L-tryptophan
• Levodopa
Non inflammatory
Necrotizing or
Vacuolar
• Alcohol
• Cholesterol-lowering
agents
• Chloroquine
• Colchicine
• Cyclosporine and
tacrolimus
• Emetine
• (-aminocaproic acid
• Isoretinoic acid
(vitamin A analogue)
• Labetalol
• Vincristine
Rhabdomyolysis and
Myoglobinuria
• Alcohol
• Amphetamine
• Cholesterol-lowering
drugs
• Cocaine
• Heroin
• Toluene
• (-aminocaproic acid
Myosin Loss
• Non depolarizing
neuromuscular
blocking agents
• Steroid
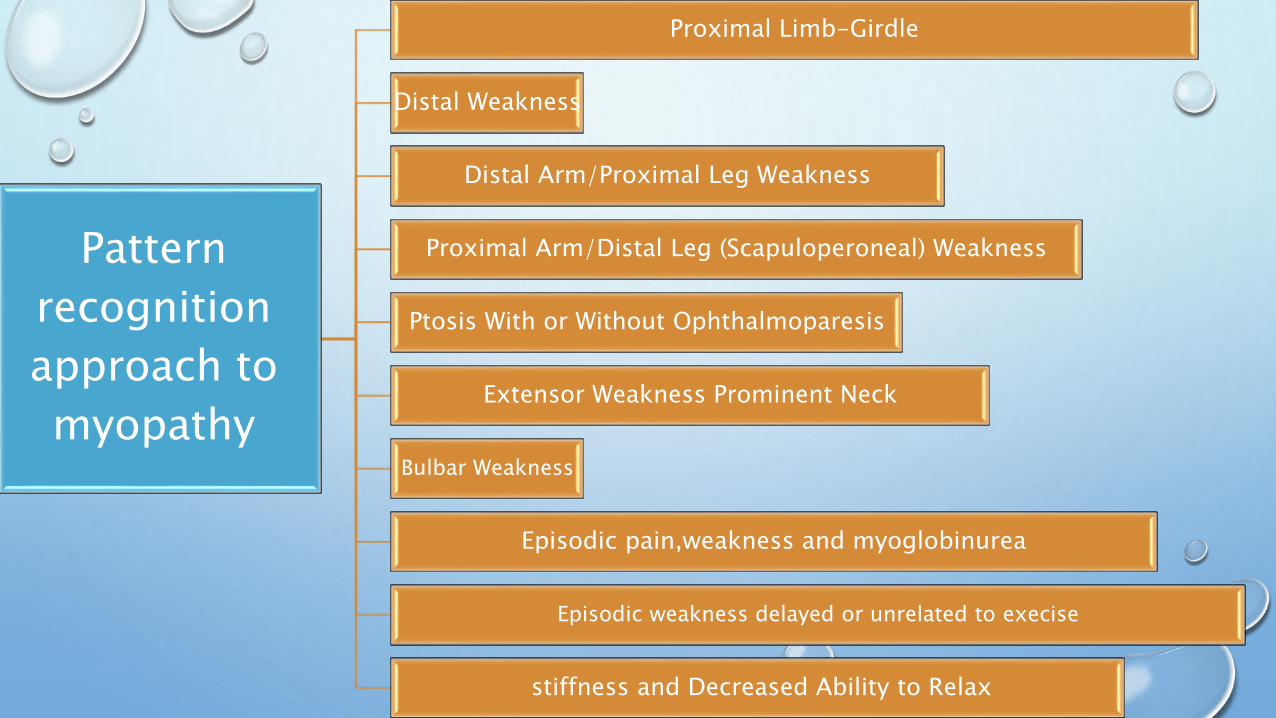
Pattern
recognition
approach to
myopathy
Proximal Limb-Girdle
Distal Weakness
Distal Arm/Proximal Leg Weakness
Proximal Arm/Distal Leg (Scapuloperoneal) Weakness
Ptosis With or Without Ophthalmoparesis
Extensor Weakness Prominent Neck
Bulbar Weakness
Episodic pain,weakness and myoglobinurea
Episodic weakness delayed or unrelated to execise
stiffness and Decreased Ability to Relax

MYOPATHIESCHARACTERIZED BY PREDOMINANTLY DISTAL
WEAKNESS
Centronuclear myopathy
Debrancher deficiency
Hereditary inclusion body myopathy
Inclusion body myositis
Myofibrillar myopathy
Myotonic dystrophy
Distal myopathies (Welander, Markes bery/Udd,Nonaka,Miyoshi,Liang)

SCAPULOPERONEALPATTERN OF WEAKNESS
Acid maltase deficiency
Central core myopathy
Emery-Dreifuss humeroperoneal dystrophy
Facioscapulo humeral dystrophy
Limb-girdle dystrophy 2A(calpain), 2C-F (sarcoglycans),2I (FKRP)
Nemaline myopathy
Scapuloperoneal dystrophy
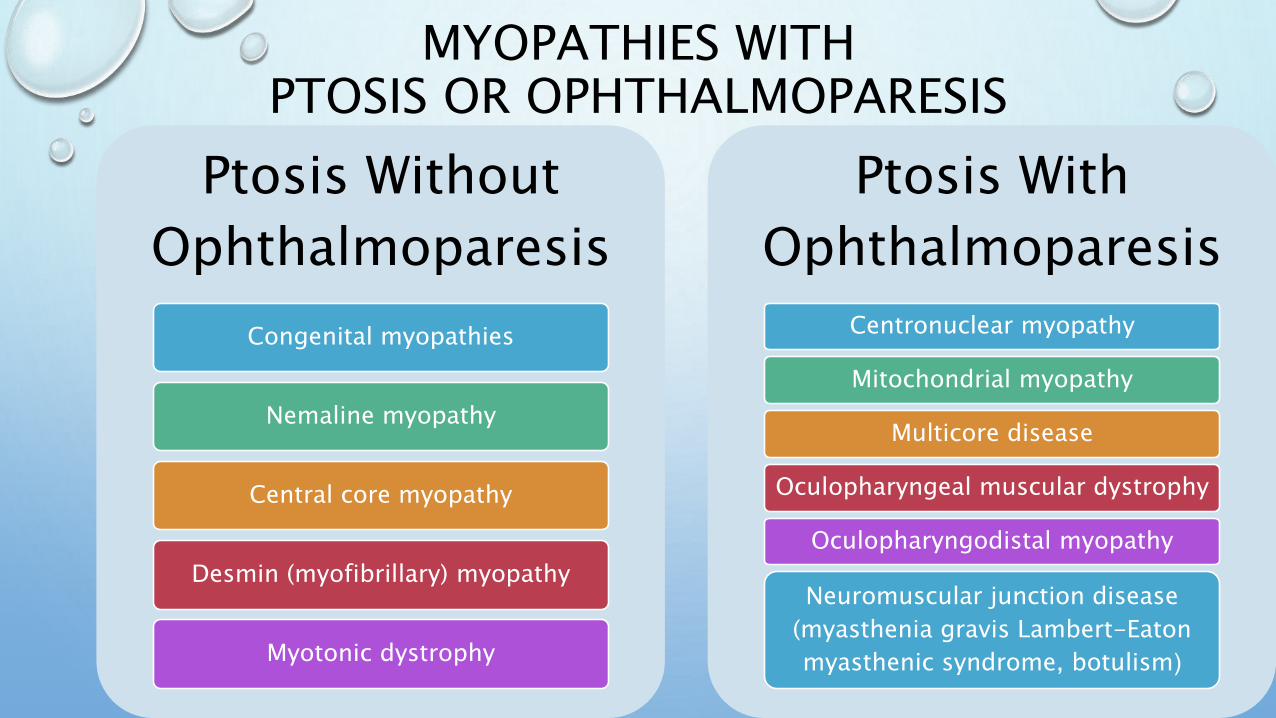
MYOPATHIES WITHPTOSIS OR OPHTHALMOPARESIS
Ptosis Without
Ophthalmoparesis
Congenital myopathies
Nemaline myopathy
Central core myopathy
Desmin (myofibrillary) myopathy
Myotonic dystrophy
Ptosis With
Ophthalmoparesis
Centronuclear myopathy
Mitochondrial myopathy
Multicore disease
Oculopharyngeal muscular dystrophy
Oculopharyngodistal myopathy
Neuromuscular junction disease
(myasthenia gravis Lambert-Eaton
myasthenic syndrome, botulism(

MYOPATHIESWITH PROMINENT NECK EXTENSOR
WEAKNESS
Isolated neck extensor myopathy
Dermatomyositis
Polymyositis
Inclusion body myositis
Carnitine deficiency
Facioscapulohumeral dystrophy
Myotonic dystrophy
Congenital myopathy
Hyperparathyroidism

MYOPATHIESWITH EPISODIC PAIN, WEAKNESS,
AND MYOGLOBINURIA/RHABDOMYOLYSISARelated to
Exercise
‘‘Couch
potato’’
syndrome
Glycogenoses (eg,
McArdle disease)
Lipid disorders (carnitine
palmitoyltransferase deficiency)
Not Related
to Exercise
Central non-neuromuscular causes :
neuroleptic malignant ,status epilepticus
Drugs/toxins
Malignant hyperthermia
Polymyositis/dermatomyositis (rarely)
Viral/bacterial infections

EPISODIC WEAKNESS DELAYEDOR UNRELATED TO EXERCISE
Periodic paralysis
Ca++ channelopathies (hypokalemic)
Na++ channelopathies (hyperkalemic)
Andersen-Tawil syndrome
Secondary periodic paralysis
(thyrotoxicosis)
Other: Neuromuscular junction
diseases
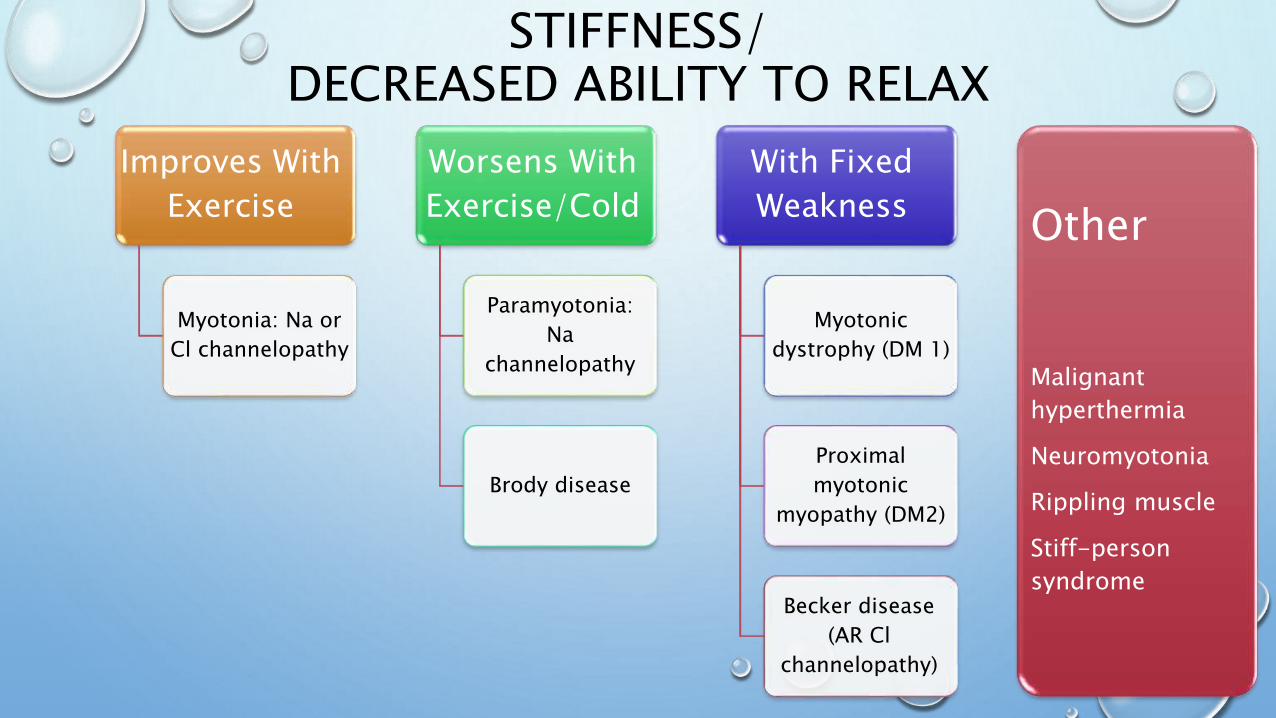
STIFFNESS/DECREASED ABILITY TO RELAX
Improves With
Exercise
Myotonia: Na or
Cl channelopathy
Worsens With
Exercise/Cold
Paramyotonia:
Na
channelopathy
Brody disease
With Fixed
Weakness
Myotonic
dystrophy (DM 1)
Proximal
myotonic
myopathy (DM2)
Becker disease
(AR Cl
channelopathy)
Other
Malignant
hyperthermia
Neuromyotonia
Rippling muscle
Stiff-person
syndrome
DR MOHAMMAD A.S KAMIL
CONSULTANT NEUROLOGIST
NEUROSCIENCES HOSPITAL